
Abstract
Introduction:
Despite the importance of compassionate leadership in health care, many of the existing publications do not account for the effect of culture. The aim of this study is to explore the views of nursing and midwifery managers from different countries in relation to the definition, advantages, and importance of compassion.
Methodology:
A cross-sectional, descriptive, exploratory online survey was conducted across 17 countries, containing both closed and open-ended questions. Data from N = 1,217 respondents were analyzed using a directed hybrid approach focusing only on qualitative questions related to compassion-giving.
Results:
Four overarching themes capture the study’s results: (1) definition of compassion, (2) advantages and importance of compassion for managers, (3) advantages and importance of compassion for staff and the workplace, and (4) culturally competent and compassionate leadership.
Discussion:
Innovative research agendas should pursue further local qualitative empirical research to inform models of culturally competent and compassionate leadership helping mangers navigate multiple pressures and be able to transculturally resonate with their staff and patients.
Introduction
Leadership in health care is recognized as a necessity to ensure high-quality care, embody support for staff, and establish working environments that prioritize people over rules, regulations, and hierarchies (West et al., 2015). It is argued that compassionate leadership has a positive impact on “patient experience, staff engagement and organisational performance” (Bolden et al., 2019, p. 2). In multicultural societies, cultural competence is a key aspect of leadership, as this is essential in achieving the culturally and linguistically competent patient services that are necessary to reduce health care inequalities; and because the expression of compassion is culturally mediated, compassionate care must necessarily also be culturally competent. Culturally competent compassion in health care has been defined as a human quality of understanding the suffering of others and wanting to do something about it using culturally appropriate and acceptable caring interventions which take into consideration both the patients’ and the carers’ cultural background as well as the context in which care is given (Papadopoulos, 2018, p.2).
Furthermore, culturally competent and virtuous leadership is ethically founded on compassion, honesty, kindness, altruism, and cooperation (Papadopoulos, 2018).
Leadership and compassion are universal concepts. The art of leading people is a basic element in the organization of group activity in any human society (Lewis, 1974). Likewise, the emotional, cognitive, and behavioral responses that arise from empathizing with others’ suffering are evolutionarily linked to caregiving for offspring (Preston, 2013). Nevertheless, leadership and compassion are crucially shaped by culture (Chiao, 2017; Koopmann-Holm & Tsai, 2017). They require a complex orchestration of sets of embodied and acquired values in relation to emotional experience and expression, power, social norms, and morality—which all pertain to distinct cultural self-definitions (Kitayama, 2002).
Available evidence on the interplay between culture and leadership has mainly built on theorizing by Triandis (1988) and Hofstede (1984). The constructs of individualistic and collectivist cultures remain relevant and have benefited from a number of refinements, for example, the qualification of horizontal and vertical individualism and collectivism to account for the level of acceptance of social hierarchy (Singelis et al., 2016); and the formulation of loose and tight cultures, which captures the level of rigidity of social norms (Gelfand et al., 2011). In the largest study on culture and leadership, the GLOBE study, several dimensions are combined to identify cultural clusters correlating with leadership styles, such as team-oriented, participative, autonomous, and humane (Dorfman et al., 2004). The humane leadership style is based on compassion, generosity, and concern for others’ well-being (Kabasakal & Bodur, 2004). Building on the GLOBE’s results, it has been maintained that the humane leadership style is a universal style, rather than specific to Western cultural milieu. In fact, similar cultural concepts from Africa (e.g., Ubuntu and Harambee), and main religious traditions, such as Hinduism and Judaism, have been identified (Winston & Ryan, 2008). Other scholars have shown instead how humane leadership style varies a great deal from one country to another. Schloesser et al. (2012), for example, found that the humane leadership construct appeared to negatively correlate with countries’ welfare state but positively correlate with the value of agreeableness in a country.
Culture plays an important role in how compassion, as an emotional or cognitive process, is experienced and expressed, and in which supportive behaviors it should result (Koopmann-Holm & Tsai, 2017). Levine et al. (2001) conducted a study in 23 nations to examine how people responded to strangers needing help. They found that the Latino cultural script of simpatia—a concept assimilable to compassion and humanness—positively correlated with helping behavior. Advances in cultural neurosciences have shown that the experience of vicariously feeling others’ suffering can be modulated by cultural values (Chiao, 2017). In this sense, Cheon et al. (2011) demonstrated that in-group empathy is generally higher in hierarchical cultures, like the Korean one, than in egalitarian contexts, like the North American.
Finally, the transcultural concept of emotion, including empathy which is an important component of compassion, has been elaborated in cultural and psychological anthropology. Work conducted among peoples in the Pacific areas argued that emotions are not universal, but rather embedded into specific sociocultural processes (Lutz, 1988). Other studies have focused on the appropriateness of empathy in societies (e.g., Micronesian and Mayan) where secrecy and privacy are highly valued, and where empathic-like knowledge of others can be perceived as intrusion or attack (Groark, 2008).
Compassionate leadership has been increasingly studied and promoted in the health care sector (Papadopoulos, 2018; Martin & Heineberg, 2017; Worline & Dutton, 2017). The development of a Compassionate Leader Behavior Index (Shuck et al., 2019) is a recent advance in understanding and measuring compassionate leadership, but like much of the evidence discussed above, this does not deepen the cultural determinants of compassionate leadership, and how these affect culturally competent and compassionate leadership. Questions remain around how conceptions and behaviors associated with both leadership and compassion are held and expressed by people with different cultural backgrounds in their local worlds. Making sense of culture in compassionate leadership can also facilitate the use of culturally competent practice in health care, rooted in cultural awareness, sensitivity, and knowledge (Papadopoulos, 2006).
This article builds on the only model that includes the impact of culture in compassion-giving in health care (Papadopoulos, 2018). According to this model, specific characteristics of cultures are the result of environmental factors (place), historical factors (time), people’s existing values (socialization), and other unique factors, such as political and economic systems, group/ethnic conflict, and education, which will affect how compassion is understood and enacted. It could be argued that these characteristics form the collective programming of the mind that distinguishes the members of one group or category of people from others, which is how culture has been defined by Hofstede et al. (2010).
Research into the role of culture and the fostering of culturally competent and compassionate leadership in health care is at an embryonic stage. In this project, we acknowledge that the participants from each country may be a mixture of native and immigrant people. It has become apparent that global mobility of health professionals has resulted in multiethnic/multicultural workforces. This poses a challenge for those researching culture at an international level. For example, in our study, participants from the United Kingdom described themselves as Asian, Australian, Black Caribbean, British, Indian, Irish, or Japanese American. However, we also need to acknowledge that migrant health care workers over time adopt the organizational culture, and they also acculturate to the national culture of their host country. Due to these challenges, this study adopts the Hofstede et al. (2010) notion of national cultural identity.
Aims
This article focuses on the following three questions: (1) “How do you define compassion?” (2) “Can you list the advantages of giving compassion to staff?” and (3) “Can you explain why receiving compassion is important to you?” Participants were invited to provide examples from their own working environments in order to underpin their responses. Furthermore, this article aspires to contribute to the notion of culturally competent and compassionate leadership; therefore, the findings are discussed taking into account the participating countries’ culture and how this may influence the participants’ views about compassionate leadership.
Method
The design of this study is an exploratory, cross-sectional, descriptive, online survey using closed and open-ended questions. The full questionnaire is publicly available online from the research center website at www.cultureandcompassion.com/victcory/international-on-line-compassion-survey (Papadopoulos, 2019).
Sample and Data Collection
A snowball sampling method was used resulting in the selection of an international convenience sample of nursing and midwifery managers (total N = 1,217 across 17 countries). The demographic characteristics of the sample are presented in Table 1. Of the 17 countries, nine were from the European region (57% of whole sample), and of these, four consisted of Eastern European countries; four countries belonged to the Middle East region, and three from the Americas—of which two were from South America. One African country was represented. The main inclusion criterion was being a nurse or a midwife manager in a hospital, community, or educational setting. Data collection occurred between the end of November 2017 and the end of July 2018. Data were collected using the web-based electronic survey software Qualtrics. International research partners circulated the invitation letter containing the link to the questionnaire to colleagues. A minimum of 40 responses were to be collected from each country for it to be included in the final sample.
Key Characteristics of Participants From the 17 Participating Countries (Total N = 1,217).

Note. F = female, M = male, p = people.
Missing one value for gender, years of experience, and number of people managed.
Data Analysis
A directed hybrid approach of inductive and deductive thematic analysis was employed to analyze the responses to the selected open-ended questions (Fereday & Muir-Cochrane, 2006). This involved examining the survey responses line-by-line and grouping them into categories and themes, as described in Braun and Clarke (2006), with one researcher examining and coding, for several rounds of reviewing and refining the themes. Coding was discussed with the principal investigator during team meetings. In addition, a coding manual was produced providing a detailed audit trail of the process. The entire analysis was supported by NVivo Version 12 software.
Rigor
Several steps were taken to ensure the quality of the methods used in this study. First, survey questions were checked for clarity by members of the international team, and problems with translation that were detected were resolved. Second, the translation and back translation into English of the survey questionnaire, the invitation letter, and the qualitative data collected followed the World Health Organization guidelines (2016). The lead researcher had the responsibility to create the links to the online survey for each country, and all data were sent to the lead researcher for analysis. Methodological rigor in the analysis was also enhanced by involving several members of the U.K. research team in coding some of the raw data from one or two countries, and by regular team discussions.
Ethical Considerations
The study was approved by the Health and Social Care ethics subcommittee (No. 1477) of the School of Health and Education at the lead researcher’s university. Additionally, every researcher from all participating countries obtained ethical clearance from their respective university/health care organization authority where required. Potential participants received the link to the survey along with an invitation letter that explained the aim and procedures of the study; that participation was anonymous, confidential, and completely voluntary; and that answering the questions constituted consent to the study.
Results
Four overarching themes were derived from the analysis, and selected subthemes and quotes per each theme are presented in four tables as follows: (1) managers’ definitions of compassion (Table 2), (2) advantages and importance of compassion for managers (Table 3), (3) advantages and importance of compassion for staff and the workplace (Table 4), and (4) culturally competent and compassionate leadership (Table 5).
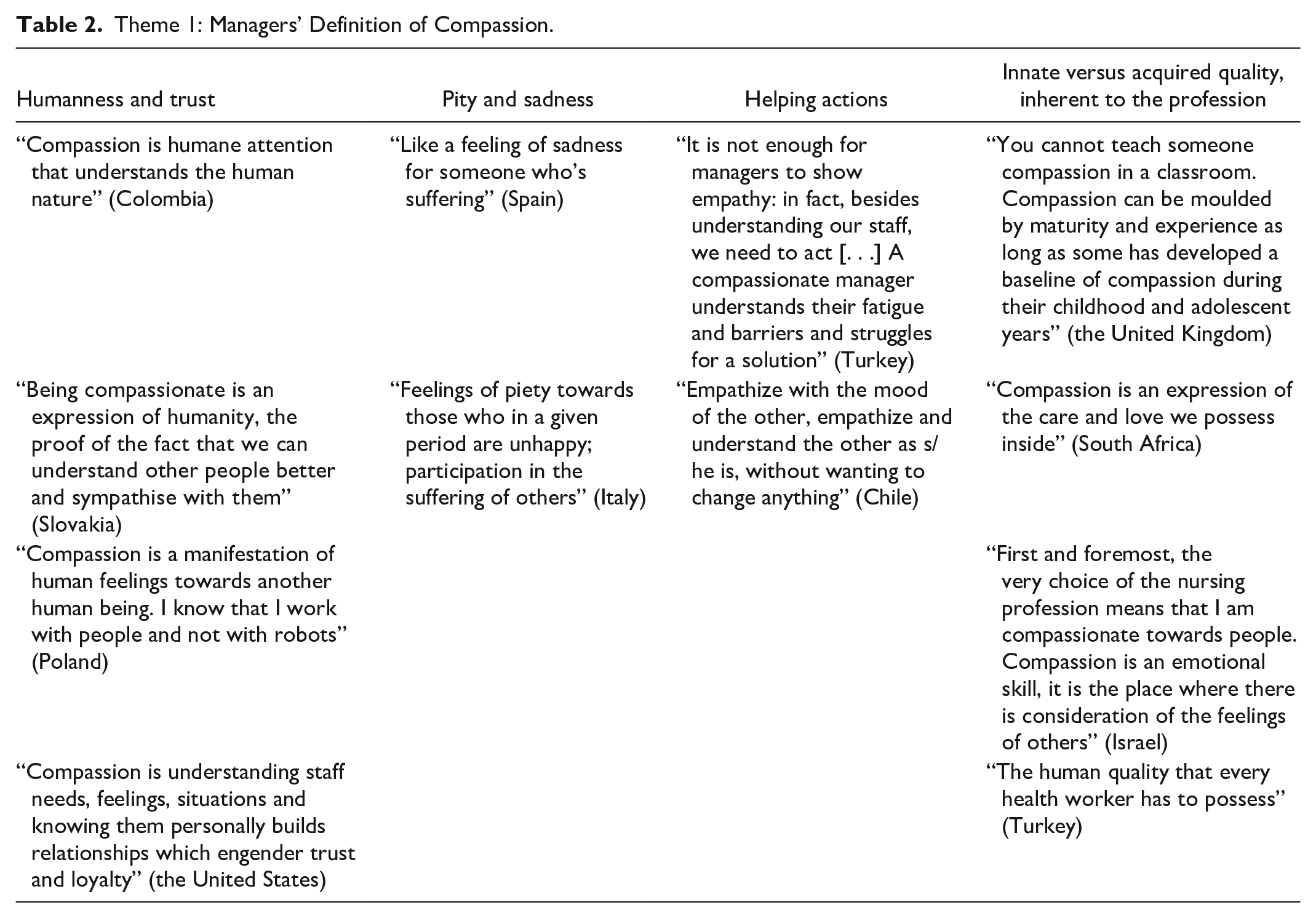
Theme 1: Managers’ Definition of Compassion.
Theme 2: Advantages and Importance of Compassion for Managers.

Theme 3: Advantages and Importance of Compassion for Staff and the Workplace.

Theme 4: Culturally Competent and Compassionate Leadership.

Note. PPD = personal and professional development.
Theme 1: Managers’ Definition of Compassion
Participants from all countries associated compassion with a virtuous quality; in particular, it was overwhelmingly associated with humanness. Another common characterization of compassion lies within the relational realm, with most managers highlighting a relationship between compassion, and trust and honesty. When conceived as a feeling or an emotion, compassion was sometimes defined in terms of pity, sadness, and feeling sorry due to empathizing with suffering staff. For some participants, feelings of compassion motivated and triggered helping actions. Some managers viewed compassion as an innate quality, others as something connected to upbringing and experience. Finally, a small proportion of participants defined compassion as inherent in the profession.
Theme 2: Advantages and Importance of Compassion for Managers
The advantages and the importance of compassion for managers were variously expressed by participants. For some, compassion and management are strictly interlinked, and others underline how compassion benefits managers directly, in terms of feeling valued and respected. Other managers emphasized how, by giving compassion to their staff, they in turn received understanding, support, and appreciation. Some participants highlighted the importance of being role models for their staff, and how compassion played an important part in their leadership style.
Theme 3: Advantages and Importance of Compassion for Staff and the Workplace
Manager–staff relationships informed by a compassionate approach become closer, more positive, and open. This results in a virtuous circle whereby compassion feeds into compassion, thus establishing a nurturing, positive environment in which managers are more approachable, staff feel more comfortable, and patients enjoy better care. Enhanced teamwork was also placed among the chief advantages of compassion-giving, because compassion helps foster harmonious, peaceful relationships; good communication; and a participatory, empowering approach in which nurses are listened to. Problem-solving, decision-making, and conflict- resolution were also seen as improving. Better performance and productivity in meeting organizational goals, on the one hand, and the improvement of the quality of care for patients, on the other, were also mentioned. Compassion is overall regarded beneficial for both managers and staff’s mental health, improving their professional life quality and satisfaction, while decreasing risk of burnout.
Theme 4: Culturally Competent and Compassionate Leadership
Being available to meet with their staff is an important element found across all countries, according to different leadership styles and to individual and cultural characteristics of members of staff. Advocating for their staff is expressed in terms of protecting them against inappropriate treatment that they may receive from patients or their relatives, and unprofessional treatment from other clinicians. Others expressed an attitude of general advocacy of the nurses’ role and their rights, based on knowing the staff and their situations. In countries where managers deal with highly multicultural teams, an open and accommodating attitude toward staff’s cultural backgrounds was especially commonly reported, also in relation to child care duties and health. Attention to personal and professional development has emerged in terms of encouraging training and the flourishing of the employee, and finally, a rich set of less tangible attitudes emerged from the managers’ responses, which was expressed in terms of participation, perspective taking, closeness and connection, and interest and active listening.
Discussion
Managers from all the participating countries defined compassion in terms of humanness, speaking to the universal dimension of compassion. The relationship between humane and compassionate health care that the participants expressed parallels conceptions put forward by the academic community (Papadopoulos, 2018; Crowther et al., 2013). In our study, managers from South America and the Philippines—two collectivist cultures, where in-group cohesion and a sense of a shared humanity appear higher (Oyserman et al., 2002)—have overwhelmingly emphasized how compassion pertains to the essence of being human. The attention to a humane approach, also expressed by Central–Eastern European managers can be read against the backdrop of the radical set of reforms in postcommunist health transitions (Safaei, 2012). These reforms have led to greater unemployment and uncertainty in the workplace (Bludau, 2014), and consequently, health care professionals may feel urged to appeal to a sense of humanity.
Compassion has been seen as functional in establishing a trustworthy manager–staff relationship, which was prevalent in the United States. The United States is a predominantly individualistic country, and it is widely accepted that employers focus on productivity and fear of litigation. It has also been reported that health care staff turnover rate has recently been alarmingly high (Nursing Solutions, 2019). These factors may explain managers’ desire to establish relationships with their staff which are informed by trust and honesty. On the other hand, the conflating of compassion with sadness and pity (which may or may not lead to supportive action) emerged in countries where traditional Christian Catholic values (e.g., Italy, Spain, and Colombia) are more strongly held.
The positive findings reported in this article could be viewed as a continuum. At one end is the emphasis on the self (the manager), moving through the benefits of compassion for the manager–staff relationship, staff well-being, and teamwork, and, finally, at the other end, are the broader benefits for the work setting. However, according to the culturally competent and virtuous compassion model proposed by Papadopoulos (2018), a number of negative factors can tip this delicate balance and turn the two ends of the continuum into toxic positions, with extreme self-interest/individualism at one end, and extreme collectivism at the other. Personal and professional pressures on managers can negatively influence their leadership styles resulting in increased self-centeredness or conversely, in creating a very tight collectivist work team, both of which are undesirable states. It is therefore important that managers are supported by their superiors and the staff in their teams to maintain a balanced culturally competent and compassionate leadership style.
Overall, these findings are consistent with findings on compassion satisfaction in nursing (Sacco & Copel, 2018), which alone may be located on the individualistic end of our continuum. In contrast, compassion flow (Tierney et al., 2017) appears to speak more to the collectivist end of the spectrum. The positive effect of compassion-giving to teamwork, which we found to be very prominent, is also consistent with the literature. This speaks to both the notion of “collective capability for compassion” (Lilius, Worline, et al., 2011) and to positive association between compassion-giving and work engagement (De Clercq et al., 2014). Finally, our evidence highlighted the crucial role of managers in establishing culturally competent and compassionate workplace cultures, which undoubtedly can influence the quality of patient care (Beardsmore & McSherry, 2017). Some of the culturally competent components and manifestations of compassion offered by our participants echo the compassion components reported by practicing nurses, such as giving time, being there, defending and advocating, and personalization (Papadopoulos et al., 2016, 2017). This suggests that compassion-giving is not drastically affected by the position one occupies in an organization. The findings reported in this article appear to support Shuck et al.’s (2019) assertion that displaying compassion is not dependent on the traditional leader–follower exchange and may not conform to traditional boundaries.
Cultural anthropologists, while neglecting compassion as such, have investigated the emotions linked to empathy (Hollan & Throop, 2008). Empathy, as compassion, implies a caring, concerned attitude and the acquisition of better understanding of the other—as our respondents have frequently highlighted—and contributes to make it a distinguished way of understansing people (Halpern, 2011). But it is possible for an empathic approach to be maintained even when understanding fails (Kirmayer, 2008), thereby making it a potent tool that can transcend differences in illness experiences, power positions, and cultural backgrounds and norms. If the cultural and political contexts influence the processes of meaning-making and the practices of compassion exchange, forms of caregiving are also transversal and transcultural. Compassion in management is increasingly recognized as a “trans-cultural source of wisdom” (Opdebeeck & Habisch, 2011).
Kleinman (2015) pointed out that “caregiving is relational and reciprocal” and can be conceived anthropologically as a “gift exchange,” which is “moral, emotional, and practical” (p. 240). This study is going one step further. Our findings suggest that compassion giving and receiving form a symbiotic transactional relationship, because a compassion giver always receives some compassion back, directly from the receiver or indirectly as self-growth, which may or may not be recognized immediately. Therefore, if compassion in general is viewed as a transactional act, it means that culturally situated, transactional compassion can be a beneficial and potent tool to transcend otherness, and ensure authentic caregiving, at all levels of the organization. The majority of the nursing and midwifery managers participating in this study have shown how compassion relates to the establishment of caring relationships that bear emotional investment and cultural resonance (Jones, 2005), as well as compassionate workplaces characterized by a focus on care, instead of productivity, and by flourishing relationships and collaborations. Transactional culturally competent compassion—as a quintessential nursing quality—sits at the core of transcultural nursing, and possibly even more poignantly with nursing and midwifery managers, who—as leaders—are particularly called on to be able to transculturally resonate with their staff and patients, organizational pressures, and national/global trends. Therefore, along with the novel conceptualization of compassion as a transactional act, this article also revitalizes the established idea of compassion as a potentially universal humane and professional tool that needs to be inseparable from cultural competence (Papadopoulos, 2006).
Strengths and Limitations
To our knowledge, this is the only qualitative exploration of how nursing and midwifery managers view, define, recognize, and practice culturally competent compassion (with a particular focus on the importance and advantages of compassion-giving). Also unique is the study’s secondary goal of improving our understanding around cultural determinants of compassion-giving among nursing and midwifery managers (which is reflected in the participatory, transnational design of the survey). Partners are pursuing further analysis of their own country’s data, with rich culturally and structurally situated analyses. This study is also of exceptional diachronic value as it constitutes a further tile (the first one being the previous international survey among nurses) in the construction of a broader theory of culturally competent and compassionate care, and how it can be studied. The study was also careful to incorporate a number of systematic measures to reduce bias in its analysis, such as adopting a hybrid approach, following systematic steps, and involving several researchers in the data analysis, which provided the necessary verification of the findings.
Regarding the study’s limitations, we acknowledge that the selection of the countries involved was dictated by the network of the coordinating U.K. research team, which accounts for the Eurocentric bias of the sample. The online survey design prevented the collection of empirical contextual data, and practical constraints limited the use of the literature in country languages. Due to the challenges that exist in the unravelling of the cultural values of participants in international studies, and our adoption of national cultures in the interpretation of this study’s data, our contribution to understanding how cultures inform compassion-giving should be viewed with caution.
Conclusion
The study of the generic and specific country cultural determinants affecting the views of compassionate leadership in health care needs expansion. Leaders sit at the intersection of multiple pressures and are required to transculturally resonate with their staff and patients, within complex sets of intersubjective contacts, organizational pressures, and national/global forces. The value placed on compassion by our participants has several implications:
Cultural values and leadership: Culturally intelligent (Rockstuhl et al., 2011) and compassionate leaders should have deep awareness of their own cultural values to account for the influence of their own culture on their leadership styles. Transcultural models and practices of ethical leadership (Eisenbeiß & Brodbeck, 2014) should be developed to establish nurturing health care working environments from which all stakeholders can benefit. Culturally specific models of leadership are to be framed within the pillars of transcultural and compassionate nursing, which are ethics, intercultural relations, sociopolitical systems, and human rights (Papadopoulos, 2006).
Building compassion into organizations: Strategies for developing culturally competent and compassionate health care leadership require a shift from the prevalent dehumanizing model of the organization as machine to a model of the organization as a complex and interconnected adaptive living system. An effort to “institutionalise compassion” (Lilius, Kanov, et al., 2011) and cultural competence should be adopted throughout the organization with collective holistic learning strategies and high levels of staff support and engagement.
The role of self-compassion: Providing training in coping and self-compassion strategies is an overdue imperative that will encourage nursing and midwifery managers to show compassion and to nurture the values that underpin professional codes of practice. The organization of transnational peer group events as occasion to reflect, self-help, and define good practices should be fostered.
An innovative research agenda in this field should pursue further multidisciplinary and local empirical research, with transnational collaborations. Finally, while always culturally situated, transactional compassion can be a potent tool to transcend otherness, and ensure authentic caregiving, at all levels of the organization.
Footnotes
Acknowledgements
We thank all the 1,217 participants who gave their time to complete the survey. We would like to additionally thank Sheila Ali, Syed Miah, and Dr. María José Morales Gázquez for their contributions to the data analysis process.
Author Contributions
Made a substantial contribution to the concept or design of the work; or acquisition, analysis, or interpretation of data: all authors
Drafted the article or revised it critically for important intellectual content: all authors
Approved the version to be published: all authors
Take public responsibility for appropriate portions of the content: all authors
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, and it was conducted on a voluntary basis, under the lead of the Research Centre for Transcultural Studies in Health at Middlesex University, London, the United Kingdom.
Ethical Approval
The study was approved by the Health and Social Care ethics subcommittee (No. 1477) of the School of Health and Education at the lead researcher’s university.