
Abstract
Aim
The aim of this study was to investigate if nurses change a child’s peripheral intravenous catheter when clinically indicated.
Background
Today, inserting a peripheral intravenous catheter is a common procedure in hospital care, but this can be painful and traumatic for children. There are guidelines when to change the peripheral catheter in adults, but no similar guidelines was found concerning children. A Cochrane review from 2010 concludes that the policy should be to change the peripheral intravenous catheter when clinically indicated. This includes phlebitis, but also pain, redness, infiltration, swelling, leakage and blockage.
Method
The design was prospective and observational. Daily observations were made at the hospital by one of the researchers and notes were made in a protocol.
Findings
Thirty-three children with a total of 47 peripheral intravenous catheters participated, and 104 observations were made. Of the children, 42% (14/33) developed complications. Among the children with phlebitis grade 2 and 3, the nurses did not change the peripherala intravenous catheter when clinically indicated.
Conclusion
This study shows that phlebitis occurs in children with a peripheral intravenous catheter and the PIC were not changed when clinically indicated. It is the professional’s responsibility to reduce the painful experiences for children during hospital care, and more research concerning nurses’ clinical decisions needs to be conducted.
Background
Inserting a peripheral intravenous catheter (PIC) is a common procedure in hospital care today and about 5,000,000 PICs are used in Sweden every year. 1 This can be a painful experience, especially for a child. 2
The diagnosis of phlebitis is controversial, and many researchers use the definition based on two or more of redness, pain, warmth, erythema, swelling and a palpable cord. 3 The prevalence of phlebitis among children varies between 4.7%, 4 and 17.4%. 5 Evidence-based knowledge of how to prevent complications such as phlebitis is essential, 6 and guidelines concerning this issue have changed over time. However, implementations of guidelines have shown to reduce the frequency of phlebitis even though documentation in medical records was found to be sparse. 6 In Sweden, professionals have produced guidelines primarily for adults, recommending that the PIC should be in situ for as short a time as possible and changed every 48–72 hours. However, in situations where it is difficult to insert the PIC in adults, or when the patient is a child, the catheter can be in situ for longer, provided there is no sign of phlebitis. 7
According to the Centers for Disease Control guidelines, there is no need to replace the PIC more often than every 72–96 hours in order to reduce the risk of phlebitis in adults 8 but scientific evidence suggesting that elective replacement of peripheral intravenous catheters reduces the incidence and severity of thrombophlebitis is limited. 9
A recent Cochrane review 10 concludes that as there is no conclusive evidence in support of such recommendations, the policy should be to change the PIC when clinically indicated. Clinically indicated includes phlebitis but also pain, redness, infiltration, swelling, leakage and blockage.
Research has shown that nurses only partly adhered to clinical guidelines, and the results also revealed that nurses appeared to replace or remove peripheral venous catheters before any severe complications occurred. 11 No similar studies in children have been found.
Aim
The aim of this study was to investigate if nurses’ change a child’s peripheral intravenous catheter when clinically indicated.
Design
An observational study.
Method
The study was performed at a university hospital in the south of Sweden with approximately 50 beds for children. All children aged 0–18 years admitted to the hospital during a three-month period were invited to participate. Inclusion criteria were children and their parents who understood and spoke Swedish and that the PIC had been in situ for at least 24 hours.
Nurses followed the standard routines concerning the care and management of the intravenous peripheral catheters, including use of local anesthetics (e.g. EMLA) and/or sucrose/glucose before inserting the needle. At the time of inclusion, the catheter was inspected by one of the authors (ML).
Daily observations (i.e., once a day) were conducted (ML) until removal, and notes were made based on a study protocol. The reason for removal was noted.
Phlebitis was classified as follows: Grade 1 discomfort/redness <15 mm at the insertion area, Grade 2 redness and tenderness >15 mm at the insertion area in combination with pain and slight swelling; Grade 3 redness, tenderness, swelling and pain at the insertion area >25 mm in combination with a palpable cord in the vein; and finally, Grade 4 was classified as redness, tenderness, swelling and pain at the insertion area >50 mm in combination with pain spreading up the arm. 12
The study was approved by the Ethics Committee at Malmö University (No. HS60-08/1091:14). Informed consent was collected from the parents and from the child where possible. In line with Swedish praxis, if the child was under 15 years of age, the parents’ informed consent was obtained but the child’s own wish was respected. Children over 15 years of age were allowed to decide for themselves. Only one child was over 15 years of age.
Results
A total of 33 children participated. The parents of two children who met the inclusion criteria declined participation. The distribution between boys (n = 18) and girls (n = 15) was almost equal. There was a variation in age between one month and 17 years and seven months. The results of the observation (n = 104) is based on 47 PICs in 33 children and phlebitis occurred among 42% (14/33). Eleven children developed grade 1 phlebitis, and three grades 2 or 3. No child suffered from grade 4. Three cases (Grade 2 and Grade 3), with totally 11 PICs, was chosen to describe whether the nurses’ changed the child’s PIC when clinically indicated or not.
Case report 1
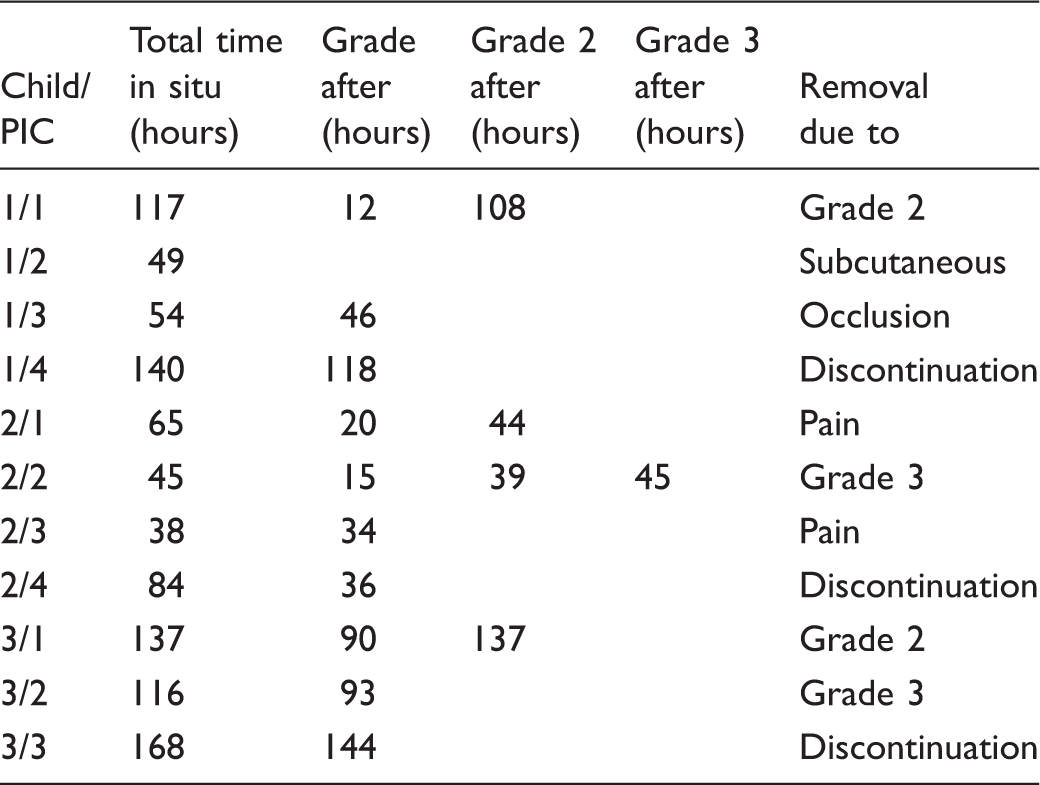
Case reports (n = 3) of PICs (n = 11) and phlebitis in relation to time in situ.
Case report 2
Boy number 2 (15 years old) received four PICs, which were in situ between 38 and 84 hours. The first PIC caused pain and Grade 1 phlebitis was observed after 20 hours. Redness occurred 24 hours later, after which the PIC was removed on account of pain higher up in the arm, approximately 8 cm from the puncture site, in accordance with the boy’s own wish. The second PIC led to pain after 15 hours and more severe pain after 39 hours. After 45 hours, a palpable cord was observed and the PIC duly removed. PIC number three was removed after 38 hours due to pain higher up in the arm, although pain was observed after 34 hours and phlebitis Grade 1 diagnosed. In the case of the fourth PIC Grade 1, phlebitis was observed after 36 hours but the PIC remained in situ for a total of 84 hours (Table 1).
Case report 3
Boy number 3 (3 years old) received three PICs. They were in situ between 116 and 168 hours. PIC number one led to Grade 1 phlebitis after 90 hours when discomfort/redness at the insertion site was observed. After 137 hours, pain was observed and Grade 2 phlebitis diagnosed, after which the PIC was removed. The second PIC was in situ for 116 hours. After 93 hours, observations revealed Grade 1 phlebitis, but it was another 23 hours before the PIC was removed. By that time, the complication had escalated to both pain and a palpable cord in the vein, which corresponds to Grade 3 phlebitis. The third PIC was in situ for 168 hours and removed when the treatment was finished, but observations revealed Grade 1 phlebitis after 144 hours (Table 1).
Discussion
These case reports reveal that the PIC was not removed when clinical complications were observed, which makes it important to highlight the individuals behind the percentage of children with phlebitis. One boy had a PIC inserted into the back of the hand and Grade 1 phlebitis occurred after 15 hours, developing into Grade 2 after 39 hours, but the PIC was not removed until 45 hours due to Grade 3 phlebitis. This is not in line with the recommendations of the Cochrane review, 10 which proposes a policy of changing a PIC when clinically indicated. Unfortunately, no information is available as to why the nurses did not change the PIC in these cases. It may well be that the child experienced severe pain when the PIC was inserted and thus a decision was made to spare the child, as the potential pain that would be caused by the complications was considered less. If so, this is according to Eiman Johansson and co-authors, 11 who showed that nurses’ actions are a balance between minimizing patient discomfort and preventing complications. Research has also indicated that nurses perceive that pain management is not performed systematically nor adapted to the individual, and that guidelines were not always adhered to. 13 Furthermore, specialist nurses have been found to possess a more comprehensive knowledge base concerning pain than general nurses 14 and a bachelor degree among nurses improves the care. 15 However, in the present study, we have no information about the nurses’ educational level.
The nurses in this study did not follow the recommendation to change the PIC when clinically indicated, which raises the question of whether the nurses were attempting to find a balance between patient discomfort, i.e., the potential pain involved in inserting a new PIC or the potential pain of Grade 2 or Grade 3 phlebitis. The present study cannot answer this interesting question, as the strategy differs depending on the nurses’ reason for their actions.
Relevance to clinical practice
The case reports reveal that nurses observe phlebitis but, for reasons that were not specified, chose not to change the PIC when clinically indicated. Although inserting a PIC is a common procedure in hospital care today, it can be a painful experience for children. Further research is required to investigate nurses’ non-compliance with the Cochrane review recommendations for the management of PICs. 10
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
The authors declare that there is no conflict of interest.