
Abstract
An 18-y-old American Saddlebred mare was admitted with fever and acute onset of neurologic signs including grade 3 of 5 ataxia, difficulty in prehension, and dull mentation. Because of financial restraints, desired testing could not be performed; the horse’s condition declined despite supportive treatment, and euthanasia was elected. Postmortem examination revealed petechiae and ecchymoses in the meninges and neuroparenchyma of the encephalon. Blast-like neoplastic round cells were identified within the vasculature and areas of hemorrhage in the neuroparenchyma, the intestinal submucosa, and other organs, including the liver, kidney, lung, and mesenteric lymph node. Necrotizing enterocolitis and acute fibrinonecrotizing bacterial pneumonia were also noted. Of the atypical round cells in the encephalon, >70% expressed ionized calcium–binding adapter molecule 1 (Iba1), 10–20% expressed myeloperoxidase (MPO), and <10% expressed PAX5, CD3, CD20, CD79a, or MUM1. The bone marrow was diffusely effaced by neoplastic round cells expressing Iba1, and ~70% of these cells expressed MPO with no expression of CD3 or CD20. CD172a also immunolabeled a portion of the neoplastic cells. These findings were consistent with the diagnosis of acute myeloid leukemia-M1 with an unusual neurologic presentation.
An 18-y-old American Saddlebred mare was admitted because of an acute onset of neurologic signs that has been present for 1 d, abnormal behavior, and fever of 40°C. The mare had dull mentation, grade 3 of 5 ataxia, difficulty in prehension, and poor body condition (3 of 9). Tachycardia (68 bpm), tachypnea (30 breaths/min), dyspnea, body temperature of 38.8°C, and injected mucous membranes with capillary refill time at 2–3 s were also noted. Because of financial constraints, a full diagnostic work-up including CBC could not be performed. Blood was collected for point-of-care blood analysis (epoc; Siemens), PCV, and total protein analysis (Table 1). Despite supportive treatment, the horse’s neurologic status worsened overnight, and euthanasia was recommended.
Enterprise point-of-care blood analysis, PCV, and total protein (TP) analysis.

On postmortem gross examination, the cerebrum, cerebellum, and brainstem had widespread pinpoint hemorrhages in the meninges and gray and white matter (Fig. 1A). Throughout the small intestinal mucosa, there were multifocal-to-coalescing, yellow-to-tan, rough, well-demarcated, mildly raised mucosal plaques with a central depression (ulceration), affecting the duodenum most severely (Fig. 1B). The cecum and the large colon had similar but milder changes. The pleural surface of the lung had widespread dark-red, flat to mildly raised, round foci of up to 1 cm diameter, and the cranioventral edges of the lung lobes were dark-red with pleural fibrin deposition. The subcutis, peritoneal serosa, thoracic wall, and epicardium had widespread petechiae and ecchymoses.
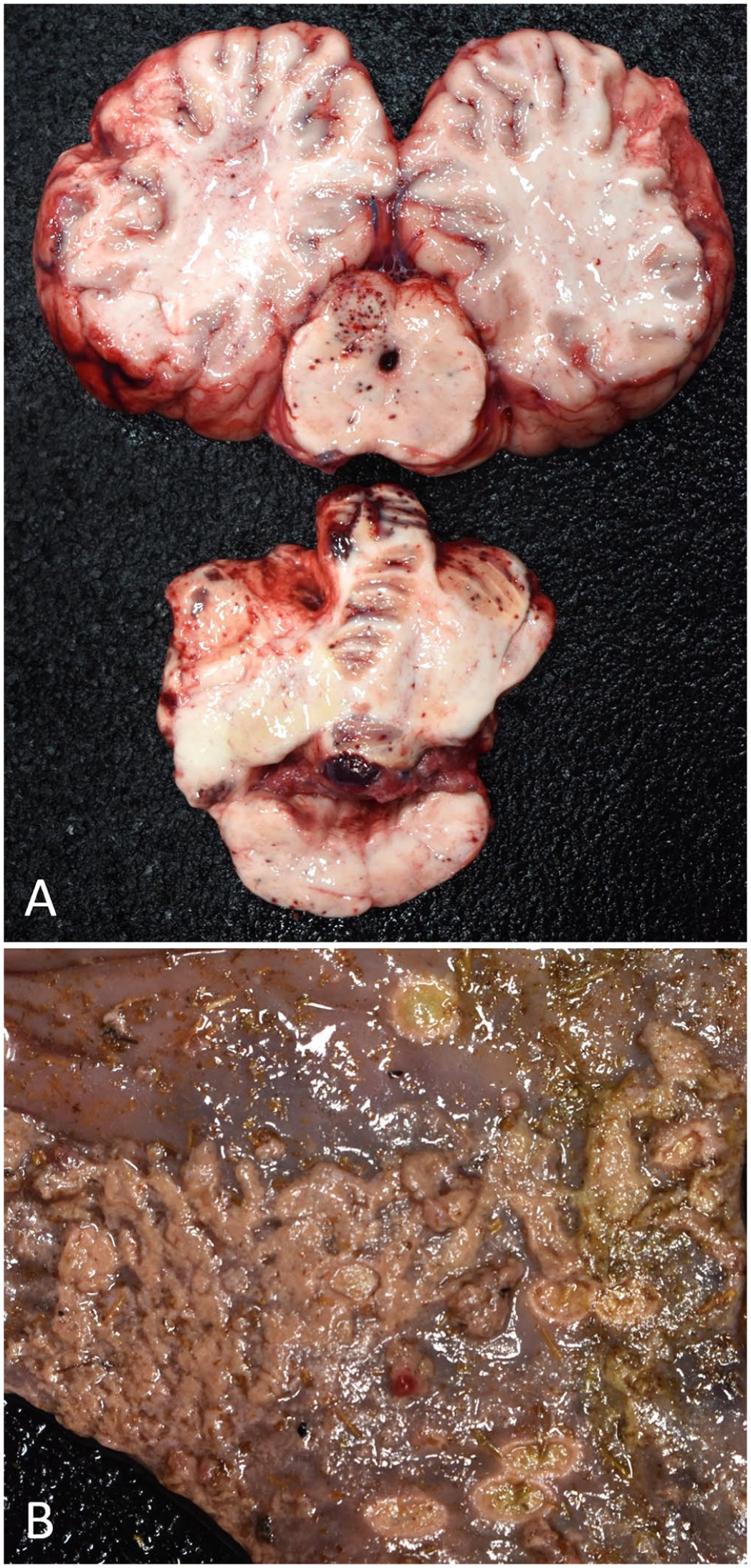
Gross lesions in a horse with acute myeloid leukemia.
On microscopic examination, the cerebrum, cerebellum, and brainstem had randomly distributed foci of hemorrhage in the meninges and neuroparenchyma, containing small aggregates of neoplastic round cells (Fig. 2A). The neoplastic round cells had small amounts of pale eosinophilic cytoplasm and round-to-indented nuclei which were 2–4× the size of an erythrocyte on histopathology, with coarsely stippled or vesicular chromatin. Similar neoplastic round cells were also within blood vessels; rare intravascular mitotic figures were noted (Fig. 2B). The cerebral and cerebellar gray matter had edema. On immunohistochemical analysis (Suppl. Table 1), >70% of the neoplastic round cells in areas of hemorrhage had weak-to-strong cytoplasmic expression of ionized calcium–binding adapter molecule 1 (Iba1), and 10–20% of the neoplastic round cells had cytoplasmic expression of myeloperoxidase (MPO; Fig. 3A, 3B). Less than 10% of the cells expressed nuclear PAX5, membranous CD3, CD20, or CD79a, and rare cells had weak nuclear expression of MUM1 (Suppl. Fig. 1). Rare cells in the hemorrhagic areas had cytoplasmic expression of CD163; CD204 was not expressed in the neoplastic cells. Approximately 10% of the cells in the hemorrhagic areas had cytoplasmic expression of MHC class II, and calprotectin. CD172a was expressed in some neoplastic cells; however, interpretation was difficult as nonspecific staining was extensive, including in the neuropil and vascular walls (Suppl. Figs. 1, 2). Scattered perivascular aggregates of similar neoplastic round cells were also identified in the liver, kidney, lung, and mesenteric lymph node; the ones in the liver and kidney expressed strong cytoplasmic Iba1.
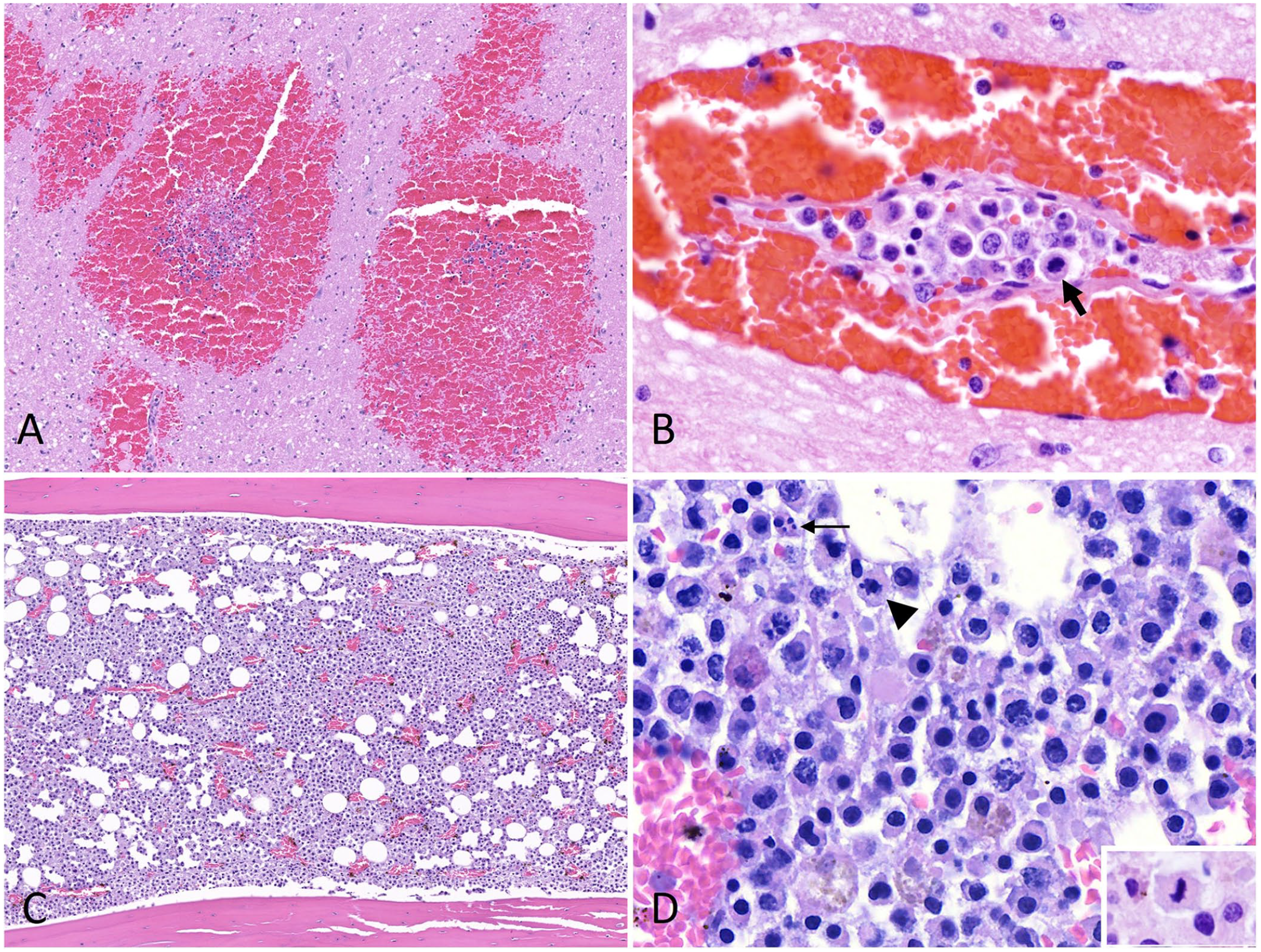
Histologic lesions in a horse with acute myeloid leukemia. H&E.
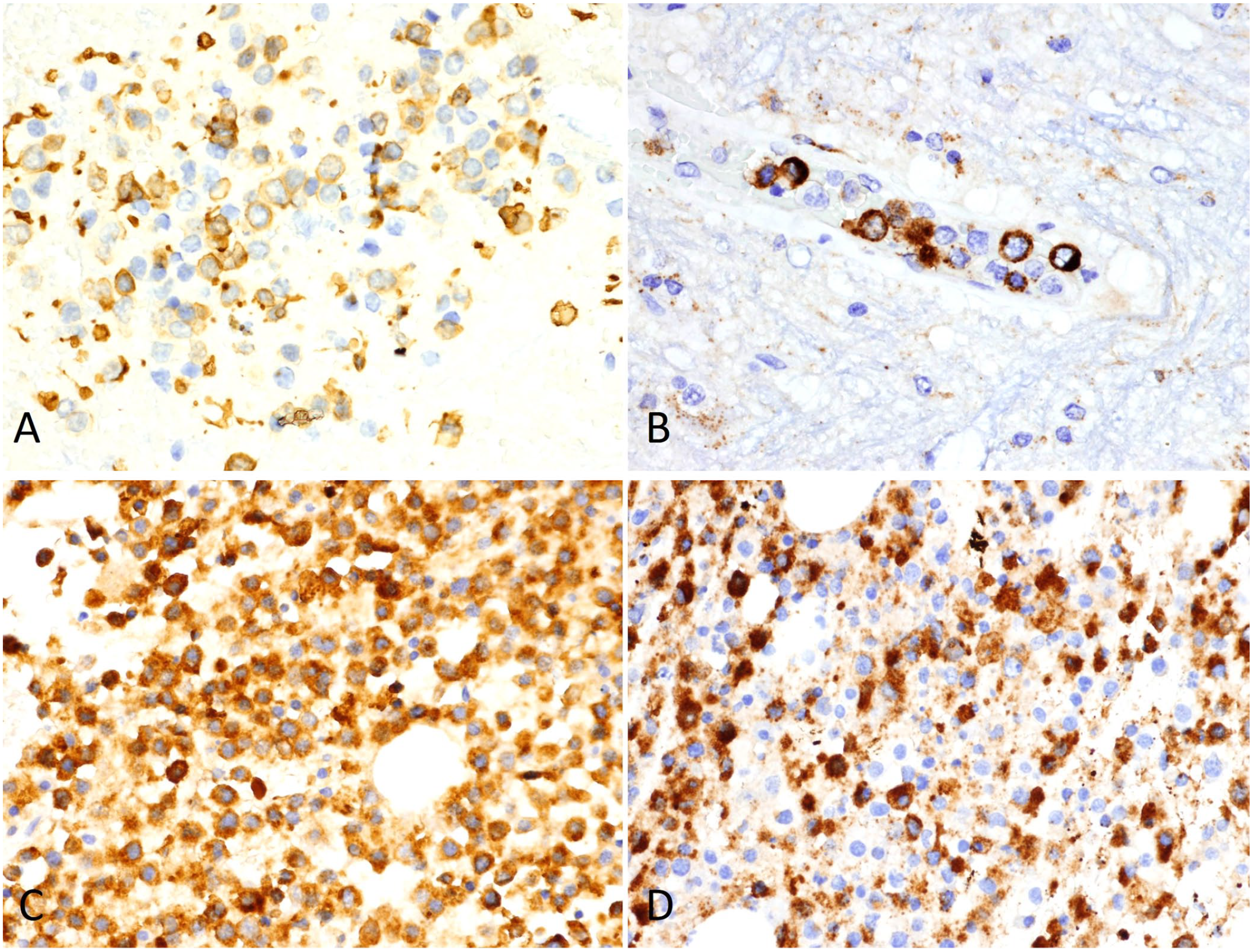
Immunohistochemical stains in a horse with acute myeloid leukemia.
The small intestinal mucosa had multifocal coagulative necrosis occasionally extending to the tunica submucosa and tunica muscularis, colonized by mixed bacteria, predominantly long bacilli, with thrombosis, vascular fibrinoid necrosis, edema, fibrin exudation, hemorrhage, and neoplastic round cells identified in areas of hemorrhage and within the vasculature. Necrohemorrhagic pleuropneumonia associated with mixed colonies of bacilli and cocci was also noted. The bone marrow had ~90% cellularity and was almost completely effaced by sheets of neoplastic round cells with moderate amounts of pale eosinophilic cytoplasm and round hyperchromatic nuclei with occasional karyorrhexis. The mitotic count was 6 per 2.37 mm2 (Fig. 2C, 2D). Megakaryocytes were absent, and only a few scattered granulocytic and erythroid lineage cells were noted. The neoplastic round cells in the bone marrow diffusely expressed Iba1, and ~70% of the cells expressed MPO (Fig. 3C, 3D). CD3 and CD20 were not expressed by the neoplastic cells, and CD172a was difficult to interpret due to nonspecific staining (Suppl. Fig. 1). Sporadic cells comprising <10% of the cells in the bone marrow had strong expression of CD163, CD204, MHC class II, and calprotectin, likely representing resident macrophages (Suppl. Fig. 2). Based on the diffuse Iba1 expression in the neoplastic round cells effacing the bone marrow and ~70% of these cells expressing MPO, with circulating blast-like cells expressing the same markers and lack of lymphoid marker expression, a diagnosis of acute myeloid leukemia (AML) was warranted. According to the 2008 updated and 2016 revised WHO criteria, this AML would be classified as AML-NOS (not otherwise specified) with morphology of AML without maturation (AML-M1).1,15,16,17
A direct immunofluorescence antibody test for rabies virus and RT-qPCR assays for eastern equine encephalitis virus (EEEV) and West Nile virus (WNV) were performed on the brain tissue. No rabies virus antigen nor nucleic acids for EEEV or WNV were detected. Bacterial culture was performed on the small intestine and lung, and ELISA for clostridial toxins was performed on small intestinal contents. From the small intestine, Bacteroides fragilis, B. pyogenes, Clostridium cadaveris, and Prevotella heparinolytica were recovered on anaerobic culture, and Escherichia coli and Providencia stuartii were recovered on aerobic culture. No Salmonella sp. was isolated from salmonella enrichment culture. No clostridial toxins were detected via ELISA for alpha, beta, and epsilon toxins for Clostridium perfringens or A and B toxins for C. difficile. From the lung, Acinetobacter baumannii, Pseudomonas aeruginosa, and Streptococcus equi subsp. zooepidemicus were cultured.
Leukemia is a malignant neoplasm arising from hematopoietic cells in the bone marrow and can be classified into either lymphocytic or myeloid types and either acute or chronic depending on the cell of origin and the percentage of blast cells (>20%) in the bone marrow or blood, respectively. 13 Acute leukemia is rare in horses and is typically suspected if there is uni- or multilineage cytopenia on the CBC, with circulating blast cells, in the absence of primary inflammation and/or infection. The observation of >20% of blast cells in bone marrow aspiration or core biopsy confirms the diagnosis. 7 The most consistent CBC findings in equine acute leukemia include thrombocytopenia, neutropenia, and anemia.2,7,11 Also, circulating neoplastic blast cells have been consistently identified on blood smear.2,7,11
In our case, antemortem CBC and blood smear evaluation were not performed as it was not anticipated to be diagnostic, and the diagnosis of AML was made on postmortem examination, based on blast-like neoplastic round cells effacing the bone marrow and scattered within and around blood vessels in multiple organs, and immunohistochemistry demonstrating expression of Iba1 and MPO. The most commonly reported types of AML in horses are myelomonocytic and monocytic AML. 13 Iba1 is a marker used for labeling of microglial cells in multiple species and has high diagnostic value in diagnosing histiocytic disorders in dogs and cats. 12 Iba1 also has been used as a marker in diagnosing AML in a veiled chameleon 8 and acute myelomonocytic leukemia in a Holstein cow. 10 In a 2021 study, Iba1 was reported to have high sensitivity and specificity in diagnosing monocytic AML in human formalin-fixed, paraffin-embedded (FFPE) tissues, outperforming CD14, CD68, and CD163. 19 In horses, Iba1 expression in AML has not been tested extensively. According to a study of acute leukemia cases in 6 horses, Iba1 was expressed in 2 AML cases but also in 2 B-cell acute lymphoid leukemia (ALL) cases; therefore, Iba1 was not used as a marker to classify the leukemia in that study. In another study of acute leukemia cases in 12 horses, Iba1 was expressed in 20–30% of blast cells in AML cases but was not tested in ALL cases. 7 In the same study, Iba1 was also expressed in rare lymphocytes in the paracortical T-cell–rich region of dog lymph node sections and in some blasts in equine bone marrow. The usefulness of Iba1 as a diagnostic marker for AML in horses needs further investigation; therefore, while expression of Iba1 may suggest monocytic differentiation, we did not use such criteria to further classify the AML in our case.
Expression of MPO indicates myeloid differentiation; MPO is expressed in myeloblasts and further-differentiated myeloid cells as well as in promonocytes and further-differentiated cells.15,16 MPO is used in dogs to classify hematopoietic neoplasms, 15 but it has not been used in horses. Our report shows that MPO can be used in horses to classify leukemia. CD172a is another granulocytic and monocytic myeloid marker used in horses.2,7,15 In our case, while a portion of the neoplastic cells expressed this marker, significant nonspecific staining made the interpretation difficult. To investigate monocytic differentiation of the neoplastic cells, we performed, using previously reported clones of antibodies in horses, 6 IHC for CD163 and CD204, which are scavenger receptors in monocyte-macrophage lineage; MHC class II, which is found on antigen-presenting cells, such as dendritic cells, mononuclear phagocytes, thymic epithelial cells, and mature B cells; and calprotectin, which is expressed in recently infiltrating monocytes-macrophages; however, these markers were either not expressed or expressed in a very small subset of neoplastic cells in our case.
Clinical signs in horses with acute leukemia are usually nonspecific and include fever, tachycardia, anorexia, tachypnea, and spontaneous bleeding.2,7 Our case had, in addition to these clinical signs, acute onset of neurologic signs, which initially raised concerns for primary neurologic diseases including equine alphaherpesvirus 1, WNV, EEEV infections, and tetanus. Neurologic signs as manifestations of acute leukemia have been reported in a horse with B-cell ALL 2 and humans with AML. 14 In humans, neurologic complications associated with AML are caused by either direct invasion of the nervous tissues by neoplastic cells or by vascular complications secondary to hyperleukocytosis or disorders of coagulation. 14 In our case, the neurologic signs were attributed to multifocal hemorrhage in the encephalon. The pathogenesis could involve thrombocytopenia as suggested by the absence of megakaryocytes in the examined bone marrow, and disseminated intravascular coagulation (DIC), which can be a complication of AML. Vascular occlusion by neoplastic leukocytes was also considered as a potential pathogenesis for the hemorrhage in our case as aggregates of neoplastic cells were noted in the areas of hemorrhage. In humans, hyperleukocytosis, which is defined as WBC counts >100 × 109 cells/L, can occur with leukemia, most commonly in AML, occurring in up to 18% of the patients, with monocytic and myelomonocytic AML subtypes identified as increased risk factors. 3 Hyperleukocytosis is associated with leukostasis causing tissue hypoxia, DIC, and tumor lysis syndrome. In horses, leukostasis has been reported in 2 myelomonocytic leukemia cases, one with hyperleukocytosis 4 and one without leukocytosis. 5 Without an antemortem CBC result, whether thrombocytopenia and DIC or hyperleukocytosis and leukostasis played a role in the pathogenesis of the intracranial hemorrhage would be difficult to prove, but these are possibilities.
Necrotizing enterocolitis and bacterial pneumonia were also noted in our case. It is unclear whether these were concurrent diseases unrelated to the acute leukemia or if the acute leukemia had predisposed to these. With the absence of a definite pathogen detected from the small intestine on ancillary testing, the enterocolitis is likely secondary to the AML, predisposed by immunosuppression and potential impaired blood perfusion caused by intravascular neoplastic cells. Bacterial pneumonia was also likely predisposed by immunosuppression secondary to leukemia. Aspiration pneumonia associated with the neurologic signs or embolic pneumonia predisposed by the enterocolitis are possible routes of infection. The azotemia was considered pre-renal as no significant lesions were noted in the kidney other than small aggregates of perivascular neoplastic cells.
Limitations of our report include lack of CBC, blood smear, and bone marrow cytology. The lack of this information posed challenges in further classifying the AML because cytomorphology and cytochemical staining are usually the primary information used to classify AML-NOS, and many antibodies used for immunophenotyping do not work on FFPE tissues. A blood smear should always be performed at a minimum as this can reveal valuable information (e.g., detection of circulating blast cells) and can be performed at a low cost. Also, bone marrow cytology performed on autopsy would have been helpful as most cytochemical stains cannot be performed on FFPE tissues.
It is possible that acute leukemia is underdiagnosed given the ambiguous clinical signs and rapid progression of the disease resulting in death or euthanasia of the patient without pursuing CBC and blood smear or autopsy. According to postmortem retrospective studies in human medicine, 30–50% of hematologic malignancies including acute leukemia were diagnosed postmortem or shortly before death, which was attributed to rapid onset and the variety of clinical manifestations of the diseases.9,18
Supplemental Material
sj-pdf-1-vdi-10.1177_10406387241268322 – Supplemental material for Acute myeloid leukemia-M1 in a horse with neurologic signs and necrotizing enterocolitis
Supplemental material, sj-pdf-1-vdi-10.1177_10406387241268322 for Acute myeloid leukemia-M1 in a horse with neurologic signs and necrotizing enterocolitis by Jeongha Lee, Sydney Mordoh, Mustajab Mirza, Mariano Carossino and Fabio Del Piero in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We kindly acknowledge the Histology and Immunohistochemistry section at the Louisiana Animal Disease Diagnostic Laboratory and Drs. Naomi Falconnier and Bianca de Cecco for taking gross pictures of the brain of the horse.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Louisiana Animal Disease Diagnostic Laboratory, Louisiana State University School of Veterinary Medicine (PG009095).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.