
Abstract
Introduction:
Labiaplasty is increasingly sought for aesthetic and functional reasons, though traditional surgical methods carry risks. Helium plasma radio frequency (RF) offers a minimally invasive alternative for labial rejuvenation.
Materials and Methods:
This single-center, evaluator-blinded prospective study included 10 female subjects (≥35 years) with Motakef Class II and Class III labial protrusion, treated using helium plasma RF’s Apyx Plasma/Radiofrequency (APR) or Micro handpieces. Follow-up visits at 1, 14-, 30-, 90-, and 180-days post-procedure included Independent Photo Review, anatomical measurements, pain evaluations, and patient- and investigator-reported outcomes.
Results:
Both handpieces demonstrated significant improvements in labial protrusion and hypertrophy. No burns or serious adverse events (SAEs) occurred. Minor expected treatment effects (ETEs) such as bruising, crepitus, and edema were more frequent in the APR group (30 ETEs) compared with the Micro group (12 ETEs). The APR group experienced four adverse events (AEs) (including hematoma and wounds), while the Micro group had none. Pain levels decreased over time, with no pain reported by day 180 in the APR handpiece group and by day 90 for the Micro handpiece. Global Aesthetic Improvement Scale scores showed substantial improvement, with the Micro handpiece achieving 100% improvement by day 180. High satisfaction rates were reported, particularly with the Micro handpiece, where all subjects expressed willingness to recommend the treatment. The Micro handpiece also demonstrated a safer profile with fewer and shorter-duration AEs compared with the APR handpiece.
Conclusions:
The helium plasma RF system, particularly the Micro handpiece, presents a promising option for minimally invasive labial rejuvenation. As this study was conducted within a predefined time frame (May to November 2023, final follow-up in April 2024), additional subjects treated after this period were not included but may be analyzed in future research to expand the sample size. While results were favorable, few statistically significant findings were observed due to the small sample size. Further research with more participants, increased diversity among participants, and advanced imaging techniques to improve measurement accuracy and objective assessments of aesthetic outcomes is recommended.
Keywords
Introduction
Labiaplasty is a surgical procedure designed to reduce excess or lax skin in the labia majora and/or labia minora, which can result from various factors including childbirth, trauma, aging, genetics, or congenital conditions. 1 This procedure is often sought by women who experience general discomfort, pain during intercourse, pain during exercise, or aesthetic concerns related to the size or shape of their labia. While labiaplasty can provide effective results, traditional surgical methods are not without risks and complications. Common complications associated with a traditional excisional labiaplasty include dehiscence, hematoma, flap necrosis, narrowing of the introitus, pain, and asymmetry. These complications can lead to prolonged recovery times and may affect the overall satisfaction with the procedure. 2
In response to these challenges, there has been a growing interest in exploring less invasive alternatives that can achieve similar aesthetic and functional outcomes with fewer risks. One such alternative is the use of radio frequency (RF) energy-based treatments. RF energy works by delivering controlled thermal energy to the tissue, promoting collagen remodeling and tissue contraction, which can help to tighten and rejuvenate the labial skin without the need for excisional surgical intervention.
The helium plasma RF system (Renuvion; Apyx Medical, Clearwater, FL), which combines helium plasma with RF energy, offers a novel approach to minimally invasive labiaplasty. Unlike other RF devices that utilize bulk-heating technology, which increases the risk of burns, 2 this system provides instantaneous heating, which enables precise tissue contraction and contouring while minimizing thermal injury to surrounding tissues. This precision potentially reduces the risks associated with traditional surgery or other bulk-heating devices.
In April 2023, the Food and Drug Administration (FDA) in the United States updated clearances for the APR handpiece allowing use for coagulation and contraction of soft tissue, including subcutaneous soft tissue following aesthetic body contouring, and for improving the appearance of lax skin in the neck and submental region, and for the delivery of RF energy and/or helium plasma for cutting, coagulation, and ablation of soft tissue during open surgical procedures.
In June 2023, the FDA cleared the Micro handpiece for the helium plasma system, specifically for delivering RF energy and/or helium plasma where coagulation and contraction are needed. This handpiece was specifically designed to treat smaller, delicate areas such as the labia, making it an appealing option for patients seeking a less invasive alternative to a traditional excisional labiaplasty. This handpiece was utilized for this study as soon as it became available.
This study aims to evaluate the use of the helium plasma RF device as a minimally invasive alternative to excisional labiaplasty procedures. This research seeks to determine the potential advantages of RF energy-based treatment in terms of patient satisfaction, complication rates, and overall effectiveness in achieving desired aesthetic and functional results. The findings could provide valuable insights into the viability of RF energy as a preferred method for labial rejuvenation, offering patients a safer and more comfortable option for addressing their concerns.
Materials and Methods
This single-center, evaluator-blinded, non-randomized prospective study evaluated the outcomes of the helium plasma RF system treatment for labial rejuvenation in female subjects aged 35–70 years with labial protrusion classified as Motakef 3 Class II and Class III, who preferred a minimally invasive procedure over traditional excisional surgery. Medical history was collected, and a physical exam was conducted prior to study treatment.
Follow-up visits were conducted at 1-, 14-, 30-, 90-, and 180-day post-procedure. Baseline and follow-up images were captured for qualitative evaluation (see Fig. 1). Morphometric measurements and classifications of labia protrusion 3 and hypertrophy 4 were recorded at baseline, and at 30-, 90-, and 180-day post-procedure. Both subjects and the investigator completed the Global Aesthetic Improvement Scale (GAIS) at 30-, 90-, and 180-day post-procedure.

Thirty-five-year-old female, helium plasma RF Micro handpiece treatment before (left), day 90 (middle), day 180 (right). Thirty-five-year-old female seeking improvement for lax labial tissue who underwent treatment with the helium plasma RF Micro handpiece (from left to right). Patient in standard anatomical position, frontal view preoperative image (left side of image, top image). Patient seated in frog-leg position, frontal view preoperative image (left side of image, bottom image). Patient in standard anatomical position, frontal view postoperative image taken at day 90 follow-up visit (middle of image, top image). Patient seated in frog-leg position, frontal view postoperative image taken at day 90 follow-up visit (middle of image, bottom image). Patient in standard anatomical position, frontal view postoperative image taken at day 180 follow-up visit (right side of image, top image). Patient seated in frog-leg position, frontal view postoperative image taken at day 180 follow-up visit (right side of image, bottom image). RF, radio frequency.
Subjects also completed the Female Sexual Function Index (FSFI) 5 and Genital Appearance Satisfaction (GAS) scale 6 at baseline, 90, and 180 days. Additionally, a Patient Satisfaction Questionnaire (PSQ) was administered at day 180, and subjects reported the number of days until they felt comfortable resuming sexual activity. Pain levels were monitored throughout the study using the 11-point Numeric Rating Scale. 7
Formal statistical hypothesis testing was performed; however, due to the small sample size (N = 10), few statistically significant results were observed. Descriptive statistics are presented to summarize outcomes. Future studies with larger samples and more precise imaging techniques (e.g., 3D photography) are warranted to enable rigorous statistical analyses.
This study received approval from the Sterling Institutional Review Board (IRB, Atlanta, GA) on February 10, 2022, and subjects provided consent for the publication of their data and photographs. All procedures adhered to the ethical guidelines set forth by the IRB and followed the principles of the 1964 Helsinki Declaration and its subsequent amendments. Treatments took place between May and November 2023, with the final study exit occurring in April 2024.
Treatment protocol and posttreatment instructions
All procedures were conducted using the helium plasma RF system to achieve controlled tissue contraction in the pubis, labia majora, and labia minora utilizing either the APR (N = 7) or Micro (N = 3) handpiece. Subjects were positioned supine and then placed into the frog-leg position for the treatment.
Prior to the procedure, the treatment area was thoroughly cleansed and prepped according to standard sterile protocols. Local anesthesia was administered to ensure subject comfort throughout the procedure. Most subjects received Cefadroxil as a pre-procedure prophylactic and 1% Lidocaine with Epinephrine and 0.5% Marcaine as a subcutaneous incision site anesthetic. For the seven subjects treated with the APR handpiece, an average of 112.6 ± 8.8 cc of tumescent solution was delivered. For the three subjects treated with the Micro HP, an average of 143.3 ± 50.3 cc of tumescent solution was administered. The treatment area was undermined using a small puncture incision (3 mm) transversely about half a centimeter above the labial fornix, small puncture incisions at the base of each labia majora base for egress, providing access for handpiece entry and energy application.
For the seven subjects treated with the APR handpiece, the helium plasma RF treatment lasted an average of 13.1 ± 1.9 minutes, with a total energy delivery of 7.8 ± 1.7 kJ. These subjects were treated at 80% power, with a helium flow rate of 2 liters per minute (LPM), and 6 antegrade/retrograde passes. For the three subjects treated with the Micro HP, the helium plasma RF treatment lasted an average of 20 ± 7.2 minutes, delivering a total energy of 3.6 ± 2.2 kJ. These treatments were conducted at 30% power, with a helium flow rate of 1 LPM, and 6 retrograde passes. See Supplementary Video, which presents helium plasma RF treatment of labia with the Micro handpiece.
Energy parameters for the two handpieces were selected based on prior clinical studies, bench testing, and cumulative real-world experience. 8 Instructions For Use guidance for the APR handpiece recommends an energy range of 60%−80% power and helium gas flow rates of 1.5–2.0 LPM flow for the most consistent results with the lowest risk of adverse events (AEs).9,10 These parameters apply to all tissue regions with the surgeon’s discretion based on tissue quality, thickness, and patient age. The RF energy waveform and frequency are identical between the APR and Micro handpieces; however, the maximum power output for the Micro handpiece is intentionally limited to 30% (12 W) to achieve an equivalent power density (watt per square millimeter) as the APR handpiece operating at 80% (32 W). 11 This is due to the Micro handpiece’s smaller exit port, which concentrates energy delivery over a smaller area, resulting in a higher localized energy density. Thermal imaging utilizing a FLIR camera confirmed that these selected settings achieve comparable surface temperature rise across both devices.
Upon completion of the procedure, the treatment area was reassessed for any immediate adverse effects. Subjects were provided with postoperative care instructions, including guidelines on hygiene, activity limitations, and pain management. Specifically, subjects were instructed to:
Use a sanitary napkin for 24–48 hours to manage any leakage from the incision sites. Stay off their feet for 24 hours to reduce swelling. Resume all activities and exercise as soon as they feel comfortable. Refrain from sexual activity for 2 weeks. Apply Aquaphor as needed if irritation occurs at incision sites. Cleanse the area with a solution of distilled water and vinegar (1:1 ratio) as needed. Take over-the-counter Tylenol as needed for pain or discomfort. Use ice packs wrapped in a thin towel every 20 minutes while awake, to reduce swelling and potential discomfort. Expect some bruising or swelling as normal treatment effects, with severity varying between individuals. Be cautious when shaving, as the labia may experience temporary numbness for several months during the healing process. Avoid hot baths or Jacuzzis for 2 weeks following treatment.
Results
Demographics
All subjects in the study were female, with an average age of 41 ± 5.1 years old and body mass index of 25.7 ± 3.8. The racial composition included American Indian/Alaska Native/Asian (n = 1), Asian (n = 1), Black or African American (n = 3), Hispanic or Latino (n = 1), and White (n = 4). The majority (9 out of 10) did not report any prior tobacco use, with one subject having a history of smoking two cigarettes a day. No subjects had any tobacco use while enrolled in the study. Most subjects (7 out of 10) reported light alcohol use, while the remaining participants did not consume alcohol. The medical histories of the subjects, which included conditions such as headaches, anxiety, hypertension, bulging disc, and acne, did not affect the study treatment or outcomes. Eighty percent of subjects were American Society of Anesthesiologists Physical Status Class I, and 20% were Class II.
At baseline, nine subjects were classified as Class II A (2–4 cm of protrusion with asymmetry) and one subject as Class II C (2–4 cm of protrusion with involvement of the clitoral hood) according to the labial protrusion classification (Motakef Scale), which rates the degree of protrusion of the labia minora past labia majora. Additionally, all subjects were categorized as Type II (from 2 cm to 4 cm) on the Hipertrofia de Ninfas scale, which measures hypertrophy of the labia minora.
Outcome measures
The primary effectiveness endpoint, evaluated through qualitative IPR (Independent Photo Review) of images at 90 and 180 days compared with baseline (see Fig. 2), demonstrated that posttreatment images were correctly identified 40% of the time across both handpieces. The Micro handpiece exhibited a higher accuracy rate of 67% (4 out of 6 correct identifications) compared with the APR handpiece, which had an accuracy rate of 29% (4 out of 14 correct identifications). It is important to note that photo quality issues, specifically lighting, positioning of the labia due to pliability of the anatomy, hair over the labia, and menstrual blood, may have contributed to the overall lower IPR results.

Forty-four-year-old female, helium plasma RF ARP handpiece treatment before (left), day 90 (middle), day 180 (right). Forty-four-year-old female seeking improvement for lax labial tissue who underwent treatment with the helium plasma RF APR handpiece (from left to right). Patient in standard anatomical position, frontal view preoperative image (left side of image, top image). Patient seated in frog-leg position, frontal view preoperative image (left side of image, bottom image). Patient in standard anatomical position, frontal view postoperative image taken at day 90 follow-up visit (middle of image, top image). Patient seated in frog-leg position, frontal view postoperative image taken at day 90 follow-up visit (middle of image, bottom image). Patient in standard anatomical position, frontal view postoperative image taken at day 180 follow-up visit (right side of image, top image). Patient seated in frog-leg position, frontal view postoperative image taken at day 180 follow-up visit (Right side of image, bottom image).
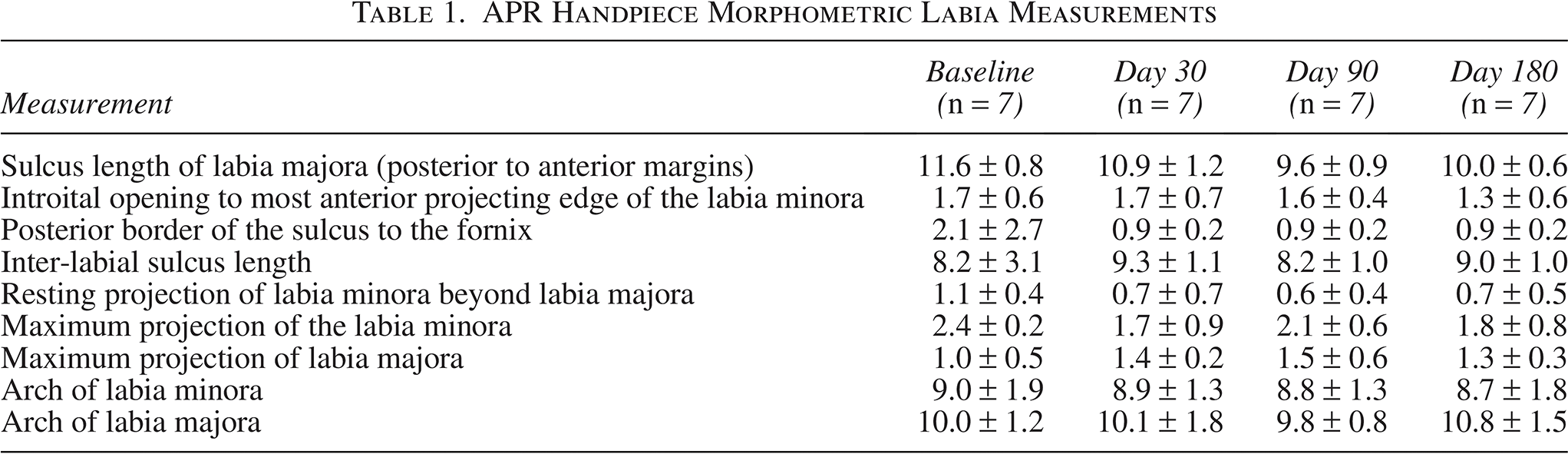
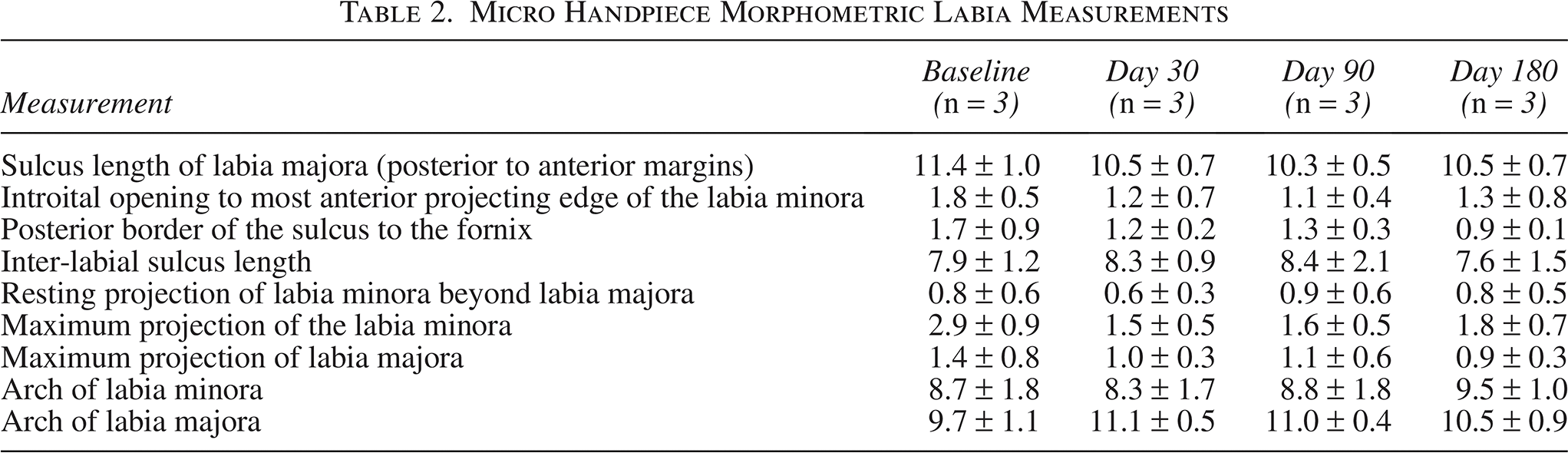
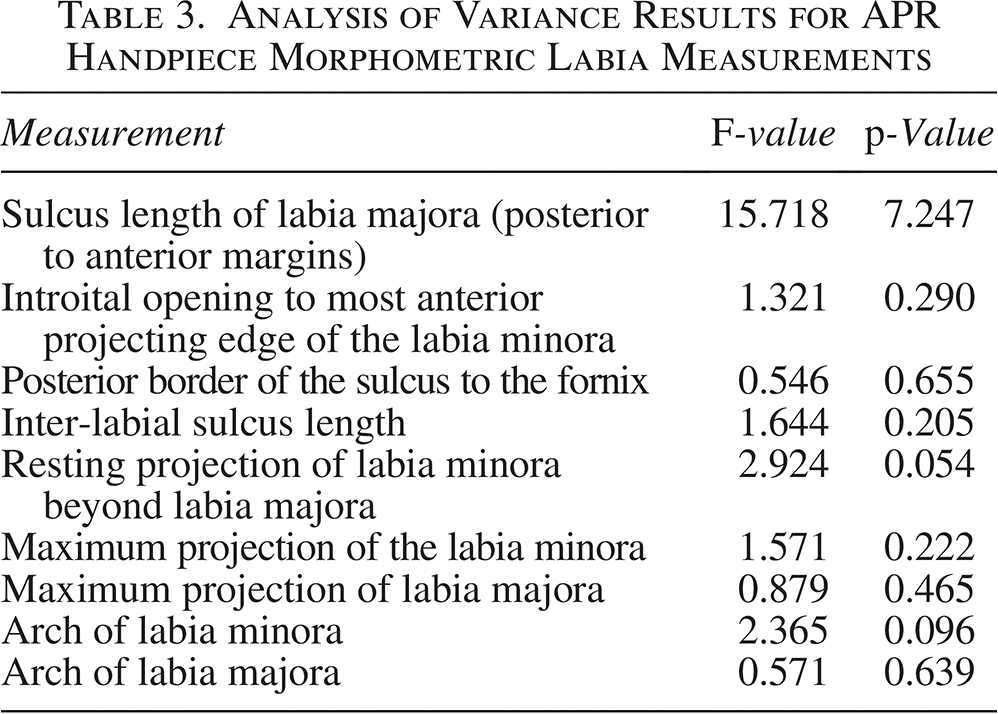
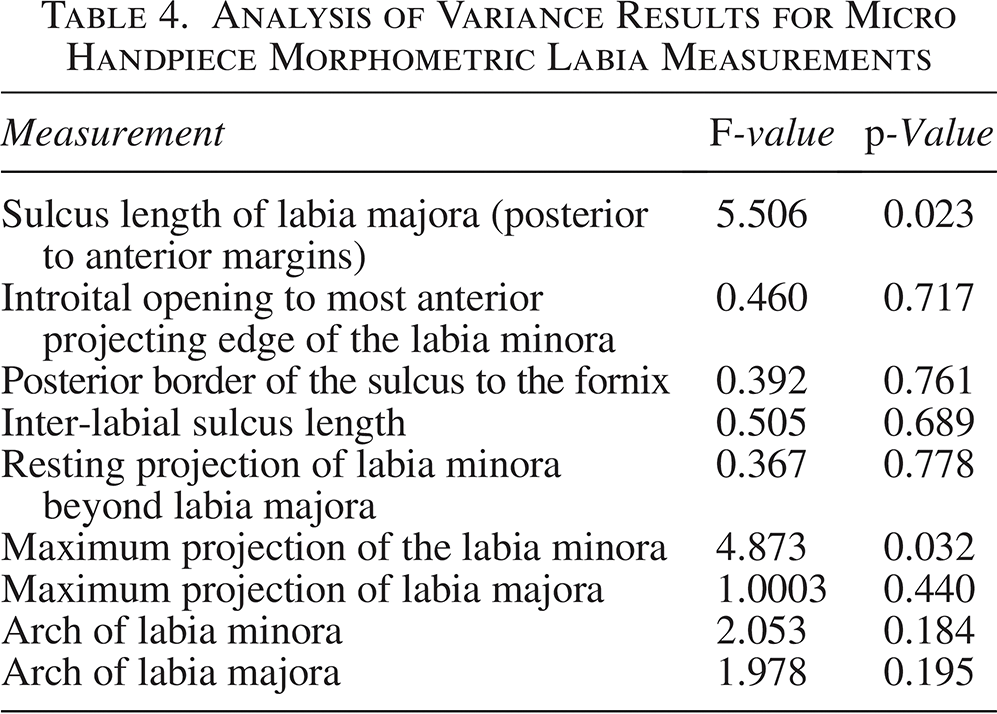
Anatomical measurements indicated a consistent and gradual decrease in the size of the labia majora and minora from baseline to day 180 across both handpieces, see Tables 1 and 2. Repeated-measures analysis of variance was conducted on the morphometric outcomes in Table 1 (APR handpiece) and Table 2 (Micro handpiece). No statistically significant results were observed across time points in the APR group (Table 3). In the Micro handpiece group, statistically significant reductions were observed in the sulcus length of labia majora (p = 0.023) and maximum projection of the labia minora (p = 0.033), see Table 4. Other morphometric parameters, including arch dimensions and inter-labial distances, showed directional trends over time but did not reach statistical significance (p > 0.05) in either treatment group, likely due to the limited sample size of this pilot study.
APR Handpiece Morphometric Labia Measurements
Micro Handpiece Morphometric Labia Measurements
Analysis of Variance Results for APR Handpiece Morphometric Labia Measurements
Analysis of Variance Results for Micro Handpiece Morphometric Labia Measurements
Improvements were observed in labia protrusion and hypertrophy classifications, with subjects showing better classifications by day 180. These changes reflect a positive impact of the treatment on labial anatomy, supporting the overall effectiveness of the procedure.
Pain levels reported by subjects decreased over time, with all subjects reporting no pain by the day 180 visit. This trend was consistent for both handpieces, indicating that the treatment was well tolerated over the course of the study. Scores for the seven subjects treated with the APR handpiece were 0.3 ± 0.8 following the study procedure, then 4.1 ± 2.5 at day 1, 3.7 ± 3.4 at day 14, 1.6 ± 1.8 at day 30, 0.1 ± 0.4 at day 90, and 0 ± 0 at day 180. Scores for the three subjects treated with the Micro handpiece were 0 ± 0 following the study procedure, then 2.3 ± 2.1 at day 1, 4.0 ± 1.0 at day 14, 2.0 ± 0.0 at day 30, and 0 ± 0 at day 90 and day 180. Notably, the Micro handpiece showed a more rapid decline in reported pain, with no pain reported by day 90.
Both Principal Investigator and Subject GAIS scores showed substantial improvement throughout the study. The Micro handpiece achieved 100% rated improvement in GAIS scores by both subject and investigator by day 180. The APR handpiece also demonstrated significant improvement, though the results were slightly less pronounced compared to the Micro handpiece. The PSQ results indicated notable improvements in labial appearance, with high levels of satisfaction reported among subjects (100% for subjects treated with the Micro handpiece and 86% for those treated with the APR handpiece).
The FSFI analysis revealed improvements across several domains over time for both handpieces. Subjects treated with the APR handpiece reported increases in desire, arousal, lubrication, and orgasm scores, although there was a decrease in satisfaction and an increase in pain during penetration. In contrast, subjects treated with the Micro handpiece showed improvements in desire, arousal, lubrication, and orgasm scores, with a concurrent improvement in satisfaction and a significant reduction in pain during penetration.
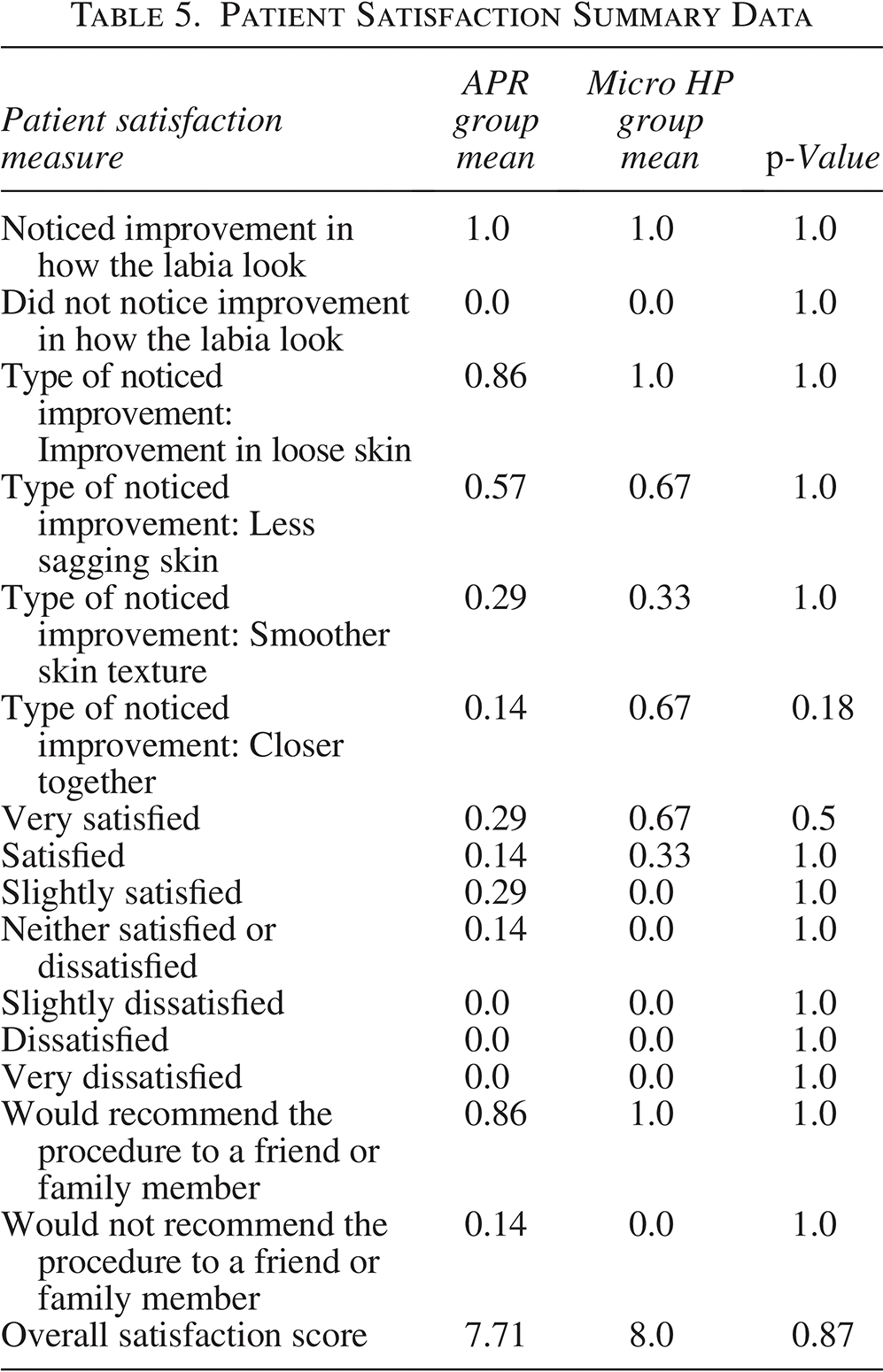
On the PSQ, 100% of subjects (10/10) reported overall improvement following treatment, and 90% (9/10) indicated they would recommend the procedure to their friends and family. Specific aesthetic improvements included reductions in loose skin (70%), less sagging (60%), smoother skin texture (50%), and closer labial folds (30%). Three subjects also reported additional improvements, such as asymmetry correction and localized contouring. Satisfaction scores included 30% very satisfied, 50% satisfied, 10% slightly satisfied, and 10% neutral; no participants reported dissatisfaction. On a 0–10 satisfaction scale, the mean score was 8.0, with a median of 9.0 (range: 5.0–10.0).
Fisher’s exact test was used to compare binary patient satisfaction and improvement responses between the APR and Micro handpiece groups. Welch’s t-test was used to compare continuous overall satisfaction scores. No statistically significant difference (p < 0.05) was observed between groups (Table 5).
Patient Satisfaction Summary Data
Subjects were instructed to wait a minimum of 2 weeks post-procedure to return to sexual activity. After the instructed waiting period, subjects treated with the Micro handpiece felt comfortable returning to sexual activity sooner (21.7 ± 8 days) compared with those treated with the APR handpiece (35.7 ± 26 days), suggesting that the Micro handpiece may facilitate a quicker recovery in terms of sexual function.
The GAS scores for participants using the APR handpiece decreased from an average of 18.57 at baseline to 9.14 at day 90, followed by a slight increase to 9.86 at day 180. In contrast, the Micro handpiece exhibited a consistent decrease in GAS scores, starting from an average of 22.33 at baseline, dropping to 12.33 at day 90, and further declining to 10.67 at day 180. These results indicate that satisfaction with genital appearance improved more consistently with the Micro handpiece.
Regarding expected treatment effects (ETEs) for the APR handpiece (n = 7 subjects), 30 ETEs were reported, including 2 instances of bruising, 7 of crepitus, 7 of edema, 7 of hypoesthesia, 6 of pain/tenderness, and 1 of pruritus/itching. In contrast, the Micro handpiece (n = 3 subjects) had 12 ETEs, including 1 instance of bruising, 3 of crepitus, 3 of edema, 3 of hypoesthesia/numbness, and 2 of tenderness. Regarding AEs, the APR handpiece group reported 1 hematoma and 3 wounds, while no AEs were reported in the Micro handpiece group. Notably, there were no burns in either group. Analysis of events (ETEs and AEs) up to day 180 visit revealed fewer types of events and shorter durations among subjects treated with the Micro handpiece compared with the APR handpiece. Across all subjects (N = 10), the most frequently reported ETEs included edema, crepitus, hypoesthesia, lasting up to 7.5 months in some APR-treated subjects. In contrast, all ETEs in the Micro handpiece group resolved within 2.5 months.
Subjects treated with the APR handpiece (n = 7) experienced edema for up to 6 months (average: ∼3.5 months), hypoesthesia for up to 7.5 months, and tenderness for up to 3 months. One subject reported a wound lasting 3.5 months. Pain typically resolved in under 2 weeks.
Among Micro handpiece-treated subjects (n = 3), edema and hypoesthesia resolved within 2.5 months. Tenderness, the most persistent event in this group, resolved within 5 weeks. No Micro handpiece subjects experienced wounds, bruising, or hematomas.
No burns were observed in either group, and all events resolved by or prior to the day 180 visit. These results support the Micro handpiece’s favorable safety profile and suggest a more rapid post-procedure recovery.
Discussion
This study evaluated the helium plasma RF system as a minimally invasive alternative to traditional excisional surgical labiaplasty. While the results demonstrate a degree of improvement in anatomical measurements and patient satisfaction, several limitations substantially impact the validity and reliability of these findings, and further research is necessary to better assess the effectiveness of this approach.
First, this initial pilot study was conducted with a predefined sample size of 10 subjects, who were treated between May and November 2023, with final follow-up completed in April 2024. This limited sample size reduces the statistical power and generalizability of our results, and no statistically significant differences were detected. Satisfaction data were analyzed descriptively, but statistical comparisons were not significant. Larger, multicenter trials will be needed to make reliable comparisons between labiaplasty procedures utilizing the helium plasma RF system and traditional surgical techniques and to draw conclusions that could apply to a broader population. Notably, recent studies have reported high patient satisfaction and low complication rates with energy-based labiaplasty approaches. In a case series by Dayan et al., bipolar RF treatment of the labia minora and majora yielded significant improvements in contour and function, and no significant complications reported. 2 These outcomes are consistent with our findings, particularly in the Micro handpiece group, which demonstrated similarly high satisfaction and minimal AEs. The favorable safety and satisfaction profiles reported with RF-based approaches further support the viability of non-excisional modalities such as the one evaluated in our study.
Second, images obtained at various follow-up intervals did not consistently reveal clear visual improvement, which complicated assessments of the treatment’s anatomical impact. Certain factors—such as lighting inconsistencies, positioning issues, hair coverage, and other visual obstructions—may have influenced the low identification accuracy in photo assessments. Additionally, considering where the subject was in their menstrual cycle or if they were postmenopausal could influence the appearance of the treatment area. Although quantitative measures indicated gradual reductions in labial size, these changes did not fully align with photographic assessments, potentially reflecting measurement constraints and limitations inherent in 2D imaging. Incorporating advanced imaging technologies, such as 3D photography with precise measurement capabilities, would improve the objectivity of the results in future studies.
Furthermore, pain scores varied, with some participants experiencing prolonged pain up to 90–100 days post-procedure, which, in some cases, exceeded pain typically reported following surgical excision. It is also noted that a subset of patients did not adhere to the postoperative instructions and experienced subsequent AEs, potentially influencing reported pain levels and recovery timelines. Compared to the author’s real-world experience with this procedure, the prolonged awareness of pain does not align with the broader patient experience.
Despite these limitations, most patients reported satisfaction with the procedure’s outcomes, particularly with reductions in physical discomfort and improvements in aesthetic concerns that initially motivated the treatment. Satisfaction scores, assessed through GAIS and PSQ, were notably higher in patients treated with the Micro handpiece. These findings are further supported by a large-scale systematic review and meta-analysis by Geczi et al., which analyzed 53 studies and nearly 4,000 patients, reporting an overall labiaplasty satisfaction rate of 94% across various techniques. 12 However, it is important to interpret these satisfaction ratings in context within the study’s qualitative and quantitative limitations, which underscore the need for expanded data and further analysis in future studies.
The findings suggest that the helium plasma RF system offers a potentially viable, less invasive alternative to traditional surgical labiaplasty, with many participants reporting functional and aesthetic improvements. However, the limitations outlined—sample size, imaging inconsistencies, and discrepancies between anatomical measurements and pain outcomes—highlight the need for more robust, multicenter trials. Enhanced methodologies, such as utilizing 3D photographic imaging, tattoo landmarks, and broadening the study population, would increase data accuracy and the generalizability of results.
Initial outcomes indicate promise; however, future studies should aim to include larger samples, comparison cohorts, and rigorous statistical testing to substantiate the helium plasma RF system’s safety and efficacy as a minimally invasive alternative for labial rejuvenation.
Conclusions
The helium plasma RF system presents a promising minimally invasive option for labial rejuvenation, offering patients an alternative to traditional excisional labiaplasty with a reduced risk of complications and a shorter recovery period. Study results suggest that this approach can lead to high levels of patient satisfaction, particularly in reducing physical discomfort and improving genital appearance. Both devices yielded high levels of satisfaction among subjects; however, the Micro handpiece demonstrated superior outcomes overall, including higher accuracy in IPR assessments and consistently better satisfaction ratings. Moreover, the Micro handpiece demonstrated a potentially safer profile with fewer AEs and shorter durations, making it a superior choice for treatment in this study. These results indicate that the Micro handpiece may be particularly advantageous for patients seeking minimally invasive alternatives to traditional excisional procedures for labial rejuvenation. However, limitations related to sample size, image analysis, and anatomical assessment emphasize the need for caution in interpreting these findings as definitive.
To strengthen the evidence base, future studies should incorporate larger, more diverse participant populations and advanced imaging techniques to improve measurement accuracy and objective assessments of aesthetic outcomes. Additionally, investigating the underlying factors contributing to variable pain responses will be critical in fully understanding the safety and comfort of this approach relative to surgical methods. With further validation, the helium plasma RF system may establish itself as a valuable addition to labial rejuvenation options, meeting patient demand for minimally invasive solutions while delivering effective, satisfactory results.
Authors’ Contributions
P.G.R. contributed to the conceptualization and design of the study, study methodology, conducted all clinical evaluations and surgical procedures, provided resources and supervision, participated in article review and editing, and secured funding for the project. A.M. contributed to study methodology, conducted data management and analysis, participated in clinical investigation, drafted and revised the article, coordinated the project, and developed visual materials for the publication.
Footnotes
Acknowledgments
Medical writing assistance was provided under the direction, oversight, and input of the authors by Kari Larson of Apyx Medical.
Author Disclosure Statement
P.G.R. is a consultant and medical advisory board member for Apyx Medical. A.M. does not have any disclosures to report.
Funding Information
This study was supported by a research grant from Apyx Medical.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.