
Abstract
Introduction:
Urinary incontinence (UI) in women is a global public health issue. However, there is a limited understanding of the experience of women from underrepresented groups suffering from UI. The purpose of this systematic review was to examine current evidence regarding the experience of women with UI from these groups.
Methodology:
A systematic search was undertaken to retrieve research studies that answered the research question. Four qualitative research studies were included. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guided this review.
Results:
Four themes emerged from this review: the perceived origin of UI, the physical, psychological, and social impact of UI, the impact of culture and religion on UI, and vice versa, and the interaction of women with health services.
Discussion:
Social determinants of health, such as religion and culture, need to be considered by professionals providing care if women from underrepresented groups experiencing UI are to receive optimal care.
Keywords
Introduction
Urinary incontinence (UI) is a highly prevalent health issue affecting women globally (Raasthøj et al., 2019) and is responsible for diminishing women’s quality of life (Vaughan & Markland, 2020). According to the National Collaborating Centre for Women’s and Children’s Health (2013) UI is understood “as any involuntary leakage of urine.” Despite the worldwide prevalence of this health problem, the relationship between ethnicity and UI is inadequately understood (Brown & Simon, 2021). The impact of ethnicity on UI has disproportionate impact of UI on women of white ethnicity (Anger et al., 2006; Dooley et al., 2008; Thom et al., 2006). Women from underrepresented groups 1 have a higher prevalence in certain types of UI than their white counterparts (Sears et al., 2009; Shah et al., 2007). Although these studies suggest health differences rather than health inequalities (Brown & Simon, 2021), a growing body of evidence highlights the under-representation of minority ethnic women in UI research (Alvarez & Harmanli, 2021; Gonzalez et al., 2021; Mckay et al., 2021). Reporting of minority groups is inconsistent due to the tendency of ethnic minorities to be treated as homogeneous groups (Karseras & Hopkins, 1987). This inadequate and inconsistent reporting of a protected characteristic, such as ethnicity (Legislation.gov.uk, n.d.), negatively affects the extrapolation of the results (Mckay et al., 2021) and clashes with the principles of social justice, affecting the distribution of resources, services, and research (Redwood & Gill, 2013). Therefore, women from underrepresented groups have been, and currently are, experiencing health disparities concerning UI, predominantly caused by structural racism (Bailey et al., 2017; Jones, 2000). Nowadays, significant and unjustifiable health inequities still exist among women in the European Region (WHO, 2016) and the United Kingdom (DHSC, 2021). Health inequities among women are also reflected in the male-as-default approach in clinical research studies and the limited research and funding available to study women’s health issues and sex-specific diseases (Macdonald & Hands, 2021). In the case of women from underrepresented groups, this existing gender health gap (Winchester, 2021) is accentuated by the intersectionality of being a woman and belonging to an ethnic group different from the country’s ethnic default (McCall, 2005). Individual characteristics and lifestyle factors, social and community networks, and general social-economic, cultural and environmental conditions also need to be considered due to their impact on health (Dahlgren & Whitehead, 1993, 2007). Social Determinants of Health (Marmot et al., 2008), defined as “the conditions in which people are born, grow, live, work and age” and “the fundamental drivers of these conditions,” are strongly associated with health inequities. In the case of ethnic groups, intersections between socio-economic status, ethnicity, and racism reinforce inequalities in health (Marmot et al., 2020). Moreover, in relation to UI, there is some evidence that link SDH with severity of symptoms in women with overactive bladder (Tellechea et al., 2021).
The experiences of women from underrepresented groups remain under-researched, absent, or rendered invisible; hence, understanding the experience of women who have remained “silenced” becomes increasingly essential (Serrant, 2020). There is a need to comprehend the experience of service users to contextualize clinical evidence and inform patients’ needs (Rand et al., 2019). This article reports a systematic review designed to address the following question:
Method
The Sample, Phenomenon of Interest, Design, Evaluation, Research type framework (Cooke et al., 2012) was used to develop a focused review question (Riesenberg & Justice, 2014) (Table 1). The population was kept broad as a preliminary search did not identify research studies solely focusing on perinatal women. This research was intended to cover UI in perinatal women, however, the preliminary search did not identify research solely focusing on this group, therefore all populations were included in this study.
The SPIDER Framework to Inform the Systematic Review Question.
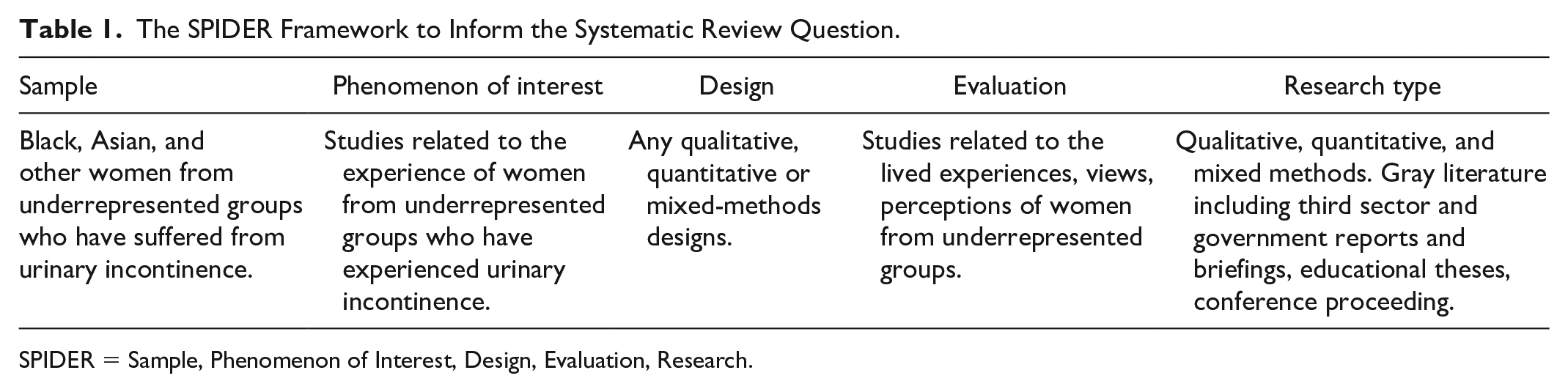
SPIDER = Sample, Phenomenon of Interest, Design, Evaluation, Research.
Search Strategy
The literature search was performed between August 1, 2022, and August 15, 2022, using Medline, PubMed, CINAHL, and EMBASE databases. The search terms were based on a two-tiered search strategy; the first tier represented terms related to the target population (“ethnicity,” “ethnic group”, “ethnic minority,” “Black,” “race,” “Asians,” “mixed-race,” “vulnerable population,” “Arabs”). The second tier represented the phenomenon of interest (“urinary incontinence”, “urinary incontinent,” “urine leak”). Each of these search tiers was run separately, and then all two tiers were combined into one final search.
Study Selection and Inclusion Criteria
Inclusion and exclusion criteria were applied to identify relevant evidence (Table 2). Due to the limited evidence on the current topic, no limiters were applied to the study design or setting. No restrictions were placed on publication type.
Inclusion and Exclusion Criteria.
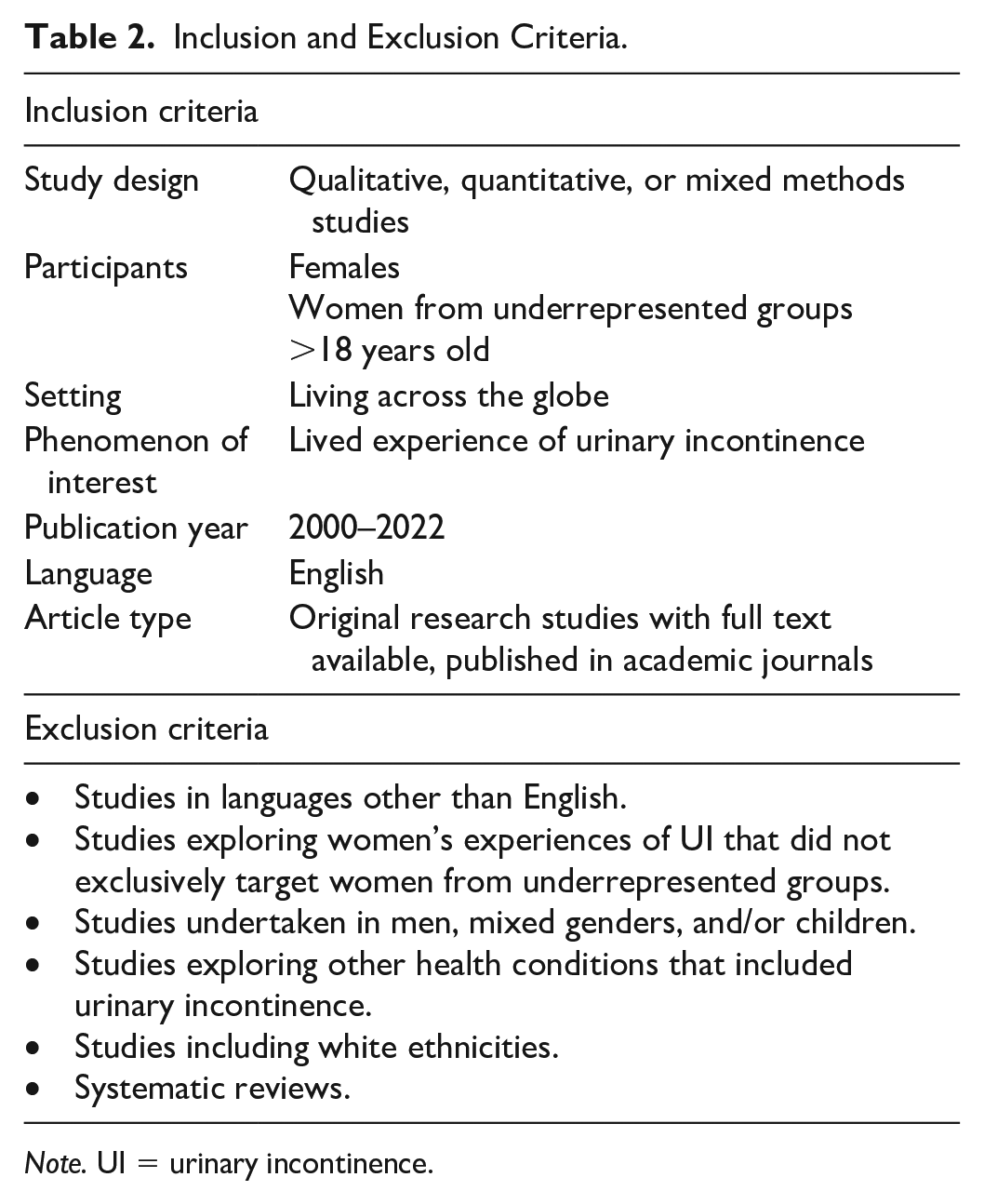
Note. UI = urinary incontinence.
The term ethnic minority used in this search was based on the Cambridge Advanced Learner’s Dictionary & Thesaurus’s definition: “a particular ethnic group (= a group of people with a shared culture, tradition, language, history, etc.) living in a country where most people are from a different ethnic group.” Therefore, studies undertaken in countries where women from certain ethnic groups (i.e., Black, Asian, Arab, mixed-race women) belonged to an ethnic minority were included. On the contrary, studies that included a combination of ethnic minorities and white ethnicities were excluded due to the difficulty of tracking themes back to individual participants’ responses. The age of the participants was established as 18 years old as the legal definition of an adult (Office for National Statistics, 2019).
In regards to the term urinary incontinence, the working definition was based on that provided by the International Continence Society (D’Ancona et al., 2019), which describes UI as a “complaint of involuntary loss of urine.” Only evidence published from 2000 to 2022 in English was included due to the limited evidence available on the subject (Paniagua, 2002). Only articles written in English were included, as this language is regarded as the “lingua franca” of science (Kamadjeu, 2019), and the application of this limiter does not appear to contribute to systematic bias (Morrison et al., 2012). Accordingly, systematic reviews were excluded, and individual studies were individually screened for eligibility.
Data Extraction and Quality Assessment
One reviewer (VB) extracted the data using a standardized template across the following categories: country/population characteristics, type of study and aim, age, recruitment, findings, limitations, and Critical Appraisal Skills Programme (CASP) tool for quality appraisal in qualitative synthesis (Table 3). The quality score was derived using the CASP (2018) checklist. The CASP tool contains 10 questions; it is considered useful for the use of novice qualitative researcher (Long et al., 2020). The tool is endorsed by the Cochrane Collaboration qualitative research groups and the WHO for use in qualitative evidence synthesis (Noyes et al., 2018). One limitation of the CASP tool is the lack of specific rating scales (Butler et al., 2016). As argued by Long et al. (2020), this tool fails to produce a classification based on “high”, “medium” or “low” quality. Consequently, the quality of the studies was assessed according to the responses to the questions pertaining to the rigor of data analysis, trustworthiness, and credibility of the findings (Lincoln & Guba, 1985).
Key Characteristics of the Studies Included in This Systematic Review.
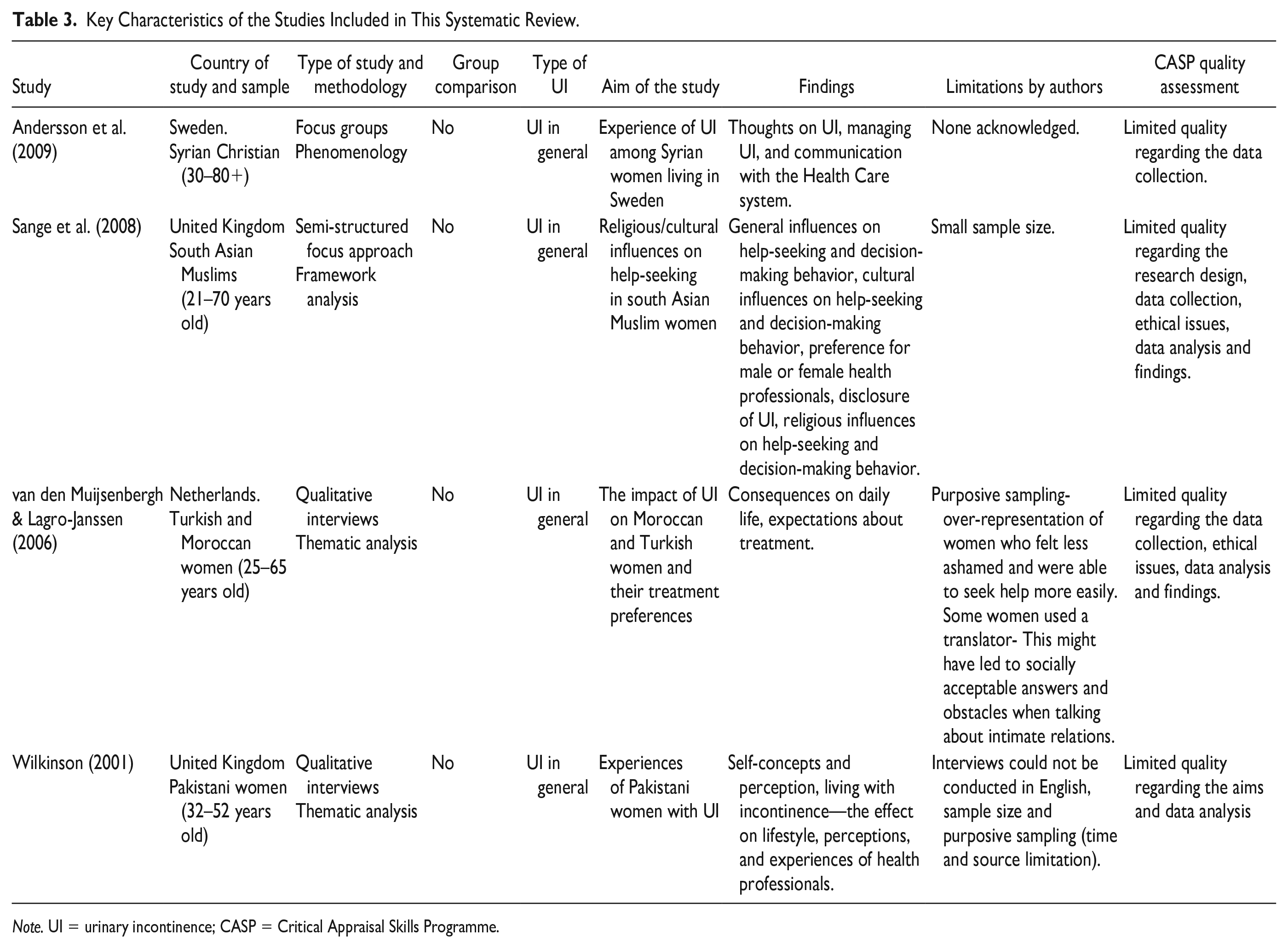
Note. UI = urinary incontinence; CASP = Critical Appraisal Skills Programme.
All decisions around inclusion, quality, and data extraction were discussed between the three authors. It is recognized that it is good practice to have two reviewers in the process of inclusion of articles but it was not feasible within the limitations of this review.
Results
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (Page et al., 2021) has been used to guide the report of the systematic review. The process of identifying relevant studies is summarized in Figure 1. One systematic review (Siddiqui et al., 2014) was identified, which included 23 studies on perceptions about female UI. Not all studies in this review focused on the population of interest, so the individual studies were reviewed. After screening each study, four of the papers met the inclusion criteria and were included in the final review.
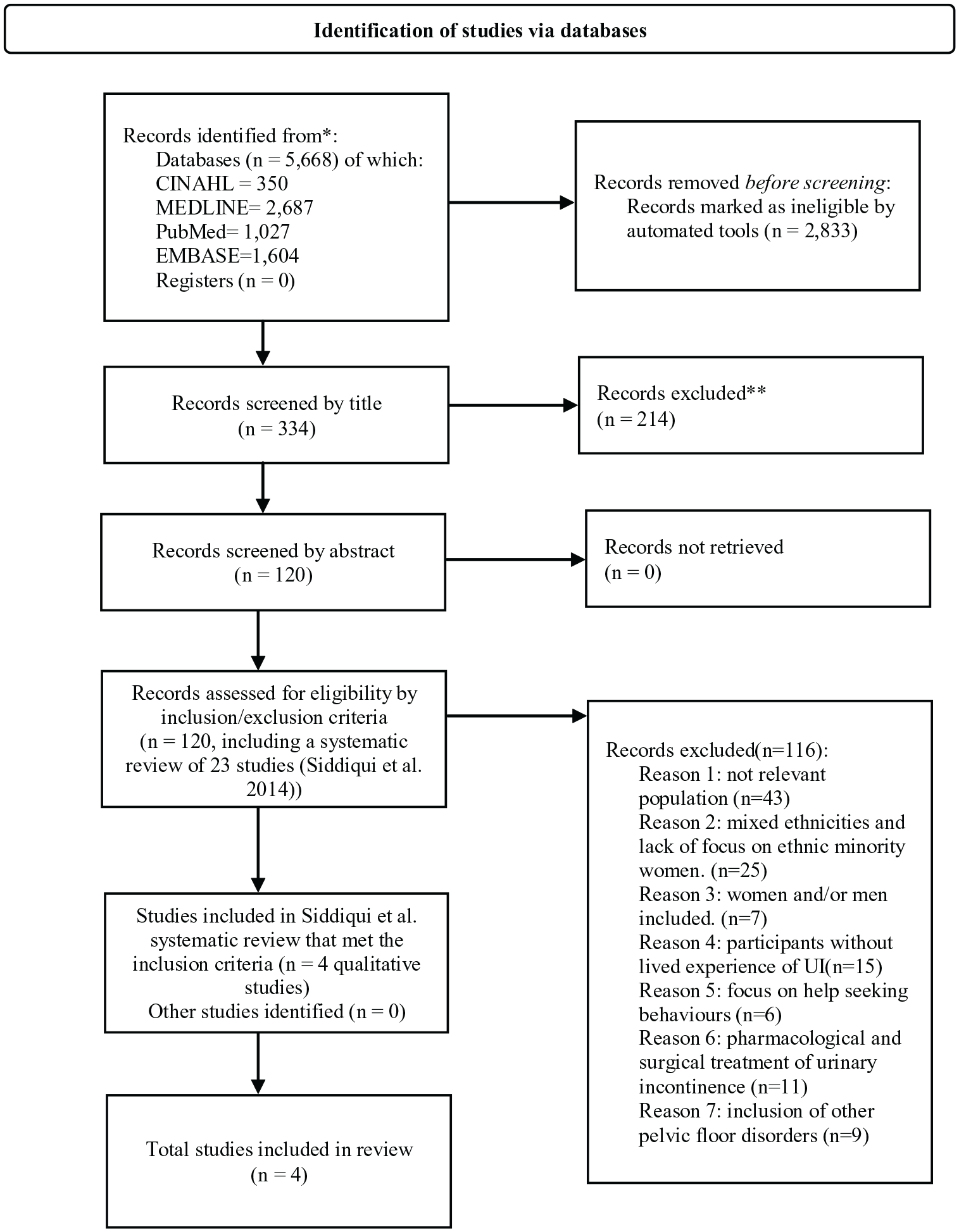
Process of Identifying the Relevant Studies
All four studies were published in peer-reviewed English language journals, although three studies used interpreters as part of their study design to overcome language barriers. Two papers were published in Nursing journals, one in a General Practice journal and one in a transcultural Nursing journal. Together the studies made a total sample of 59 women. Two studies were conducted in the United Kingdom, one in Sweden, and one in the Netherlands, between 2001 and 2009. The ethnicities of the women were South Asian Indian, Syrian, Pakistani, Turkish, and Moroccan. All studies used a qualitative design and employed data collection methods such as semi-structured interviews and focus groups. The key characteristics of the studies included in this systematic review are summarized in Table 3.
All the studies had limited quality in one or multiple domains of the CASP tool (Table 4). One study did not provide a clear statement of the research aims (Wilkinson, 2001). The use of a qualitative methodology was found appropriate in all papers, but in one study the method used for data collection was unclear and unjustified (Sange et al., 2008). This paper also lacked evidence on data saturation and an explanation of sample size. Similarly, the study by Andersson et al. (2009) omitted information related to data saturation and justification of the sample size and structure of the focus groups.
Applied CASP Tool to Research Studies.
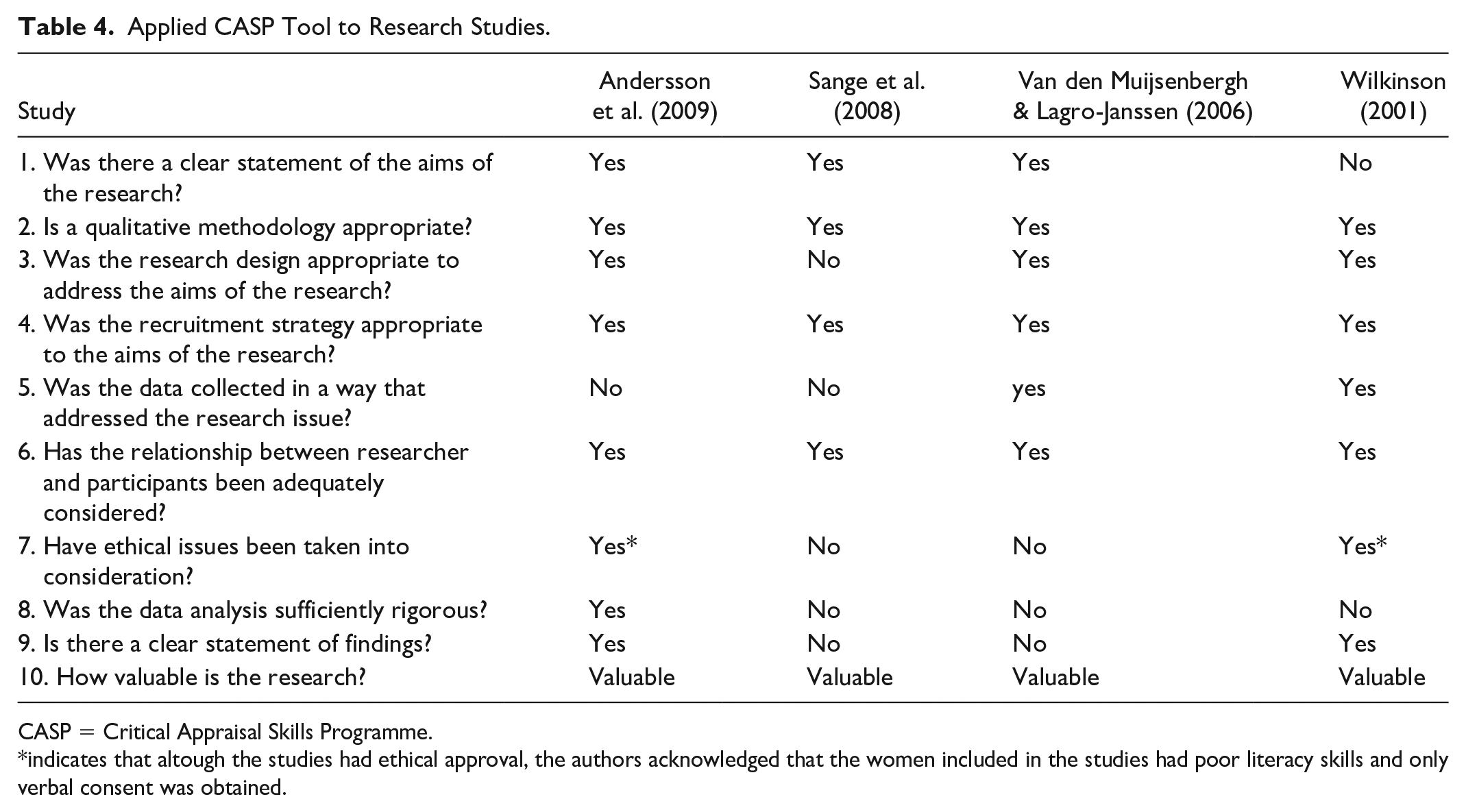
CASP = Critical Appraisal Skills Programme.
indicates that altough the studies had ethical approval, the authors acknowledged that the women included in the studies had poor literacy skills and only verbal consent was obtained.
All authors declared limitations in their studies regarding the impact of language barriers and the use of translators. Two studies did not report seeking ethical approval (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006), and, although the other two studies provided evidence of ethical approval, only verbal consent was gained due to the illiteracy of participants (Andersson et al., 2009; Wilkinson, 2001). The data analysis was declared insufficient in three studies due to a lack of in-depth explanation of how the analysis was performed (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen 2006; Wilkinson, 2001). Two studies did not provide a clear statement of findings (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006). Despite these limitations, all studies were included in the review as they provide valuable contributions to the phenomenon of interest in this neglected population.
Emerging Themes
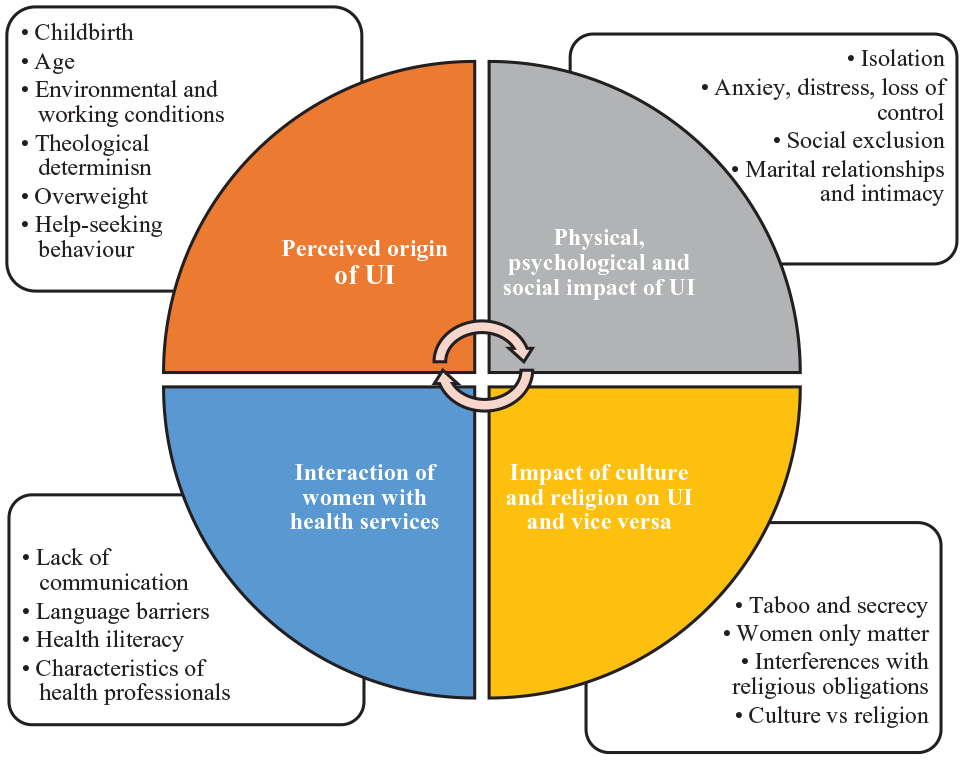
Four themes emerged from this review (Table 5) and the findings of each study by theme are shown in Figure 2.
Emerging Themes.
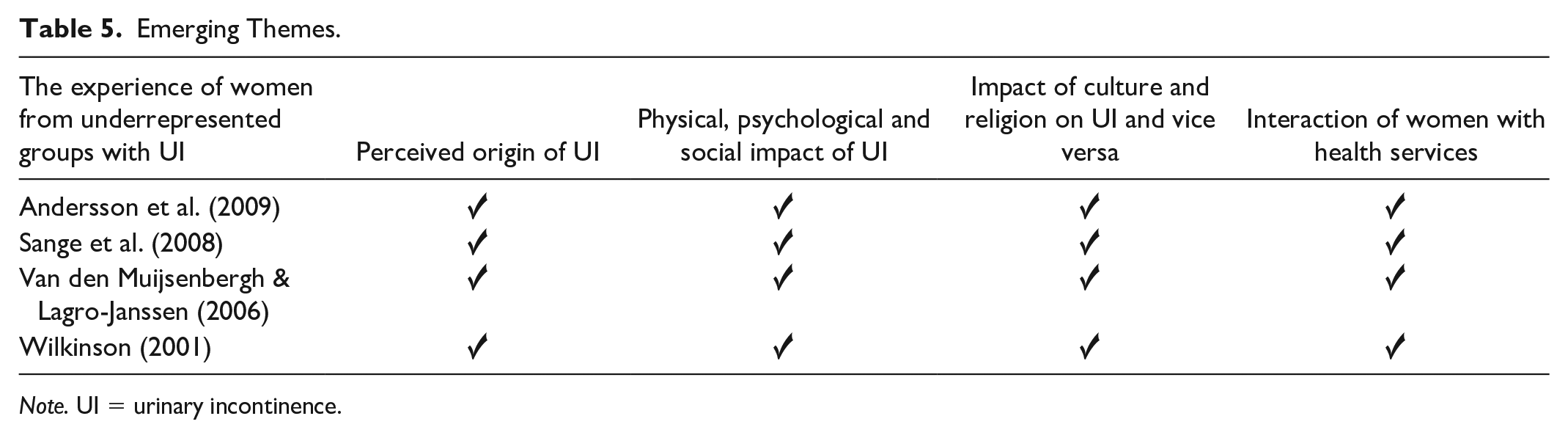
Note. UI = urinary incontinence.
From Findings to Themes
The Perceived Origin of UI
Across all the studies, participants provided an explanation of their perceived origin of UI. Some women regarded UI as a “woman’s problem,” and a consequence of childbirth and age (Sange et al., 2008). Decision-making behaviors differed according to age and country of birth. Other women believed that UI was a “normal situation” at their age (van den Muijsenbergh & Lagro-Janssen, 2006) and a direct consequence of the aging process and childbirth (Andersson et al., 2009). Some women blamed themselves for their UI due to being overweight and their lack of help-seeking behavior (Wilkinson, 2001), while others believed that UI was caused by environmental factors, such as the type of work undertaken in their home country or the climate of the country they migrated to, as UI coincided with migration (Andersson et al., 2009). Among other explanations of the origin of their UI was the influence of religion in an attempt to justify its occurrence. Muslim women regarded Islam as the most dominant and vital aspect of their life with some believing that UI was theologically determined, that is “their condition was created by Allah” (van den Muijsenbergh & Lagro-Janssen, 2006) and that “illnesses are from God and God is the only source that will send you a cure too [. . .]” (Sange et al., 2008).
The Physical, Psychological, and Social Impact of UI
UI was identified as embarrassing, shameful, and taboo by all the women in all studies (Andersson et al., 2009; Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006; Wilkinson, 2001). Some women also expressed the psychological consequences of having UI, such as mental stress, loss of control, low self-esteem, and anxiety (Wilkinson, 2001). Irrespective of their religious beliefs, women felt socially isolated and restricted by UI (Andersson et al., 2009; Sange et al., 2008; Wilkinson, 2001).
Marital relationships and intimacy were also reported to be negatively affected by UI. Women expressed that UI could only be discussed in the presence of men in the absence of female relatives or friends (Andersson et al., 2009). As a result, some women hid this condition from their husbands due to shame and concerns over their husbands’ reactions, and preferred to exclude them from knowing about UI (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006). However, women groups were of high importance for some participants as a source of support and problem-sharing (Wilkinson, 2001).
The burden of UI complicated the marital relationships of most of the women and left women feeling humiliated and distressed (Van den Muijsenbergh & Lagro-Janssen, 2006; Wilkinson, 2001), particularly due to leakage of urine during intercourse (Wilkinson, 2001). For some participants, UI was the reason for not remarrying (Van den Muijsenbergh & Lagro-Janssen, 2006). Participants were also mindful and ashamed when visiting other people’s homes. Most women refrained from social gatherings or going out (Sange et al., 2008) and were limited by the proximity of toilet facilities (Andersson et al., 2009; Sange et al., 2008; Wilkinson, 2001).
The Impact of Culture and Religion on UI and Vice Versa
Religion and culture had a significant influence on the experience of women suffering from UI. The sample in three of the studies included Muslim women (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006; Wilkinson, 2001), and one study included Christian women (Andersson et al., 2009). On occasions, the boundaries between cultural and religious behaviors appeared to be blurred. Age had an influence on the perceived relationship between culture and behavior, where the younger the participant, the stronger was the belief that parental views were, in fact, religious obligations (Sange et al., 2008).
In terms of practicing the Muslim faith, UI was regarded as sinful due to its association with being unclean. The urine leakage interfered with ablutions and interrupted or prevented prayer (Sange et al., 2008; Van den Muijsenbergh & Lagro-Janssen, 2006; Wilkinson, 2001). In the case of Christian women, poor past experiences in their home country triggered fear and distrust of doctors with religions different from Christianity (Andersson et al., 2009).
Interaction of Women With Health Services
All women suffering from UI discussed their encounters with health care professionals. A common area seen as a barrier to accessing health care was the gender of the health professional when presenting to health services. It was evident in all studies included in this review that Muslim women provided different responses when asked about their preference for male or female health professionals. Some participants did not want to discuss their UI with their general practitioners (GPs) “under any circumstances” due to the fear of a physical examination, while older women reported having intentionally chosen a health professional with similar cultural and language backgrounds (Sange et al., 2008; Wilkinson, 2001). Women interviewed were ashamed or unwilling to bring up the subject in the presence of a male GP, particularly if a physical examination was required (van den Muijsenbergh & Lagro-Janssen, 2006) On the contrary, Christian women held the doctor just below God, and therefore most of them were acceptant of both male and female health professionals (Andersson et al., 2009). However, some older women found it embarrassing to get undressed in front of a man and preferred a female doctor.
Another critical aspect of the interaction between patient-professional was communication and language barriers. Difficulties in communicating and expressing health concerns led to perceptions of not being helped (Andersson et al., 2009). To overcome limitations with language, women reported the use of interpreters. However, the gender and acquaintance of these interpreters were also seen as problematic. To resolve this problem, women often brought a female friend or relative. Other issues that jeopardized the patient-professional relationship were women’s inhibition, lack of health education, and illiteracy (Wilkinson, 2001). These issues left women with feelings of frustration and they perceived that doctors were disinterested. Furthermore, some women demonstrated a knowledge gap concerning the basic functions of the bladder and genital organs (Van den Muijsenbergh & Lagro-Janssen, 2006).
Discussion
This systematic review examined the experience of women from underrepresented groups living with UI. The findings concur with existing evidence, where women refer to UI as “part and parcel of being a woman” (Peake et al., 1999), which encompasses childbirth and the aging process (Waetjen et al., 2018). Perceived personal failings, such as being overweight, confirmed the findings from Siddiqui and colleagues (2014) who noted that feelings of self-blame were commonly identified among Black, Arab, Hispanic and Asian women. However, the theological determinism of UI was particular to women from underrepresented groups. This has also been described as the origin and expected cure of the illness (Javanmardifard et al., 2021). These perceptions of UI promote the normalization of this chronic health issue and contribute to women disengaging with health services, preventing help-seeking behaviors (Wood, 2020). Therefore, health promotion strategies should be developed to target these perceptions and change the social narrative, which will ultimately modify and facilitate help-seeking behaviors. Female prevalence of UI is double that of men, but men are more likely to be referred to specialist care due to its potential relation with cancer. On the contrary, UI in women is often regarded as a minor issue (Altaweel & Alharbi, 2012; Strickland, 2014; Visser et al., 2014). In the United Kingdom, the publication of a Women’s Health Strategy has highlighted the importance of women-specific support and services (Department of Health and Social Care, 2022). Future UI research among women, especially in different ethnic groups, is urgently needed.
Another common theme discovered was the physical, psychological, and social impact of UI. Nowadays, incontinence remains an essential source of shame and stigma, and its consideration as a taboo subject is inherently human (Toye & Barker, 2020) and exists across different cultures (Wan et al., 2014). Throughout the decades, a wealth of evidence has highlighted the magnitude of the impact of UI on women’s psychological wellbeing and quality of life (Aoki et al., 2017; Mendes et al., 2017; Pizzol et al., 2021). The findings of this review coincide with reports found in the literature regarding discomfort, low self-esteem, anxiety, depression, mood disorders, forced isolation and alterations to lifestyle, and, as a result, deterioration of women’s personal, social and professional life (Farage et al., 2008; Felde et al., 2012; Melville et al., 2009; Tettamanti et al., 2013; van der Vaart et al. 2007). As identified in this review, sexual function is also another aspect of women’s health that is negatively affected by UI (Caruso et al., 2017) and, as an extension, marital and intimate relationships (Achtari & Dwyer, 2005; Liebergall-Wischnitzer, 2011; Lukacz et al. 2007). Evaluating and acknowledging the impact of UI on every aspect of women’s health, particularly around body image and sexuality, enhances the quality of care provided for women with UI (Kao et al., 2015). In order to provide holistic and meaningful interventions, the inclusion of partners in health promotion strategies is recommended (Senra & Pereira, 2015). Although this review revealed that some women find it unacceptable to discuss UI with their husbands and family members, a study undertaken in Iran found that most of the women who took part in the study disclosed the condition to their families, particularly with their husbands, as this matter also affected them directly. Nonetheless, cultural differences exist among Muslim countries (Hadizadeh-Talasaz et al., 2021). Additionally, special consideration should be taken when discussing sexual activity with women. Traditional patriarchal societies view sexual relations as an obligation of the woman with her husband, leaving women pressured to have sexual relationships (Amini & Mccormack, 2021).
The impact of culture and religion on UI and vice versa was also a recurring theme in this review. Culture and religion are believed to be inseparable since both concepts overlap and exert an influence on each other (Croucher et al., 2017). This struggle to differentiate between socio-cultural norms and religious rules, particularly in relation to the gender of the health professional, has also been described by Alqufly and colleagues (2019). Islam religious laws allow male doctors to examine and treat Muslim women in emergency events and when a female physician is not available so that their care is not compromised. Despite these allowances, strong individual cultural beliefs could lead to opposition. In these cases, non-judgmental and sensitive discussions should take place to acknowledge and accommodate cultural and religious preferences (Aldeen, 2007).
Other implications are the interactions between UI and religion. These interferences are consistent with current literature around cleanliness prior to prayers (Wells & Wagg, 2007) and can be particularly bothersome for Jewish and Muslim women (Treister-Goltzman & Peleg, 2018). Besides, some women believe that UI has spiritual attributions (Gjerde et al., 2013) and will be cured by praying (Hadizadeh-Talasaz et al., 2021). Although religion could be regarded as detrimental to women’s health, the use of faith as a coping strategy has been identified as a predictor of improved quality of life (Senra & Pereira, 2015).
Interaction of women with health services was the last emerging theme in this review. Preferences of female doctors over their male counterparts to discuss UI have been reported in a study among South Asian (Doshani et al., 2007) and Bangladeshi women (Wells & Wagg, 2007), although this preference is common to women regardless of their ethnicity (Siddiqui et al., 2014). Issues around language and communication barriers (Elstad et al., 2010), knowledge gaps in the physiology of the bladder and genital organs (El-Azab & Shaaban, 2010), health promotion, and illiteracy have also been highlighted in current literature. This situation leaves women with feelings of being unheard and jeopardizes help-seeking behaviors (Alshammari et al., 2020). Regarding lack of health literacy, a recent study in Canada concluded that immigrant women had less knowledge of pelvic floor disorders, including UI, compared with Canadian-born women (Roa et al., 2021). This highlights the need for targeted community interventions tailored to ethnically diverse groups, since a lack of knowledge of symptoms and treatment reduces the likelihood of seeking help (Washington et al., 2013). However, this lack of knowledge is reinforced by sub-optimal consultation and management skills in continence care, as ascertained by other studies (TuiSamoa et al., 2022; Yip & Cardozo, 2007; Zeznock et al., 2009). Consequently, this hidden problem is often underestimated by patients and professionals alike (Higa et al., 2008) and portrayed within a culture of secrecy (Toye & Barker, 2020). To avoid these inadequate interactions, education for patients and health professionals and early detection and management is recommended (Alshehri et al., 2022). Efforts should also be made to empower women throughout their life span, raise awareness and promote a culture of self-knowledge and education on the pelvic and genital areas to embrace normality and destigmatize these parts of the human body (Pintos-Díaz et al., 2019).
This review has highlighted the importance of considering SDH when professionals provide health care to women experiencing UI. This broader context is vital to understanding the influence of non-health-related factors on well-being and illness. The health of a population can only be fully understood after considering the cultural and religious factors that influence people’s health attitudes and behaviors (Rizk & El-Safty, 2006). In male-dominated cultures, women’s roles and health behaviors are shaped by religion (El-Saft, 1992, 2004). Often, attitudes toward women’s health, pregnancy, and childbirth are “necessarily rooted in the broader milieu of culture” (Rizk & El-Safty, 2006).
This review has focused on adult non-pregnant females, but current scientific literature suggests that childbearing women experience UI similarly. Perinatal incontinence is often normalized (Avery et al., 2015), seen as part of women’s lives (Melville et al., 2008), and a source of stigma, shame (Israfil-Bayli et al., 2015), and loneliness (Brett, 2021). Women’s lack of understanding of bladder health is reinforced by professional neglect and lack of direct inquiry into urinary symptoms, as newborns’ health is often prioritized over women’s wellbeing by health providers and women themselves (Gutiérrez et al., 2019). An amalgamation of professional lack of knowledge and embarrassment, alongside women’s unwillingness to disclose incontinence issues, has also been described during and after pregnancy (Williams et al., 2003). Moreover, the media’s negative impact on the normalization of UI after pregnancy has also been described as encouraging the use of pads instead of seeking help (Wagg et al., 2017). Given that women can experience UI throughout their life course and the subsequent repercussions on their lives and those around them, this topic requires further attention from professionals, women, researchers, and governing bodies.
Societies are becoming increasingly multicultural due to global migratory movements. This multicultural reality leads health professionals to communicate and provide care for women and families from various cultural backgrounds (Belintxon & López-Dicastillo, 2014). These encounters often face difficulties derived from cultural and linguistic factors, health literacy, socio-economic disadvantages, prejudices, and stereotypes of health providers (Atanga & Ayong, 2017; Belintxon & López-Dicastillo, 2014), as echoed in this review. In consequence, it is essential to embrace the influence of culture on UI by promoting cultural competence education for health professionals to tackle poor health outcomes due to health disparities and structural inequalities (Horvat et al., 2014). Finally, although women across all ethnic groups might show similarities in their experiences (TuiSamoa et al., 2022), treating women from underrepresented groups like a homogeneous group should be avoided. Barriers specific to communities exist as a result of SDH, and therefore, personalized care approaches must be sought.
Implications for Practice and Recommendations
This systematic review has the potential to raise awareness of the importance of SDH and the provision of holistic urinary continence care, particularly among women from underrepresented groups. Health providers have the social and professional responsibility of becoming culturally competent to reduce health inequalities and eliminate structural racism. This review also highlights the need for good quality research on female UI throughout women’s life span. More efforts should be placed on increasing the representation of minoritized ethnic groups in research studies to achieve a fairer distribution of resources and services. Robust mechanisms to report protected characteristics within studies and avoid treating underrepresented women as uniform groups is paramount.
Limitations
Despite a high occurrence of UI across ethnic groups, one limitation of this review is the scarce number of studies retrieved and included, and the lack of current studies on this topic. In addition, there was an overrepresentation of minoritized ethnic women from the Islam faith, and no studies focused on other ethnic groups, such as Black or women from other Asian backgrounds.
Regarding the limitations of the review process, several aspects should be taken into account. Only articles in English were included. In addition, only one person undertook the literature search and screened and reviewed potential studies. On one hand, the fact that the same author conducted all the steps of this review could confer consistency. On the other hand, there is also the potential that bias has been included at some point throughout the process.
Although this review of the literature has provided an insight into the experience of women from underrepresented groups living with UI, it has not been able to address the question of women from underrepresented groups with perinatal UI. There is a need to investigate the experiences of women from diverse ethnic backgrounds suffering from UI during and after pregnancy.
Conclusion
This systematic review explored the experience of women from underrepresented groups living with UI and identified SDH that influenced their experiences. The findings shed light on how cultural and religious factors significantly affect women’s experiences, health attitudes, and behaviors toward incontinence and the interaction with health care providers when presenting to health services. The physical, psychological, and social impacts of UI on quality of life might not be specific to ethnic groups, and the extent might vary according to socio-cultural beliefs and attitudes. Service users and professionals require adequate culturally competent health education to break the normalization cycle, support health promotion, and tackle health inequalities.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596231172205 – Supplemental material for The Experience of Women From Underrepresented Groups With Urinary Incontinence: A Systematic Review
Supplemental material, sj-docx-1-tcn-10.1177_10436596231172205 for The Experience of Women From Underrepresented Groups With Urinary Incontinence: A Systematic Review by Verónica Blanco Gutiérrez, Vanora A. Hundley and Susan Way in Journal of Transcultural Nursing
Footnotes
Acknowledgements
I would like to thank my supervisors, Professor Vanora Hundley and Professor Sue Way, for their patience, guidance, and dedication and for being an inspiration and role model for research midwives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I also would like to thank the Iolanthe Midwifery Trust for believing in me and funding my project. This systematic review was supported by an Iolanthe Midwifery Trust Award received/awarded to the principal author.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.