
Abstract
Introduction:
Despite evidence showing Latinos’ high prevalence of mental health, little is known about Latina migrant farmworkers’ mental health experiences, especially those working in Midwestern states. Considering the multiple vulnerabilities observed among Latina migrant farmworkers, it is necessary to gain insight from own accounts and perceptions of mental health and mental health–seeking experiences
Method:
A qualitative descriptive approach, using in-depth semi-structured interviews with open-ended questions, served to retrieve data from 34 Latina migrant farmworkers. This study was informed by Chicana, postcolonial, and Black feminist epistemologies.
Results:
Thematic analysis identified themes within the data. These findings pertained to the conceptualization of mental health within the contexts of family, capacities, stigma, denial, and faith.
Discussion:
Our results demonstrate the need for health care providers to consider Latina migrant farmworkers’ perceptions about mental health and apply those in designing and implementing culturally informed policy and practice.
Keywords
Introduction
Latina 1 immigrants in the United States access lower mental health services than nonimmigrant women although they have urgent mental health needs (Derr, 2016). For example, Latina women have the highest rates of postpartum depression; however, undocumented status, language and cultural barriers, and chronic financial pressures limit their access to mental health care (Casas et al., 2020; Sampson et al., 2021). While mental illness affects women’s ability to meet their employment and household responsibilities, it may be difficult to diagnose and treat specifically among Latina migrant farmworkers 2 who face poor access to health insurance, high rates of poverty, and, in some cases, cultural and language barriers (National Center for Farmworker Health, 2020).
Latina Migrant Farmworker Mental Health
Latina migrant farmworkers experience significant mental health problems, such as stress, anxiety, and depression (Arcury et al., 2018). Risk factors related to farm work include relocation away from their support systems and exposure to discrimination and alienation (Zapata Roblyer et al., 2016). The lack of a support system among individuals from a culture that values collectivity affects their ability to cope with significant stressors related to farm work, such as sporadic employment, long working hours in hazardous conditions, and high rates of sexual harassment in the farm industry (Chaney & Torres, 2017). In addition, a previous study found that Latina farmworkers associated mental illness and depression with work instability and lack of income (Arcury et al., 2018).
Gender Role, Faith, and Mental Health
The evidence noted the role of cultural practices, beliefs, and language in health care–seeking behaviors and health outcomes (Sampson et al., 2021). For example, Latinas have higher risk factors for depression due to gendered work and related challenges, such as child and elder care, job inequality, economic discrimination, and stress from role conflict between concurrent employment and household responsibilities (Pulgar et al., 2016). In addition, the Latino culture values “marianismo” as a virtue in which women must emulate the Virgin Mary in selflessness, caring, and sacrifice for their family (Sanchez et al., 2018). Latino women may thus avoid seeking mental health care for fear of affecting their children’s well-being or even losing their families (Chan & Corvin, 2016). Furthermore, the Latino culture observes a characteristic of an external locus of control characteristic by which individuals believe that outside forces, such as fate, luck, and divine influences control their life circumstances and outcomes (Timmins & Martin, 2019). In addition, evidence shows that many Latino people profess Christianity as part of their faith values and belief system (Caplan, 2019). From these perspectives, depression, and mental illness become manifestations of sin and religious punishment. Latino immigrants thus depend on their religious beliefs and institutions for support and spiritual counseling to cope with stressors faced in the United States, such as immigration and acculturation (Sanchez et al., 2018).
There is limited literature specifically regarding the mental health needs and the mental well-being of Latina migrant farmworkers. The existing literature includes studies about mental illness; depression screening; use, translation, and validation of diagnostic tools; risks factors; the relationship between migratory status and mental health; and the effectiveness of treatment of mental illness in the Latino community (Arcury et al., 2014; Casas et al., 2020; Cobb et al., 2016; Pulgar et al., 2016). However, an understanding of Latina migrant farmworkers’ perspectives about mental health care needs from a cultural and gender perspective is less frequent.
Method
Theoretical Framework and Positionality
This study was informed by Chicana feminist thought, postcolonial feminist theory, and Black feminist thought (Collins, 2002; Garcia, 1989; Mohanty, 1995). The application of these theories allows for an in-depth analysis of Latina migrant farmworkers’ mental health and how it is affected by the intersection of race, class, and gender amid the current sociopolitical environment and anti-migratory rhetoric (Graf et al., 2022). In addition, the use of a feminist approach promotes a reflective, interactive, and nonhierarchical interaction between researchers and participants who become collaborators and are not merely “subjects” of study (Ritchie et al., 2014).
The authors 3 of this article self-identify as Latina, Black and White scholars from different locations of privilege (middle class, higher education, and heterosexual), and locations of marginalization (immigrants and women of color). Our scholarship informed by feminist theory requires acknowledging our social location as it guides our research design, the methodology of our study, the analysis of data, and our writing.
Design
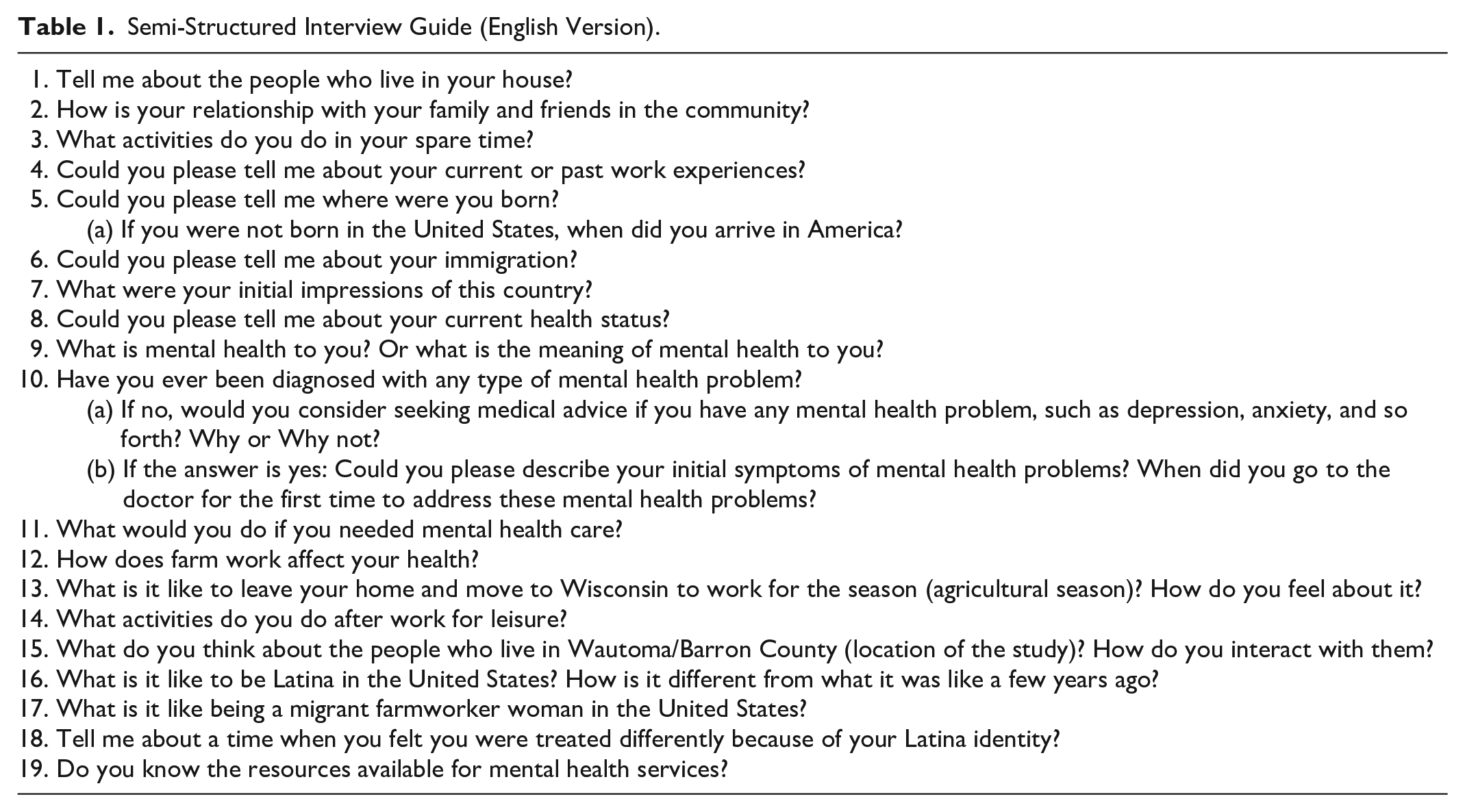
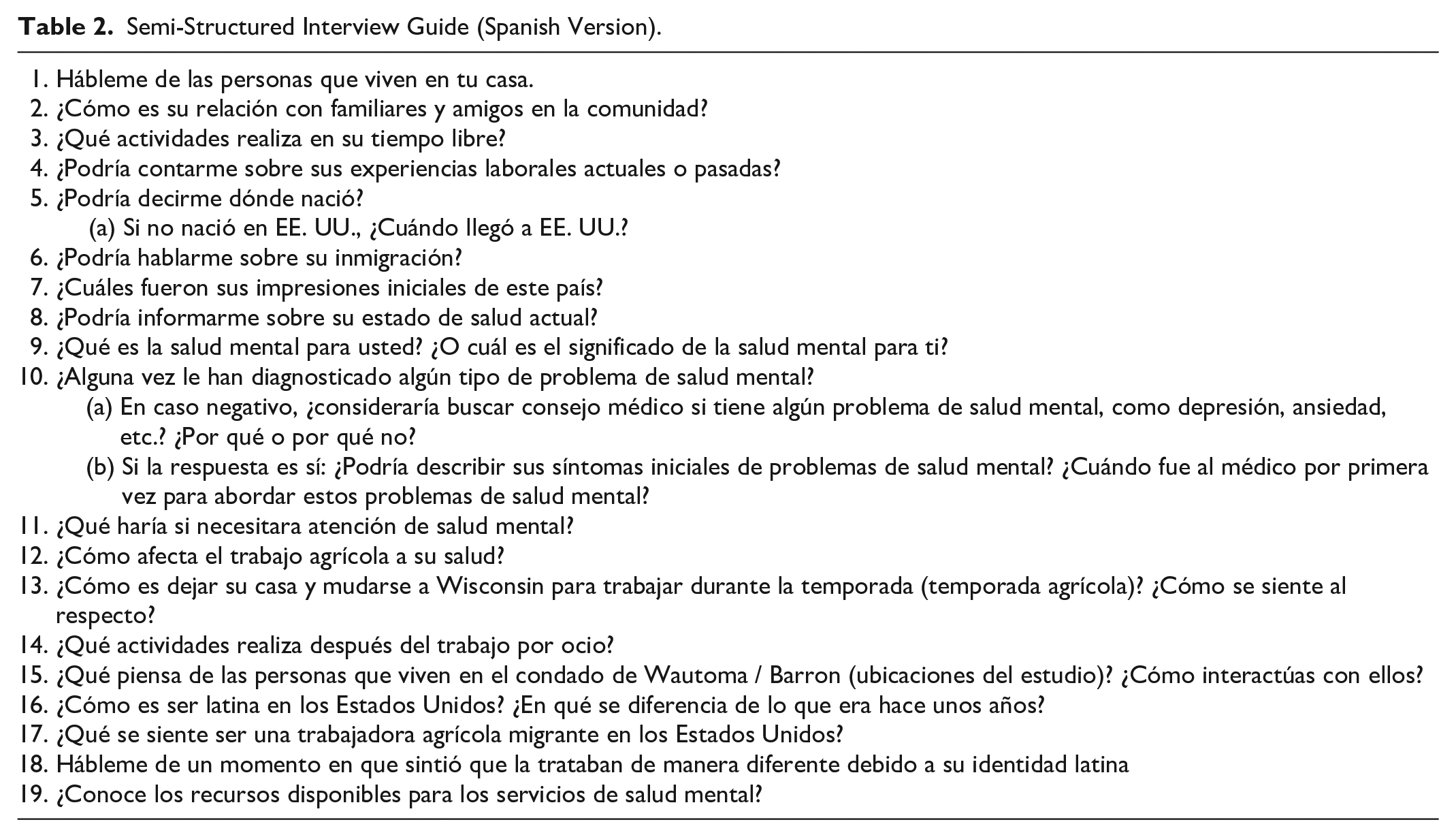
This study followed a qualitative descriptive design using in-depth semi-structured interviews with open-ended questions and the use of follow-up questions to clarify or expand the participants’ answers. The questionnaire included questions about health in general and family dynamics, followed by questions about mental health and immigration. The interviews were offered in English (Table 1) and Spanish (Table 2), and face-to-face or by phone. In addition, demographic data were obtained at the beginning of the interviews (Table 3).
Semi-Structured Interview Guide (English Version).
Semi-Structured Interview Guide (Spanish Version).
Demographic Data for Women Interviewed a (n = 34).
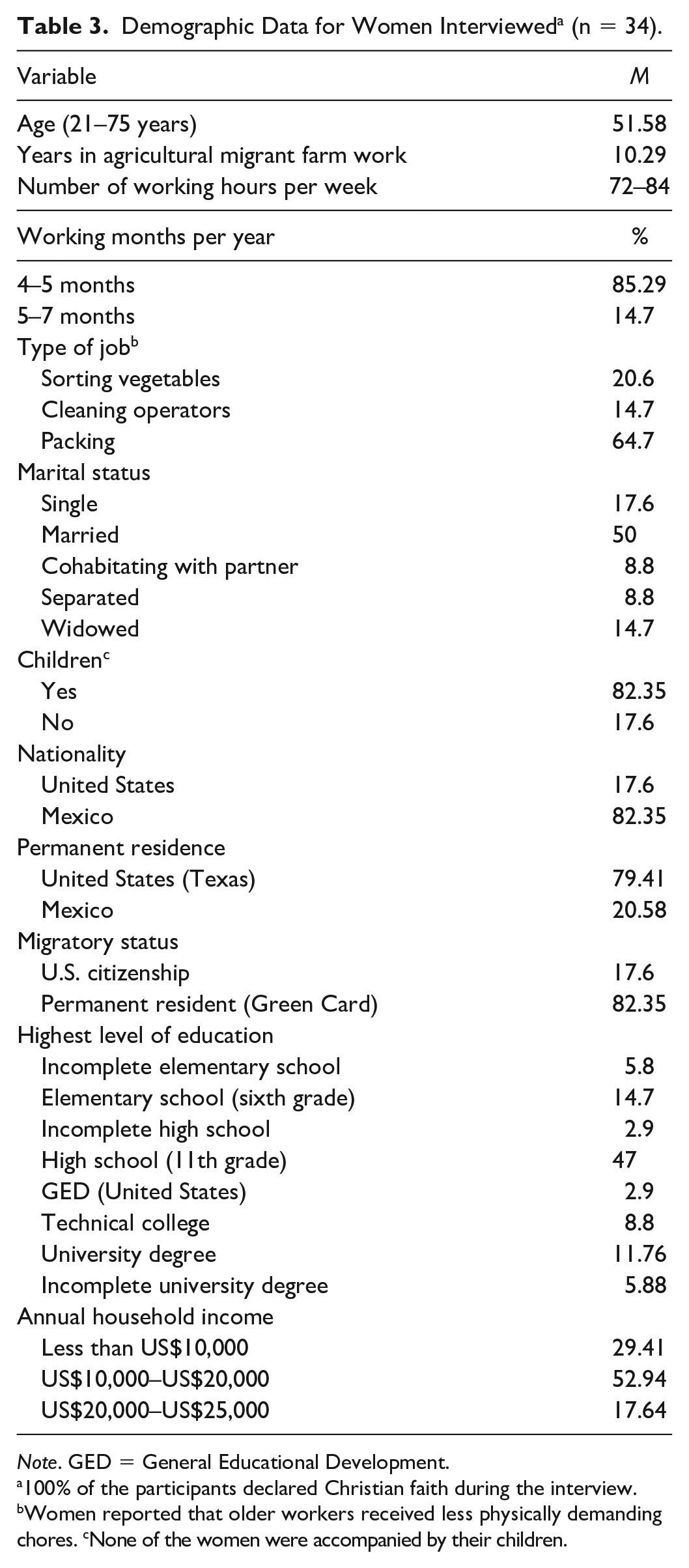
Note. GED = General Educational Development.
100% of the participants declared Christian faith during the interview. bWomen reported that older workers received less physically demanding chores. cNone of the women were accompanied by their children.
The principal researcher is a Latina PhD-prepared nurse fluent in English and Spanish, who designed this study, developed the research questions, and conducted the interviews in the women’s language of preference (English or Spanish) to enhance the communication and accuracy of the data gathered. The principal investigator’s reflective journaling, iterative data analysis, and random audits of the interviews transcripts by the senior coauthor were used to build trustworthiness, enhance credibility, and to minimize biases in the data analysis.
Sample and Setting
Purposive sampling was used to recruit the women participants in this study. Family Health La Clinica, a federally funded health care institution serving migrant farmworkers, and Embrace Services, a domestic violence and sexual assault agency, facilitated recruitment. Family Health La Clinica offers primary health care services in their mobile clinic during the agricultural season. In coordination with the farm or factory management, La Clinica mobile clinic scheduled visits to the migrant camps, where migrant workers receive services upon previous appointment. The principal researcher joined La Clinical mobile clinic and collected data throughout Wisconsin rural areas. Informative flyers were posted at the camp’s cafeteria and offices. Snowball sampling followed the first few interviews. The inclusion criteria included women who self-identified as Latina, were 18 years of age or older, and were working as migrant farmworkers at the time of the interview. Face-to-face individual interviews took place near the mobile hospital in a safe and private environment.
Data Collection
The semi-structured interviews lasted 60 to 90 min and were conducted over 4 months (between August and November) in 2021. Due to scheduling conflict, 4 participants agreed to one face-to-face meeting. After inclusion criteria were established, verbal consent was obtained. All the interviews were in Spanish and were audio-recorded to capture in detail the information provided by the women without losing data. Twenty-three interviews were conducted face-to-face and 11 by phone. Besides the audio recordings, the interviewer took notes of the women’s body language and other nonverbal information during the interview. Each interview received a code number, and any potential identifiers captured in the audio recording were removed from the transcription. At the end of the interview, each participant received a US$25.00 Walmart gift card as a token of appreciation for their time and willingness to participate in the study. The principal researcher provided information regarding local resources available for the Latino community.
Data Analysis
After the audio-recorded interviews were manually transcribed and translated by the first author, back translation was used to confirm the accuracy of the transcriptions. These transcripts were coded using line-by-line thematic analysis, allowing for the discovery, interpretation, and report of patterns and clusters of meaning found in the data (Ritchie et al., 2014). Finally, field notes were used as reflective information during the thematic analysis.
Ethical Considerations
This study received approval from the institutional review board at the University of Wisconsin–Milwaukee. Before beginning the interviews, the women received detailed information regarding the study details, risks, benefits, and their right to withdraw from the study at any time without penalty.
Results
This article focuses on the participants’ perceptions and conceptualizations of mental health. After thematic analysis, five themes were identified: (a) family relationships and work productivity, which we labeled “Mental health is everything”; (b) emotional state and capacities, which we labeled “Mental health is in tu mente (your mind)”; (c) stigma, which we labeled “It is when you are like medio loca (crazy)”; (d) denial and shame, which we labeled “It was a problem that I had to sufrir sola (suffer alone)”; and (e) faith and spirituality, which we labeled “Praying helped my mental health” (Figure 1).
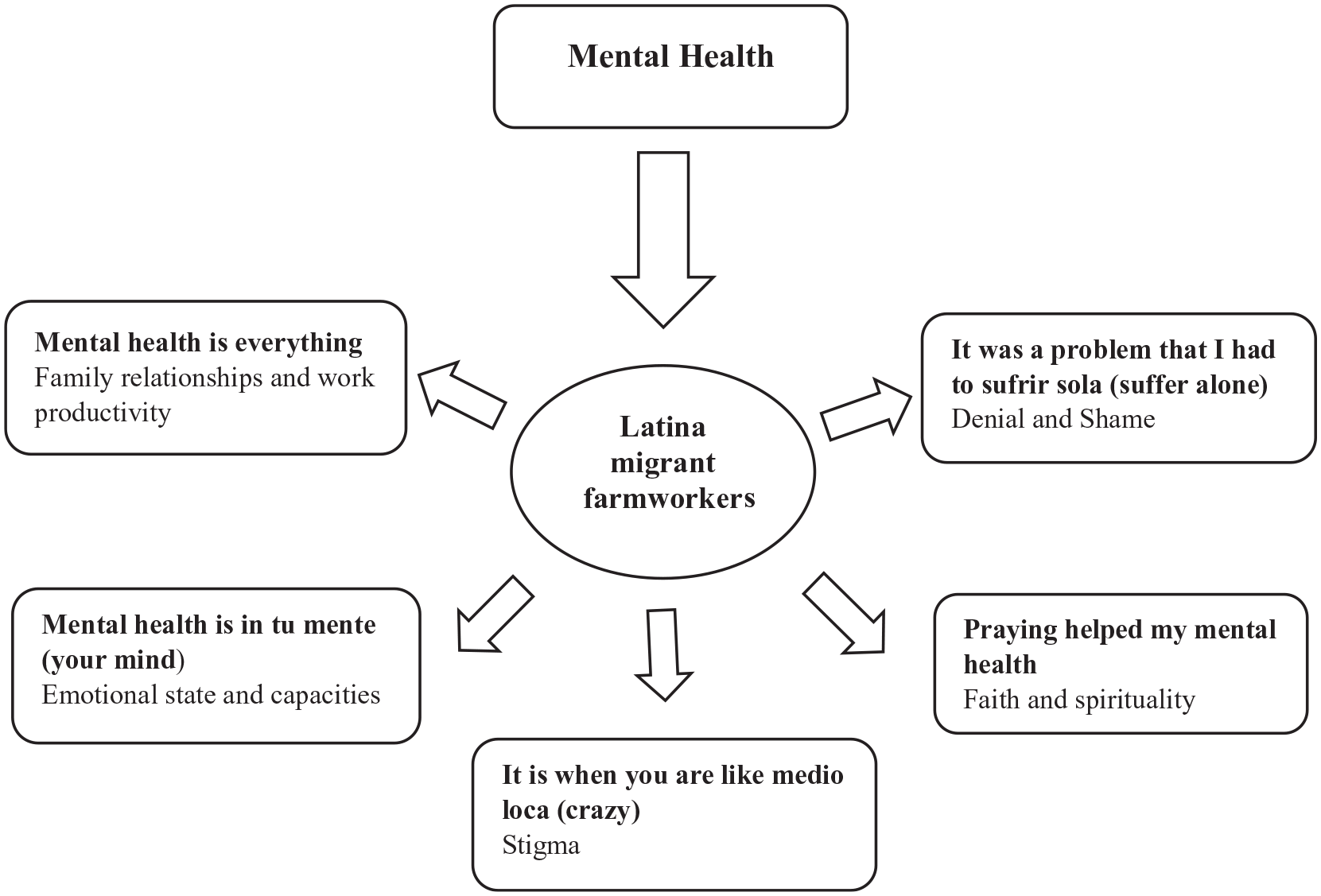
Thematic Diagram to Illustrate Women’s Conceptualizations of Mental Health
Mental Health Is Everything
Participants’ conceptualization of mental health was associated mainly with family relationships and financial income. In other words, family relationships, work productivity, and mental health were all interrelated. One factor had an effect on the others. For example, one woman said, Mental health, well, I think it has to do with everything with the family, how you are with your family, how you are at your job, all of this affects your mental health, if you are not comfortable in your job, if you have family problems, it affects your mental health. (Participant 1)
Another woman explained the effects of mental health on family dynamics and work performance. She explained the connection between physical and mental health and how mental ill-health affects her work performance and family relationships.
These statements demonstrated the women’s understanding of mental health and how it affects their priorities, which, in this case, are family and income. Furthermore, women’s conceptualization of mental health was related to their ability to provide for their families by maintaining an adequate work performance as many women’s income is the sole source of family income. For instance, one woman explained that mental health . . . is an important part of life if you are physically well but emotionally or mentally you are not then you do not perform well at work. . . . you cannot do your job, as you want it, or you are sufriendo (struggling) to finish. (Participant 3)
The women also defined mental health based on positive and negative impacts on family dynamics. A woman compared mental health with being alive and having a positive intergenerational family relationship. She said, “Mental health means life. . . . I want to be mentally well so I can enjoy my grandchildren; take care of them, talk to them, play with them, and continue working. It means mantenerse viva (staying alive)” (Participant 25). In addition, this woman also conceptualized mental health from the perspective of self-esteem and self-worth, productivity, and socialization: “As long as we have 100% mental health we can continue working and we can continue to have our social life” (Participant 25). Conversely, negative behaviors affected mental health and altered the family dynamic. This is described by one of the women in the following statement: “Mental health affects the family because when there are many fights and when there is violence, well, one is not mentally well” (Participant 19). The disruption of family dynamics caused by mental illness was incentive enough for women to consider the importance of adequate mental health care. The same woman added, “. . . it is important to take care of mental health so that one can live well with your husband, with your children, and you can be tranquila (at ease), yes, and con tu mente en paz (having peace of mind)” (Participant 19).
Mental Health Is in Tu Mente (Your Mind)
Some women operationalized the concept of mental health as a physical ailment located in the individual’s cabeza (head) and expressed by changes in mood and emotional state. A woman said, Mental health is your nervios (nerves), it’s inside your cabeza (head), like when one is worried about something. Like when you do not have money or your family, or like when something bad is going to happen to you, or your family. . . one keeps thinking . . . . I wanted to stop thinking, but I could not stop. (Participant 23)
Women’s perception of mental health was explained as a state of continuous anxiety called “los nervios” in which psychosomatic symptoms were reported. A woman shared her perception of mental health as a collective health issue that can be passed from one individual to others. She said that this perception could be related to Latino’s community-oriented nature: If you hear that someone has a disease, soon after you have the same disease. . . . It’s like you llamas a la enfermedad (call the disease); because you live with los nervios (nerves) and you can’t stop thinking about it. (Participant 9)
Some women offered a definition of mental health related to intellectual capacities, cognition, and decision-making. In these cases, women conceptualized mental health as la mente (the mind) in which positive behaviors included being focused, rational, and cuerdo (coherent) to make good decisions, “Mental health is what you think . . . like your thoughts. It is when you are thinking right. It is in your head, in tu mente (your mind)” (Participant 5). Conversely, the absence of mental health leads to distress and even fatal consequences, “if your mind is well, you will do fine, but if . . . you are not mentally well, you do not think well, nothing works well” (Participant 21).
It Is When You Are Like Medio Loca (Crazy)
Some women’s perceptions were informed by a negative association of mental health with the stigmatized concept of “loco” (crazy) or “locura” (craziness). The concept of loco was described with examples of individuals experiencing auditive and visual hallucinations, and behaviors indicative of poor health. One woman said, “. . . is when you are not well in your head. . . like wandering in the street and talking to yourself . . . like you are lost in your head, like loco (crazy)” (Participant 15). Other women further described mental health using the figure of “loco” highlighting inadequate behaviors including violent outbursts, “. . . is when you go all dirty, you do not bathe, yelling at the people and eating garbage, like loco (crazy)” (Participant 27). This example is further evidence of the stigma and fear associated with mental illness. Women demonstrated awareness of the relationship between substance abuse and mental health. Furthermore, they provided examples of the effects of drugs on individuals’ mental health leading to the stigmatized characteristics of “el loco.” A woman said, I knew a man from my rancho (village) who went loco (crazy) because of using drugs. He had a good job, but the bad influences got him into drugs. (Participant 21)
It Was a Problem That I Had to Sufrir Sola (Suffer Alone)
Some women’s definitions of mental health include statements of shame. Women avoided using terms such as depression, anxiety, or stress and, instead, they explained their symptoms using terms such as cansancio (tiredness), nervios (nervousness), or tristeza (sadness). One woman defined mental health in the context of her grieving experience after the death of her adopted baby who was born with a congenital disease and the passing of her mother due to a chronic illness: When my baby daughter died everyone thought I was going loca (crazy). . . . My doctor asked me if I was deprimida (depressed) and I told him that it was not depression, but cansancio (tiredness). I took care of my mom until the day she died. I was close to my mom . . . And then my baby died. . . . I was very triste (sad), and I am still sad, but I am not depressed, I do not need to take medications. (Participant 12)
Another woman, despite receiving a diagnosis of depression, related her symptoms of depression to sadness. She said, Once a doctor told me I had depression. But I was not thinking about quitarme la vida (taking my own life), nothing like that. I do not like to be alone, because then I feel tristeza (sadness) and soledad (loneliness). It’s not that I am depressed, but sad instead. (Participant 22)
While women throughout the interview expressed their closeness to family and community, they chose to keep issues related to mental health private. Some women considered that mental health problems should be endured privately to avoid shame and distress to their families. One of the women shared that she kept her daughter’s mental illness a secret. She said, One of my daughters was diagnosed when she was 13. . . she was bipolar. . . I have never talked about this problem to anyone. Her illness was a problem that I had to sufrir sola (suffer alone). (Participant 17)
Praying Helped My Mental Health
Women also offered a description of mental health through the lens of their faith and spirituality. Several women spoke about a strong relationship between their faith and good mental health. Divine intervention was reported as a source of “protection” against mental ill-health. A woman said, “I trust in God to keep me healthy. . . . . Thank God, I have never been told I have depression or anxiety or anything like that” (Participant 4). Furthermore, divine intervention and faith were cited as the sources of comfort and hope against emotional distress: . . . when I was younger, I had some problems. I was in a bad relationship. Todo el dia era de llorar y nada más (All I did was cry all day long). I was consumida (consumed) by la tristeza (sadness), you know, eso que le dicen depresión (what is called depression). My mom told me we had to pray and go to the church. . . . doing that help my mental health. (Participant 33)
Mental health treatment and recovery were also associated with divine intervention. Prayer was associated with therapeutic effects and fewer side effects: I was taking Citalopram and Clonazepam, but I stopped taking them like eight months ago. I was afraid that I was getting addicted to them. My friend told me that I had to get closer to God, to talk to God. So, I prayed, and God helped me. (Participant 21)
Finally, some women’s definition of mental health was associated with penance and reflection. These concepts are explained from a cause–effect perspective. One woman said, “Well, for some people mental health is something you do to yourself. Because if you deserve sufrir (suffering) from mental health, you have to think what you did to deserve it and suffer the penance” (Participant 29).
Discussion
As we discuss the implications of our study, we must point out that we believe our findings are transferable to other groups of minority migrant farmworkers within and even outside of the United States. Our qualitative inquiry could be applied to populations of different ages, gender, culture, and geographical location, who are underrepresented in research studies; however, broader studies would offer a more profound understanding of perceptions and conceptualization of complex concepts such as mental health. This study, informed by feminist epistemologies, centered women’s voices, eliciting their conceptualization of mental health based on their worldviews and life experiences. Although our sample included a wide range of ages among participants, their responses were consistent. Most women in our study described mental health as a determining factor in their family relationships and overall daily functioning. This finding is similar to previous studies that noted a relationship between Latina mental health and family dynamics. For example, Lorenzo-Blanco et al. (2017) identified a relationship between Latino parents’ stress and depressive symptoms and lower parent-reported family functioning, which is a mediator to youth alcohol and cigarette use. Similarly, another study found that Latinas identified the adverse effects of being away from their families, as one risk factor for depression and psychological stress (De Oliveira et al., 2017). Finally, women in our study knew the relationship between intrafamilial violence and mental health. Intrafamilial violence and other forms of violence are health challenges identified in other studies with Latinas, which have significant implications for their mental health (Basile et al., 2015; Gonzalez et al., 2020; Reyes et al., 2023).
Participants’ perceptions of mental health concerning mood and emotional state are consistent with previous studies. For instance, Zvolensky et al. (2016) conducted a study in which the interaction between depression and anxiety was significantly related to suicide, social anxiety, mood/anxiety diagnoses, and disability. Furthermore, the role of external locus of control in Latinas’ anxiety and stress has been linked to increased emotional distress and decreased help-seeking behaviors (Anastasia & Bridges, 2015; Rosales & Calvo, 2017). In addition, Barrera and Longoria (2018) explained Latinos’ use of some idioms, such as nervios or miedo, to describe emotional distress and suggest the importance of cultural competence in understanding the meaning of such terms.
The women in our study related mental health with fear and stigma. Stigma was associated with loco or locura, which also involved isolation and fear of ostracism. These findings concur with previous studies in which poor mental health was associated with stigma. For instance, Lopez et al. (2018) argued that these perspectives are related to low health literacy levels and that the lack of knowledge about mental health had an inverse relationship with stigma. Other studies found a relationship between mental health-related stigma and Latinas’ underutilization of mental health services and poor mental health outcomes (DeFreitas et al., 2018). Evidence suggests the need for mental health care that considers the presence of stigma and how it informs mental health–seeking behaviors (Sickel et al., 2019) and the development of culturally congruent policies and interventions (Gopalkrishnan, 2018).
The women in this study also reported the need to maintain privacy regarding aspects related to mental health. Mendoza et al. (2015) found that some Latinas conceal mental illness to protect their family’s honor and avoid bringing social disgrace to themselves or their families. Women’s decision to conceal their or a close family member’s mental illness is consistent with the idea of “marianismo” in which Latinas should be open to personal sacrifice for the benefit of their children and family (Da Silva et al., 2021).
The relationship between faith and spirituality, and mental health, as reported by the women in this study, is consistent with previous evidence. A study by Caplan (2019) found that lack of faith, not praying, demonic intervention, and sinful behaviors of parents were considered risk factors for depression among Latinos. Women’s narratives about faith as a mental health protective factor concur with previous studies that support a religious coping framework in which faith and spirituality offer unique methods and strategies to manage negative experiences and emotions, and therefore protect against poor mental health (Caplan, 2019; Haney & Rollock, 2020; Turner & Llamas, 2017). In addition, Latinos who believe prayers could cure a physical or mental illness prefer help from a priest, spiritual healer, or curandero (folk healer) than Western mental health care (Barrera & Longoria, 2018). Spirituality and faith are protective factors among Latinos’ mental health and could serve as complementary therapies to improve mental health care outcomes and destigmatize mental illness.
Implications for Nursing
Our findings support transcultural nursing’s involvement in developing mental health policy and practice that informs culturally appropriate care. Nurses’ strategic position allows them to advance mental health knowledge based on the narratives of populations at risk of poor mental health outcomes, including Latina migrant farmworkers. Learning about the wide age range among Latina migrant farmworkers offers the opportunity to develop age-appropriate mental health interventions. Similarly, the data obtained from the participants serve to update the information available from this population as a reference for future research. From a feminist perspective, systems and processes must capitalize on cultural empowerment, moving away from a deficit approach and facilitating new avenues for integrated mental health care approaches (Gopalkrishnan, 2018). From a transcultural nursing perspective, the application of cultural care theory will aid nurses and other health care professionals to design and implement mental health care interventions informed by Latina migrant farmworkers’ cultural values (Maurer et al., 2018). Considering the strengths observed in the narratives of Latina migrant farmworkers regarding mental health, health care providers could center these as protective mechanisms and include them in culturally congruent care plans.
Limitations
Women who participated in this study were Mexican or of Mexican ancestry. Findings could have been different for Latinas with different nationalities or cultural ancestry. Phone interviews (n = 11) limited the collection of nonverbal data. However, thematic consistency was confirmed across all the interviews. Receiving a gift card may have influenced participants’ willingness to participate in the study. The participants’ working schedule reduced their availability to one interview only. More opportunities to meet with the participants may have facilitated more in-depth discussions. Finally, the lack of evidence and demographic information hindered our ability to analyze trends or changes within this population.
Conclusion
Latina migrant farmworkers face challenges that increase their risk for mental ill-health. The lack of current literature addressing Latina migrant farmworkers’ mental health perspectives and mental health care needs in Wisconsin hinders the implementation of adequate interventions. The utility of this qualitative study, informed by Chicana, postcolonial, and Black feminist epistemologies, is to bridge the existing knowledge gap by offering a deeper understanding of mental health from the voices of Latina migrant farmworkers. This includes the narratives of their mental health and health care–seeking experiences, allowing for the design of culturally informed policy and practice.
Footnotes
Acknowledgements
The authors are grateful to Ms. Erin McArthur and Mr. Pedro Graf for their assistance in formatting this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.