
Abstract
Introduction:
This study aimed to determine the relationship between ablution ritual and foot knowledge, self-care behaviors, and the presence of diabetic foot ulcers in Muslims with type 2 diabetes mellitus (T2DM).
Methodology:
A descriptive, comparative method was utilized to identify ablution ritual and foot knowledge, self-care behaviors, and the presence of diabetic foot ulcers.
Results:
There were 228 persons with T2DM, with 162 participants (71.1%) in the ablution group and 66 participants (28.9%) in the no-ablution group, with 19.7% having diabetic foot ulcers. Diabetic foot knowledge and foot self-care behaviors of persons with T2DM were below a medium level, and there was a significant difference between ablution behavior and the presence of diabetic foot ulcers (x2 =6.646, p<.05).
Discussion:
Culturally congruent interventions that acknowledge and understand the cultural practices and beliefs of Muslims with T2DM may be recommended to enhance their knowledge levels and promote positive behavior changes.
Introduction
Type 2 diabetes mellitus (T2DM) is a significant health problem that has reached worrisome levels. Today, there are 537 million people in the world living with diabetes. The prevalence of diabetes is on the rise worldwide, and projections indicate that the number of people living with diabetes will reach 643 million by 2030 (International Diabetes Federation [IDF], 2021). This increase is expected to be particularly significant in countries with Muslim-majority populations. According to estimates, the global Muslim population affected by diabetes is around 148 million individuals (Jabbar, 2016; Shaikh et al., 2020). The prevalence of diabetic foot in the predominantly Muslim countries of the Middle East and North Africa region ranges from 5.0% to 20.0% (Monteiro-Soares & Santos, 2022; Samad Omar et al., 2023). The recurrence prevalence of diabetic foot ulcers in our country is 43.0% (Monteiro-Soares & Santos, 2022).
More than 95% of people with DM have T2DM. Among the complications of T2DM are cardiovascular diseases, nephropathy, retinopathy, neuropathy, and amputation of the lower extremities (IDF, 2021). Diabetic foot ulcers are accepted as one of the most avoidable complications of T2DM. These are correlated with risk factors, insufficient information, and lack of compliance with treatment. Understanding the levels of knowledge and practice in persons with T2DM is necessary to bring the potential complications of T2DM under control (Bekele & Berhanu, 2021; Pourkazemi et al., 2020).
Cultural and religious beliefs affect an individual’s attitudes to their health and illness and their health practices, behaviors, and thoughts. Islam is accepted by many Muslims as a “lifestyle” which provides a social system for living and regulates such topics as family life, law and order, morals, dress, and cleanliness through religious ritual and observance. For many Muslims, Islamic practice governs every aspect of their lives and behavior. It is also known that Islamic values and practices affect the daily activities of persons with DM (Attum et al., 2021; Heidari et al., 2017; Permana et al., 2019; Yazla et al., 2018).
Islamic Principles
It is known that independent of where they live in the world, Muslims share Islamic principles. Among these Islamic principles is that of praying five times a day and performing ritual ablution (washing the face, hands, and feet) before prayer (Attum et al., 2021). When performing ablution, the feet are washed three times up to the ankles, and care is taken to wash between the toes (Shankhdhar, 2021).
Washing the feet every day is among the important behaviors recommended for foot health in persons with T2DM. Among the recommended behaviors is that after washing the feet, the gaps between the toes should be thoroughly dried (Howarth, 2019). A foot-washing behavior which is important in ensuring foot hygiene; thorough drying between the toes, if it is not done properly, can lead to a tendency to foot infection (Manickum et al., 2021).
The purpose of this study was to determine the relationship between ablution ritual and foot knowledge, self-care behaviors, and the presence of diabetic foot ulcers in Muslims with T2DM. The research questions were:
Methodology
Study Design
This is a quantitative research design. A descriptive, comparative method was utilized to identify ablution (washing) ritual and foot knowledge, self-care behaviors, and presence of diabetic foot ulcers.
Setting
The study was conducted in the internal medicine and endocrine clinics of a teaching and research hospital in the east of Turkey. The data were collected by the researchers through face-to-face interviews between March and August 2022.
Participants
Inclusion criteria for the study were 18 years of age or older, agreeing to participate in the research, having a diagnosis of T2DM, not having any visual or auditory problems, being able to communicate, and filling in the questionnaire form completely. Not included were patients with a visual or auditory problem, those with a recent diagnosis (≤1 month), those with a history of amputation, those who did not agree to participate in the research, and those who left gaps when filling out the questionnaire form. Data collection was performed between March and August 2022.
Data Sources/Measurement
The questionnaire form consisted of three sections: a patient information form, the Diabetes Foot Knowledge Questionnaire (DFKQ), and the Foot Self-Care Observation Guide (FSOG). The first section was prepared by the researcher according to the literature and consisted of 24 questions on the participants’ sociodemographic and disease-related characteristics and a dermatological assessment of their feet (Indrayana et al., 2019; Johnson et al., 2018; Pourkazemi et al., 2020). The DFKQ had five items and the FSOG 15, so that the total number of questions on the questionnaire was 44. The questionnaire took approximately 10–15 min to answer.
Diabetes Foot Knowledge Questionnaire (DFKQ)
The DFKQ was developed in 2001 by Garcia et al. to measure knowledge on the foot care of persons with DM (Garcia et al., 2001). The questions on the scale are answered with “yes,” “no,” or “I don’t know.” The scale is assessed on the total score. The lowest possible score on this five-item scale is 0, and the highest is 5. A higher score indicates a higher level of knowledge. The validity and reliability of the scale for Turkish society were tested in 2011 by Biçer and Enç. The Cronbach α value of the scale of 0.58 was found (Kır Biçer & Enç, 2011). In the present study, the Cronbach α value was found to be 0.62. Acceptable Cronbach α values range from 0.60 to 0.95. If the number of items in a scale is low, lower values of Cronbach’s α may be considered acceptable (Kır Biçer & Enç, 2011; Taber, 2018).
Foot Self-Care Observation Guide (FSOG)
The FSOG original scale was developed by Borges and Ostwald in 2008. The scale consisted of 16 items measuring the development of foot self-care behaviors in persons with DM (Borges & Ostwald, 2008). In 2011, Biçer and Enç tested the validity and reliability of a 15-item Turkish scale. The scale is graded in this way: 1 = Never, 2 = Occasionally, 3 = Sometimes, 4 = Frequently, and 5 = Always. The lowest possible score on the scale is 15 and the highest is 75. A high score on the scale indicates good foot care behavior. The Cronbach α value of the scale was reported to be 0.83 (Kır Biçer & Enç, 2011). In the present study, a Cronbach α value of 0.88 was found. The Cronbach’s α value of the scale is within acceptable limits.
Study Size
Because no data on the number of patients in the internal medicine and endocrine clinics of the hospital could be accessed, the size of the research sample was calculated by the unknown population sampling method with the formula n = t2pq/d2, using the rate of 15.9% of the occurrence of T2DM in Turkey according to the International Diabetes Federation 2021 (IDF, 2021) and a sample of 228 persons with T2DM was calculated. Persons with T2DM who agreed to participate in the study were selected from the population by the non-probability sampling method.
Statistical Methods
Assessment of the data obtained in the research was performed using the program package SPSS 28.0 (Statistical Package of Social Sciences, Chicago, IL, USA). Continuous variables were expressed in mean (M), standard deviation (SD), median, minimum (min), maximum (max), and categorical variables in numbers (percentage). Testing for normal distribution was performed with the Kolmogorov–Smirnov test. The Mann–Whitney U test was used to compare variables that did not show a normal distribution between groups. In the comparison of categorical variables, the chi-square test and where necessary Fisher’s exact test were used. In interpreting the results, the level of statistical significance was taken as p < .05.
Ethical Approval
Ethical approval was obtained from the Health Research and Publication Ethics Committee of a university before data collection (Decision no: 2022-02). Informed consent was obtained from all individual participants included in the study. This study was performed in line with the principles of the Declaration of Helsinki.
Results
Distribution of the Participants’ Information
The study revealed that among persons with T2DM, a significant majority (71.1%) regularly engaged in ritual ablution. The ablution group comprised 162 participants, while the no-ablution group consisted of 66 participants. Only a small proportion (11.7%) of these persons consistently dried between their toes. Demographic information provided by the participants indicated that 51.3% were female, 88.2% were married, and 21.5% were literate. Of the participants, 55.3% were working, and 51.7% reported having a good income level, while 56.1% were smokers. The participants had a mean age of 51.09 years (SD = 12.53), and the mean body mass index (BMI) was 27.35 (SD = 3.53). Regarding treatment, 44.7% of the participants were using insulin, and 57.9% demonstrated conformity to their treatment. More than half of the participants did not demonstrate conformity to their diet, did not take regular exercise, and did not go for regular checkups. Furthermore, 75.9% of the participants reported not receiving education on diabetic foot care, 61.4% reported no hospitalization due to T2DM in the past year, and 53.1% indicated having an additional chronic illness. Examining the presence of additional chronic diseases, the study found that 52 of the participants (22.8%) had hypertension, 25 (11.0%) had asthma, 21 (9.2%) had chronic obstructive pulmonary disease, 15 (6.6%) had kidney failure, and six (2.6%) had other chronic diseases. The mean duration of T2DM was 8.74 years (SD = 5.92), and the mean fasting plasma glucose (FPG) level was 148.10 mg/dL (SD = 29.44). 19.7% of the participants reported currently having diabetic foot ulcers.
Ablution Behavior and Sociodemographic/Disease Characteristics
Table 1 shows the ritual ablution behavior of persons with T2DM according to their sociodemographic characteristics. There was no difference in ablution behavior according to age, gender, marital status, smoking, or BMI. A difference was seen in ablution behavior according to income status, with the rate of performing ablution lower in those with a good income status (p < .05) (Table 1). Table 2 shows the ablution behavior of persons with T2DM according to their disease-related characteristics. No difference was seen in ablution behavior according to conformity to treatment, getting education on diabetic foot ulcers, the presence of an additional chronic illness, years of T2DM, or FPG (p > .05). However, there were differences according to the variables of conformity to diet, taking regular exercise, going regularly for checkups, and having been hospitalized for T2DM within the previous year (p < .05). The study found that the behaviors of conformity to diet, taking regular exercise and regularly going for checkups of persons with T2DM who performed ablution were less, while hospitalization for T2DM during the previous year was more (p < .05) (Table 2). Table 3 shows the presence of risk factors for diabetic foot ulcers in persons with T2DM. No statistically significant difference was found between the ablution behavior of persons with T2DM and their risk factors for diabetic foot ulcers (Table 3).
Comparison of Participants’ Ablution Behavior According to Sociodemographic Characteristics.
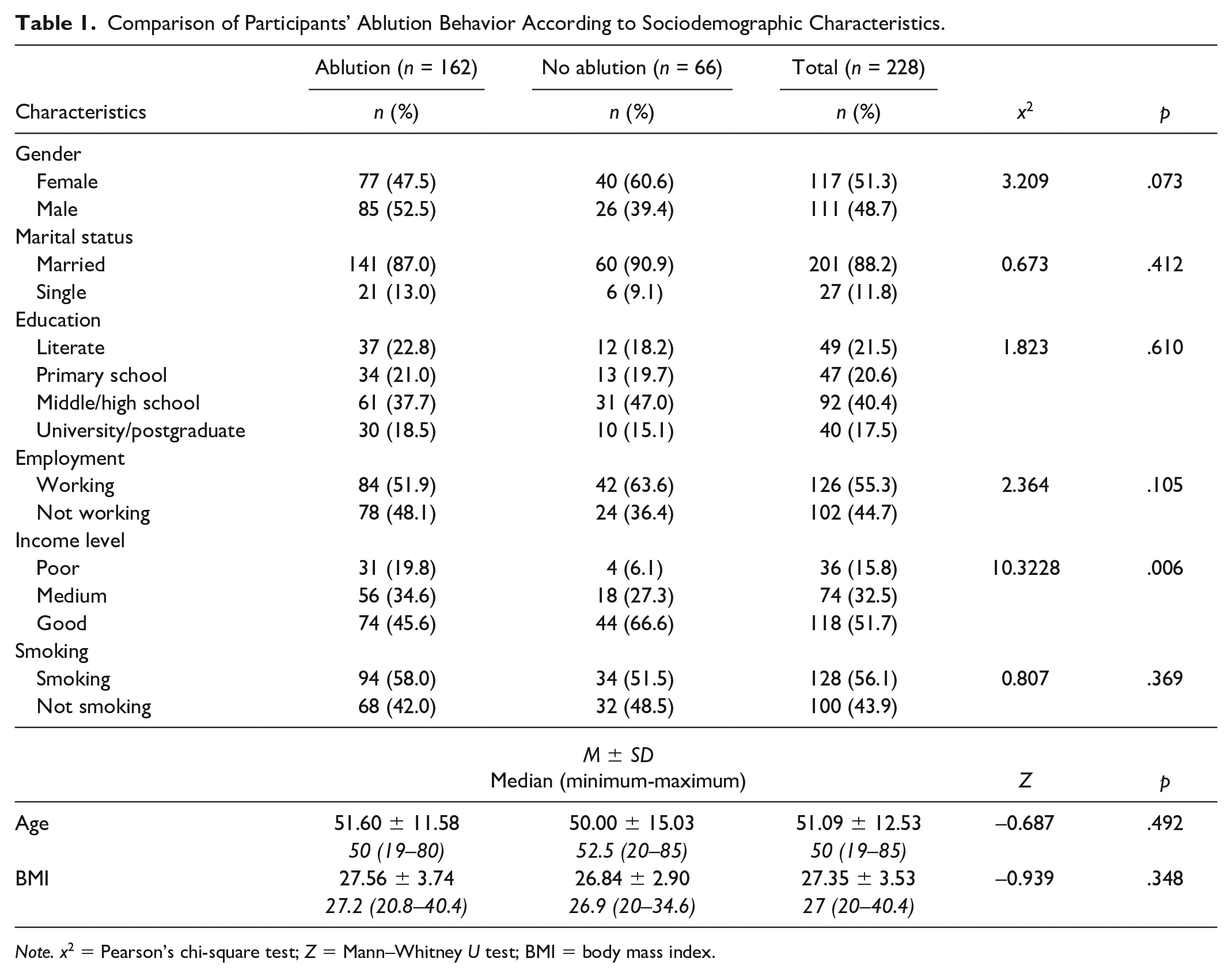
Note. x2 = Pearson’s chi-square test; Z = Mann–Whitney U test; BMI = body mass index.
Comparison of Participants’ Ablution Behavior According to Disease-Related Characteristics.
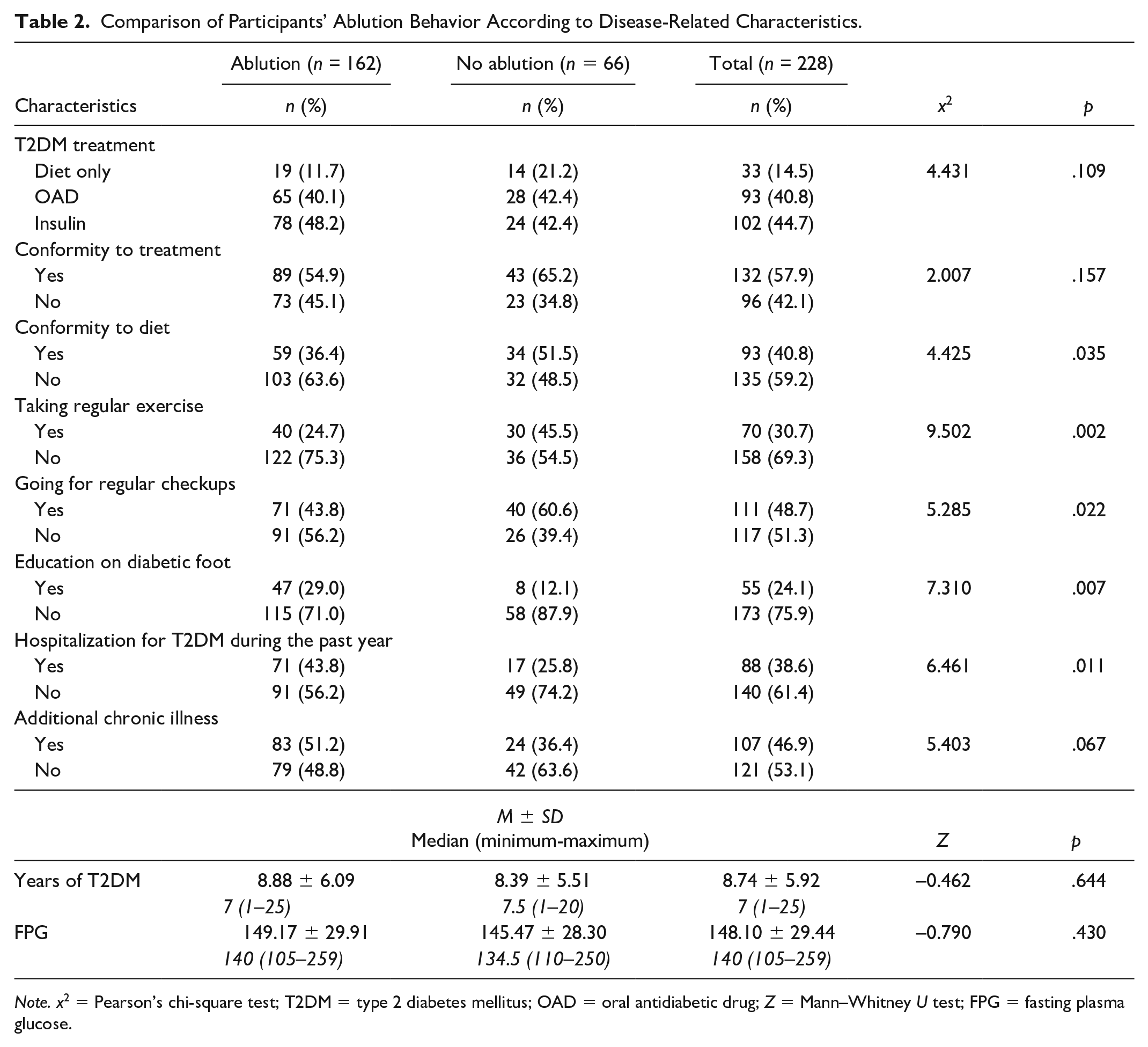
Note. x2 = Pearson’s chi-square test; T2DM = type 2 diabetes mellitus; OAD = oral antidiabetic drug; Z = Mann–Whitney U test; FPG = fasting plasma glucose.
Comparison of Participants’ Ablution Behavior According to the Presence of Risk Factors for Diabetic Foot Ulcers.
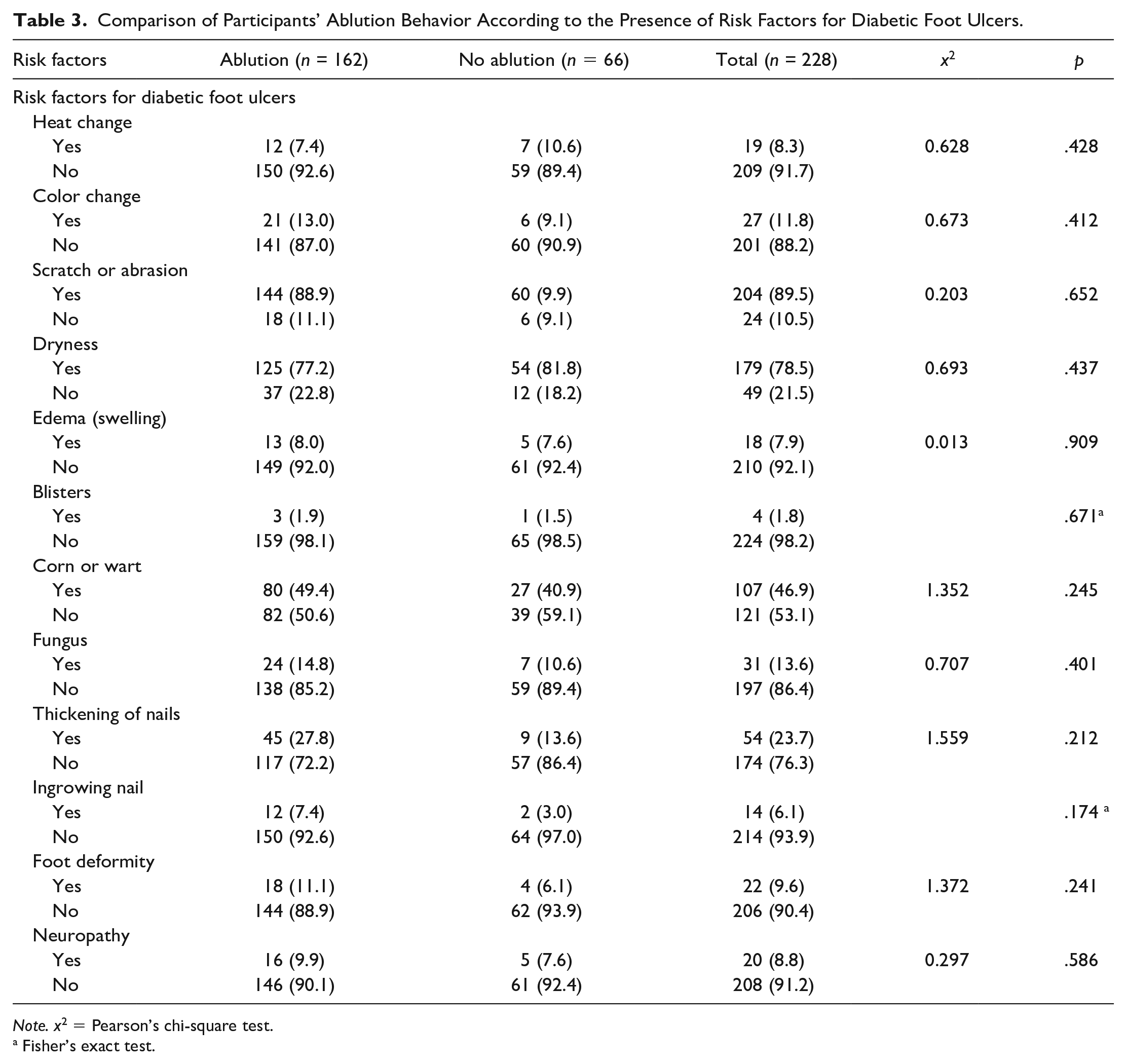
Note. x2 = Pearson’s chi-square test.
Fisher’s exact test.
Ablution Behavior and Foot Knowledge
The participants’ DFKQ scores were found to be M = 1.98, SD = 1.67. However, no statistically significant difference was observed between the DFKQ total score means of the participants and their ablution behavior (p > .05) (Table 4).
Comparison of Participants’ Ablution Behavior According to Their Mean Total DFKQ and FSOG Scores.
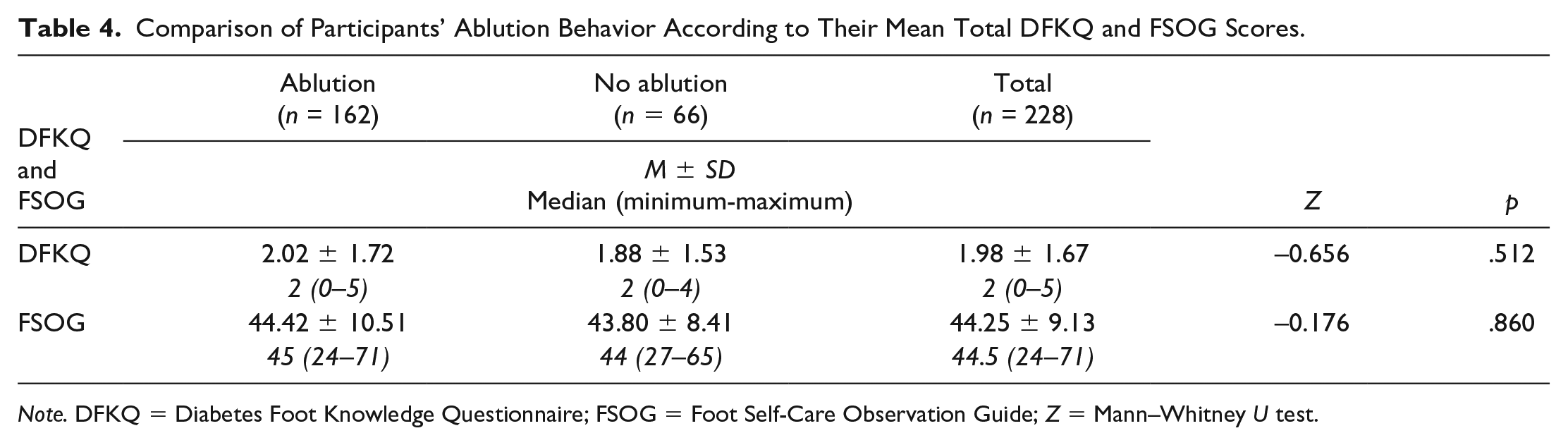
Note. DFKQ = Diabetes Foot Knowledge Questionnaire; FSOG = Foot Self-Care Observation Guide; Z = Mann–Whitney U test.
Ablution Behavior and Foot Self-Care Behaviors
The participants’ FSOG scores were found to be M = 44.25, SD = 9.13. Table 4 shows that there was no statistically significant difference between the FSOG total score means of the participants and their ablution behavior (p < .05) (Table 4).
Ablution Behavior and Diabetic Foot Ulcers
Table 5 shows the analysis of the ablution behavior of persons with T2DM and diabetic foot ulcers. The rate of ablution behavior of the participants was significantly higher in the group with current (x2 = 6.646, p < .05) or past (x2 = 5.311, p < .05) diabetic foot ulcers than those without diabetic foot ulcers (Table 5).
Comparison of Participants’ Ablution Behavior According to the Presence of Diabetic Foot Ulcers.
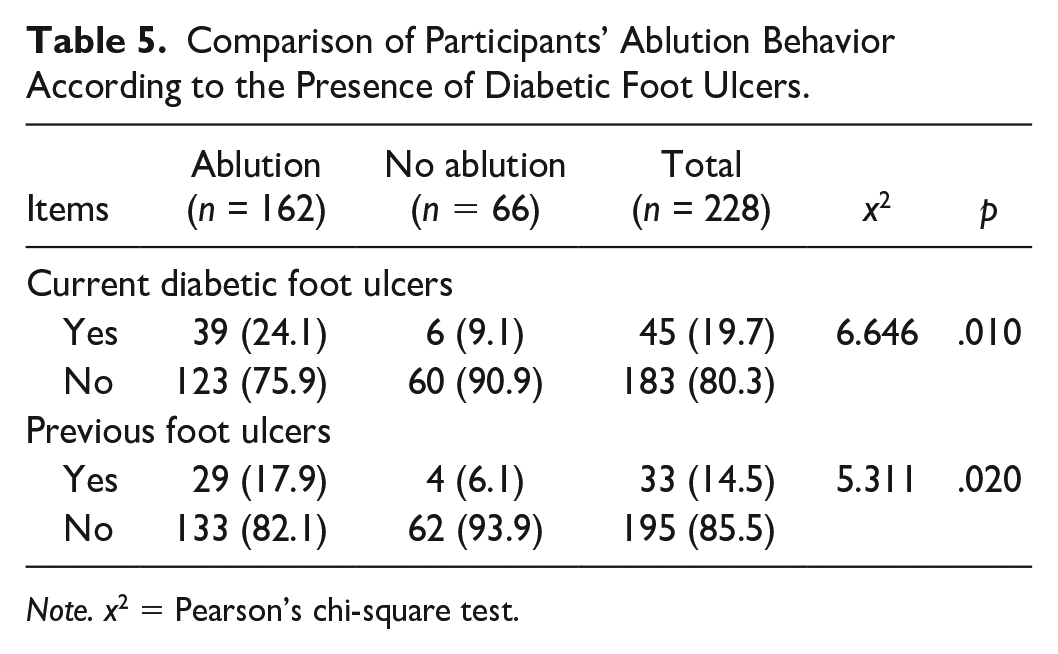
Note. x2 = Pearson’s chi-square test.
Discussion
In a scan of the literature conducted for this study, no study was found focusing on ablution behavior in persons with DM. Therefore, research results evaluating foot care behavior in persons with DM were used in the discussion. Daily washing of the feet of persons with DM is among the important behaviors recommended for foot health (Howarth, 2019). In a study in which many in the sample were Muslim, Indrayana et al. found that the foot care behavior most frequently performed by the participants was washing the feet. The reason was reported to be ablution behavior, which includes washing the feet five times a day before prayer (Indrayana et al., 2019). In the present study, it was found that 71.1% of the persons with T2DM regularly performed ablution; that is, they washed their feet five times a day; however, foot ulcers are reported in 19.7% of the population. The study found that only 11.7% of those persons with T2DM who performed ablution dried the gaps between their toes after every washing. In a study by Azmi et al., it was reported that 93.8% of persons with T2DM washed their feet daily, while 74% dried between their toes (Azmi et al., 2020). The observed differences may be attributed to the sociodemographic factors of the countries or the participants’ status of receiving diabetic foot education. Only 24.1% of the participants in this study reported receiving diabetic foot education.
The behavior common among persons with DM of not drying the feet turns the behavior of foot washing, which is important in maintaining foot hygiene with regard to the formation of diabetic foot ulcers, into a disadvantage. This is because, it is reported, the damp areas between the toes can be a risk factor for fungal infections, which are frequently seen and are the prelude to diabetic foot ulcers (Manickum et al., 2021). Persons with DM are more sensitive to fungal infection. Saud et al. found that the rate of fungal infection in persons with DM was 34%, but 4.7% in those who did not have diabetes (Saud et al., 2020). Some studies have found that the rate of occurrence of maceration or fungus in the feet of persons with DM was between 17.3% and 36.0% (Aronson et al., 2021; Saud et al., 2020; Vural et al., 2018). In the present study, it was found to be 13.6%. For this reason, persons with DM must be told that it is necessary to dry their feet well, including the gaps between the toes, after washing them.
In this study, the participants’ DFKQ scores were found to be M = 1.98, SD = 1.67, and their FSOG scores were M = 44.25, SD = 9.13. Considering the maximum and minimum scores obtainable on those scales, it can be said that the diabetic foot knowledge and self-care behaviors of the persons with T2DM were below the medium level. There are similar results in the literature (Azmi et al., 2020; Bekele & Berhanu, 2021; Gökdeniz & Akgün Şahin, 2022; Pourkazemi et al., 2020; Sulistyo et al., 2018). In one scoping review, 58 studies on determining diabetic foot care knowledge and its implementation in persons with DM, it was reported that there were differences in the levels of foot care knowledge and implementation in persons with DM (Manickum et al., 2021). These results emphasize the need for intervention in foot care in persons with DM.
The results reveal that the presence of diabetic foot ulcers and their presence in the past were statistically significantly higher in those who performed ritual ablution than in those who did not. No statistically significant difference was found between the participants’ ablution behavior and their diabetic foot knowledge and foot care behavior level. Frequent foot washing and not drying the feet thoroughly after each washing including the gaps between the toes may cause problems in persons with DM (Manickum et al., 2021). The skin is an important barrier against infection and is a first line of defense. When the integrity of the skin is endangered, it becomes defenseless against the entry of pathogens from the outside environment and can function as a portal for infection. A person with DM with a disruption of skin integrity may be more sensitive to complications such as diabetic foot ulcers, which threaten the limbs (Johnson et al., 2018). Persons with DM must have knowledge of how to achieve and maintain skin integrity. Suitably conducted foot care and regular daily checking for and early detection of findings such as scratches, abrasions, fungus, or color changes that may occur are important in the prevention of diabetic foot ulcers (Akça Doğan & Enç, 2022). When persons with DM perform ablution, they should dry their feet well and not leave them damp. We know that this knowledge is essential in diabetic foot education, regardless of population. However, it may be important to emphasize in the education of persons with DM who perform ablution.
In addition, conformity to diet, taking regular exercise and having regular checkups were less in persons with DM who performed ablution, and this may encourage the development of diabetic foot ulcers. The reason for this difference in behavior between the groups who perform ablution and those who do not should be investigated. In this study, the sociodemographic characteristics of the two groups were found to be similar, and the only difference which was found was in the variable of income level: this was that the income level of those who did not perform ablution was higher. It is known that economic level on a national and individual basis has a direct effect on the protection of health and access to health services (Oguzhan et al., 2020). It may be thought that income level affects such things as nutrition, exercise, and access to health services. Therefore, when health professionals are educating individuals with low-income levels, they should devote sufficient time to topics such as cost-effective opportunities for nutrition and exercise and free access to health facilities.
Limitations
The HbA1c of participants was not established, which may be a limitation of the study. The potential introduction of bias due to the use of a non-probability sampling method in participant selection is a limitation of this study. In addition, the limited sample size taken from a single city within a specific country could affect the generalizability or external validity of the study. To enhance generalizability and external validity, it would be beneficial to replicate the study with a larger and more diverse sample group, encompassing participants from different regions and cultural backgrounds.
Conclusions
The results reveal that the diabetic foot knowledge and self-care behaviors of persons with T2DM were below a medium level. The rate of ablution behavior of the participants was significantly higher in the group with diabetic foot ulcers than those without diabetic foot ulcers. Acknowledging and understanding the cultural practices and beliefs of individuals is crucial for health care providers to deliver care that respects and accommodates their cultural identities. Discussing the potential relationship between Islamic ritual ablution and foot care practices can provide insights into the cultural factors that may influence health-related behaviors, contributing to the development of culturally appropriate interventions and strategies. In these interventions, the risk posed by belief-based practices such as ablution and the measures that can be taken should be emphasized.
Health professionals should know that practices based on culture or religion can affect the health of individuals. For this reason, these practices should be considered when planning education for persons with DM and providing counseling. If such practices pose a risk, behaviors to preserve health by reducing this risk should be emphasized.
Footnotes
Acknowledgements
The authors are grateful to all patients with diabetes who participated in this study.
Authors’ Contributions
Derya Akça Doğan: Conceptualization, Methodology, Data analysis, Writing—original draft, Writing—Review & Editing; Sevda Efil: Conceptualization, Methodology, Writing—original draft, Writing—Review & Editing; Yasemin Kalkan Uğurlu: Conceptualization, Methodology, Writing—Review & Editing; Gazi Baran Camci: Conceptualization, Methodology, Data collecting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study received ethical approval on 23 February 2022 from the Bursa Uludag University Health Sciences Research and Publication Ethics Committee. Approval Number: 2022/02.
Informed Consent
Informed consent was obtained from all individual participants included in the study. This study was performed in line with the principles of the Declaration of Helsinki.