
Abstract
Midlife, beginning at 40 years and extending to 65 years, a range that encompasses the late reproductive to late menopausal stages, is a unique time in women’s lives, when hormonal and physical changes are often accompanied by psychological and social evolution. Access to sexual health and sexual well-being (SHSW) services, which include the prevention and management of sexually transmitted infections, contraception and the support of sexual function, pleasure and safety, is important for the health of midlife women, their relationships and community cohesion. The objective was to use the socio-ecological model to synthesise the barriers and enablers to SHSW services for midlife women in high-income countries. A systematic review of the enablers and barriers to women (including trans-gender and non-binary people) aged 40–65 years accessing SHSW services in high-income countries was undertaken. Four databases (PubMed, PsycINFO, Web of Science and Google Scholar) were searched for peer-reviewed publications. Findings were thematically extracted and reported in a narrative synthesis. Eighty-one studies were included; a minority specifically set out to study SHSW care for midlife women. The key barriers that emerged were the intersecting disadvantage of under-served groups, poor knowledge, about SHSW, and SHSW services, among women and their healthcare professionals (HCPs), and the over-arching effect of stigma, social connections and psychological factors on access to care. Enablers included intergenerational learning, interdisciplinary and one-stop women-only services, integration of SHSW into other services, peer support programmes, representation of minoritised midlife women working in SHSW, local and free facilities and financial incentives to access services for under-served groups. Efforts are needed to enhance education about SHSW and related services among midlife women and their healthcare providers. This increased education should be leveraged to improve research, public health messaging, interventions, policy development and access to comprehensive services, especially for midlife women from underserved groups.
Plain language summary
Midlife, beginning at 40 years and extending to 65 years, a range that encompasses the late reproductive to late menopausal stages, is a unique time in women’s lives. Access to Sexual Health and Sexual Wellbeing (SHSW) services, which include the prevention and management of sexually transmitted infections, contraception and the support of sexual function, pleasure and safety, is important for the health of midlife women, their relationships and community cohesion. The objective of this systematic review was to use the socio-ecological model to synthesise the barriers and enablers to SHSW services for midlife women in high income countries. Eighty-one studies were included; a minority specifically set out to study SHSW care for midlife women. The key barriers that emerged were the intersecting disadvantage of under-served groups, poor knowledge, about SHSW, and SHSW services, among women and their HealthCare Professionals (HCPs), and the over-arching effect of stigma, social connections, and psychological factors on access to care. Enablers included intergenerational learning, interdisciplinary and one-stop women-only services, integration of SHSW into other services, peer support programmes, representation of minoritised midlife women working in SHSW, local and free facilities, and financial incentives for under-served groups to access services. The appetite for education about SHSW and SHSW services among midlife women and their HCPs should be capitalised upon, and utilised to improve research, public health messaging, interventions and access to holistic services, particularly for midlife women from under-served groups.
Introduction
The publication of the UK government’s first Women’s Health Strategy in 2022 1 coincided with the welcome and long overdue global recognition of the necessity for more multi-disciplinary research in both women’s2 –5 and older people’s sexual health and sexual well-being (SHSW).6 –8 Public health approaches to sexuality focus on adverse biomedical outcomes, 9 despite the growing evidence for the importance of a holistic approach when evaluating sexual health,8,9 and the inclusion of positive sexuality and sexual experiences in the World Health Organization’s definition of sexual health. 10 In this review, we have followed Mitchell’s framework, which separates SHSW into two separate, inter-linked foci of public health enquiry. 11 Sexual health is defined as encompassing the prevention and management of sexually transmitted infections (STIs) including HIV, sexual violence prevention, support of sexual function, desire and arousal and fertility management. Sexual well-being is a multi-dimensional concept,12,13 which comprises sexual safety and security, sexual respect, sexual self-esteem, resilience in relation to sexual experience, forgiveness of past sexual experience, comfort with sexuality and self-determination in one’s sexual life. 11 SHSW services are often combined and offered in primary care, secondary care (sexual health and gynaecology services), health services which look after physical and mental health conditions interlinked with SHSW, and community and charitable services. Midlife is defined as beginning at 40 years and extending to 65 years, 14 a time when hormonal, physical and psychological changes in the lives of women 15 are often accompanied by evolution in their relationships,16,17 and social developments. 18 This stage can be a positive transition point for women, 19 empowering them to determine how they envision spending the latter half of their years, and can result in varied sexual experiences. 20
Midlife women are a growing population, often responsible for being both primary caretakes of children and elders, and major economic contributors.21,22 Increasing societal demands impact on their sexual experiences. 23 Cultural shifts in relationship patterns, 24 and population changes due to the stretching of mid years, 25 mean that SHSW services are an increasingly important part of the lives of midlife women, integral to the physical and mental health of many.26,27 Intimate partner violence and sexual assault are major public health issues, which have long-term effects on the health and functioning of many midlife women. 28 Prompt, effective diagnosis and treatment of STIs and gynaecological diseases, and the provision to support midlife women in having enjoyable, safe sex, has wide-ranging benefits to individuals, partnerships 29 and communities. 30 Indeed, the provision of sexual and reproductive health services is related to multiple human rights and should be available in adequate numbers, physically and economically accessible without discrimination and of good quality for everybody, including all midlife women. 31 Studies are often framed in a male, hetero-normative 32 perspective and the heterogeneous needs of midlife women are sometimes stereotyped by ageist and sexist misconceptions, or forgotten, 24 squeezed between the higher prevalence of STIs in adolescents and the increasingly apparent high prevalence of sexual dysfunction in older adults. 33
General health issues, such as diabetes, cardiovascular disease and arthritis, begin to emerge during the latter half of midlife and operate both to impact on sexual experience, with implications for the need for help-seeking, and should also provide opportunities for issues relating to sexual matters to be raised in routine healthcare. 8 However, many healthcare professionals (HCPs) are reserved about, and ill equipped to discuss SHSW with midlife women.5,6,15,32,34 –37 Stigma and negative attitudes about women’s sexuality, and sexuality at older ages, may inhibit discussion with HCPs. 38 Embarrassment may inhibit women from accessing help when symptomatic, 15 and SHSW services are not designed in a way that encourage midlife adults to seek help.5,6,15,32,34 –37 Health policies about ageing often omit sexuality, further contributing to the lack of research and services available. 39 Technology has not been sufficiently harnessed; the only evidence available for improving access to SHSW services for midlife women lies in the menopause field, but many menopause apps lack a credible evidence base. 40
In addition to the health inequalities related to identifying as female gender, 41 including the diminishing healthy life expectancy despite a longer life expectancy of women, 42 and the historical default of medical research being carried out on men, 43 there are also significant disparities in access to, and engagement with, healthcare services among women, largely due to the social determinants of health. 44 Within globally privileged settings, there is already a high disparity in access to services. The review was therefore restricted to high-income countries to improve the specificity of findings. It has enabled us to disentangle the impact of different strands of marginalisation within the context of affluent economies, which have separate challenges from low- and middle-economic locales. The World Bank’s definition of high-income countries was employed; high-income countries had a gross national income per capita of US$13,845 or more in 2022, calculated using the Atlas method. 45
This review evaluated the research that identified the enablers and barriers to midlife women’s access to SHSW services and established whether any groups of midlife women were particularly disadvantaged. It thereby delineated the key foci for policy and strategy change to improve quality and equity of SHSW care for midlife women in high-economic countries. The socio-ecological model (SEM) recognises the multiple and dynamic factors that can affect the barriers and enablers to accessing healthcare by considering the complex interplay between individual, interpersonal, organisational, community and public policy factors. 46 These factors affect SHSW decision-making for an individual and can both enable and inhibit healthy sexual behaviours. 47 The SEM approach has been successfully employed to interrogate many aspects of SHSW services for different populations, for example SHSW services for female sex workers, 48 adolescents49,50 and migrant Asian women, 51 and has enabled a holistic consideration of the different SHSW needs of midlife women within the complex context of the societies in which they live.
Objectives
The objectives of this review were to identify the barriers and enablers to SHSW services for midlife women in high-income countries 45 using the SEM, 52 and to identify the groups of midlife women in high-income countries who found accessing these services particularly challenging.
Method
Reporting of the review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations (Figure 1). The protocol was Registered with the PROSPERO database on 8 June 2023, registration number: CRD42023433812.

PRISMA flow diagram. The barriers and enablers to accessing sexual health and well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Eligibility criteria
The inclusion criteria (Table 1) were studies that had been published between November 1993 and November 2023, peer-reviewed, employed any methodology to capture primary data and investigated barriers to, or enablers of, access to SHSW care for midlife women (40–65 years old) who resided in high-income countries, 45 grouped into intrapersonal, HCP relationship, community and organisation perspectives. Studies on anyone who identified as a woman, gender diverse and non-conformist to either gender were included in this review. Transgender women and non-binary people (TGNB) experience different levels of stigma and discrimination than their cisgender counterparts, 53 but can share more in common with cisgender women than they do with men who have sex with men, 54 a group with whom they are often aggregated in SHSW research. 55 The review states when conclusions were drawn from TGNB-specific studies.
Inclusion and exclusion criteria for the barriers and enablers to accessing sexual health and sexual well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review.
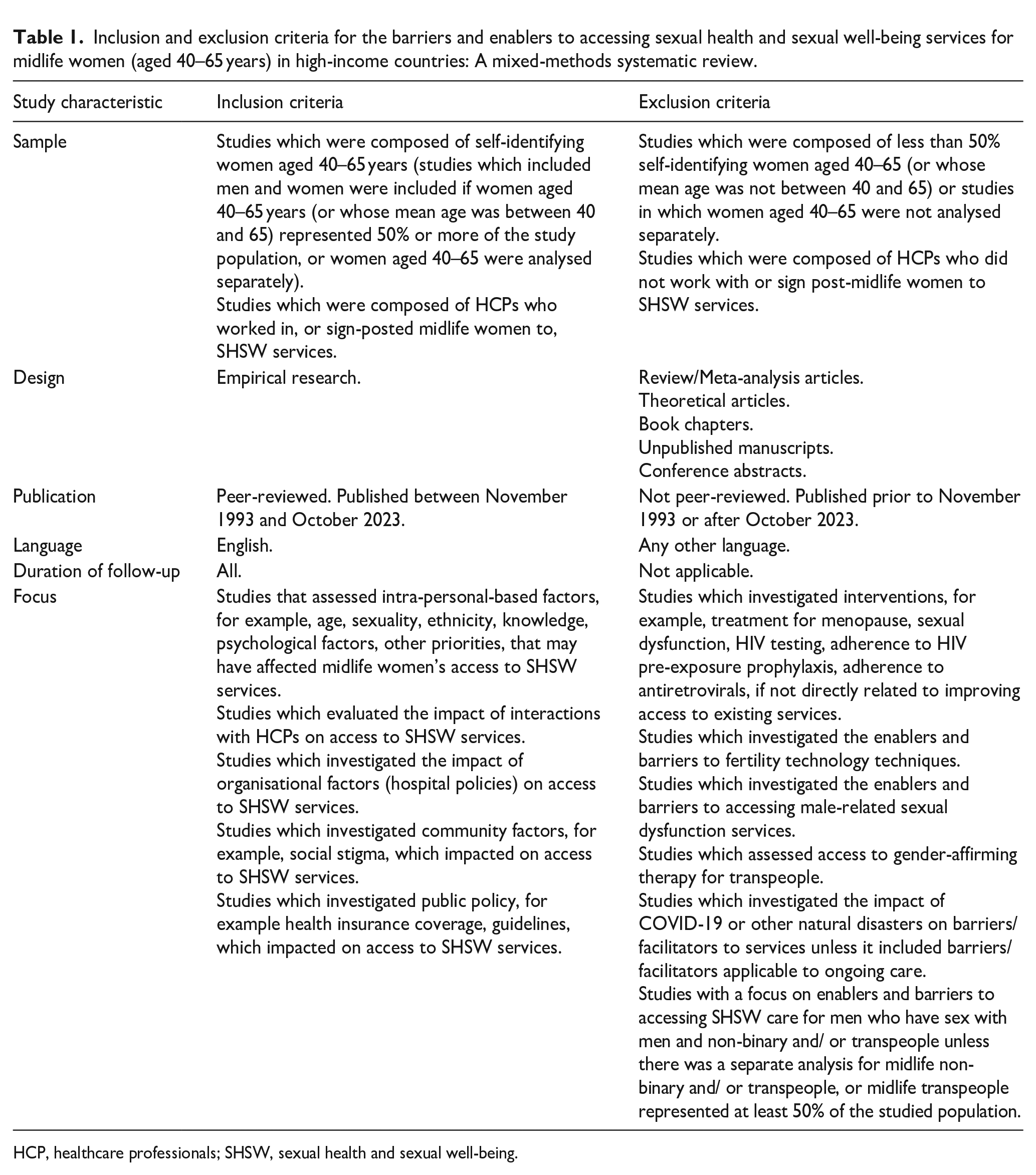
HCP, healthcare professionals; SHSW, sexual health and sexual well-being.
Exclusion criteria (Table 1) comprised studies which investigated fertility technology techniques, as this was felt to widen the scope of the review too much and warrant a separate analysis. Male-related sexual dysfunction services were excluded, as although these would affect some women as partners in a relationship, women would not be the primary focus of the services. Studies addressing enablers and barriers to care for midlife TGNB people were only included in the review if they met the criteria of including at least 50% TGNB people and did not focus solely on gender-affirming therapy, a subject that warrants a separate review. COVID-19 may have had a significant impact on access to SHSW services 48 ; studies were only included if enablers and barriers that could be attributed to the COVID-19 pandemic had not yet reverted back to their state prior to the pandemic.
Search strategy
The search strategy was devised by KS with the assistance of CI, CL and SB. PubMed, PsycINFO, Web of Science and Google Scholar databases were searched between 23 April 2023 and 1 August 2023. The search strategy (Figure 2) was based on the SPIDER tool. 56 Sample: Women aged 40–65 years (and their HCPs); Phenomenon of Interest: Barriers and enablers to SHSW services; Design: Peer-reviewed research (qualitative/quantitative/mixed-methods); Evaluation: Critical Appraisal Checklists (CASP) criteria 57 ; Research type: Systematic review to optimise identification of relevant articles. The detailed search strategy is documented in Figure 2. Search limits included: English language and adults and middle-aged adults. No date or country of setting limits were applied. The included articles’ reference lists were hand-searched for additional relevant articles. Articles identified in the search were exported to EndNote. After removal of duplicates, 45 the remaining articles were exported to Excel.

Detailed search strategy criteria for the barriers and enablers to accessing sexual health and well-being services for midlife women (aged 40–65 years) in high-income countries: a mixed-methods systematic review.
Selection
Titles and abstracts were screened for relevance by KS and articles that did not meet the inclusion criteria were removed. Full texts of the remaining articles were reviewed independently in Microsoft Excel by KS and CN. Any disagreements were resolved through discussion between KS, CN and CI to reach a final decision.
Data extraction
Study characteristics were extracted by KS using a pre-set proforma on Excel (author, title, year published, participant characteristics, study aim.) Further study characteristics were then extracted by hand by KS onto a table in Microsoft Word (participant characteristics: sample, age range, gender of participants, relationship status, sexual orientation, language requirements, education level, ethnicity, study design and study findings).
Quality assessment
The CASPs 57 were used to systematically assess the trustworthiness, relevance and results of the articles. The appropriate checklist was used for each study, for example the qualitative checklist was used for qualitative studies. The reporting of the results of the study were assessed for validity, what the results were, and whether the methodology was sound. KS rated the studies (high, moderate or low quality) using the checklists as guides. About 10% were randomly selected and rated by a second author (CI, SB, CL, CN) to ensure validity. Any discrepancy in the rating was discussed, and if required, a third or fourth author would have been consulted to ensure unanimity. However, there were no discrepancies, resulting in a Cohen’s Kappa rating 51 of 1. Eligibility of articles was not determined by quality rating.
Data synthesis
The socio-ecological model (SEM) 52 was used to conceptualise and organise the findings into the enablers and barriers to accessing SHSW care, in terms of intra-personal factors, interactions with providers, organisational factors, community factors and public policy. The use of the SEM model has precedence in contextualising the complex levels of socioecology in which individuals are embedded, and the social, structural and cultural influences on behaviours affecting access to SHSW care. In the past, it has proved valuable in the analysis of the barriers and enablers to SHSW care for female sex workers, 58 adolescents, 59 urban men 49 and migrant Asian women. 50 Narrative synthesis was used to explore relationships within and between study findings. This method was employed because characteristics of the study designs and outcomes were too heterogenous to yield a meaningful summary of findings using a meta-analysis. The main findings and conclusions were grouped and coded inductively into descriptive themes that emerged from the data within the categories of ‘barriers to’ and ‘enablers of’ access to SHSW care, as defined by the inclusion criteria (Table 1). Data were further grouped and coded to iteratively develop and refine descriptive themes, with each study contributing new themes, using the SEM. Generation of higher-level analytical themes was undertaken.
Results
Study characteristics and main findings
Eighty-one studies were included in the final selection (Table 2).
Quality assessment of studies for the barriers and enablers to accessing sexual health and sexual well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review.

CASP, Critical Appraisal Checklists; HCP, healthcare professionals; HPV, human papilloma virus; HRT, hormone replacement therapy; SHSW, sexual health and sexual well-being; STI, sexually transmitted infection.
Study locations
Most of the studies were conducted in the United States (46), and the United Kingdom (17), with the remaining being conducted in Canada (7), Australia (2), Hong Kong (1), Israel (2), Spain (1), Italy (1), Ireland (1), Spain and Serbia (1), England, Finland, Denmark, New Zealand, Australia and United States (1) and Europe (1).
Design of included studies
Studies included in the review were quantitative (45), qualitative (30) and mixed methods (six). Of those using qualitative methods, nine employed focus group discussions, 16 used interviews, four used both focus group discussions and interviews and one was a qualitative content analysis. Of those employing quantitative methods, one was a review analysis, 10 were cohort studies, 32 were cross-sectional studies and two were randomised trials. Mixed methods trials included cross-sectional studies linked with interviews (three) or interviews (one) and focus groups (one), a cohort study linked with interviews (one) and a mixed quantitative and qualitative content analysis (one).
Study samples
Most studies (60) were presumed to have been conducted on cisgender women, although this was not specifically documented. Ten studies were conducted on transgender women. Three studies were conducted on both transgender and cisgender women. Eight studies were conducted on HCPs.
Recruitment methods
Convenience sampling was the most common method of recruitment (51), followed by purposive sampling (20). Four studies used a mixture of purposive and snowballing sampling, one study used convenience and snowballing sampling, four studies used randomised sampling, one study used ‘mixed recruitment’.
Quality assessment
The CASP checklists 57 were used to critically appraise the studies with systematic consistency (Table 2). Studies were assessed for validity and methodological reliability. Sixty-five of the studies were deemed to be of high quality, 15 of moderate quality and one of poor quality.
Type of SHSW areas examined
The enablers and barriers to accessing different SHSW services were examined. The SHSW services investigated included: sexual experience and function services, cervical screening, human papilloma virus (HPV) and cervical cancer care, HIV and STI testing, primary and preventive care, HIV care, HIV pre-exposure and post-exposure prophylaxis, menopause care, Hormone Replacement Therapy (HRT), gender-based violence services, contraceptive care and women’s health services in general. Thematic extraction of findings (Table 3).
Thematic extraction of findings, based on the socio-ecological model. (specific to people who identify as trans and non-binary in italics)

The barriers and enablers to accessing sexual health and well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review. HC, healthcare; HCP, healthcare professionals; PrEP, pre-exposure prophylaxis; SHSW, sexual health and sexual well-being; STI, sexually transmitted infection.
Intra-personal themes
Intersecting disadvantage of marginalised groups
Twenty-eight studies revealed the intersecting disadvantage of being a midlife woman and belonging to other marginalised groups with relation to accessing SHSW services. There is evidence that age,72,90,108,113,130,134 sexuality,108,130 ‘physical appearance’ as a cause of perceived discrimination, 135 gender,90,134 gender identity,75,99,136 race,99,113,137 ethnicity,96,131,137 immigration status, 61 cultural group,61,78 nationality,87,114 colonial legacy, 98 linguistic ability,78,125 level of deprivation, 89 income, 79 perceived income inadequacy, 121 area of residence, 84 level of education79,82,84,138 and belonging to a stigmatised group,63,74,77,103,113 impact on the ability of midlife women to access SHSW care. This intersecting marginalisation was demonstrated by an Australian study which investigated whether a ‘hub and spoke’ model would improve access to testing for STIs. Primary HCPs reported that they ‘rarely’ provided sexual health consultations for the most marginalised communities, which were identified as lesbian, gay, queer and transexual people, sex workers, people who inject drugs, certain ethnicities, the incarcerated, and refugees. 106
Older age, within the midlife range, often inhibited access to SHSW services:63,66,130,134,109 increased age was associated with worse sexual healthcare experiences, 130 being less likely to consider HIV pre- and post-exposure prophylaxis for HIV, older women who had experienced a premature menopause were less likely to receive treatment than their younger counterparts, 63 and younger women were more likely to seek sexual health help following breast cancer than their older counterparts. 109 Although older age inhibited access to some services, perhaps due to a combination of discrimination, self-advocacy and lack of current knowledge, the wisdom acquired with age, sometimes resulted in improved access to services. Confounding factors such as ethnicity, family poverty status, urbanisation and HIV exposure risk, may have affected the results, but a large cohort study in the United States demonstrated that women aged 60–64 were more likely to have been screened for HIV than women aged 50–54. 132 Similarly, one small study, which investigated the sexual behaviour of midlife women who had experienced incarceration, suggested that (older) women were more likely to use precautions to protect against STIs than when they were younger, and were more likely to co-test with new partners pre-sex compared to when they were younger. 139
Non-heterosexual women faced more barriers to accessing SHSW services than heterosexual women. They described hesitancy seeking help due to negative past experiences after disclosing their sexuality, 108 and worse sexual healthcare experiences. 130 Bisexual and homosexual women in the United States had lower cervical screening rates than heterosexual women; 140 proposed reasons were difficult past experiences, 141 and poor HCP knowledge about when screening was required. 142 One study in the United States found that perceived discrimination due to ‘physical appearance’ (not defined), and gender, were associated with the reduced receipt of cervical smears; 94 the authors suggested that the discrimination that these women perceived to be present may have inhibited their access to screening. The gender imbalance in sexual relationships remains an ongoing issue: two different UK studies found that both women and men frame the necessity to seek help for sexual difficulties predominantly in relation to erectile dysfunction.8,90 It can be postulated that this minimises the importance that women face on seeking help for their own sexual dysfunction. Gender identity also affects midlife women’s access to care:99,103,115,136,143 three studies demonstrated that transphobia was a strong barrier to enrolling in,115,144 and engaging in, 99 HIV care. Transwomen also faced unique challenges when accessing care following sexual assault. 75
Six studies demonstrated that race99,113,132 and ethnicity61,131,137 affected use of preventive healthcare, 60 HIV-testing, 132 HIV-related stigma, 113 HIV care for transwomen, 99 and awareness of HIV PrEP for transwomen. 137 Similarly, Black women were significantly less likely than White women to report being offered HRT, 131 and a study in Israel revealed that Arab women were more likely than Jewish women to present at an advanced stage of cervical cancer. 96 Although, in contrast, one study found that perceived racial discrimination was not found to be associated with receipt of cervical smears, 94 this research had many limitations including the unusually frequent exposure that the study participants had to healthcare services.
Access to HRT varied significantly depending on country of residence.87,114 Despite the fact that self-reported menopausal symptoms did not differ significantly among women of different nationalities, there was a marked difference in the utilisation of hormone therapy, for example with much higher use in France compared to Spain. 87 An analogous finding was that linguistic ability was a barrier to accessing menopause care for Hispanic women in the United States, 78 and affected women’s desire to participate in medical decision-making around menopause issues. 125 Cultural inhibitions and the need for a higher level of assertiveness than previously required when dealing with American providers limited women’s access to menopause care, 78 and an Australian study described the legacy of colonialism as a barrier to women accessing cervical smears. 98
The social determinants of health, 145 including income,79,89,121,122 area of residence, 84 and level of education,79,82,84,138 have been associated with access to SHSW services for midlife women. Sexual and reproductive health behaviour was associated with socio-economic indicators in Spanish women who were born before the 1950s. 84 Both socio-economic inequity in Canada, 98 and lowest perceived income adequacy as an emotional barrier in the United States (higher fear of cancer being detected), 122 have been associated with decreased access to cervical screening. Similarly, in the United States, higher level of income was associated with an increased likelihood of HRT counselling being obtained by women, although the results may be out-dated, as the study was conducted in 1998. 80 A UK-based study found a strong association between HRT prescription rate and socio-economic deprivation. After adjusting for cardiovascular risks, there was an 18% lower HRT prescription rate in the most deprived practices compared with the least deprived. 89 Poverty has also been cited as a major barrier to transgender midlife women accessing HIV care. 115 Likewise, area of residence has been associated with access to SHSW services: American women living in urban areas were much more likely to have been screened for HIV than those living in rural areas. 132 Level of education, a significant factor influencing access to public services, was found to impact on access to SHSW care.61,79,82,98,134 Five studies, investigating HRT, 82 preventive healthcare use, 61 STI testing, 134 cervical screening 98 and likelihood to receive HRT counselling, 80 found positive associations between the level of a woman’s education and their ability to access SHSW services.
Belonging to a stigmatised group, such as being a sex worker, 144 selling 144 and using recreational drugs, 74 having been recently imprisoned, 77 and living with a condition such as HIV,63,113 negatively impacted on access to SHSW for midlife women. For example, engagement in sex work and selling drugs were identified as prohibiting factors for women who required HIV care in the United States. 103 A Canadian study demonstrated that injecting drugs was associated with worse adherence to antiretroviral therapy for midlife women living with HIV. 74 Recent incarceration was found to be independently associated with not achieving HIV virological suppression in a cohort study of women living with HIV in Canada. 77 Although there are many reasons, apart from belonging to a minoritised group, why these women found accessing care challenging, establishing where care is most needed is the first step in disentangling where services should be focused.
Knowledge, awareness and behaviour
Twenty-five studies exploring knowledge about STI risks,24,70 HPV, 120 cervical cancer,95,121 menopause,22,29,34,117,146 HRT,91,111,114,147 contraception, 66 HIV PrEP62,65,85 and HIV Treatment as Prevention,129,148 revealed a poor depth and breadth of SHSW knowledge among midlife women, which was a barrier to accessing services. The incorporation of different formats of education into healthcare systems64,93,100,109 was viewed as an enabler to accessing SHSW services.
Interviews with mid-lifers in the United Kingdom, following the end of long-term relationships, found that participants used indicators such as demeanour and appearance to assess the STI status of new partners. 24 Similarly, very few heterosexual mid-lifers in Scotland used condoms or co-tested with new partners for STIs if their new partners reassured them that they were ‘low-risk’ (few previous partners, recently had a long previous relationship). 70 Indeed, some women cited freedom from the risk of pregnancy as a reason not to use condoms, simultaneously (and perhaps unknowingly) increasing their exposure to STIs.70,123 Unfamiliarity, or inexperience, with condoms after not using them for a long time, also prevented their use. 24 Women in the United States, as recently as 2018, demonstrated disappointing knowledge about contraception and emergency contraception 66 and had poor knowledge about HPV, cervical cancer and HPV vaccination. 120 In focus groups about HIV Pre-exposure Prophylaxis in the United States, women were surprised and angry that they had never heard about it; they advocated for educational campaigns. 85 More reassuringly, although still in need of improvement, an Irish study found that 84% of women were aware of why they should have regular cervical smears. 95 Reflecting the need for access to evolving health education at different stages of women’s lives, a study in the United States in the year 2000 found that women who reported never having had sex as adults had lower cervical screening rates and lower rates of HRT use. 140
Middle aged women’s knowledge about menopause symptoms and management was disappointing.22,34,73,81,126,146 Focus groups in the United States reported a need for (more) reliable, accessible and current information about the menopause. 81 In one study of women living with epilepsy, only 31% had confidence that they were knowledgeable about the menopause; the authors attributed this to inadequate patient–physician communication. 146 An Italian survey found that a minority of midlife women received information about the menopause, and possible therapies, and those who did found it of poor quality. 73 Of 3046 postmenopausal women with vulvar-vaginal atrophy, only 24% attributed their symptoms to the menopause. 34 Breast cancer survivors with menopausal symptoms, in a study in 2013, described difficulty distinguishing between credible and non-credible sources of information, and uncertainty about which HCPs to approach for advice. 147
The importance of multiple formats of SHSW educational resources for midlife women was highlighted,22,64,93,109 regarding sexual health following cancer treatment,64,93 sexual health concerns, 109 the menopause22,78 and HRT. 100 Women attributed the poor quality of information available about HRT as a barrier to making informed decisions, described the internet as confusing, 100 and suggested a comprehensive HRT website, with regular seminars for menopausal women 100 and consumer decision aids summarising the evidence about HRT. 100 Hispanic women were disappointed that brochures and videos were non-specific and failed to address the intensity of their menopausal symptoms. They called for better tailored, individualised information and described a lack of access to advice due to the death of matriarchs, and cultural challenges with asking elders to educate them. 78 Women in Hong Kong felt that information about the physical and emotional changes in the menopause which can affect sexual function should be specifically addressed by HCPs, and suggested seminars and pamphlets, documentaries, storytelling programmes, adverts, newspapers and magazines as useful sources of information. 29 It must be acknowledged that historically limited research about the management of menopause compounded the lack of access to good information and may have influenced the findings of these studies. 149 In a more recent study, nurses in the menopause transition described spending a long time looking for information, with poor results. Due to the widespread use of smart phones, they felt that it should be possible to have quick, easy access at any time in an anonymous way, secure platform with evidence-based information. They described the necessity for digital resources to be culturally sensitive, with podcasts, videos, virtual reality, mindfulness, and expert blogs. 22 Survivors of breast cancer who requested education about sexual dysfunction had a preference for in-person options and support groups. 93 Similarly, women (cisgender and transgender) who were consulted about how to improve their engagement with PrEP education advocated for learning from peers. 129
A facilitator to accessing SHSW services was when women made visiting services into a habitual behaviour. Midlife women in the United States, where there was not a universal screening recall system, were significantly more likely to have a cervical smear if they had one previously. 121 However, not re-assessing personal changes in risk with time and circumstance may have resulted in adverse outcomes for some women. One study found that women’s self-perceived STI risk was sometimes rooted in past long-term relationships: even if they were taking chances with their SHSW, they still viewed themselves as at the same exposure as when they were in a long-term monogamous relationship. 24
Psychological factors
Midlife is a particularly vulnerable phase for experiencing mental health problems. 150 In the United States, rates of depression are highest in women in their midlife, compared to men, and women of other ages. 151 Sexual health problems can be interlinked with mental health challenges, 152 and poor mental health can significantly impact on a woman’s ability to access SHSW care.70,99,102,121,122,124 In addition, poor self-confidence has been associated with holding stigmatising beliefs, 135 and risk-taking behaviour. 124 Midlife women with low levels of self-esteem and sexual assertiveness, and high levels of self-silencing, were more likely to report HIV-stigmatising beliefs than women with higher levels of self-confidence. 135 It can be postulated that holding such views prevented them from accessing services. Women in the United States cited depression, loneliness, low self-esteem and defensiveness, as reasons for engaging in high-risk sexual behaviours.99,124 Similarly in the United Kingdom, feelings of guilt and loss of self-esteem influenced sexual risk taking, and experiencing intimacy was prioritised, and seen as exclusive, to self-protection from STIs. 70 Breast cancer survivors who had lower self-efficacy were more likely to seek help for sexual dysfunction from outlets other than HCPs. 109 Discomfort with thinking about and discussing SHSW, can sometimes be attributed to culturally embedded psychological hurdles to accessing services. Fear, worry and embarrassment have been identified as barriers to cervical screening, 121 two-thirds of postmenopausal women in one study were uncomfortable discussing vaginal atrophy, 102 and discomfort with the topic of sexuality made it hard for cancer patients to seek psychosexual help. 153 The impact of trauma can also pervade healthcare choices, for example one study demonstrated that the experience of trauma was a barrier for adherence to antiretroviral therapy for midlife women. 74
However, some psychological factors, for example the sexual liberation often associated with ageing, have been shown to enable access to SHSW care.123,130 Older women living with HIV in the United States described many different elements which may have prompted them to seek SHSW services: aging was associated with sexual freedom, a growth in sexual expression and increased self-awareness. 123 They described respite from feeling like sexual objects, articulated a renewed sense of autonomy over sexual experiences after divorce and conflicting feelings over a new lack of sexual desire. 130
Competing priorities
Midlife women have many competing priorities. Lack of time to look after themselves,86,153 care-giving responsibilities, 129 increasing prevalence of comorbidities8,61,92,123 and worries about the side effects of treatment and interactions with other medications60,87,90,115,146 can present challenges to accessing SHSW services. Priorities also change with age and circumstance, for example as the risk of pregnancy diminishes, 70 or the need for support with children decreases, 123 factors that have had an impact on SHSW help-seeking, such as the balance of risks versus pleasure, may change.
Stage of the menopause journey was shown to be both a barrier and an enabler to accessing care.74,105 Women aged 40–50 years had better adherence to antiretrovirals than women aged less than 40; the authors suggested that in seeking help for menopausal symptoms, women were exposed to services more often. 105 In contrast, symptoms could interfere with the ability to access care. Two studies found an association between severe menopausal symptoms and suboptimal antiretroviral adherence,74,119 and one study found an association between intensity of menopausal symptoms and reduced HIV clinic attendance. 119
The fear of side effects from treatments (HRT,60,87 HIV PrEP60,85) worry about medication interactions (HIV PrEP on hormone use, 60 hormones on antiretrovirals, 115 antiepileptic drugs and HRT, 146 comorbidity medications on sexual dysfunction treatment 90 ) and other health issues sometimes took precedence over SHSW concerns.76,129 Women described the negative impact of comorbidities on their sex life, physical limitations in sexual activity, and changes in the experience of orgasm, factors which increased their need for, but complicated their access to, SHSW services. 123 Poor self-rated health was associated with less use of preventive care. 61 Women living with HIV were less likely to access hormone therapy for premature menopause than other women. 63 In a UK study, the odds for being sexually active were lower for women who saw themselves as being in bad or very bad health compared with those in very good health. 8 It can be postulated that poor health not only affects the ability to have and enjoy sex, but also to access SHSW services if more sexual activity or satisfaction is desired. Transwomen identified mental health problems as a significant barrier to accessing HIV care63,115 and prioritised gender affirming therapy over HIV PrEP.99,115 Midlife women in the United Kingdom sometimes spent years considering whether to access professional help for sexual difficulties, 90 and 40% of women with vaginal atrophy in one study in the United States waited more than 1 year before consulting a HCP 117 ; this could be attributed to many factors, including competing priorities for their time, attention and health.
Interaction with providers
Four themes emerged about the barriers and enablers imposed by HCPs: women’s perceptions of the knowledge and beliefs of HCPs, the objective knowledge of HCPs, beliefs of HCPs about their own knowledge, and representation of midlife women in SHSW services.
Women’s perceptions of HCPs
Negative encounters with HCPs, including being made to feel dismissed, 130 not taken seriously 90 and encountering ageist, 130 sexist, 130 heterosexist, 130 transphobic, 99 racist 99 and HCP attitudes, fostered an ongoing distrust amongst midlife women of SHSW services. Women in one study in the United States, some of whom also worked as HCPs, felt that HCPs needed more training about the needs of midlife women. 130 Women described poor access to competent physicians, as a barrier to accessing: sexual health following oncological treatment, 93 sexual health in primary care, 76 sexual health concerns, 104 menopause care, 78 sexual dysfunction services for postmenopausal women, 154 transgender competent HIV PrEP care 65 and transgender competent HIV care. 101 In contrast, knowledgeable physicians were described by women as having enabled them to access HRT. 100 The importance of multi-skilled HCPs who could deliver tailored care was highlighted by three studies: women described aspirations to receive personalised, preventative, truthful, unbiased menopause care78,128 and transwomen felt that HCPs should be competent in performing many different roles. 99 Women felt that HCPs should provide more holistic care,30,123 for example they felt that physical activity should have been offered as a possible treatment for the menopause, 30 and sexual satisfaction should have been discussed at the same time that STI care had been offered. 123 Women felt that HCP’s prioritisation of general health over sexual health 34 was a barrier to SHSW services.
Behaviour, such as communication skills, 128 displayed by HCPs influenced midlife women’s access to SHSW care. Women wanted to feel equal in the decision making relationship, 81 and physicians who made unilateral decisions 100 were viewed as barriers to care. Approachable HCPs, who were non-judgemental and did not make assumptions about them, 108 and who were able to develop a good rapport, 76 and normalise age-related changes, 130 encouraged them to access services. Physicians across primary and secondary care and a range of specialties were reticent to initiate conversations about sexual health,76,90,154 yet women stated that they would have preferred physicians to broach sexual health topics.55,102,105,108,124,150 Women surmised that HCPs did not broach sexual health topics due to embarrassment, ageism and social taboos around older women and sex 76 ; it was not specified whether the gender of the HCP made any difference to women’s assumptions.
HCP’s knowledge and beliefs
A range of HCPs support the SHSW of midlife women; the review found there was a need for better training in this subject across this group of professionals.69,75,90,106,112,146 In one study, 52% of women living with epilepsy who had discussed the menopause with their HCP still wanted more information. 146 In the United Kingdom, there were too many missed opportunities to test women for HIV, which had resulted in (preventable) irreversible consequences. 112 Similarly, a different study found that contraception had only been documented to have been offered to 15% of eligible women living with HIV. 69 HCPs questioned whether menopause was even an issue for immigrant Hispanic women, indicated that socialisation to minimise gynaecological discomforts limited the significance of their symptoms, and believed (without any evidence) that women were managing their symptoms through local medicine women. 78 The majority of women in one study, despite having conditions which were known to affect sexual function, had never been asked by their GP about sexual well-being. 90 Furthermore, a large survey in the United States which explored sexual concerns, found that most women wanted to discuss these with a HCP (but had not managed to), but encouragingly the discussion had proved helpful for those who had done so. 104
Compelling evidence demonstrated an appetite among HCPs for better, wider-ranging training.67,75,83,88,106,110,127 A questionnaire for community HCPs about HRT, 110 a questionnaire eliciting nephrologists’ confidence in SHSW for women, 88 a questionnaire investigating barriers to sexual dysfunction screening, 127 interviews exploring competence in sexual healthcare, 67 a questionnaire which determined HCP trainees’ views in delivering perimenopausal care, 83 a study of HCPs caring for survivors of sexual assault 75 and an evaluation of a hub-spoke model, 106 verified lack of HCP confidence in SHSW issues, and a desire for further education among HCPs. Training needs identified included taking a non-judgemental sexual history, using culturally appropriate terms, and management of work flow in the clinic. 106 The initial findings of the Women’s Health Initiative, a large-scale national trial, influenced the professional and public health narrative about the dangers of HRT, 64 and thereby controversially continues to negatively impact on practitioner’s HRT prescribing rates. 155 However, a positive fall-out of the study was that many HCPs expressed the feeling that patients should be the main decision-maker with regard to HRT. 64
Representation in healthcare
A UK-based study which explored women’s midlife transitions, 130 and a study in the United States which investigated unmarried midlife women’s sexual health-seeking behaviour, 108 found that midlife women welcomed more female representation in healthcare. Women in the United States expressed a preference for an older female provider when discussing menopause treatment. 71 Correspondingly, women with type 2 diabetes viewed female HCPs as facilitators to them accessing sexual healthcare discussions, 76 and having a female physician correlated with women having had a cervical smear. 86 Arab women’s low use of preventative healthcare was related to a lack of physicians of the same culture and gender. 61
Organisational factors
Perceptions of healthcare systems
Institutional distrust was a barrier to healthcare services 130 within the remits of: access to HRT, 100 HIV care for women, 113 and HIV care for transwomen.115,123,133,143 Systems which offered emotional and information support together with clinical care were viewed as enablers to accessing care for transwomen.133,156
Format of healthcare systems
Strategies to make healthcare systems more accessible that were proposed centred around combining expertise 88 and services,106,133 and establishing women-only clinics.54,123 Nephrologists suggested that interdisciplinary clinics could improve their ability to manage women’s SHSW needs. 88 Similarly, combining SHSW services,53,54,99,101,129,133,135 co-locating SHSW services within other existing healthcare services, 99 and self-service and self-testing possibilities,97,122 were suggested as possibilities to improve access. HCPs in one study felt that a recall-based system, employed in many other countries, would have improved cervical screening rates among an Aboriginal community in Canada. 98 Canadian women in this study also advocated policy change to allow health professionals other than physicians to prescribe HRT. 100 This would improve access, by increasing the availability of services. Enablers for access to SHSW services that were suggested for transwomen included creating trans-positive environments and services with trans-positive policies, 75 co-location of gender-affirming and other SHSW services,54,99,101,133 and including social care provision. 129 Transwomen preferred services in a safe space away from men,54,123 and valued anonymous services. 133
Community factors
Cultural factors
Although stigma is a cross-cutting theme which affects all levels of the SEM, 157 here we concentrate on the effect of stigma in the community as a barrier to SHSW care. Fourteen studies attributed community-based stigma to be a barrier to midlife women accessing a wide range of SHSW care: sexual function care, 90 postmenopausal sexual healthcare, 154 menopause care,22,29,78 HIV care, 113 preventive sexual health services 135 and specific to transwomen: sexual health,54,133 HIV PrEP 60 and HIV care.99,103,115,133
Social norms influenced SHSW care-seeking behaviour. For example, normalisation of condomless sex with new partners, paying for sex and ‘othering’ of those at risk of STIs, were barriers to SHSW services. 24 Women experienced age-gender barriers to accessing condoms in shops and pharmacies 24 and described seeking help for sexual difficulties as only being appropriate up to a certain age. 90 Cultural expectations of stoicism around menstruation and menopause prevented Hispanic women from seeking help. 78 Similarly, it can be postulated that the stigma and lack of understanding from healthcare colleagues prevented nurses in the menopause transition in one study from seeking help. They described how ‘tiredness related to menopause symptoms was not socially acceptable’, and one woman described how (at work) ‘you just get on with it, that sort of thing’. 22
Evolving cultural landscapes may have complicated women’s ability to access SHSW services. A study which investigated gender-based violence described how the (increasing) normalisation of violence affected the healing process, 118 and this cultural norm may have been a significant barrier to accessing care for some women. At the conclusion of a long-term relationship, some women felt pressured to re-partner to fit into (current) ‘couple culture’, 24 whereas others described how sexual liberation from the fear of pregnancy, and from the traditional gender norms of when they were younger, such as the expectations of being in a committed relationship and needing financial support, 123 meant that they had chosen more partners and sex whenever they wanted, compared to in their younger years. 123 These changes in cultural expectations may have contributed to midlife women struggling to identify when to use SHSW services. However, prevalent social ideas may have prompted some women to seek SHSW care. For example, a content analysis of women’s magazines in the United States found the portrayal of sex as good exercise which benefitted the health of women, and the implication that a woman was responsible for her husband’s sexual fulfilment, as recurring themes, 68 both of which may have encouraged women to access SHSW services.
Social connection
Relationship dynamics and communication affected whether safe sex was practised. 123 Women who were partnered were more likely to seek help for sexual health concerns after breast cancer treatment than those without a partner, 109 but partnership with somebody not interested in (or capable of) sex significantly contributed to sexual inactivity.8,92 One woman described ‘missing the closeness of cuddles before and after’ but also ‘feeling sorry for my husband’ (beta-blockers and arthritis affected his ability to have sex). 8 Another woman explained that because the sex practices she had previously enjoyed with her partner were no longer possible, they did not want to explore alternatives. 8 In a different study, women described sex as less pleasurable compared with when they were younger due to their partner’s impaired sexual performance, and unhappiness and the feeling of being trapped in sexless relationships. 123 These relationship complexities may have made accessing help challenging, even though it may have been desired. Conversely, women in a UK study described continuing to have sex despite a health-related reduction in their own sexual desire for the benefit of their partner. 8 This highlights the need for holistic SHSW services for older couples, which include relationship counselling. Anxiety about communicating with intimate partners had a negative impact on access to services. One study demonstrated how inhibitions relating to conversations about sex with their partner prevented older adults from seeing professional help for sexual difficulties. 90
Studies which investigated the nature of healing from gender-based violence, 118 the repercussions of trauma experienced by transwomen living with HIV, 54 and the legacy of unwanted sexual experiences on midlife women, 123 highlighted themes which encompassed the need to learn how to reconnect with others, and the importance of belonging to a community in terms of facilitating access to SHSW services. Similarly, an exploration of the inclusion of transwomen in HIV services found that ciswomen’s openness to education about trans issues was much better than the trans community expected. If their receptivity had been recognised, social connection and enhanced inclusivity in services may have been accomplished more successfully. 54 Without awareness and understanding from colleagues, nurses in the menopause transition felt judged and uncertain of the validity of their own experiences. 22 It is likely that if women working in healthcare settings are sometimes expected to minimise their menopause symptoms, women in other workplaces may also be discouraged from accessing care by the expectations of employers and other employees.
Intergenerational factors
Midlife women matured in a context of different sexual norms, sex education and SHSW campaigns. Midlife nurses in one study explained how female relatives had not helped to prepare them for the menopause by not discussing their experiences in any detail or depth. 22 In contrast, one study demonstrated that younger relatives positively influenced midlife women’s understanding of sexual safety, and thereby enabled access to care. 24 Women in a study in the United States railed against ageist stereotypes about their sex lives. They narrated how younger generations thought older women should not be sexually active, and how younger men perceived sex with older women as lower risk behaviour, and therefore expected condomless sex. 123 Their ability to challenge this fallacy may have empowered them to access appropriate SHSW services. In contrast, other studies depicted midlife women as othering themselves from young people’s behaviour, despite engaging in similar risks. While midlife women perceived condoms as associated with youth, 24 they also described pressure to adjust to a new sexual culture quickly, leading to rapid progression to sex in new relationships. 70
Public policy
Public health messages
In a study about risk taking in 40–65 year olds, participants described disconnection from safe sex promotional services. 24 The study identified a discrepancy between the positive broader public discussion about sexuality, and the sensationalised media coverage of sex in older women. 24 These confusing messages may have contributed to increased stigma and discomfort around sex in the midlife and may have affected women’s decisions to access SHSW services. When discussing HIV PrEP campaigns, there was a concern that information was not available in the places that midlife women would frequent: they advocated for it to be advertised all over the city on the buses, metro stations, on doors, in doctors’ offices and social media, with phone numbers to contact. 85 Transwomen described the need for better quality of public health campaigns. They worried about the need for clarity in messages about the lack of interactions between feminising hormones and HIV PrEP 65 and felt that HIV PrEP adverts needed to include trans-specific messages 60 in order to begin to tackle some of the barriers to uptake.
Although there are many barriers and enablers to SHSW care that are uniform across high-income countries, public health messages may benefit from being country specific. An international survey of four high-income countries found marked differences between the nations: 51% of postmenopausal women in the United States compared to 10% in Finland were aware of local treatment options for vaginal atrophy. 158 There was a similar significant discrepancy between high-income nations in a study which examined HRT prescription rates. 87 The identification of risk behaviours and group or nation-specific problems could help to target messages, for example, Parkes’s latent class analysis of NATSAL-3, which identified six classes for women, including ‘unwary STI risk takers’. 107
Material barriers
The material barriers to accessing SHSW which were identified included: financial challenges,121,133 transport difficulties,121,129 shortage of both HCPs and the time that they can offer78,83,98,100,127,128 and poor mainstream treatment options. 78 Cost of care was found to be a barrier to accessing cervical screening 122 and HIV care 133 in the United States, SHSW services during the menopause in Hong Kong, 29 and bioidentical HRT in Canada. 100 Transwomen living with HIV proposed that financial incentives to meet their basic needs would be a facilitator to accessing HIV care. 133 Similarly, some women discussing HIV PrEP in focus groups in the United States felt that financial incentives should be attached, although others felt that preventing HIV itself should be the incentive. 85 Limited transport options were found to be barriers to accessing cervical screening in Canada 98 and the United States,98,122 and HIV care in the United States. 133 Both women and HCPs felt that better availability of HCPs would improve access to SHSW services. A shortage of appropriate HCPs 98 and not having a primary care physician 86 were associated with worse cervical smear uptake in the United States. HCPs felt that lack of consultation time was a significant barrier to providing good SHSW services,78,83,127 particularly in relation to menopause care78,83 and sexual dysfunction care. 127 The lack of treatment options available for conditions affecting midlife women’s SHSW, such as sexual dysfunction, 90 and menopause,34,87 may inhibit women from seeking, and HCP from offering, some SHSW services. A woman in one study expressed ‘I talk to mums everyday about babies and everything . . . there are so many variations on how it is for premenopausal women, like maybe we don’t really understand enough’. 22 The lack of prioritisation for research into treatment options for conditions that affect midlife women means that even for those women who are able to access care, it can often feel fruitless.
Mobile technology, for example, applications have been used to improve access to menopause services. 116 An analysis of 18 menopause applications found that data reports and visualisations encouraged application users to seek out help and facilitated conversations with HCPs. 116 In particular, applications with clear links to HCP support were viewed positively by application reviewers, and all of the three applications with HCP support had ‘good’ quality scores. 116 Importantly, however, few of the menopause applications were explicitly supported by HCPs, and many scored poorly in relation to the credibility of the source. 116 A different study corroborated this: only 22.7% of the applications analysed had documented evidence-based practice in the form of guidelines or treatment protocols. 41
Discussion
To our knowledge, this is the first systematic review of the evidence that addresses the barriers and enablers to SHSW care for women aged 40–65 years in high-income countries. The gender disparity in healthcare research, 159 the ethical challenges of conducting SHSW studies 160 and the sociocultural pressures of the midlife phase, 18 together with the increasing prevalence of general health issues which may both impact on sexual health and facilitate increased access to HCPs, 24 resulted in limited, evolving and sometimes conflicted evidence with regard to the factors affecting access to services. Most research to date has identified the barriers and enablers that cisgender women encounter in accessing sexual health services. Encouragingly, there is increasing representation of transwomen in the literature and a developing recognition of the importance of sexual well-being.
The limited number of interventions that have been trialled to improve access to SHSW services for midlife women have mostly been found to be efficacious. 161 The majority of successful interventions have included education or knowledge sharing (including health literacy and support and healthcare system navigation), been tailored to the specific population or sub-population (e.g. cancer survivors) and have included a diversity of methods of communication with which to engage participants.162 –168 Studies indirectly exploring interventions to improve access to SHSW care in midlife women living with and surviving cancer provide valuable insights to guide future research. Examples include evidence for readily accessible self-treatments such as comparison between vaginal lubricants in breast cancer, 169 physical activity to improve sexual well-being in endometrial cancer 170 and technological psychoeducational interventions for breast, colorectal and gynaecological cancer survivors (telephone, text and internet approaches) which were found to reduce geographical barriers and confer convenience (ill health, competing care giving/work responsibilities) and privacy advantages.166,171
Consistent evidence has emerged about the wide disparity in access to care within the high-income setting. The intersecting disadvantage of being a midlife woman from an under-resourced group provides a clear indication as to where services should be focused. There is compelling evidence, and appetite for, multi-format, updated, education about SHSW issues and services for midlife women, their communities and their HCPs (across specialties166,172), not least so that improved, more equitable care can be advocated for. Mobile technology has been employed to democratise menopause education, but information on applications must be evidence-based 40 and extended to other SHSW issues. We must capitalise on both intergenerational and peer-led learning and targeted community action 173 to address unacceptable norms such as the socialisation of women to minimise discomfort, the framing of sexual dysfunction from a solely male perspective and to destigmatise and improve inclusivity of sexual health and well-being services for all midlife women.167,174 Public health messages focusing on predictors of risk behaviour, offering more evidence-based self-care interventions175 –177 and steering the cultural discourse to positive, safe, enjoyable midlife sex for women are required. The impact of poor mental health provision on access to SHSW services should not be underestimated.162,165,178 The false economy of denying midlife women the holistic, free, easily accessible and integrated SHSW services that they deserve must be recognised.
Strengths and limitations of the systematic review
The variety of study designs, comprising of qualitative, quantitative and mixed methods studies, prevented meta-analysis of findings. However, the inclusion of a wide range of methodologically diverse studies, and the narrative synthesis, enabled the emergence of complex themes, providing an in-depth understanding of the barriers and enablers to SHSW care for midlife women. The qualitative evidence complemented the quantitative results. For example, cohort and cross-sectional studies identified the more marginalised groups of women, and qualitative findings helped to describe the barriers faced by those women in their own words or the words of their HCPs.
SHSW services are deliberately combined in this review in an effort to support the World Health Organization’s approach of acknowledging positive sexuality and sexual experiences as key public health outcomes that are intrinsically linked with sexual health. 11 However, SHSW services are inconsistently conceptualised. Although the review sought to include all SHSW services as per Mitchell’s 2021 framework, 11 SHSW services in high-income countries that have been defined in different ways may not have been captured. Many of the included studies excluded an important group of transgender and gender non-binary people who have SHSW needs and experiences that are similar in some ways, but also unique, to those of cisgender women. 179 Research lags behind our understanding of the imperative necessity to recognise and distinguish between the needs of women with non-binary and transgender identities. Most studies included in the review are presumed to have been conducted on cisgender women, but we are unable to differentiate women who were not asked, and those who did not want to reveal their gender identities. Therefore, we are unable to judge whether the review reflects access to care for non-binary and transwomen.
The exclusion of non-English language articles may have resulted in the lack of representation from important national and cultural perspectives. Furthermore, most studies were conducted in English-speaking countries, which impacts on the generalisability of the results for women living in non-English speaking countries. Although this review investigated the barriers and enablers to accessing care for women in high-income countries, only a small number of studies specifically addressed access to care for women resident, but who had not been born in, these countries. These women have unique needs, and further research is required to elucidate how to distinguish their challenges in accessing care from women resident in the countries in the high-income countries in which they were born.
Strengths and limitations of the included studies
Overall, the quality of the reporting of the studies was high, with sound methodology and valid results. Studies addressed clearly focused issues. Study methodologies were appropriate for the aims of the studies, and closely aligned with the outcome measures. Half of the studies did not include the race or ethnicity of the participants, which may have had a significant bearing on the barriers and enablers to accessing care. When race or ethnicity was specified, most studies attempted to include women of different races and ethnicities, with mixed results.
Strong theoretical foundations for the work were clearly elaborated in most studies. Many studies used convenience sampling strategies, which may have resulted in an overrepresentation of women who were better able to overcome barriers to accessing care, and women who were already seeking care. Qualitative studies used focus groups, interviews or a mixture of both methods considered appropriate for eliciting views on sensitive topics such as SHSW. 180 However, few of the qualitative studies reported on the quality assessment criteria of ‘reflexivity’, the acknowledgement of cultural bias in the researcher–participant relationship. Many of the quantitative studies were cross-sectional studies, either cross-sectional designs or cross-sections from other research samples. Most surveys were administered individually and verbally, modes considered most accessible for those with low literacy. 180 However, some surveys required computer literacy, which will have excluded more marginalised and women in the older bracket of midlife, rendering the findings less generalisable.
Implications for clinical practice and future research
Clinical practice
SHSW is interlinked with many aspects of mental and physical health and should therefore be provided as an important component of holistic care. Midlife can be viewed as a time of opportunity, where education about positive links between the adoption of sexual health and well-being behaviours can promote a healthier older age. HCPs with a range of roles and responsibilities, require and desire better training in delivering, and signposting, midlife women to SHSW services, and should therefore be offered appropriate training to give them the confidence and ability to do so in an inclusive, sensitive manner.
Policy
Maintaining an active, satisfying and fulfilling sexual life as women age is positively linked with life satisfaction. 182 It is evident that policies which optimise SHSW as integral parts of holistic healthcare benefit women and the societies in which they live. There is a crucial need to advocate for policy change and social campaigns aimed at raising awareness among policymakers, workplaces and communities about the SHSW needs of midlife women. Such initiatives are essential for ensuring that appropriate resources and support are allocated to address the unique challenges faced by this demographic. This review demonstrates that midlife women can enjoy the changes that midlife brings to their SHSW but that they face many barriers to accessing research and services. Policies to educate the public and de-stigmatise SHSW and SHSW services are overdue. Women, especially those from the most under-served groups, must have access to high-quality information; this will help to address other barriers to care such as gender-age dynamics and harmful social norms. The competing priorities that midlife women juggle must be acknowledged within policies, by ensuring flexible appointment times, childcare options, knowledgeable employers and considering accessible one-stop or integrated and interdisciplinary services, with innovative delivery such as self-service and self-testing. Inadequate consultation time and lack of skilled HCPs are pervasive issues, and in countries where women pay for SHSW services, cost is a barrier to vital services.
Future research
Research about how to best enable the participation of midlife women, particularly those who belong to under-resourced groups, in SHSW research is needed. Midlife women’s voices can then be used to prioritise management strategies, including treatment options, education, use of technology and implementation of accessible services. Future research should include longitudinal cohort studies for in-depth examination of the sexual health and well-being challenges of midlife women, randomised controlled trials, with implementation science elements, to test service designs, for example women-only services, and targeted public health messages, as well as qualitative research such as in-depth interviews, focus group discussions and co-creation of education and policies, to ensure that midlife women’s voices are always at the forefront of new policies.
Conclusion
The advent of the physiological and psychological changes that midlife brings to women can serve as an opportunity for workplaces, HCPs, communities, healthcare organisations and women themselves to evaluate, improve access to and co-create essential sexual health and well-being services. Implementation of changes must be evidence-based, and address the wide disparities in access, and the intersecting disadvantages of under-served groups.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241277723 – Supplemental material for The barriers and enablers to accessing sexual health and sexual well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057241277723 for The barriers and enablers to accessing sexual health and sexual well-being services for midlife women (aged 40–65 years) in high-income countries: A mixed-methods systematic review by Kiersten Simmons, Carrie Llewellyn, Stephen Bremner, Yvonne Gilleece, Claire Norcross and Collins Iwuji in Women’s Health
Footnotes
Acknowledgements
We would like to thank the Public Participant Involvement group for their advice, Dr Johann McGavin for his ongoing support, and Scott Innes, Senior Library Assistant at Sussex Health Knowledge and Libraries, for working extremely hard to source some of the articles.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.