
Abstract
Introduction:
Nurses must possess the capacity for compassionate care and exhibit empathy to promote culturally competent care. This research investigated the mediating role of compassion in the relationship between ethnocultural empathy and intercultural sensitivity among nurses.
Method:
The study was conducted at a hospital that provides health care services to refugees. In total, 125 nurses were recruited through the simple random sampling technique. Data were collected using a personal form and three scales. Statistical analysis was performed using SPSS23 and AMOS24.
Results:
Nurses’ cultural sensitivity positively influenced their compassion competence and ethnocultural empathy. Compassion competence did not function as a full mediator in the relationship between intercultural sensitivity and ethnocultural empathy.
Discussion:
This study revealed that exposure to different cultures contributed to compassion competence, ethnocultural empathy, and cultural sensitivity skills in nurses. Cultural competence is a critical component of nursing care; therefore, it should be developed through curriculum revisions and a sensitive and supportive discussion of experiences.
Introduction
The health, disease, disability, birth, and death-related needs of individuals vary significantly depending on their cultural context (Çaglar and Bilgili, 2020). Anatolia, a large part of the Republic of Türkiye, possesses a rich heritage of beliefs and folklore, having been home to many ancient civilizations. Traditional medicine practices, which have developed and diversified over the centuries, are commonly used for various diseases in Türkiye (Karatas et al., 2021). In addition, especially the phenomenon of migration and the resulting cultural change, the changing global population structure have brought different traditional practices to the forefront (Mula et al., 2023). As a result, healthcare institutions, especially hospitals, are critical spaces for providing care to individuals with diverse cultural and personal backgrounds encompassing differences in ethnicity, religion and affiliation. Receiving culturally congruent health care is not merely a privilege but an entitlement for all individuals (Prosen, 2015). This requires healthcare systems to meticulously consider the cultural backgrounds and needs of patients when providing culturally sensitive services (Oikarainen et al., 2019).
Achieving high-quality and patient-centered health care depends on the cultural competence exhibited by health care providers (Papadopoulos et al., 2016). Nurses constitute the largest group of the health care team, have the most contact with patients, are important actors in the health system, and promote culturally sensitive care (Sarkhani et al., 2022). Therefore, nurses should have high cultural sensitivity to provide culturally appropriate care to patients and their relatives, who are considered important stakeholders in patient care. As a result, nurses are expected to not only acquire technical skills but also to demonstrate sensitivity to practices that reflect the cultural context of the individuals they care for and the communities they serve (National Core Education Program in Nursing [HUÇEP], 2022; International Council of Nurses [ICN], 2019). Adopting a holistic approach inherent in nursing practice requires consideration of the cultural backgrounds of patients (Prosen, 2015). Nurses are also subject to cultural diversity and have cultural values that may affect their decision-making processes and behaviors (Papadopoulos et al., 2016). Therefore, they should demonstrate cultural sensitivity to communicate effectively with patients from different cultural backgrounds and implement care adapted to individual needs (Bakan & Yildiz, 2021; Kuwano et al., 2016). The cultivation of cultural sensitivity encompasses a myriad of personal attributes, including but not limited to empathy, sympathy, effective communication, self-esteem, faith, compassion, and loyalty (Arli Karadag & Bakan, 2018; Vural Dogru & Utli, 2022).
Ethnocultural empathy, defined as an individual’s capacity to understand and empathize with the feelings, perspectives, and concerns of individuals with different cultural backgrounds (Egitim and Akaliyski, 2024), serves as an important tool for nurses to develop a higher receptivity to different cultural values and norms and thus promote intercultural sensitivity (Purabdollah et al., 2021; Yurttas and Aras, 2020). This predisposition enables the development of constructive attitudes and behaviors towards patients from different cultural environments (Çingöl et al., 2021). Culturally sensitive care entails the acquisition of comprehensive knowledge, skills, attitudes, and effective interpersonal relationships vis-à-vis diverse cultural, belief, and religious backgrounds, thereby facilitating the delivery of empathetic and compassionate health care services (Arkan et al., 2020; Beaumont et al., 2016; Durkin et al., 2016; Vural Dogru & Utli, 2022) and promoting empathic connections with patients from diverse cultural backgrounds (Yurttas & Aras, 2020). Implementing culturally competent care not only improves patient outcomes but also reduces health disparities (Papadopoulos et al., 2016).
Compassion, an integral part of cultural sensitivity, represents the essence of nursing practice (Babaei et al., 2022). This approach enables nurses to understand the subtleties of a patient’s conditions, accurately discern their emotional states, and provide encouragement. Compassionate nurses can effectively empathize with patients, provide emotional consolation, and strengthen their spirits by adapting to the physical, spiritual, and emotional challenges they face (Lee & Seo, 2022). As a result, compassion ensures the provision of individualized nursing care that is compatible with the unique imperatives of each patient (Hong et al., 2017).
In healthcare settings, the provision of care requires a dual approach characterized by cultural competence and compassion, where individual values, cultural backgrounds, and health beliefs are duly taken into account (Papadopoulos et al., 2016). Although compassion is a universal emotion, its manifestation may vary across cultures as it is contextualized by cultural norms, values, and practices (Kariyawasam et al., 2022). Nurses can skillfully interact with individuals from different cultural backgrounds with compassion through the development of ethnocultural empathy and cultural sensitivity (Singh et al., 2018). As a result, they need to actively develop their cultural competence to navigate these multifaceted interactions (Beaumont et al., 2016; Durkin et al., 2016). In essence, ethnocultural empathy, intercultural sensitivity, and compassion competence are indispensable components for providing high-quality, patient-centered healthcare in diverse and multicultural healthcare settings. These skills improve effective communication, promote trust, and ultimately contribute to improving health outcomes for patients from diverse cultural backgrounds (Dewar & Nolan, 2013).
In recent years, significant global migration trends have been observed, with individuals settling in foreign countries voluntarily or forcibly due to numerous factors such as ethnic conflicts, oppressive governments, wars, environmental crises, and economic difficulties (Çingöl et al., 2021). The Syrian civil war, in particular, has led to one of the most serious refugee crises in history, resulting in a significant influx of migrants (United Nations High Commissioner for Refugees [UNHCR], 2015). Türkiye, adopting an “open door” policy since the onset of the war, has become the foremost destination for refugees, having accommodated approximately 3,194,185 (62.6%) Syrians (Directorate of Migration Management, 2024 While some resided in designated camps, the majority were settled in other cities (International Organization for Migration, 2024). This global phenomenon has received significant attention in both national and international scholarship. On the other hand, the recent collapse of the Afghan government has resulted in Afghans constituting one of the largest refugee populations worldwide (UNHCR, 2023). Türkiye, hosting 133,062 Afghans under international protection status, ranks as the second-highest recipient of international protection applications (UNHCR, 2022). Presently, the nation hosts over 3.5 million individuals under temporary protection status, primarily Syrians, alongside hundreds of thousands of refugees and protection beneficiaries, predominantly from Afghanistan, Iran, Iraq, and other nations.
Refugees encounter numerous challenges in host countries, including dire economic circumstances, substandard housing conditions, inadequate sanitation, malnutrition, limited access to education and employment opportunities, unfamiliarity with the local language, social exclusion, and instances of discrimination (Amnesty International, 2016). In addition, factors such as low education levels, unequal resource distribution, inequalities in access to health services, language barriers, and cultural differences negatively affect overall health outcomes (UNHCR, 2015). In this context, assessing and enhancing the cultural competence of health care practitioners serving refugee populations is imperative to improve their health status (Matlin et al., 2018). Given that empathy and compassion are pivotal predictors of cultural sensitivity, this study aimed to determine the mediating role of compassion in the relationship between ethnocultural empathy and intercultural sensitivity among nurses. Our research hypotheses are as follows:
Hypothesis 1 (H1). There is a positive correlation between the levels of intercultural sensitivity and ethnocultural empathy of nurses.
Hypothesis 2 (H2). There is a positive correlation between the levels of intercultural sensitivity and compassion competence of nurses.
Hypothesis 3 (H3). There is a positive correlation between the levels of compassion competence and ethnocultural empathy of nurses.
Hypothesis 4 (H4). Compassion competence has a mediating role in the correlation between nurses’ intercultural sensitivity and ethnocultural empathy levels.
Method
Study Design
A cross-sectional, correlational, and descriptive research design was employed in this study.
Working Environment and Sampling Method
This study was conducted in a province in the western region of Türkiye, which has a significant refugee population due to its role as an industrial hub. According to the latest data from the Directorate of Migration Management (2024), there are 53,427 registered Syrian refugees and 13,675 foreign residents with residence permits in the city. The target population consists of 160 nurses working in a training and research hospital providing healthcare services to refugees. The sample size was determined as 114 nurses using the known population formula with a 95% confidence level and a 5% margin of error. Considering possible attrition, the sample size was increased by 10% and the final recruitment target was determined as 125 nurses. Nurses eligible for inclusion had at least one year of nursing experience, were responsible for caring for at least one adult refugee patient, and gave their consent to participate in the study using simple random sampling. Nurses with administrative roles, such as service managers, were excluded because they were not directly involved in the provision of patient care. Figure 1 illustrates the general methodology of our research.
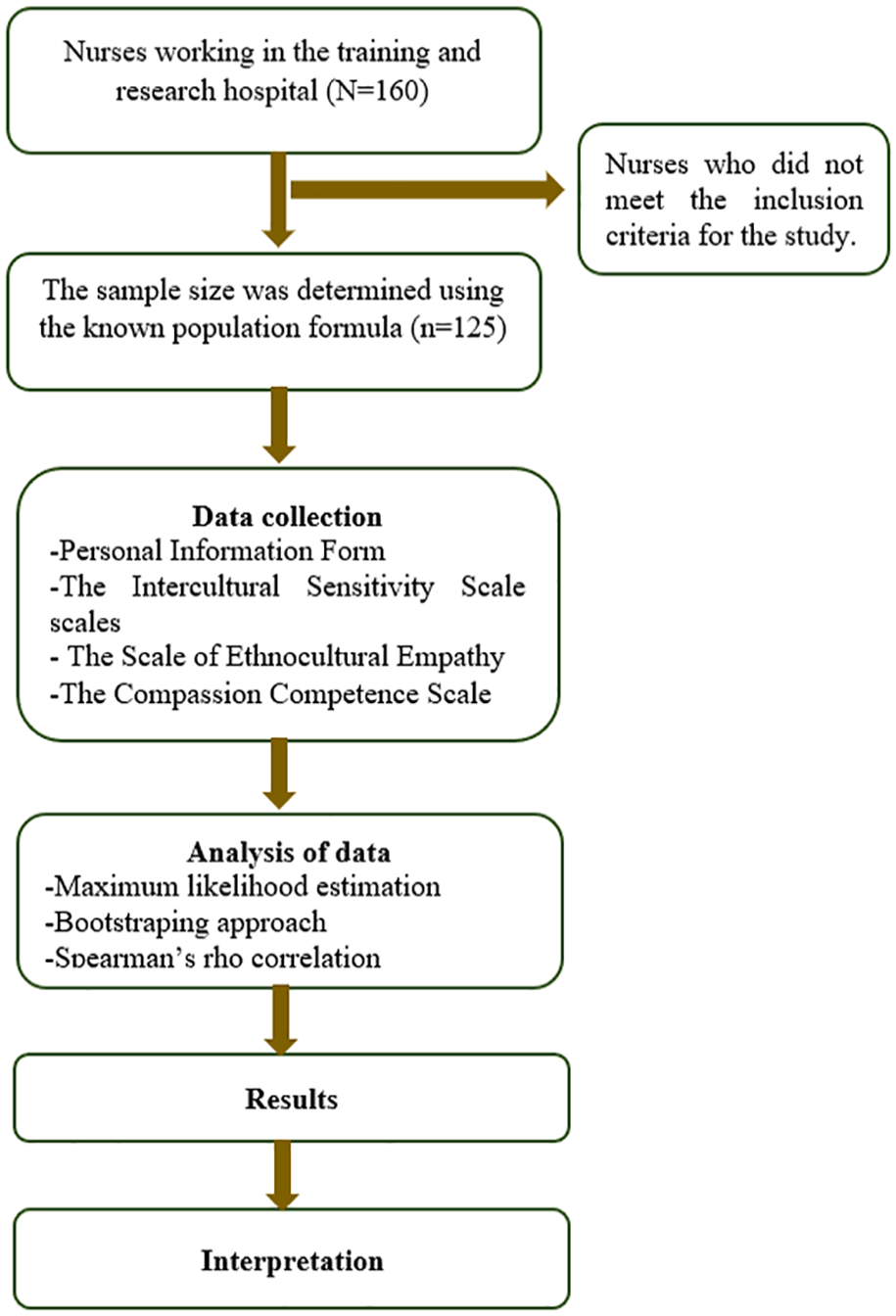
Data Flow Diagram for This Research.
Data Collection
First, the necessary permissions were obtained from the hospital administration and the Provincial Health Directorate to conduct the study. Two researchers (R.N., PhD) tried to contact potential participants through regular visits (every Friday) to hospital clinics. These visits targeted internal and surgical units within their scope, where researchers informed nurses about the study and distributed data collection forms to interested participants. The forms, which were expected to be completed in approximately 15 minutes, were then collected during follow-up visits. The data collection process began in March 2023 and was completed in May 2023 when the required sample size was reached. Data were collected using the Personal Information Form, Intercultural Sensitivity Scale (ICS), Ethnocultural Empathy Scale (ETS), and Compassion Competence Scale (CCS).
Instruments
Data were collected using a descriptive information form and three scales.
Personal Information Form
The researchers prepared this form in accordance with the relevant literature. The survey consisted of eight questions regarding the sociodemographic information of the nurses (such as age and gender), their professional characteristics (such as level of education, length of service and department), and their experiences of providing care to refugees (such as difficulties encountered and the use and adequacy of interpreter support).
Intercultural Sensitivity Scale
The Turkish validity and reliability study of the scale developed by Chen and Starosta (2000) was conducted by Bulduk et al. (2011). This scale uses a five-point Likert-type structure consisting of 24 items distributed into five sub-dimensions: interaction participation (seven items), respect for cultural differences (six items), interaction confidence (five items), interaction enjoyment (three items), and interaction attention (three items). Scores on the scale range from a minimum of 24 to a maximum of 120, and there is no specified cut-off point. Higher total scores indicate greater cultural sensitivity. While the Cronbach alpha coefficient was found to be 0.72 in the Turkish validity and reliability study, this coefficient was calculated as 0.66 in our study.
Scale of Ethnocultural Empathy
The SEE, developed by Wang et al. (2003), is a 30-item scale using a five-point Likert-type scale. Özdikmenli-Demir and Demir (2014) conducted the Turkish validity and reliability study of the scale. It consists of three sub-dimensions: empathic feeling and expression (11 items), empathic perspective taking and acceptance of cultural differences (11 items), and empathic awareness (8 items). High total scale scores indicate high levels of ethnocultural empathy. While the Cronbach alpha coefficient was reported as 0.93 in the Turkish validity and reliability study, this coefficient was calculated as 0.64 in our study.
Compassion Competence Scale
CCS, developed by Lee and Seomun (2016), is the Turkish validity and reliability study of the scale conducted by Çiftçi and Aras (2021). The scale consists of 11 items and three sub-dimensions: communication (five items), sensitivity (three items), and insight (three items). Each item in the scale is scored between 1 and 5, with higher total scores indicating higher levels of compassion competence. While the Cronbach alpha coefficient was reported as 0.79 in the Turkish validity study, it was calculated as 0.78 in our study.
Ethical Considerations
Necessary permissions were obtained for the use of measurement tools during the planning phase of the study. Ethical approval was obtained from the local clinical research ethics committee before the study was conducted (date: 26 January 2023, number: 2023–2020), and the study complied with the principles stated in the Declaration of Helsinki. Participants were provided with comprehensive verbal and written explanations about the study before participating in the study. Participants were informed that their participation was voluntary, that their responses in the questionnaires would remain anonymous, and that the study findings would be used only for educational and scientific purposes. Submission of completed questionnaires was considered as consent to participate in the study.
Data Analysis
Data were analyzed using IBM SPSS V23 and IBM AMOS V24 package programs. Descriptive statistics were used to present categorical outcome variables as number (n) and percentage (%). In this study, nurses’ ethnocultural empathy level was the independent variable, intercultural sensitivity level was the dependent variable and compassion competence was the mediator variable. The normality of the scale scores was assessed using the Kolmogorov-Smirnov test. The Maximum Likelihood Estimation (MLE)-Bootstraping approach was used to test the research model and the mediating role. Model fit was assessed using fit indices, CMIN/DF (Χ2/DF), Comparative Fit Index (CFI), Incremental Fit Index (IFI), Normed Fit Index (NFI), Tucker-Lewis Index (TLI) and Root Mean Square Error of Approximation (RMSEA). Spearman’s rho correlation coefficient was used to examine the relationships between scale scores that did not show normal distribution. The significance level was taken as p < .05. Confirmatory factor analysis (CFA) was used to evaluate the construct validity of the research variables, thereby ensuring the validity of the measurement tools (Table 1).
Fit Indices of Measurement Tools.

Results
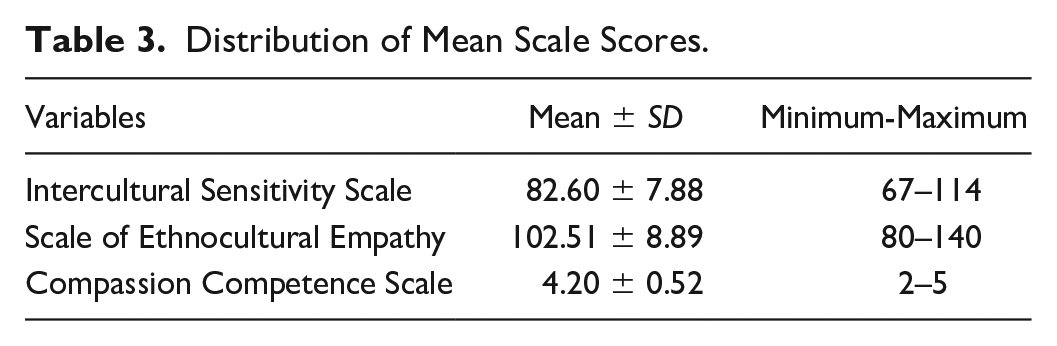
The personal and professional characteristics of the 125 nurses who participated in the study are presented in Table 2, and the mean scores on the scales are presented in Table 3. Analyses showed a moderate positive correlation between the nurses’ ethnocultural empathy and intercultural sensitivity scores (r = .564; p < .001), a low positive correlation between ethnocultural empathy and compassion competence scores (r = .34; p < .001), and a low positive correlation between intercultural sensitivity and compassion competence scores (r = .235; p = .008; Table 4).
Characteristics of Nurses (N=125).
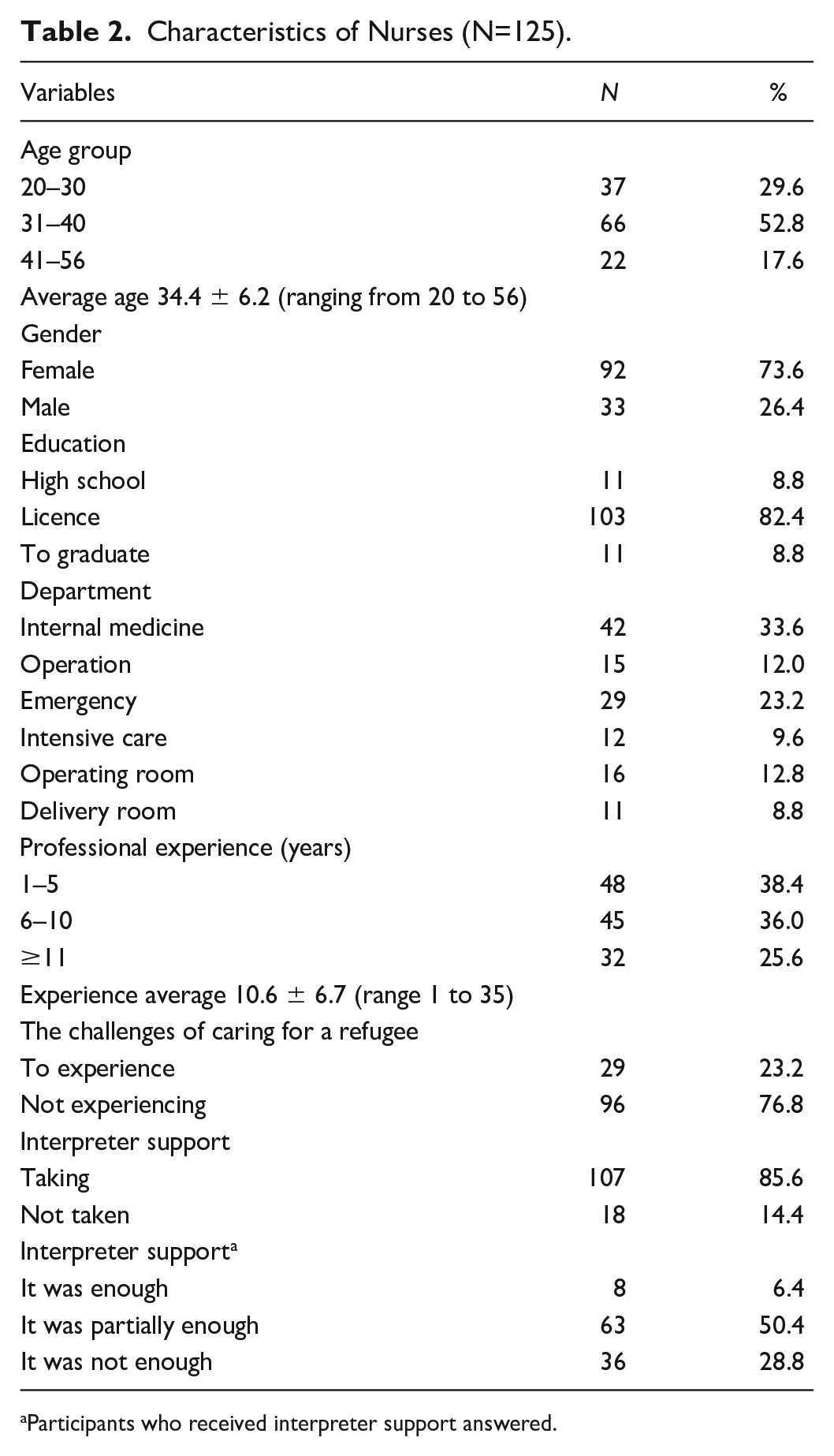
Participants who received interpreter support answered.
Distribution of Mean Scale Scores.
Relationship Between Scales.
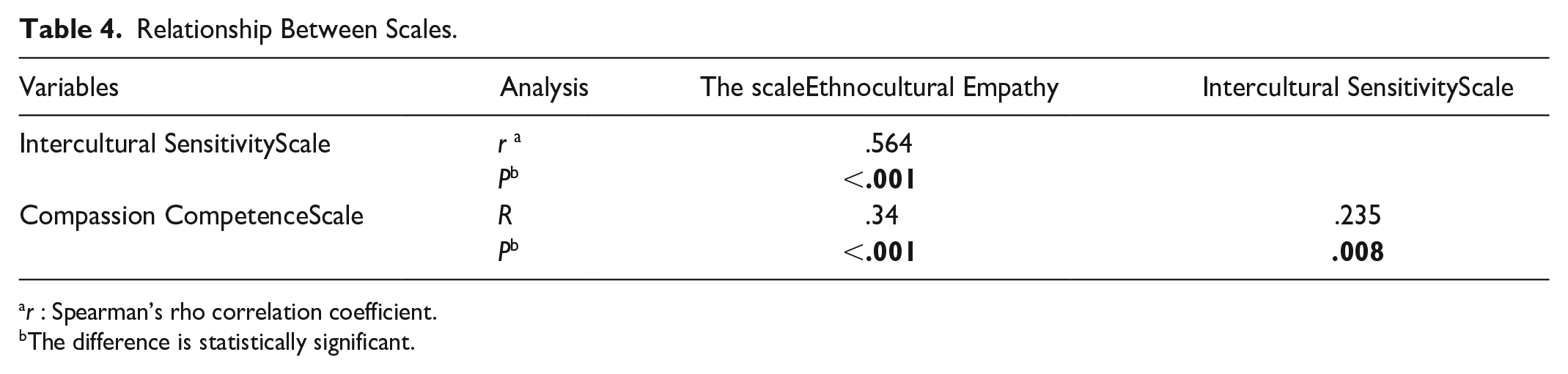
r : Spearman’s rho correlation coefficient.
The difference is statistically significant.
Our initial hypothesis was supported by analyses showing a positive correlation between nurses’ intercultural sensitivity and ethnocultural empathy (β = 0.756; p < .05). The relationships were then re-evaluated by including compassion competence as a mediator in the model. The findings revealed a significant direct positive relationship between intercultural sensitivity and compassion competence (β = 0.271; p < .05) and between ethnocultural empathy and intercultural sensitivity (β = 0.643; p < .05). These results confirmed our second and third hypotheses. However, when compassion competence was included in the model, the previously significant direct relationship between compassion competence and ethnocultural empathy became statistically insignificant (β = 0.100; p > .05; Table 5). As a result, our final hypothesis was not supported because compassion competence did not fully mediate the relationship between intercultural sensitivity and ethnocultural empathy. The intercultural sensitivity levels of the nurses participating in the study positively affected both compassion competence (0.27) and ethnocultural empathy (0.64), and statistically significant β coefficients were found between them (p < .05; Figure 2).
Mediator Structural Modeling for the Intercultural Sensitivity Scale, Ethnocultural Empathy Scale, and Compassion Competence Scale.
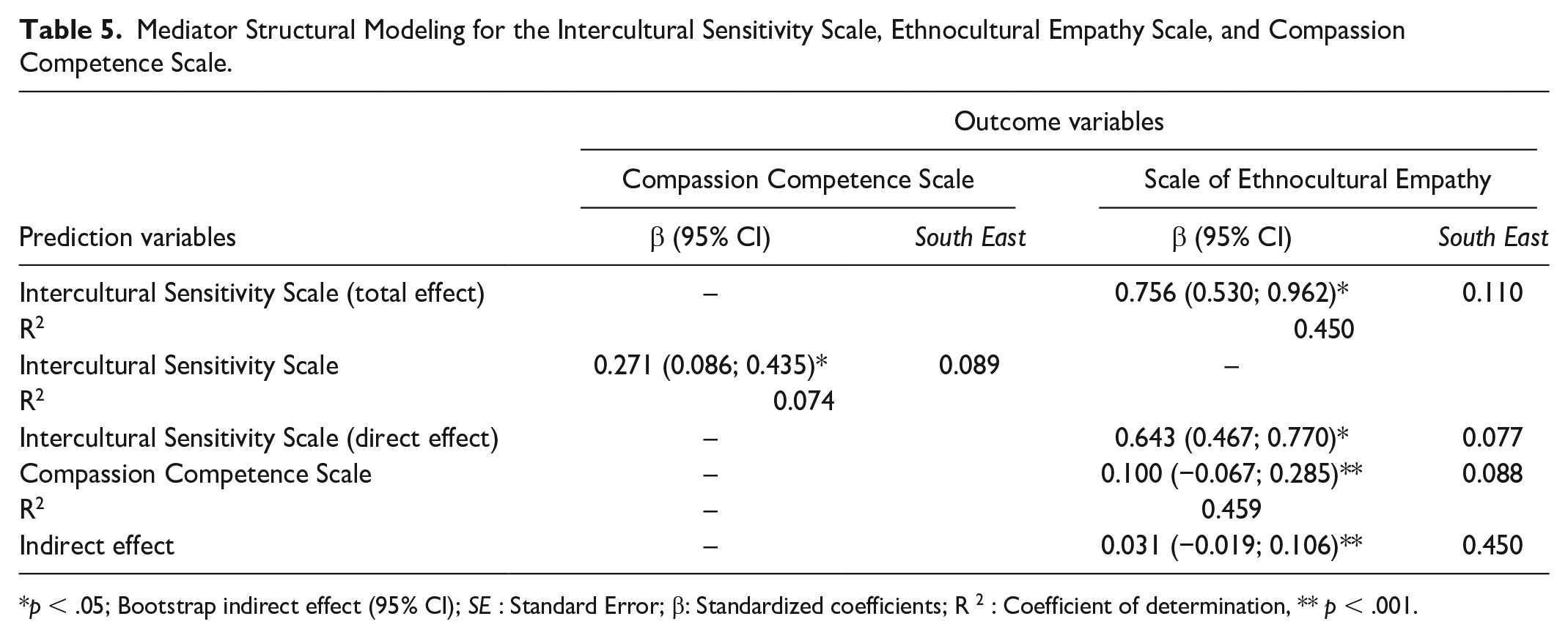
p < .05; Bootstrap indirect effect (95% CI); SE : Standard Error; β: Standardized coefficients; R 2 : Coefficient of determination, ** p < .001.
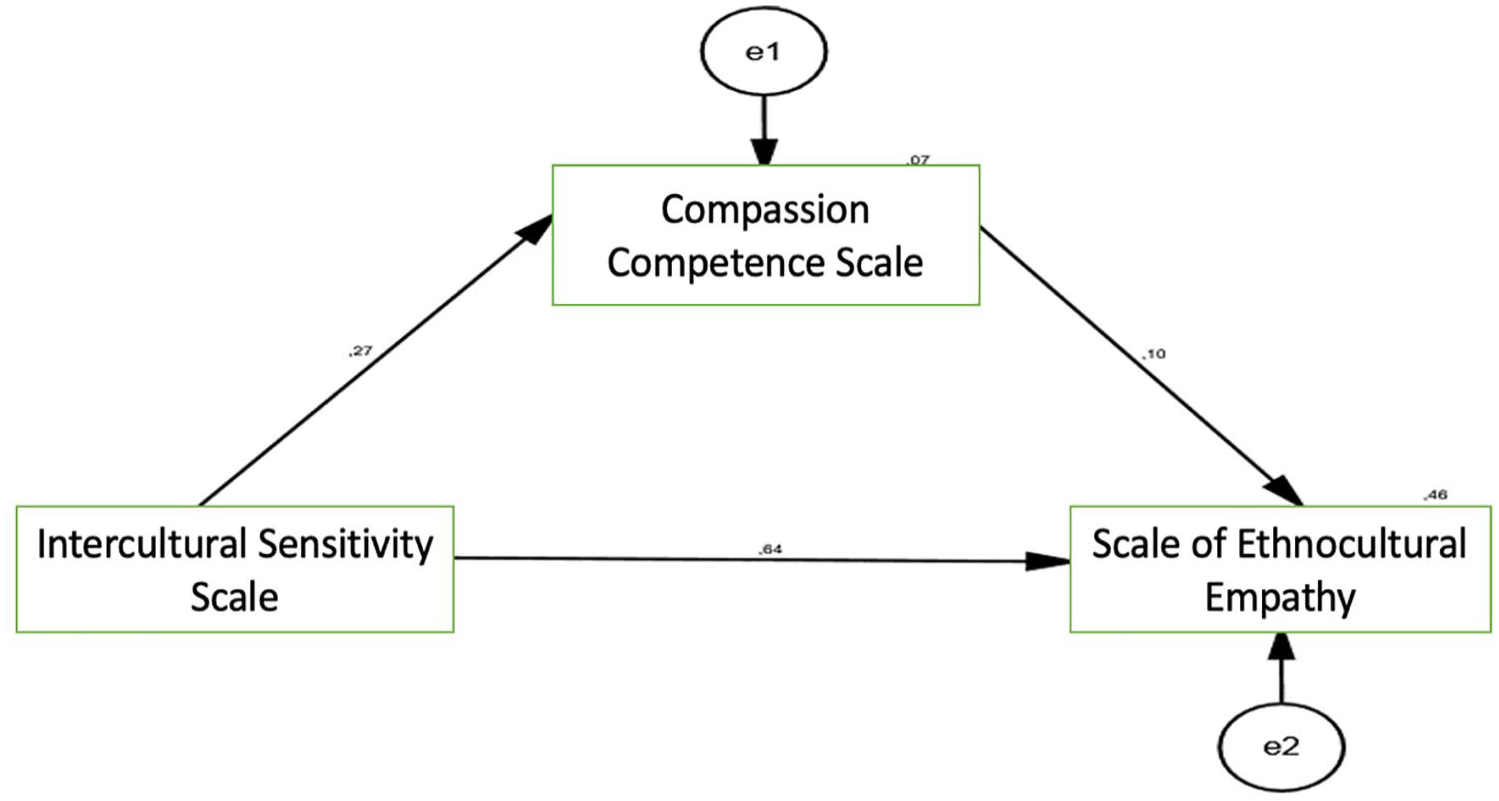
Relationships among Variables in the Basic Structural Model for Intercultural Sensitivity, Ethnocultural Empathy, and Compassion Competence
Discussion
Given its geographical location, the region in which this study was conducted hosts many refugees, and nurses frequently encounter patients from diverse cultural backgrounds. Consequently, they must provide culturally sensitive care with an empathetic approach to meet the specific needs of these patients (Yurttas & Aras, 2020). Our study revealed that the intercultural sensitivity of nurses was at an average level. This finding is consistent with the findings of several studies conducted in Türkiye on intercultural sensitivity levels (Özdemir et al., 2022; Polat & Terzi, 2020; Yilmaz et al., 2017). In contrast, a study in Iran by Purabdollah et al. (2021) indicated low intercultural sensitivity among nurses, and another study involving community health nurses in Taiwan reported low mean scores for cultural sensitivity (Chang et al., 2013). The findings of the research conducted in our country differ from those of studies conducted in other countries. This discrepancy may be attributed to the frequent provision of care by nurses to individuals from different cultural backgrounds because of the country’s geopolitical location. In addition, the limited effectiveness of cultural sensitivity training, owing to the absence of structured and comprehensive educational programs on cultural competence (Karataş et al., 2021; Lekas et al., 2020), may have hindered the enhancement of nurses’ cultural sensitivity.
In this study, the compassion level of nurses was notably high. Previous studies conducted in Türkiye revealed similar findings (Çinar, 2019; Yerköy Ates, 2023). However, studies conducted in Korea have indicated that nurses exhibit a moderate level of compassion competence (Cho & Seo, 2018; Hong & Han, 2021; Jeong & Seo, 2022; Lee & Seo, 2022). The observed differences in nurses’ compassion levels may be attributable to the cultural diversity of the sample groups.
Nurses must adopt a humanistic and empathetic approach to patient interactions to deliver effective and appropriate nursing care (Özdemir and Kaplan, 2024). The findings of our study indicated high levels of ethnocultural empathy among nurses. Erçek Karcı and Şen (2024) observed that nurses and midwives possessed empathetic skills, with an associated increase in intercultural sensitivity in care delivery as their empathy skills improved. Other studies have reported persistent levels of ethnocultural empathy between officials and other health care workers: high (Aliabadi et al., 2021; Sahin Akgün and Özdemir, 2015; Sahin et al., 2018), medium (Sedaghati Kesbakhi et al., 2017) and low (He et al., 2024). These different findings in the literature in our research can be attributed to various situational and personal factors such as genetics, gender, education and the ability to develop empathy skills (Sedaghati Kesbakhi et al., 2017). It is thought that the individual characteristics of the nurses in our sample may have impacted their empathy skills, contributing to the observed variations in the results.
Our study revealed that nurses’ intercultural sensitivity increased as their level of ethnocultural empathy also improved. These findings are similarly consistent with previous research that emphasized a positive development between intercultural and empathy support among nurses (Kürtüncü et al., 2018; Yurttas and Aras, 2020). Nurses who exhibit sensitivity to diverse cultures and heightened empathy skills tend to deliver more effective care (Dikmen et al., 2016). Studies conducted with intensive care nurses (Soleimani and Yarahmadi, 2023) and clinical nurses (Geun, 2023; Suk et al., 2018) indicate that empathy is a significant and explanatory variable predicting cultural competence. These findings underscore the importance of heightened intercultural sensitivity among nurses to facilitate enhanced empathic understanding of patients from diverse cultural backgrounds, consequently leading to more effective and higher-quality care.
This study found a positive correlation between intercultural sensitivity and compassion competence among nurses and showed that intercultural sensitivity serves as a predictor of compassion competence. The literature emphasizes that nurses’ perceptions of compassion have a significant impact on their intercultural sensitivity (Vural Dogru & Utli, 2022). Arli Karadag and Bakan (2018) also reported a significant positive correlation between nurses’ intercultural sensitivity and compassion levels. The tendency to address challenges arising from culturally sensitive care with compassion enables nurses to comprehend the underlying motives behind their emotions, thoughts, and subsequent behaviors (Özdelikara & Babur, 2020; Vural Dogru & Utli, 2022). Therefore, interventions aimed at increasing nurses’ intercultural sensitivity are expected to improve their compassion competence.
The study found that there was a significant positive correlation between nurses’ empathy skills and compassion competencies. These findings are consistent with previous research showing a positive relationship between compassion and empathic tendencies among nursing students (Özdelikara & Babur, 2020). Nurses who exhibit empathic attitudes towards patients tend to exhibit higher levels of compassion, with empathy having a positive effect on compassion (Arkan et al., 2020). In line with these findings, it can be said that nurses who provide care to patients with different cultural backgrounds communicate more sensitively and empathically; thus, their compassion competencies are positively affected.
Intercultural sensitivity can increase compassion and empathy, which in turn can increase intercultural sensitivity (Ménage et al., 2017). In our study, structural equation modeling was used to examine the last hypothesis, which revealed that nurses’ intercultural sensitivity positively affects both compassion competence and ethnocultural empathy skills. However, contrary to our hypothesis, the model indicated that compassion competence did not serve as a mediator between intercultural sensitivity and ethnocultural empathy skills. This finding, which rejects our last hypothesis, may be related to the fact that although these concepts are intertwined, they direct nursing actions differently. Compassion competence, which emphasizes the emotional dimension of care, is not specifically contingent on cultural considerations (Goetz et al., 2010). Compassion is a broader concept that encompasses how nurses connect with patients and respond to their needs, regardless of their cultural background. In contrast, intercultural sensitivity and ethnocultural empathy focus specifically on the awareness, understanding, and recognition of cultural differences and encompass appreciation and respect for various cultural norms, values, and communication patterns (Samovar et al., 2010). While these three concepts complement each other and are valuable in providing inclusive and effective healthcare, our study highlights the importance of developing nurses’ intercultural sensitivity and ethnocultural empathy skills to meet the healthcare needs of culturally diverse patient populations, including refugees. The provision of holistic and patient-centered care within diverse and multicultural health care settings is possible with nurses who demonstrate compassion, empathy, and sensitivity toward individuals from varied cultural backgrounds.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the study was conducted in a single province in Türkiye, which limits the generalizability of the results. Future studies that include a larger cohort of nurses providing care to refugees across age groups, including children and adolescents, may reveal different findings. Additionally, the analyses in this study used only the compassion competence variable to predict ethnocultural empathy and cultural sensitivity. Beyond these variables, future research should investigate the potential effects of individual variables such as cultural background and organizational variables such as ethical climate on compassion competence. In addition, data collection relied on self-report scales.Given the complexity of ethnocultural empathy, cultural sensitivity, and compassion, participants may be inclined to present themselves in a positive light, potentially affecting the results. Therefore, supplementing quantitative approaches with qualitative research methods and observational data can provide deeper insights into the dynamics between these constructs.
Conclusions and Recommendations
Our study revealed that nurses had above-average cultural sensitivity scores and also showed high levels of ethnocultural empathy and compassion. Compassion competence, in particular, emerged as a predictor of both intercultural sensitivity and empathy among nurses. In addition, this study revealed that as nurses’ intercultural sensitivity level increased, their ethnocultural empathy skills and compassion competence increased, and compassion competence in turn increased their ethnocultural empathy skills. However, our findings showed that compassion competence did not act as a mediator between nurses’ intercultural sensitivity and ethnocultural empathy skills. Given that these three competencies are essential for comprehensive and effective healthcare delivery in our increasingly diverse world, it is imperative that nurses are competent in these areas.
In addition to the didactic instruction integrated into nursing undergraduate and graduate curricula regarding intercultural sensitivity and ethnocultural empathy, offering students practical experiences with patients from diverse cultural backgrounds and engaging them in discussions on case studies and simulations featuring culturally diverse scenarios can enhance nurse candidates’ ability to recognize cultural factors influencing patient interactions and care. Furthermore, integrating assessment tools for cultural competence into nursing education evaluations enables students to critically assess their progress in intercultural sensitivity and ethnocultural empathy, thereby identifying areas for enhancement.
Recognizing that cultural competence is an ongoing process that involves continuous learning and adaptation to meet the changing needs of diverse patient populations, nursing professionals should be encouraged to participate in seminars, educational programs, and workshops focused on increasing cultural competence. Nurses equipped with high levels of ethnocultural empathy and intercultural sensitivity are well positioned to address disparities in healthcare access and treatment among culturally diverse populations, including refugees. As a result, nurses with a heightened awareness of such issues can advocate for equitable care and actively work to reduce such disparities.
Footnotes
Acknowledgements
The authors would like to thank all the nurses who contributed to our work. They would also like to thank the Reviewers who strengthened our article with their suggestions.
Author Contributions
RAE: Manuscript design and primary author; study design, design analysis, and interpretation of data; tables; critical revision of manuscript. TB: Study conception and design; data collection and interpretation; tables; writing of manuscript. FE: Study conception and design; data collection and interpretation; tables; writing of manuscript.
Conflict of Interest Statement
The author(s) declared that there were no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financing
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Statement
This study was approved by the local clinical research ethics committee (dated 26 January 2023, approved number: 2023–2020).