
Abstract
Introduction:
Globally, health care organizations need to provide quality, culturally congruent health care to increasingly diverse patients. Nursing education institutions must therefore produce culturally competent nursing professionals to provide safe and culturally congruent care. This review aimed to identify and outline strategies to enhance cultural competence of undergraduate nursing students.
Methodology:
The integrative literature review followed the five steps of Lubbe et al. searching the university Libguides, EBSCOhost, Scopus, and Google Scholar databases for literature published between 2014 and 2023 that met the inclusion criteria. The methodological quality was ensured through the John Hopkins Evidence-based Appraisal Tool.
Results:
Five themes emerged as strategies that can enhance cultural competence for nursing students: integrating cultural competence into undergraduate nursing curriculum, cultural immersion, innovative pedagogical approaches, role of nurse educators, and students’ assessment.
Conclusion:
Findings provide nurse educators with evidence-based information on strategies to enhance cultural competence of undergraduate nursing students at nursing education institutions.
Keywords
Introduction
Forming connections with culturally diverse individuals without cultural competence is a challenging endeavor (Rukadikar et al., 2022). Globally, health care organizations need to provide quality, culturally congruent health care to increasingly diverse patients; this is compounded by global movement of nursing professionals. Gradellini et al. (2021) argued that it is essential to therefore incorporate cultural competence and intercultural communication in nursing education institutions (NEIs). As a primary foundation of clinical nursing, cultural competence is crucial in enhancing patient trust, reducing health care inequalities, and improving cultural safety (Sharifi et al., 2019). Cultural competence is the vigorous process of developing the ability to deliver effective, safe, and quality care to patients by considering their different cultural aspects (Sharifi et al., 2019). Previous research indicates that nurses in culturally diverse contexts struggle with the notion of cultural competence (Almutairi et al., 2015, 2017; Shopo et al., 2023). Nursing students, through clinical practice, encounter different linguistic backgrounds, religious affiliation, ethnic or racial origins, immigrants, migrants, and refugees. Therefore, there is a need for health care professionals, including students, to be adequately trained to render culturally competent care (Zarzycka et al., 2020).
Diversity is based on a variety of factors, including beliefs, attitudes, values, languages, religion, birthplace, citizenship status, ethnicity, race, kinship and family networks, educational background, past discrimination, and bias experiences, among others (Jeffreys, 2019). Cultural competence therefore refers to how the concept of respect is practiced in ensuring that varied populations’ cultural beliefs, values, rights, and expectations are recognized in the delivery of culturally relevant health care (Rukadikar et al., 2022). Cultural competence as a strategy improves the capacity of health care systems, and providers, to render culturally responsive health care and positive patient outcomes. Cultural competence is associated with better communication during patient–nurse interactions, improved patient understanding of health issues, and compliance with recommendations for medication and lifestyle modifications (Zarzycka et al., 2020).
Cultural competence as a model of health care service delivery consists of five concepts: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desire (Campinha-Bacote, 2002). These concepts of Campinha-Bacote’s (2002) model have a symbiotic relationship with each other and therefore must be addressed in every encounter with the client.
Cultural competence is a skill that can be taught, trained, and achieved (Stubbe, 2020). Nursing students from multicultural contexts experience challenges during transcultural nursing care, suggesting a lack of cultural competence (Nuuyoma et al., 2024). Owing to that, health care organizations where clinical practice is conducted, together with NEIs, have substantial roles in preparing and improving nursing students’ cultural competence. In addition, incorporating cultural competence into higher education institutions is a principal aspect of the creation of cross-cultural settings where undergraduate students and academics can expand their conceptions of how culture and belief systems influence professional decision-making (Cross et al., 2020). This is also the case in nurse–patient interactions.
Research demonstrates that nurses who share a similar culture and language as their patients score higher on perceptions of cultural competence than those who were born in different countries (Almutairi et al., 2017). However, a multi-nation study with undergraduate nursing students from Belgium, Spain, Portugal, and Turkey reports learning needs and gaps in training regarding students’ ability to provide culturally and linguistically appropriate care, as well as a lack of exposure to culturally diverse clients (Antón-Solanas, Tambo-Lizalde, et al., 2021). Moreover, findings from a recent study by Nuuyoma et al. (2024) suggest that the cultural competence of undergraduate nursing students in low-and-middle-income countries like Namibia warrants enrichment. Similarly, Mhlongo (2016) argues that cultural competency pedagogy in nursing in South Africa is inadequate, and advocates for the development of nursing education that is culturally appropriate for the low-and-middle-income country’s context.
Given this background, there is a critical need for NEIs to produce nursing professionals who are culturally competent to render health care that is culturally safe and sensitive for all patients. A gap exists in evidence-based literature, which outlines strategies that can be used to enhance the cultural competence of undergraduate nursing students at NEIs. Therefore, this review aimed to critically evaluate and synthesize recent peer-reviewed scientific literature to understand and outline strategies that can be used to enhance the cultural competence of undergraduate nursing students at NEIs.
Method
The integrative literature review (ILR) is described as a distinctive form of research that generates new knowledge of an identified topic (Toracco, 2005). The authors followed a rigorous process guided by the five steps of ILR described by Lubbe et al. (2020).
Composition of a Review Question
Riva et al. (2012) suggest that a strong research question can be framed using the PICOT framework. The PICOT framework refers to Population, Phenomenon of Interest, Comparison, Outcome and Timeframe. However, in line with the current ILR, the researchers in this current study applied PIOS as this framework was also applied by Nyaloko et al. (2023). The PIOS framework variation refers to P—population, I—phenomenon of interest, O—outcome, and S—setting (Nyaloko et al., 2023). The following research question was then formulated: “What is the best available evidence on strategies to enhance the cultural competence of undergraduate nursing students at nursing education institutions?”
Sampling Process
A systematic sampling process based on the two steps described below was followed.
Step 1: Scoping Search and Search Strategy
The inclusion criteria were developed systematically to ensure that relevant and recent literature was included. The inclusion criteria were literature that was relevant to the cultural competence of undergraduate nursing students, written in English, available in full text, and published between 2014 and 2023. The exclusion criteria were literature that was older than 10 years (i.e., published before 2014), gray literature (e.g., research reports), and that which did not address cultural competence strategies for undergraduate nursing students’ education. Databases for the search process included EBSCOhost, Scopus, Google Scholar, and University X Libguides which included CINAHL and PubMed databases. A librarian at the university was consulted to assist in the initial search process and enhance the credibility of the process. The search string included a combination of keywords: (cultural competence AND nursing students or student nurses AND strategies or measures AND enhance or improve AND nursing education institutions). The use of Boolean operators and a librarian ensured that the most appropriate literature was included (Lubbe et al., 2020). Initial searches yielded a vast number of results (e.g., 22,000 at one stage) and limiters in the form of inclusion criteria were then applied. The final comprehensive search yielded (N = 122) results which were then considered in the subsequent steps of the ILR process. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) framework (Page et al., 2020) was used to report the outcome of the literature search and selection processes. The PRISMA flow diagram depicted in Figure 1 ensures adequate reporting and transparency and further ensures credibility of the study.
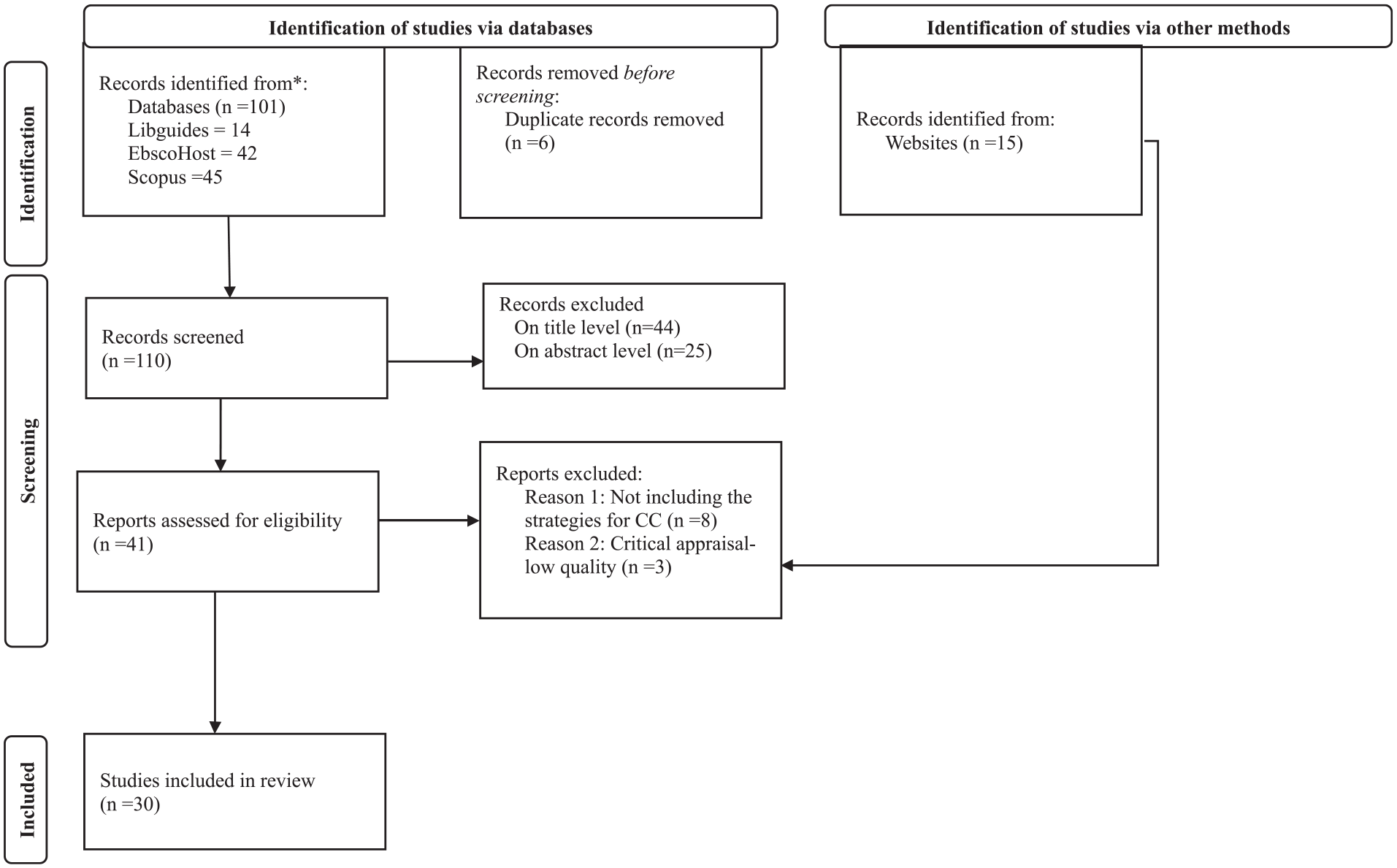
PRISMA 2020 Flow Diagram (Page et al., 2020).
Step 2: Screening
A manual process to screen and record the literature was conducted. Porritt et al. (2014) support two-reviewer or group review to ensure transparency and reproducibility of the literature review. The PRISMA flow diagram depicted above (Figure 1) assisted the authors to systematically identify literature, screen and determine a final number of papers to be included. Initial screening was completed by two authors (V.N. and L.C.), while K.D.S. reviewed papers that the first two authors had not reached consensus on for inclusion. A consensus meeting with all authors was held, in which the papers to be included and excluded, based on the inclusion and exclusion criteria, were agreed upon. During the initial screening step, duplicates were excluded (n = 6) and a total of (n = 44) papers were excluded during title screening, with (n = 25) being excluded during abstract screening. A further (n = 8) papers were excluded as they were not relevant to strategies to enhance cultural competence, and (n = 3) were excluded due to low quality during critical appraisal. No paper was excluded as being written in a language other than English. Following this strategy, a total of 30 papers (N = 30) were included for data extraction and analysis.
Data Collection
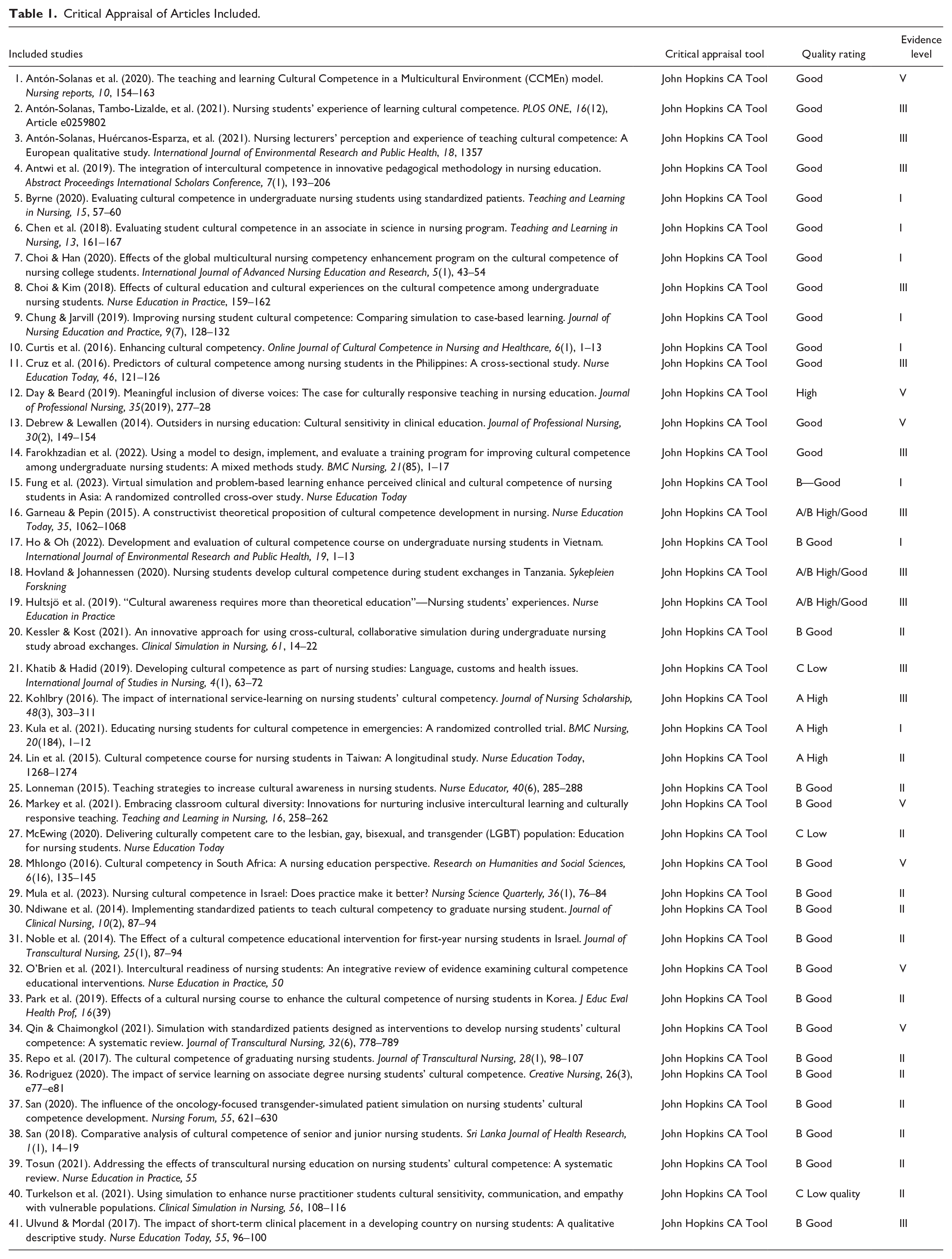
Appraising the studies to be included in a review is important to evaluate the quality and credibility of the included literature (Porritt et al., 2014). The methodological quality of the studies was reviewed by all authors, with each paper being discussed for consensus on whether to be included or not, while being guided by the set criteria. The John Hopkins Evidence-based Appraisal Tool (Dang et al., 2022) was chosen by the authors due to its rigorous quality criteria and process, thereby reducing the likelihood of bias on the part of the authors. A total number of (n = 41) papers were initially included for the critical appraisal process. From that sample, seven (n = 7) were of high quality, 31 (n = 31) were of good quality, and three (n = 3) were of low quality. Low-quality studies were excluded, and eight (n = 8) were excluded due to not focusing on cultural competence strategies. The authors reached a consensus to include 30 (n = 30) papers. Table 1 outlines the studies reviewed with their respective quality ratings.
Critical Appraisal of Articles Included.
Data Analysis
Data Extraction
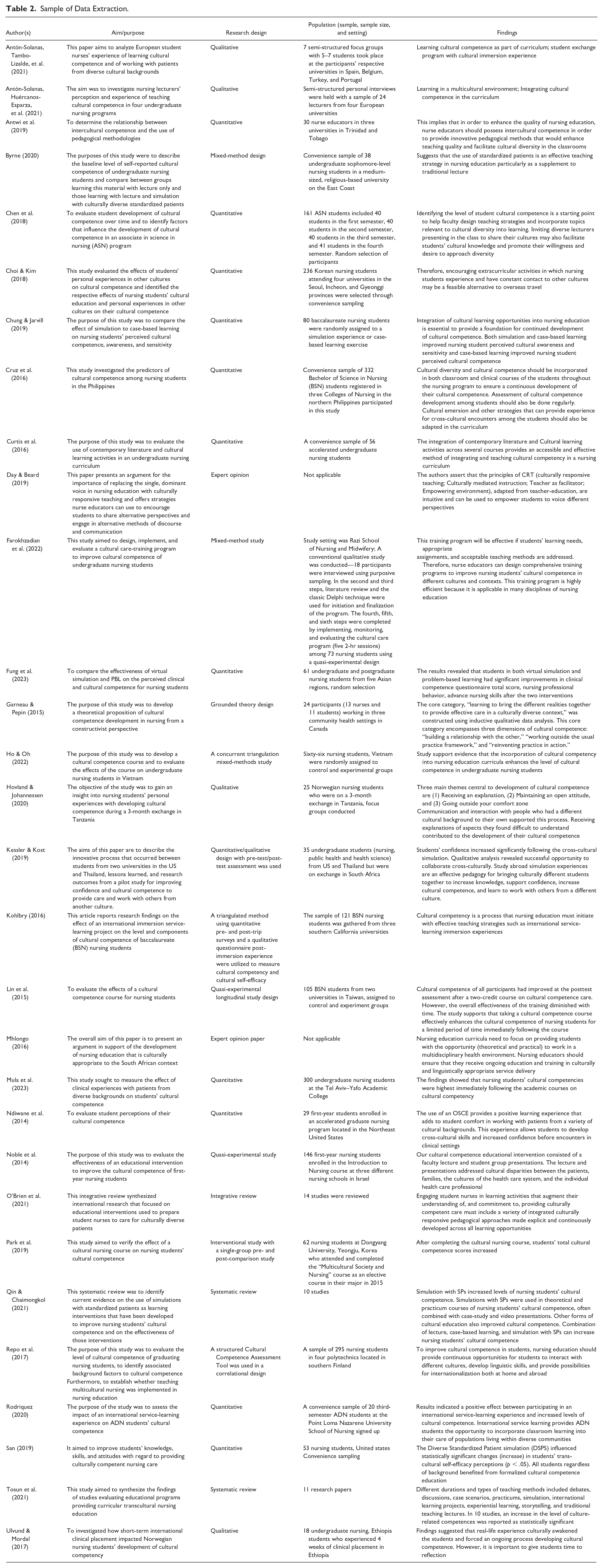
A standardized tool was used to extract data. Lubbe et al. (2020) argue that to allow for data analysis, the final list of selected documents must be read thoroughly, following which the purpose, design, population, and findings must be summarized with a data extraction tool. This process was undertaken by all authors with a focus on answering the research question (see Table 2). The authors decided to use the tested data extraction forms to ensure that relevant data is extracted; this process assisted the authors to minimize bias and other research errors (Munn et al., 2014).
Sample of Data Extraction.
Data Synthesis and Thematic Analysis
Data synthesis and thematic analysis followed the extraction phase. Data synthesis was conducted concurrently with thematic analysis whereby patterns within the data were analyzed and reported (Braun & Clarke, 2006). The authors applied the six steps of thematic analysis by Braun and Clarke (2006) which included familiarizing themselves with the extracted data; generating initial codes; searching for themes; reviewing themes; defining and naming themes; and finally, writing up the report. This process was followed until the data in Table 3 were formulated. The systematic process followed allowed the authors to reach consensus on the themes reported.
Thematic Synthesis Table to Summarize New Constructs Derived From Good Quality Documents.

Findings
Thirty (n = 30) papers were included in the review process. Of these, nine (n = 9) were non-experimental quantitative studies, six (n = 6) quantitative experimental and intervention studies, five (n = 5) qualitative studies, five (n = 5) mixed-method studies, three (n = 3) review studies, and two (n = 2) expert opinion papers. The empirical research papers included reported on the findings of studies conducted in the United States of America (n = 9), Korea (n = 3), and Israel (n = 2). The following countries had one paper each: Ethiopia, Taiwan, Finland, Norway, Vietnam, Canada, Iran, Philippines, and Trinidad and Tobago. There were four multi-country studies with participants from Spain, Belgium, Turkey, and Portugal (n = 2), Hong Kong, Mainland China, Thailand, Korea, and Taiwan (n = 1), and the United States of America and Thailand (n = 1).
Thematic analysis of the extracted data revealed five strategies to enhance the cultural competence of undergraduate nursing students at NEIs, which are reported in the following sections.
Strategy 1—Integrating Cultural Competence Into the Undergraduate Nursing Curriculum
Integrating cultural competency into the undergraduate nursing curricula, as supported in 12 papers (Antón-Solanas, Huércanos-Esparza, et al., 2021; Antón-Solanas, Tambo-Lizalde, et al., 2021; Chen et al., 2018; Chung & Jarvill, 2019; Cruz et al., 2016; Curtis et al., 2016; Ho & Oh, 2022; Lin et al., 2015; Mula et al., 2023; Noble et al., 2014; Park et al., 2019; San, 2019), covers a variety of curricula-related interventions to enhance the cultural competence of students. This includes designing teaching strategies that enhance cultural competencies, and incorporating topics related to cultural diversity into subject content and their activities (Chen et al., 2018). Educational interventions to enhance cultural competency were reported to include faculty and student group presentations (Noble et al., 2014), and the use of contemporary literature on cultural competency (Curtis et al., 2016). However, Cruz et al. (2016) indicated that for this to be effective, cultural competence should be incorporated in both clinical training and theory courses. San (2019) highlighted that nursing students benefit from formalized cultural competence education. Formalization can be achieved by the design and implementation of culturally competent care courses for nursing students (Lin et al., 2015; Mula et al., 2023; Park et al., 2019).
Strategy 2—Cultural Immersion
To enhance cultural competence in undergraduate nursing students, as identified in 12 papers (Antón-Solanas, Huércanos-Esparza, et al., 2021; Antón-Solanas, Tambo-Lizalde, et al., 2021; Antwi et al., 2019; Choi & Kim, 2018; Cruz et al., 2016; Hovland & Johannessen, 2020; Kessler & Kost, 2021; Kohlbry, 2016; Mhlongo, 2016; Repo et al., 2017; Rodriguez, 2020; Ulvund & Mordal, 2017), culturally immersive experiences should be provided. Cultural immersion is important as it provides students with exposure to different patient backgrounds and encourages learning to take place in consideration of cultural diversity. Cultural immersion reported in the included papers provided learning in multicultural environments (Antón-Solanas, Tambo-Lizalde, et al., 2021; Mhlongo, 2016), allowing for cross-cultural encounters for both theoretical and practical learning (Cruz et al., 2016), and communication and interaction between students and culturally diverse individuals (Hovland & Johannessen, 2020). Interactions with different cultures help students to develop their basic linguistic skills (Repo et al., 2017) and provide an opportunity for ongoing training and education in culturally appropriate health care delivery (Mhlongo, 2016).
Furthermore, the reviewed studies reported cultural immersion through student exchange programs which included studying abroad or international placements for a specified period of time (Antón-Solanas, Tambo-Lizalde, et al., 2021; Kessler & Kost, 2021; Kohlbry, 2016; Repo et al., 2017; Rodriguez, 2020). Some student exchange programs incorporated simulation experiences with culturally diverse students to promote collaborative learning (Kessler & Kost, 2021) and international service learning (Kohlbry, 2016; Rodriguez, 2020). Other culturally immersive experiences reported were the facilitation of cultural diversity in the classroom (Antwi et al., 2019) and extracurricular activities with an option to have constant contact with other cultures (Choi & Kim, 2018).
Strategy 3—Innovative Pedagogical Approaches
The reviewed studies reported innovative pedagogical approaches used to enhance cultural competency in undergraduate nursing students (Antwi et al., 2019; Byrne, 2020; Chung & Jarvill, 2019; Day & Beard, 2019; Farokhzadian et al., 2022; Fung et al., 2023; Garneau & Pepin, 2015; Kessler & Kost, 2021; Ndiwane et al., 2014; Noble et al., 2014; O’Brien et al., 2021; Qin & Chaimongkol, 2021; San, 2019; Ulvund & Mordal, 2017). Simulation as a pedagogical approach was reported by Chung and Jarvill (2019), Fung et al. (2023), Kessler and Kost (2021), Qin and Chaimongkol (2021), and San (2019). Simulation was conducted in face-to-face encounters and virtually. In some cases, simulation was conducted together with other approaches such as case-based study and problem-based solving to enhance its effectiveness and impact on student learning. Qin and Chaimongkol (2021) reported that simulation with standardized patients in theoretical and practical courses increased student cultural competence. While standardized patients may be from similar backgrounds to students, diverse standardized patients provide positive outcomes when embedded in formalized cultural competence education (San, 2019). Standardized patients were used in some educational contexts as a supplement to traditional teaching (Byrne, 2020). For an improved cultural competency learning experience, detailed preparation and immediate feedback after simulation encounters should be provided (Ndiwane et al., 2014).
In addition, comprehensive training programs were followed to improve nursing students’ cultural competency (Farokhzadian et al., 2022), with opportunities to engage students in learning activities that promote critical thinking and opportunities to reflect. Some included objective structured clinical examinations (OSCE) in students’ cultural learning experiences to provide opportunity to practice asking culturally appropriate questions (Ndiwane et al., 2014). This increased student confidence and facilitated the development of cross-cultural skills in preparation for encounters with real patients. In some contexts, examples and case studies were used to illustrate the theory of cultural competence (Antón-Solanas, Huércanos-Esparza, et al., 2021). A grounded theory study reported that students became culturally competent through building relationships with others, working outside the usual practice context, and reinventing practice in action (Garneau & Pepin, 2015). In some contexts, educators considered culturally responsive teaching to consist of elements such as culturally mediated instructions and an empowering environment (Day & Beard, 2019).
Strategy 4—Role of Nurse Educators
Six studies provided evidence that nurse educators (NEs) play a role in enhancing the cultural competency of nursing students (Antwi et al., 2019; Chen et al., 2018; Day & Beard, 2019; Farokhzadian et al., 2022; Mhlongo, 2016; Tosun et al., 2021). The NE is a facilitator of cultural competence education and has a mandate to design comprehensive training programs that are responsive to student learning needs, with appropriate learning activities and acceptable teaching techniques (Farokhzadian et al., 2022). Training programs can be of different duration and make use of different types of teaching techniques to increase cultural competence (Tosun et al., 2021). The variety of teaching techniques reported included storytelling, case discussions, simulations, practicum, traditional lecture method, case scenarios, discussions, debate, international learning projects, and experiential learning experiences. To facilitate innovative pedagogical approaches, NEs should possess intercultural competence (Antwi et al., 2019). Thus, they should be able to facilitate cultural diversity through quality classroom teachings. NEs have a role to invite diverse lecturers to provide classroom presentations on their own culture; this practice increases students’ cultural knowledge and, in a way, facilitates their desire and willingness to work with diverse individuals (Chen et al., 2018).
Moreover, to fulfill their roles in facilitating cultural competence, the review indicated that NEs need to practice cultural awareness. This can be done by appreciating that they are cultural beings themselves (Mhlongo, 2016). Mhlongo (2016) further reported that NEs should apply the theory and principles of cultural competency during their daily practice, and not only in the process of teaching. Consequently, NEs have a responsibility to make sure they obtain necessary continuous training and education for culturally and linguistically appropriate service delivery.
Strategy 5—Students’ Assessment
The findings of the reviewed studies demonstrate that the assessment of students has a role in enhancing cultural competence (Chen et al., 2018; Cruz et al., 2016; Ndiwane et al., 2014). Findings from Chen et al. (2018) indicated that for NEs to design relevant topics and teaching pedagogies relevant for cultural diversity in learning, identifying the levels of cultural competence in students should be the starting point. In addition, assessing students via OSCE with standardized patients provides feedback on professionalism, communication skills, history taking, and closure of interviews (Ndiwane et al., 2014). Cruz et al. (2016) recommended regular assessment of students for the monitoring and evaluation of their cultural competence development.
Discussion
The objective of this ILR was achieved as the strategies that can be used to enhance the cultural competence of undergraduate nursing students at NEIs were outlined. Five themes emerged as strategies to enhance cultural competence: integrating cultural competence into the undergraduate nursing curriculum, cultural immersion, innovative pedagogical approaches, the role of nurse educators, and students’ assessment.
The first strategy, integrating cultural competence into the undergraduate nursing curriculum, included integration at the curriculum design level by designing stand-alone cultural competence courses, or by incorporating different cultural competence learning activities into existing classroom and clinical teaching programs. To prepare nursing students to be culturally competent practitioners, the nursing curriculum must be inclusive of activities that enhance culturally competent care of diverse populations (James & Al-Kofahy, 2021).
The second strategy, cultural immersion, focused on exposing students to or integrating their learning activities with diverse or multicultural contexts. According to Granel et al. (2021), cultural competence is developed as an outcome of both national/local and international experiences. International student exchange programs allow students to experience a new culture and develop competencies in terms of interaction skills, confidence, discovering new potentials, and increasing their understanding of global perspectives of nursing (Aldén-Joyce et al., 2023).
Some international and local culturally immersive experiences for nursing students incorporated service-learning. Due to students’ immersion in the community context through the provision of services, this approach enhances the students’ cultural competence (De Leon, 2014; Emrani et al., 2024). Wall-Basset et al. (2018) using Campinha-Bacote’s model confirmed that the use of reflective journals, service-learning projects, site exposures, and participating together during an international service learning helped deepen and progress the cultural competence process for students. Moreover, students develop cultural competence by gaining knowledge and skills to work with diverse patients. This sets the stage for developing an understanding of cultural diversities, practicing ethical decision-making, developing problem-solving and critical thinking skills, and acquiring self-efficacy in new environments (Rodriguez, 2020).
Placement in multicultural contexts is, however, associated with challenges related to language barriers, a lack of awareness of cultural practices, differing values, norms, and cultural expectations of patients, and resistance to health care interventions (Nuuyoma et al., 2024). This review demonstrates that these placements enhance cultural competence due to communication and interaction with different cultural backgrounds, thereby facilitating the development of linguistic skills and understanding of diverse cultural practices.
The third strategy, innovative pedagogical approaches, was supported by the majority (n = 14) of the papers reviewed. This strategy focuses on using teaching methods or techniques that accommodate students with a variety of learning styles, and the active involvement of students, to enhance cultural competence. Simulation as an innovative pedagogical approach in reviewed studies was conducted either in face-to-face encounters or virtually. In nursing education, simulation as a pedagogic tool allows for the application of knowledge and the advancement of clinical and critical thinking skills (Qin & Chaimongkol, 2021). When conducted virtually, NEs facilitating simulation sessions should make sure activities are appropriate for learners’ levels, and the sequencing of cases should be appropriate to facilitate the building and scaffolding of knowledge (Verkuyl & Atack, 2024). The findings of our review indicate that simulation is, in some cases, conducted together with other approaches such as case-based study, use of examples, and problem-based solving to enhance its effectiveness and impact on student learning.
NEs are encouraged to use culturally responsive teaching (CRT) as part of innovative pedagogical approaches (Day & Beard, 2019; O’Brien et al., 2021). CRT is an umbrella concept for pedagogies that prepare students to support social justice in and beyond the classroom (Day & Beard, 2019). CRT may be implemented with the guidance of three principles: culturally mediated instruction, teacher as a facilitator, and creating an empowering environment. While caring for diverse patients, students learn cultural competence by bringing different realities together to provide effective care, working outside the prescribed practice framework, and building relationships with others, especially people from diverse cultures (Garneau & Pepin, 2015). Irrespective of the CRT principle and method followed, it should be explicit, regularly updated, and integrated into all available learning opportunities (O’Brien et al., 2021). In addition, students should be allowed time to reflect on learning experiences to promote developing cultural competence (Ulvund & Mordal, 2017).
The fourth strategy, the role of nurse educators (NEs), focused on the actions and mandate of NEs in enhancing the cultural competence of nursing students. This review reveals that NEs should possess intercultural competence. Rahimi et al. (2023), in agreement, state that to prepare culturally competent nursing students for clinical practice, NEs themselves should be culturally competent. Therefore, NEs should receive ongoing training and education in culturally and linguistically appropriate health care service delivery (Mhlongo, 2016). This may be conducted via short courses or formal postgraduate training courses.
The current ILR further revealed that NEs should practice cultural awareness. Literature emphasized the practice of cultural awareness and cultural desire as extensively contributing to the development of cultural competence in NEs (Majnoon et al., 2023). One of the roles of NEs in enhancing the cultural competence of undergraduate nursing students is acting as a facilitator.
The fifth strategy, students’ assessment, focused on how assessment may be used to enhance cultural competency in undergraduate nursing students. Through assessment, NEs can make informed decisions about a student’s level of competence and help to bridge the gap between theory and practice (Donough, 2022). Assessment is not only for monitoring and evaluation of student progress but also to guide NEs in designing appropriate teaching pedagogies and topics for cultural diversity that are responsive to identified needs (Chen et al., 2018). Moreover, this review reveals that there should be continuous assessment for students to develop cultural competence. This is relevant because cultural competence is not stagnant; rather, it is a process that can be affected by cultural context, social, historical, and political aspects, and even individuals’ immediate financial situation (Sharifi et al., 2019). NEs should use a variety of assessment methods; however, an OSCE with standardized patients is preferred as it allows feedback on aspects such as professionalism, communication skills, and generally how history taking and closure of interviews are done (Ndiwane et al., 2014).
Implications, Strengths, and Limitations
This study’s findings have implications for nursing education and practice. The strategies identified can be used by different nursing education stakeholders to promote cultural competency education in curriculum design, implementation, and evaluation phases. The stakeholders in this context refer to educators in NEIs as well as nurse practitioners in clinical settings. Moreover, these strategies may be used to inform the development of local frameworks and guidelines to enhance the cultural competency of undergraduate nursing students. Future researchers may consider assessing the cultural competency levels of undergraduate nursing students from developing or middle-to-low-income countries and interventions to promote cultural competence in these contexts.
A strength of this ILR is the diverse quality and evidence levels of the literature reviewed. However, empirical studies were conducted outside the African continent, except for one from Ethiopia. This is considered a limitation as cultural competence tends to be influenced by political, social, historical, cultural, and financial situations.
Conclusion
The objective of this ILR was to understand and outline strategies that can be used to enhance the cultural competence of undergraduate nursing students at NEIs. Most of the reviewed literature supported the use of innovative pedagogical approaches, the integration of cultural competence training in the undergraduate nursing curriculum, and cultural immersion of students. These strategies are foundational to enhancing cultural competence and should be supported by NEIs to ensure that appropriate pedagogy and teaching strategies are designed. The role of nurse educators is critical in the process of enhancing nursing students’ cultural competence as they are facilitators of this process. These strategies thus provide nurse educators with evidence-based information to incorporate in nursing curricula. It is recommended that nurse educators be capacitated with cultural competence skills as only then will they be able to facilitate this process for students, which should start with the development of innovative curricula focused on cultural competence.
Footnotes
Acknowledgements
The authors acknowledge their respective universities for Open Access publishing.
Author Contributions
All authors contributed to the manuscript to merit authorship. The submitted manuscript is approved by all authors. KDS, VN, and LC conceived and planned the review. KDS, VN, and LC collected and analyzed the data. KDS, VN, and LC interpreted the data. KDS, VN, and LC drafted and revised the manuscript. KDS and VN took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Data Availability
All analyzed data supporting the findings of this research are included in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views and opinions expressed in this manuscript are those of the authors and they do not necessarily reflect the official policy or position of any affiliated agency of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.