
Abstract
Introduction:
This narrative review identifies barriers and facilitators influencing breast cancer screening among Arab Muslim immigrants and refugees. Low participation rates create health inequities in breast cancer screening among this population.
Method:
A systematic search of peer-reviewed empirical articles was performed. PRISMA, CASP, and MMAT checklists were used to appraise the studies.
Results:
Results include 3 themes: individual, health care system and health providers, and cultural factors.
Discussion:
Lack of fluency in the new country’s language, lack of knowledge, and poor exposure to breast cancer screening may contribute to the Arab Muslim women’s vulnerability to undiagnosed or delayed breast cancer diagnosis.
Keywords
Introduction
Breast cancer represents the most frequent neoplasm affecting women globally (Ferlay et al., 2018). Breast cancer has now surpassed lung cancer in terms of incidence and mortality rates (Bray et al., 2018) and one in every eight women faces breast cancer during their lifetime (World Health Organization [WHO], 2021). Although breast cancer is not preventable, risk factors can be decreased to reduce morbidity and mortality (Azubuike et al., 2018; Chetlen et al., 2016; Coleman, 2017). Women living in sub-Saharan African countries present the highest mortality rate of breast cancer globally (Karbakhsh, 2021).
Breast Cancer Among Arab Muslim Immigrant and Refugee Women
Socio-cultural factors influence Arab Muslim immigrant and refugee women’s breast awareness and explain low participation in early screening programs (Elobaid et al., 2016; Gray et al., 2017; Racine et al., 2021a, 2021b; Vahabi et al., 2017; Vrinten et al., 2016). A recent study indicates that health literacy and language barriers are the most important factors limiting access to breast and cervical cancer prevention among Arab Muslim refugees in the United States (Siddiq et al., 2020). Women’s gender roles and the lack of open discussion about breast cancer may generate shame and taboos among Arab Muslim women (Siddiq et al., 2020). For some women, getting cancer is a matter of destiny, which ultimately decreases breast screening rates (Banning & Hafeez, 2009; Salman, 2012; Shirazi et al., 2015; Zorogastua et al., 2017). Although Islam supports women’s duty to take care of their health (Siddiq et al., 2020), religious beliefs may create fatalism, placing breast health beyond women’s locus of control (Pinchas-Mizrachi et al., 2021). Beliefs in modesty, women’s willingness or tolerance to being physically touched, and a male provider may decrease participation in breast cancer screening and create embarrassment or fear of clinical breast examination and mammography (Siddiq et al., 2020). The fear of pain from the mammogram and of the results negatively impact breast cancer screening practices. Lack of understanding of the receiving country health care system and lack of linguistic, geographic, and financial accessibility reduce breast cancer screening (Al-Amoudi et al., 2015; Elobaid et al., 2016; Islam et al., 2017; Kamaraju et al., 2019; Mellon et al., 2013; Raymond et al., 2014; Saadi et al., 2012, 2015; Wang et al., 2019; Zorogastua et al., 2017). Lack of health care providers’ support and discrimination within the health care systems further decrease breast cancer screening among Arab Muslim immigrant and refugee women (Racine et al., 2021b; Tackett et al., 2018).
Despite medical and technological advancement, health disparities related to breast cancer exist (Gray et al., 2017; Karbakhsh, 2021), and these inequities likely affect Arab Muslim refugee women due to disruptions in their home countries and lack of breast health care in refugee camps (Al-Smadi et al., 2017; Bakkal Temi et al., 2017; Bowser et al., 2017; Gammouh et al., 2015; Mansour et al., 2018; Samadi, 2017; Siddiq et al., 2020). Low rates of breast cancer screening in Muslim native and refugee women have been documented in Gulf countries, Jordan, Lebanon, Turkey, and other countries in the Arab world (Al-Amoudi et al., 2015; Donnelly & Hwang, 2015; El-Arnaout et al., 2019; Elobaid et al., 2016; Gammouh et al., 2015; Hashim et al., 2018; Kamimura et al., 2018; Mansour et al., 2018; Siddiq et al., 2020). Low survival rates and late-stage diagnosis have been reported in Libya and Malaysia (Coleman, 2017). More than half of women in the Middle East present lymph nodes indicating an advanced stage of the illness coupled with a low survival rate (Ghoncheh et al., 2015). Donnelly and Hwang (2015) mentioned that Qatari women are more likely to develop breast cancer at a younger age than Western women.
Researchers suggest that Arab Muslim refugee women who migrated to Western Europe and North America are likely to present poorer health outcomes when it comes to breast cancer than women in the general population (Abolfotouh et al., 2015; Saadi et al., 2015; Salman, 2012; Shirazi et al., 2015; Tackett et al., 2018; Vahabi et al., 2017). Increased migration to Western nations may increase breast cancer morbidity as Arab Muslim refugee women present minimal exposure to breast cancer screening programs in their home countries coupled with a lack of understanding of preventive health care (Karbakhsh, 2021; Mansour et al., 2018; Siddiq et al., 2020). Studies in Turkey, Lebanon, and Jordan indicated that the increased influx of Syrian refugees added pressure on these countries’ health care systems affecting access to preventive and curative services (El-Arnaout et al., 2019). Finally, resettlement challenges like learning a new language and seeking employment may impinge breast cancer screening as health promotion and prevention may not be seen as a priority compared to social and economic integration activities (Siddiq et al., 2020).
Method
Design
This integrative review focused on examining the barriers and facilitators of breast cancer screening in Arab Muslim immigrant and refugee women. The review relies on a narrative approach to synthesize the data (Popay et al., 2006). The research question was:
Search Methods
A comprehensive systematic search of English-language, original empirical peer-reviewed papers was performed from January 2000 to July 2021. We searched MEDLINE, CINAHL, Embase, Cochrane Library, Web of Sciences, and PubMed databases. Search terms included “Breast Cancer Screening” and “Refugee.” Then, we added “immigrant,” “Muslim,” “women,” “refugee,” and “Islam” as keywords. Cross-sectional, descriptive, randomized controlled trials, qualitative, and mixed-methods design studies were retrieved. We excluded non-empirical and theoretical papers, editorials, gray literature, letters to the editor, and conference abstracts. The initial database searches yielded 231 records. The Medline search yielded 58 peer-reviewed articles that met the inclusion criteria. Out of these 58 publications, three were duplicates, and 18 did not meet the inclusion criteria. A total of 37 articles was retrieved from Medline. The CINAHL search retrieved 139 articles. Out of 139 articles, 11 were duplicates, 125 were excluded, and three were selected. The PubMed search produced 34 results, but 11 articles were duplicates, 21 were rejected, and two were retrieved. Three articles were retrieved through a manual search. Figure 1 illustrates the process of selection using Preferred Reporting Items for Systematic Reviews and Meta-Analysis diagram (PRISMA) (Moher et al., 2009). (Figure 1 PRISMA Flowchart)
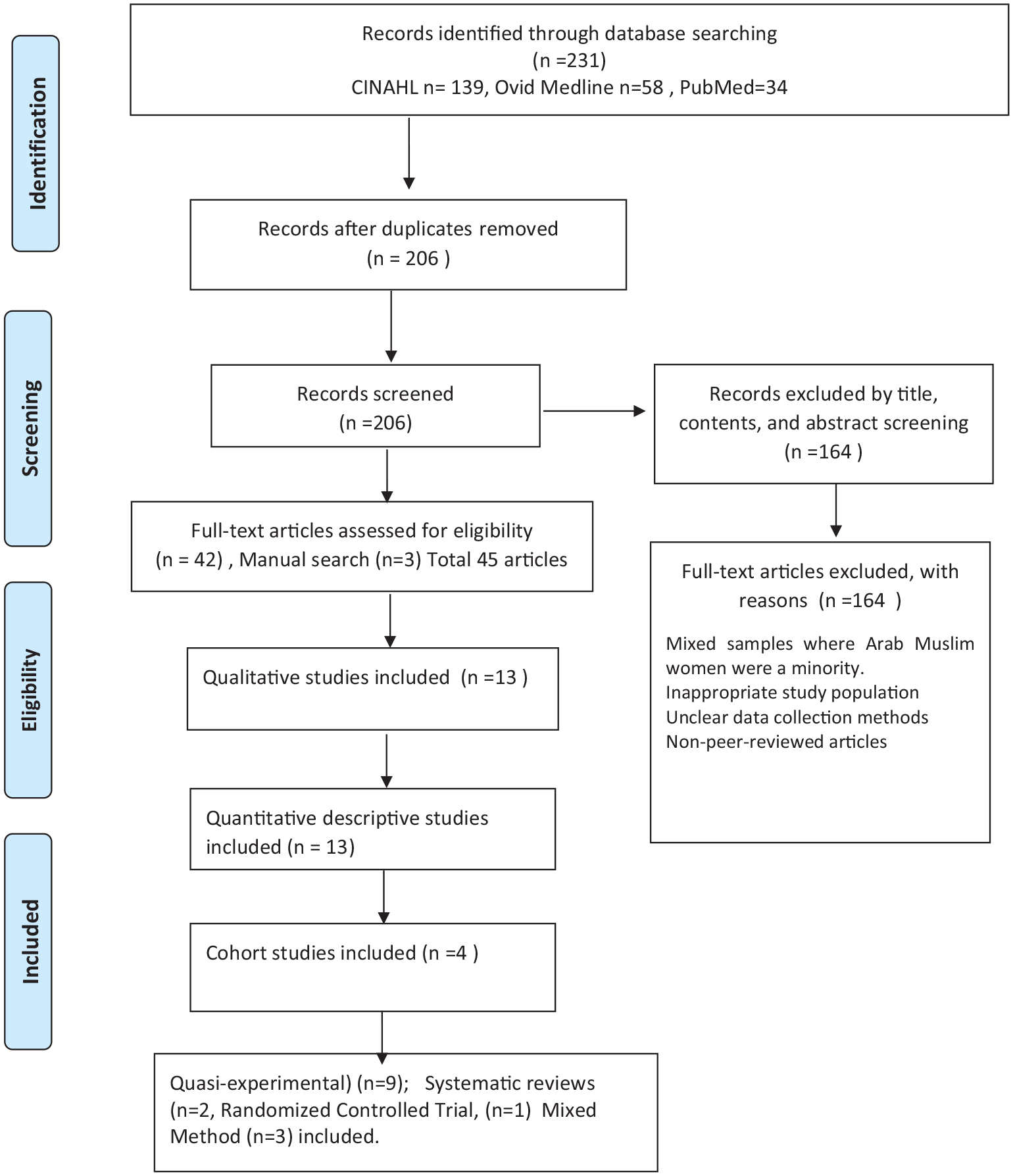
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Flowchart of Study Selection
Appraisal of the Studies
We used the Critical Appraisal Skills Program (CASP) checklists (Critical Appraisal Skills Programme, 2020) and the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018) to appraise the quality of the studies. CASP provides various checklists to effectively assess a range of studies using a ranking system to ensure the quality and rigor of the studies. A positive answer to any question on the CASP checklists was worth one point, and a negative response or a zero score was given if the answer was unclear.
The Mixed Methods Appraisal Tool (MMAT) Version 2018 (Hong et al., 2018) was used to appraise the quality of the three mixed-method studies. The MMAT starts by asking two screening questions: 1) Are there clear research questions; and 2) Do the collected data address the research questions? As these three studies met the screening questions, we assessed the five statements for mixed-method studies (Hong et al., 2018). A yes response was worth 1 point, while a no or cannot tell answer was assigned zero. This scoring scheme is similar to the one we applied with CASP checklists to maintain consistency. The two team members participated in the quality appraisal of the studies. Disagreements were solved through consensus.
Data Extraction and Synthesis
The review relies on a textual approach to data synthesis (Popay et al., 2006). The two team members read the articles and extracted the data. A synthesis table was used to organize and critique the extracted data into meaningful units of analysis (Pinch, 1995). Study title, author, journal, year of publication, purpose, research questions, methodology, data collection, statistical tests used, results, and conclusions were extracted (Table S1). We used thematic analysis to interpret the findings.
Results
Search Results
Forty-five publications met the inclusion criteria for the review. The characteristics of the studies are presented in Table S1. Thirty-one studies (69%) were conducted in the United States of America, nine (20%) in Canada, four (9%) in the United Kingdom, and one study (2%) in Turkey. In terms of study designs, 13 (28.9%) were qualitative, 9 (20%) quasi-experimental, 8 (18 %) descriptive quantitative, 5 (11%) cross-sectional, 4 (8.9%) retrospective cohort design, 3 (6.6%) mixed methods, 2 (4.4%) systematic reviews, and 1 (2.2%) randomized controlled study.
Nine studies guided by a quasi-experimental design were retrieved (Dunn et al., 2017; Gondek et al., 2015; Kamaraju et al., 2018, 2019; Padela et al., 2018, 2019; Percac-Lima et al., 2012, 2013; Pratt et al., 2020). These studies described interventions to promote breast cancer screening in Arab Muslim immigrant or refugee women. A mean score of 5.89 out of 10 was assigned to quasi-experimental studies indicating quality but with some limitations related to lack of reporting of effect sizes and experimental conditions and lack of generalizability.
Thirteen qualitative studies were retrieved (Al-Amoudi et al., 2015; Ayash et al., 2011; Banning & Hafeez, 2010; Islam et al., 2017; Kawar, 2013; Mellon et al., 2013; Padela et al., 2016; Racine et al., 2021a; Raymond et al., 2014; Saadi et al., 2012, 2015; Shirazi et al., 2013, 2015). Qualitative studies investigated barriers and facilitators related to breast cancer screening, while others focused on Arab Muslim immigrant and refugee women’s beliefs and attitudes about screening practices. Qualitative data were collected through focus groups, face-to-face and telephone interviews. A mean score of 9.54 was compiled for the qualitative studies indicating a very high quality of the selected studies.
Three mixed-method designs were retrieved (Banning & Hafeez, 2009; Wang et al., 2019; Zorogastua et al., 2017). Each mixed-method study scored 5 out of 5 statements supporting the robustness of the methodology and the trustworthiness of the results. Thirteen descriptive and cross-sectional quantitative studies documented predictors of breast cancer screening among Arab Muslim women (Alatrash, 2020; Hasnain et al., 2014; Jaffee et al., 2021; Kamimura et al., 2018; Kobeissi et al., 2014; Lofters et al., 2018; Padela et al., 2015; Racine et al., 2021b; Rashidi & Rajaram, 2000; Salman, 2012; Schwartz et al., 2008; Shirazi et al., 2006; Szczepura et al., 2008). Quantitative data were collected through written or telephone surveys and follow-up questionnaires. Quantitative descriptive and cross-sectional studies received a mean score of 8.77. This score points to the high quality of the selected studies and confidence in the validity of the results.
A randomized controlled study (Erenoglu & Sozbir, 2020) scored 5 out of 11. This study was included as it met the criteria of a straightforward research question, randomization, and the value and impact of the study. The effect size, generalizability, and costs/benefits ratio were not mentioned, decreasing the score. Two systematic reviews (Bowser et al., 2017; Schoueri-Mychasiw et al., 2013) were retrieved and scored 9 out of 10 points, indicating a very high quality of the findings. Four studies involving a retrospective cohort design (Lofters et al., 2019; Price et al., 2010; Vahabi et al., 2016, 2017) were selected and scored 9 out of 10 points on the CASP cohort checklist. This score indicated a very high quality of the research and confidence in the results and the findings’ applicability in practice.
The number of subjects included in the samples varied from 12 (Islam et al., 2017) to 238 (Vahabi et al., 2017). Thematic analysis was used to analyze and synthesize the data (Braun & Clarke, 2006). Thematic analysis generated three themes: (a) Individual factors, (b) health care system and health providers’ factors, and (c) cultural factors.
Theme 1: Individual Factors
Individual factors include personal barriers and facilitators affecting the uptake of breast cancer screening practices of Arab Muslim immigrant and refugee women. Language and education, time constraints, breast cancer beliefs, and contextual facilitators are included as subthemes.
Language and Education
Education constitutes both a barrier and a facilitator of BCS in Arab Muslim women (Banning & Hafeez, 2009; Shirazi et al., 2006). Women’s lack of knowledge and lack of awareness about breast cancer represent significant individual barriers influencing breast cancer screening behaviors (Al-Amoudi et al., 2015; Banning & Hafeez, 2009, 2010; Padela et al., 2015; Shirazi et al., 2006, 2013; Szczepura et al., 2008; Zorogastua et al., 2017). Limited proficiency in the receiving country’s language and low literacy affect the uptake of breast cancer preventive practices (Racine et al., 2021a).
Time Constraints
Issues of time, geographic accessibility of the clinics, lack of transportation, and family and child care commitments constrained Arab Muslim women’s access and participation in breast cancer screening practices (Kamaraju et al., 2018; Saadi et al., 2015; Zorogastua et al., 2017). More urgent priorities like searching for employment, learning the language, and child care may affect breast cancer screening practices (Wang et al., 2019).
Breast Cancer Beliefs
Several studies indicated that Arab Muslim women’s health beliefs affected breast cancer screening behaviors. For instance, self-efficacy, perception of risk (susceptibility to breast cancer), perceived importance of breast self-examination (BSE), perceived importance of mammography, and intention to be screened positively relate to active participation in screening activities (Hasnain et al., 2014; Islam et al., 2017; Price et al., 2010; Zorogastua et al., 2017). Studies using the Health Belief Model reported that perceived seriousness of breast cancer and health motivation were associated with increased screening behaviors among Arab American women (Schwartz et al., 2008; Zorogastua et al., 2017). Perceived benefits of prevention, perceived seriousness of the illness, health motivation, higher level of education, confidence, and skills in performing breast self-examination (BSE) correlated with increased awareness of breast cancer risks (Shirazi et al., 2006). The fear of negative findings (Kamaraju et al., 2018), fear of pain during the procedure (Raymond et al., 2014; Saadi et al., 2012, 2015; Zorogastua et al., 2017), beliefs about cancer (Mellon et al., 2013), fatalism (Al-Amoudi et al.,2015) and stigma contributed to reduced screening (Raymond et al., 2014).
Contextual Factors
Contextual factors have a significant impact on women’s mammography use. Having a higher knowledge about breast cancer impacts Arab Muslim women’s mammogram uptake (Kobeissi et al., 2014), the same as having a relative who presented breast cancer (Padela et al., 2015). Racine et al. (2021b) found that Muslim Arab refugee women with family responsibilities such as looking after children and other relatives at home had a higher mammography rate. In addition, Arab Muslim women who realized the importance of mammography had more screening (Hasnain et al., 2014). Media, magazines, and newspapers indirectly increased women’s knowledge on breast cancer by increasing awareness of the issue and may lead to increased participation in screening programs (Banning & Hafeez, 2009, 2010).
Theme 2: Health Care System and Health Care Providers’ Factors
Health Care System
Breast cancer screening practices involve interactions with the receiving country’s health care system and health care professionals. Years of residence in the receiving country, degree of acculturation, and citizenship influence Arab Muslim women’s access to breast preventive services (Hasnain et al., 2014; Islam et al. 2017; Kamaraju et al., 2019; Kawar et al., 2013; Lofters et al., 2019; Padela et al., 2015; Wang et al., 2019; Zorogastua et al. 2017). Exposure and participation in preventive breast cancer programs in the home country were likely to affect post-resettlement experiences with the receiving country’s health care system. Mellon et al. (2013) indicated that family experiences of discrimination with the receiving country’s health care system affected Arab American women’s breast cancer behaviors. Religious discrimination within the health care system constituted another obstacle to clinical breast examination and mammograms (Padela et al., 2015).
Health Care Providers
However, guidance and support of health care providers facilitated access and utilization of breast cancer preventive care (Kamaraju et al., 2018). Jaffee et al. (2021) underlined that a lack of providers’ support negatively affects Arab Muslim women’s BC screening behaviors and increases women’s mistrust of health care professionals. Al-Amoudi et al. (2015) indicated that Somali immigrant women who did not receive any recommendation for BCS from their physician negatively affected breast cancer behaviors. Bowser et al. (2017) reported statistically significant relationships between physician gender and breast cancer screening practices among Arab Muslim women from the Middle East and North African countries. Ability to speak Arabic and preferences for health care providers of similar religious backgrounds or female physicians or nurses play a crucial role among Arab Muslim immigrant and refugee women (Banning & Hafeez, 2009; Racine, 2021a; Rashidi & Rajaram, 2000; Raymond et al., 2014; Zorogastua et al., 2017).
Health Care System and Health Care Providers’ Facilitators
Access to publicly funded health care systems facilitated breast cancer screening practices (Bowser et al., 2017; Islam et al., 2017). Having health insurance and access to a primary physician increased women’s access to mammography (Padela et al., 2015). Trusting relations and communications with health care providers were fundamental in supporting Arab Muslim immigrant and refugee women’s use of mammograms (Bowser et al., 2017). Studies showed that Arab Muslim immigrant and refugee women preferred female physicians from the same ethnocultural groups and a provider able to speak Arabic (Kamimura et al., 2018; Lofters et al., 2018; Padela et al., 2016; Saadi et al., 2012; Vahabi et al., 2016, 2017). Appointment reminders and personal contact from health providers facilitated breast cancer screening (Banning & Hafeez, 2009; Rashidi & Rajaram, 200; Raymond et al., 2014; Saadi et al., 2015).
Theme 3: Cultural Factors
This theme includes cultural beliefs and facilitators that may affect Arab Muslim immigrant and refugee women’s breast screening practices (Alatrash, 2020; Racine et al., 2021a; Zorogastua et al., 2017). The embarrassment of revealing breasts represented obstacles among Arab Muslim women in Michigan (Alatrash, 2020). Arab Muslim women may present shyness, modesty, and embarrassment in their home countries and abroad due to the belief that breasts must be hidden (Abolfotouh et al., 2015; Banning & Hafeez, 2009; Elobaid et al., 2016). Stigma about cancer creates barriers affecting Arab Muslim women’s breast awareness and participation in breast cancer screening activities (Racine et al., 2021b; Zorogastua et al., 2017).
Some traditional beliefs affected women’s views toward breast cancer screening (Al-Amoudi et al., 2015; Islam et al., 2017; Padela et al., 2016, 2019; Shirazi et al., 2013). Kawar et al. (2013) reported that embarrassment, family relationships, and traditional healers’ consultations decreased motivation to seek breast cancer preventive care. Religious beliefs might decrease motivation to screening. A few women thought that breast cancer came from divine intervention and that prayers can help cope with illness (Hashim et al., 2018). Fatalistic attitudes were among the most frequently mentioned cultural barriers in Arab Muslim immigrant and refugee women (Al-Amoudi et al., 2015).
Cultural Facilitators
The literature indicates that gender, language, and religion facilitate breast cancer screening education and uptake among Arab Muslim immigrant and refugee women. Eight quasi-experimental intervention studies focused on promoting breast cancer screening in Arab Muslim immigrant or refugee women (Ayash et al., 2011; Dunn et al., 2017; Erenoglu & Sozbir, 2020; Gondek et al., 2015; Kamaraju et al., 2018; Padela et al., 2018, 2019; Percac-Lima et al., 2012, 2013; Pratt et al., 2020). Educational interventions consisted of education programs or programs combined with navigation assistance, group discussions and messages, culturally appropriate educational materials, and video presentations. Individual interventions with specific attention to gender and language significantly decreased breast cancer inequities among Arab American immigrant women in New York City (Ayash et al., 2011) and in Bosnian and Somali Muslim refugee women in Boston (Percac-Lima et al., 2013). Culturally or religiously congruent interventions used bilingual or bicultural health educators and were conducted in mosques and other socio-cultural organizations.
Discussion
Our results underline that knowledge, language, gender, traditional beliefs, and health care providers’ characteristics can act as barriers and facilitators to Arab Muslim immigrant and refugee women’s breast cancer screening practices. Lack of knowledge on breast cancer, minimal formal education, fatalism, and stigma are significant individual barriers decreasing breast cancer screening. Lack of time due to resettlement also negatively impacts breast cancer screening. Lack of fluency in English and a poor understanding of the receiving’s country health care systems affect access to care and programs. Health care providers’ lack of cultural competency negatively affects Arab Muslim immigrants’ and refugees’ attitudes and behaviors toward breast cancer screening. A geographically and financially accessible health care system, the presence of culturally and religiously tailored educational strategies, and health care professionals’ support are likely to influence Arab Muslim immigrant and refugee women’s breast cancer screening practices positively. Our results indicate the need to develop and implement culturally competent health promotion interventions. As reported in recent studies, education programs must target non-Muslim health care providers to decrease Arab Muslim women’s mistrust and perceptions of ethnocentrism and racism (Jaffee et al., 2021; Racine et al., 2021b). Education programs positively impacted Syrian refugee women’s breast awareness (Erenoglu & Sozbir, 2020) and intentions to screen (Pratt et al., 2020). Religiously tailored mosque-based interventions targeting beliefs impinging mammography uptake improved mammography rates (Padela et al., 2018, 2019). Culturally tailored and language-concordant navigator programs increased mammography screening rates among Muslim refugee women (Percac-Lima et al., 2012). Utilizing a health educator of the same ethnic group reduces cultural, linguistic, and health care barriers (Milenkov et al., 2020).
Implications for Nursing Practice and Research
Our review highlights the need to specifically address gender, language, and cultural and religious beliefs (Saadi et al., 2012, 2015). Breast cancer awareness and education must occur early in the resettlement process to develop or maintain health promotion behaviors. Arab Muslim immigrant and refugee women present knowledge and language barriers and time constraints related to post-resettlement activities, collaborations with religious or community leaders, and settlement agencies represent the cornerstone of the breast cancer prevention programs. This review indicates the urgent need to tailor preventive interventions to improve breast cancer screening among Arab Muslim immigrant or refugee women. Interventions should enhance women’s knowledge, skills, and confidence, toward breast screening while addressing religious and cultural factors such as fears, fatalism, stigma, and taboos. Nurses should not hesitate to rely on interpreters and be aware of the resettlement issues affecting Arab Muslim women’s access to breast cancer screening activities. Nurses must be knowledgeable about time constraints and understand that breast cancer early screening may not be a post-resettlement priority. Future research should design and test culturally sensitive interventions for this population of women who may be vulnerable due to pre-and post-resettlement conditions.
Limitations
Though we conducted an extensive literature search, we only retrieved articles in English. Most studies used self-reports to assess women’s breast cancer screening practices introducing potential biases. Several studies collapsed Arab Muslim immigrants and refugees into one category, obfuscating the specific needs of refugee women. The strength resides in capturing empirical studies beyond North America to include Turkey, Lebanon, and Jordan.
Conclusion
Addressing Arab Muslim refugee women’s lack of knowledge on breast care and increasing early exposure to breast cancer screening is recommended in the early stage of resettlement. Culturally adapted and religious-based interventions delivered in Arabic represent promising avenues to increasing breast cancer screening and avoiding late-stage diagnosis.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596221085301 – Supplemental material for Barriers and Facilitators Influencing Arab Muslim Immigrant and Refugee Women’s Breast Cancer Screening: A Narrative Review
Supplemental material, sj-docx-1-tcn-10.1177_10436596221085301 for Barriers and Facilitators Influencing Arab Muslim Immigrant and Refugee Women’s Breast Cancer Screening: A Narrative Review by Louise Racine and Isil Isik Andsoy in Journal of Transcultural Nursing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding provided by Sigma Theta Tau International and the Canadian Nurses’ Foundation to the first author. The second author was funded by The Scientific and Technological Research Council of Turkey (TUBITAK).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.