
Abstract
Acute leukemia is rare in horses. Herein we describe historical, clinicopathologic, and postmortem findings in 6 horses with acute leukemia. Medical records of horses with >20% bone marrow blasts and cytochemical or immunophenotyping results were reviewed. Affected horses were 2–8 y of age and of different breeds and sex. Horses were presented acutely with nonspecific signs (e.g., fever, lethargy). Characteristic hemogram findings were bi- or pancytopenia with low blast numbers. Histologic examination revealed extramedullary infiltrates, especially in lymph nodes, spleen, kidney, liver, and lungs. Leukemias were classified as B-cell (n = 3) and acute myeloid leukemia (AML) (n = 3). Tumors in 4 cases expressed multiple lineage markers, which complicated classification. Acute leukemia should be suspected in horses with moderate-to-severe bi- or pancytopenia. Blood smears should be reviewed for neoplastic cells, and bone marrow examination is required for diagnosis. Leukemia classification is best achieved using combined morphologic, cytochemical, and immunophenotyping results.
Leukemia is a hematopoietic neoplasm that primarily involves the bone marrow or blood. Leukemia is generally classified by the degree of differentiation (acute or immature vs. chronic or mature) and lineage commitment (acute lymphoblastic leukemia [ALL] vs. acute myeloid leukemia [AML]). Both ALL and AML are rare in horses, and have been described as individual cases or small case series. Our objective is to describe historical, clinicopathologic, and postmortem findings in 6 horses diagnosed with acute leukemia at Cornell University (College of Veterinary Medicine, Ithaca, New York) over 22 y. Horses were identified through a medical record search for a diagnosis of acute leukemia, based on the presence of >20% bone marrow blasts. 9
All horses were young (2–8 y of age) and of different breeds with an equal mix of sexes. Historical clinical signs were acute (2 d to 2 mo) and included intermittent or persistent fevers (n = 6) unresponsive to antibiotic and anti-inflammatory therapy (n = 2), lethargy (n = 3), and, in single horses, inappetence, weakness, ataxia, and distal limb edema. Physical examination at initial presentation revealed fever (n = 5), tachypnea (n = 3), tachycardia (n = 3), peripheral or mandibular lymphadenopathy (n = 3), and, in single horses, ventral and limb edema, pallor, muscle wasting, and multiple joint effusions (Table 1).
Signalment, historical clinical signs, and initial physical examination findings in 6 horses with acute leukemia.*
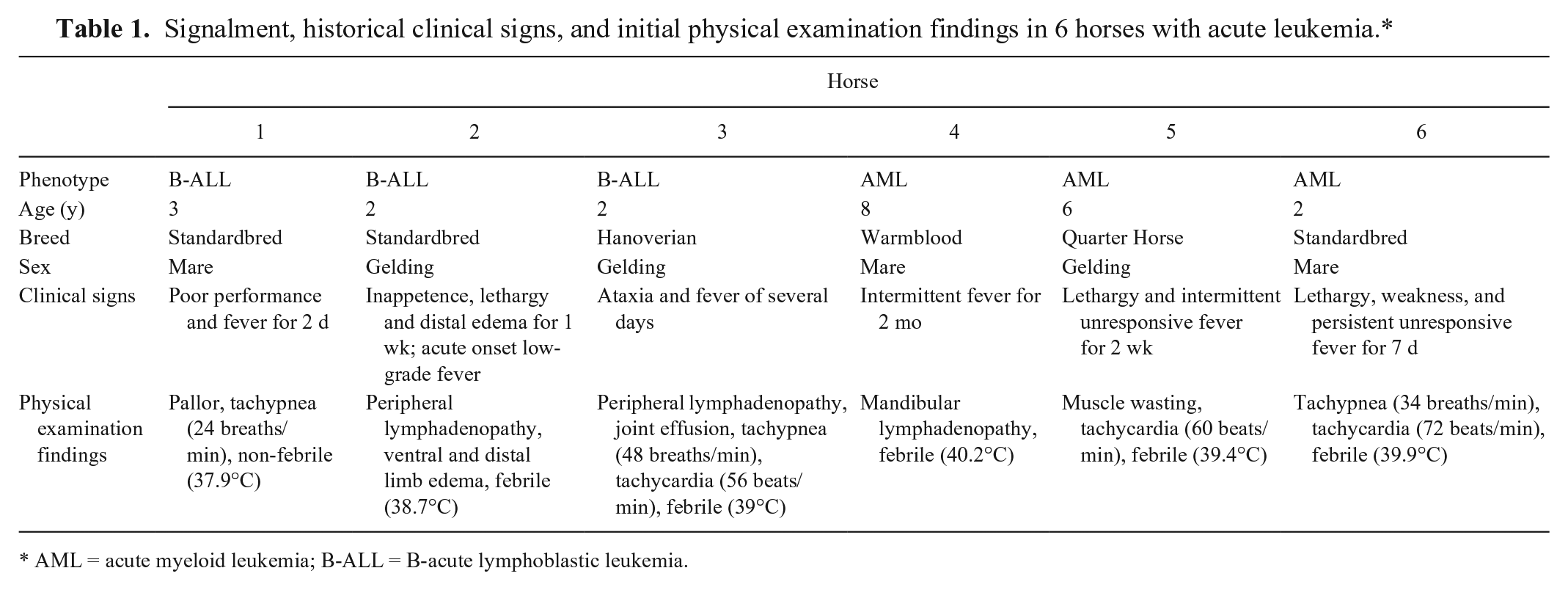
AML = acute myeloid leukemia; B-ALL = B-acute lymphoblastic leukemia.
Hemograms in 4 horses revealed moderate-to-severe anemia, which was mostly normocytic normochromic (Table 2). Case 5 had macrocytosis without anemia; many macrocytes and several nucleated erythrocytes (Fig. 1A), some of which were dysplastic (blebbing, peanut-shaped nuclei, binucleation, larger than normal), were observed in a blood smear (Fig 1B). All horses were severely neutropenic with mildly increased numbers of band neutrophils (left shift) and mild-to-moderate toxic change in neutrophils (cytoplasmic basophilia, Döhle bodies) in 2 and 4 horses, respectively. The left shift to band neutrophils and toxic change indicated a concurrent inflammatory leukogram in these horses. All horses had mild-to-severe thrombocytopenia. Circulating tumor cells were identified in all horses and were large (15–25 μm) mononuclear cells that contained round-to-oval nuclei with finely dispersed to clumped chromatin and 0–1 nucleoli in small-to-moderate amounts of light-blue cytoplasm (blasts). Many tumor cells in case 5 had pleomorphic nuclei (Fig. 1C). Biochemical findings included mild hypomagnesemia (0.55 mmol/L, reference interval [RI]: 0.65–1.15 mmol/L; 3 of 4), hypoalbuminemia (19–29 g/L, RI: 30–37 g/L; 4 of 6), hyperglobulinemia (50–60 g/L, RI: 24–44 g/L; 2 of 6) as a result of polyclonal gammopathy (based on electrophoresis), mild hyperglycemia (6.8–7.7 mmol/L, RI: 3.5–6.2 mmol/L; 2 of 6), and mildly increased γ-glutamyl transferase activity (34–35 U/L, RI: 8–25 U/L; 3 of 6). Bone marrow aspirates revealed >70% blasts in all horses (Fig. 1D), with tumor cells largely comprised (70–80%) of monocytoid cells, with 20–30% typical blasts (round-to-oval nuclei), in case 5 (Fig. 1E). Residual hematopoietic cells were reduced in all cases, and dysplasia was evident in erythroid progenitors in cases 5 and 6 (Fig. 1F). Cytologic examination of mandibular lymph node aspirates revealed a suspected tumor infiltrate in cases 4 and 5. Tumor cells were seen in joint and abdominal fluids in case 3. The final diagnosis was acute leukemia in all cases.
Hematologic data from 6 horses diagnosed with acute leukemia between 1990 and 2012.*
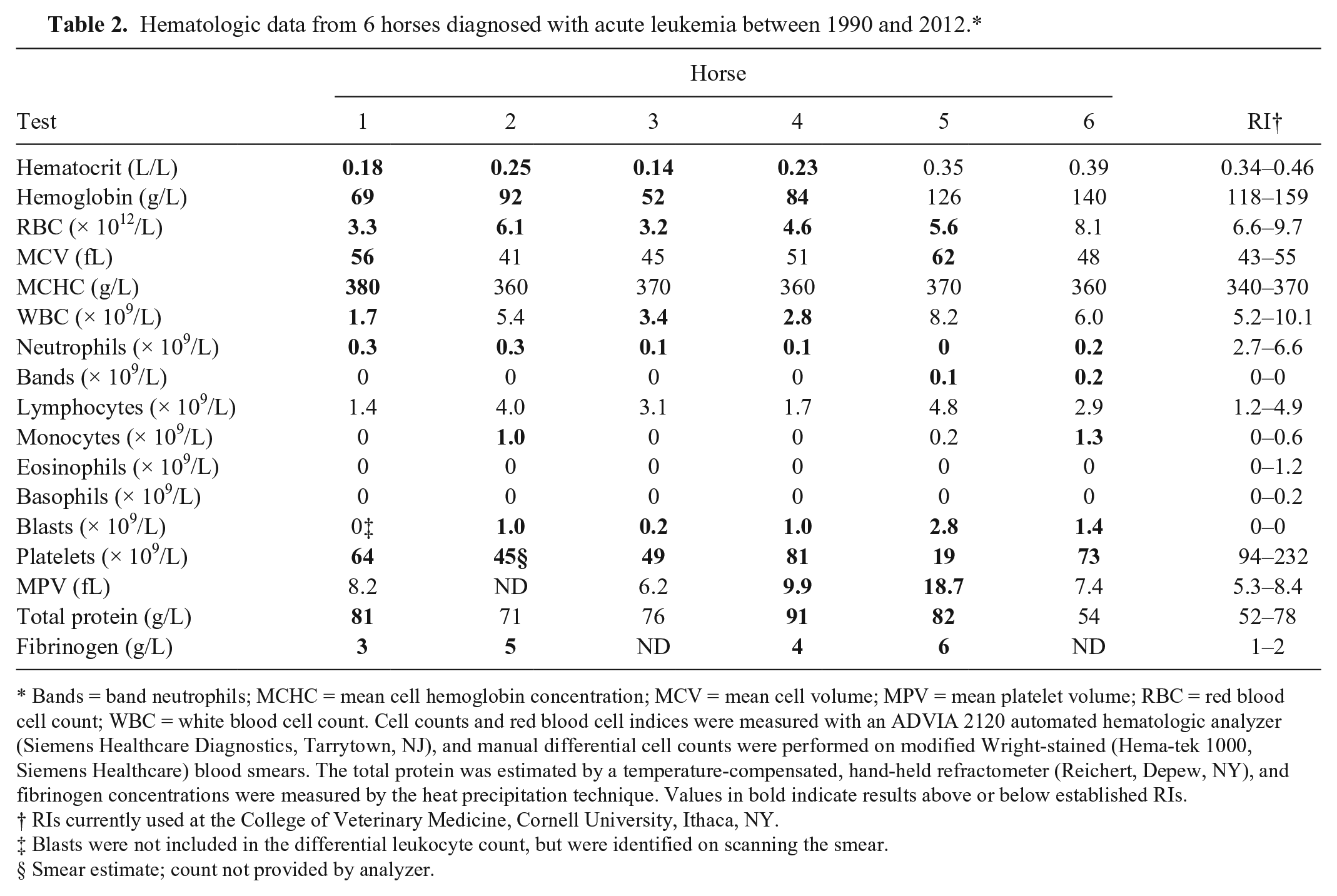
Bands = band neutrophils; MCHC = mean cell hemoglobin concentration; MCV = mean cell volume; MPV = mean platelet volume; RBC = red blood cell count; WBC = white blood cell count. Cell counts and red blood cell indices were measured with an ADVIA 2120 automated hematologic analyzer (Siemens Healthcare Diagnostics, Tarrytown, NJ), and manual differential cell counts were performed on modified Wright-stained (Hema-tek 1000, Siemens Healthcare) blood smears. The total protein was estimated by a temperature-compensated, hand-held refractometer (Reichert, Depew, NY), and fibrinogen concentrations were measured by the heat precipitation technique. Values in bold indicate results above or below established RIs.
RIs currently used at the College of Veterinary Medicine, Cornell University, Ithaca, NY.
Blasts were not included in the differential leukocyte count, but were identified on scanning the smear.
Smear estimate; count not provided by analyzer.
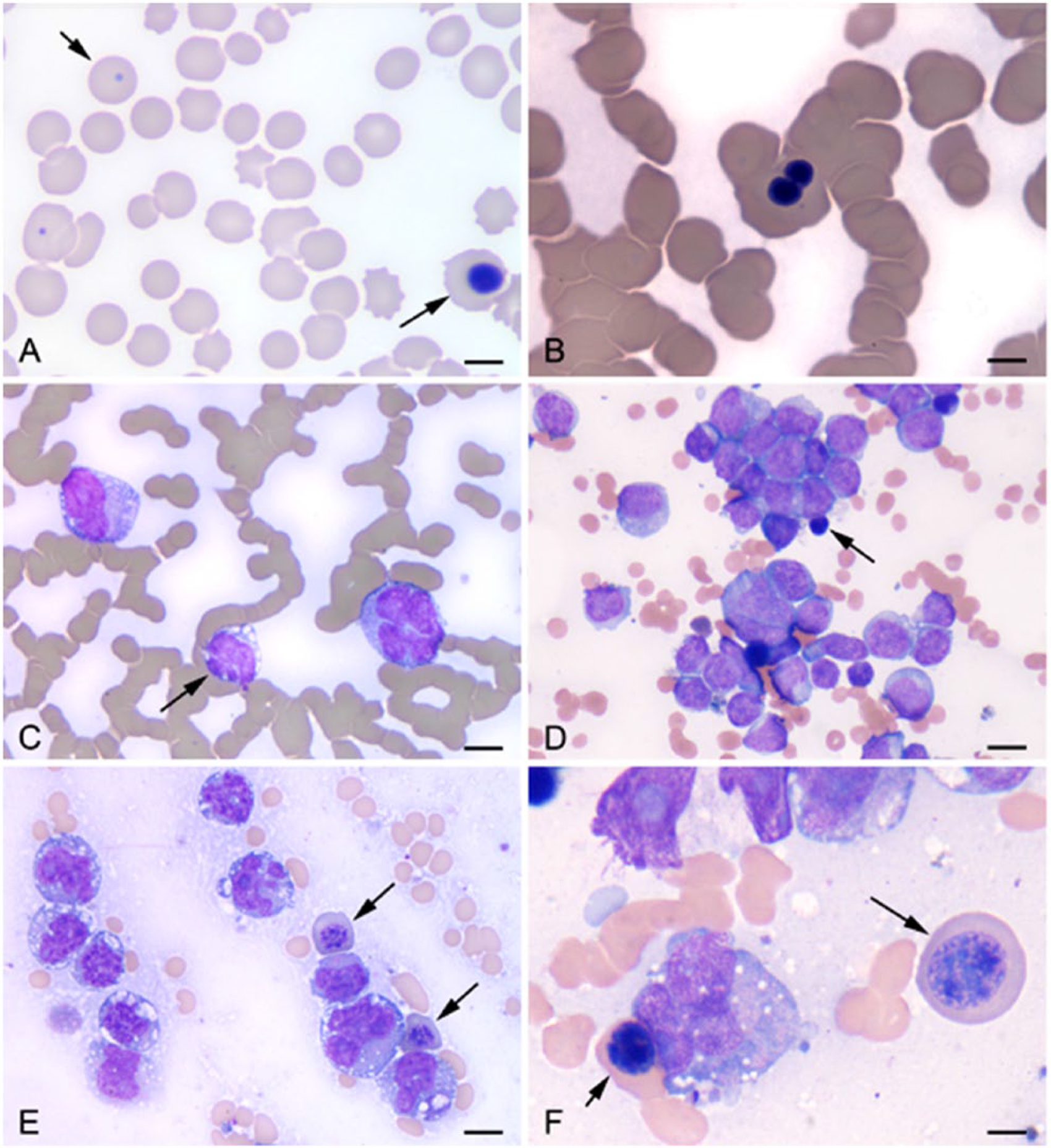
Representative photomicrographs of venous blood and bone marrow from horses with acute leukemia (modified Wright stain).
Cytochemical staining and flow cytometric–based immunophenotyping was performed on bone marrow aspirates (Table 3). Based on negative cytochemical reactions and positive labeling for T-cell markers, a diagnosis of T-ALL was made in cases 1 and 2 and undetermined ALL in case 3. Based on positive cytochemical reactions or myeloid antigen expression with flow cytometry, a diagnosis of AML was made in cases 4–6.
Phenotyping results from immunohistochemical staining of paraffin-embedded, formalin-fixed tissue or flow cytometric analysis of bone marrow and cytochemical staining results from bone marrow aspirate smears with associated final leukemia classification in 6 horses with acute leukemia.*
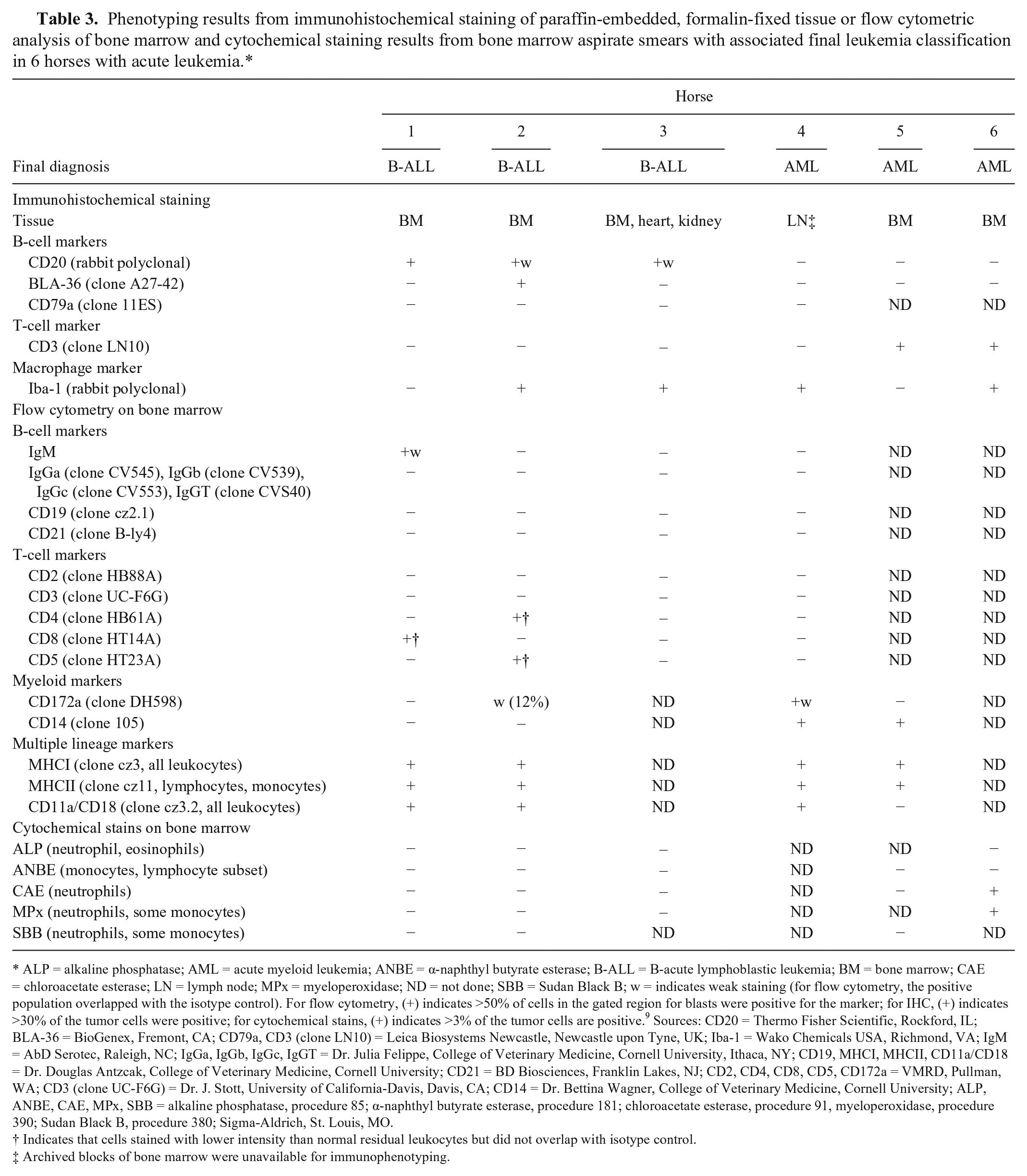
ALP = alkaline phosphatase; AML = acute myeloid leukemia; ANBE = α-naphthyl butyrate esterase; B-ALL = B-acute lymphoblastic leukemia; BM = bone marrow; CAE = chloroacetate esterase; LN = lymph node; MPx = myeloperoxidase; ND = not done; SBB = Sudan Black B; w = indicates weak staining (for flow cytometry, the positive population overlapped with the isotype control). For flow cytometry, (+) indicates >50% of cells in the gated region for blasts were positive for the marker; for IHC, (+) indicates >30% of the tumor cells were positive; for cytochemical stains, (+) indicates >3% of the tumor cells are positive. 9 Sources: CD20 = Thermo Fisher Scientific, Rockford, IL; BLA-36 = BioGenex, Fremont, CA; CD79a, CD3 (clone LN10) = Leica Biosystems Newcastle, Newcastle upon Tyne, UK; Iba-1 = Wako Chemicals USA, Richmond, VA; IgM = AbD Serotec, Raleigh, NC; IgGa, IgGb, IgGc, IgGT = Dr. Julia Felippe, College of Veterinary Medicine, Cornell University, Ithaca, NY; CD19, MHCI, MHCII, CD11a/CD18 = Dr. Douglas Antzcak, College of Veterinary Medicine, Cornell University; CD21 = BD Biosciences, Franklin Lakes, NJ; CD2, CD4, CD8, CD5, CD172a = VMRD, Pullman, WA; CD3 (clone UC-F6G) = Dr. J. Stott, University of California-Davis, Davis, CA; CD14 = Dr. Bettina Wagner, College of Veterinary Medicine, Cornell University; ALP, ANBE, CAE, MPx, SBB = alkaline phosphatase, procedure 85; α-naphthyl butyrate esterase, procedure 181; chloroacetate esterase, procedure 91, myeloperoxidase, procedure 390; Sudan Black B, procedure 380; Sigma-Aldrich, St. Louis, MO.
Indicates that cells stained with lower intensity than normal residual leukocytes but did not overlap with isotype control.
Archived blocks of bone marrow were unavailable for immunophenotyping.
Four horses (cases 1, 2, 4, 5) were euthanized after diagnosis. Case 3 was treated supportively with antibiotics and anti-inflammatory drugs, but developed pitting edema and was euthanized after 14 d. Case 6 was treated with vincristine (0.005 mg/kg bodyweight intravenously once), cytarabine (1.7 mg/kg body weight [bw], constant rate infusion over 24 h), and prednisone (2.2 mg/kg bw orally every 24 h). Serial hemograms showed minimal response, the horse developed neurologic signs, and was euthanized after 3 d. Blasts were identified in atlanto-occipital cerebrospinal fluid collected immediately postmortem.
Postmortem examinations were performed on all horses. Gross examination revealed mild-to-moderate (n = 4) or marked (case 3) single or multiple peripheral and internal lymphadenopathy, subcutaneous or limb edema (n = 2), colonic petechiae (case 5), necrotizing enteritis (case 6), and multifocal-to-coalescing small nodules in the skin, renal cortex, lung, and heart (case 3). Histologic examination of postmortem tissue showed extensive bone marrow involvement in all cases, with mild-to-moderate extramedullary infiltrates in lymph nodes (n = 6), kidney (n = 5), spleen (n = 5), liver (n = 3), lungs (n = 3), brain or spinal cord (n = 2), mediastinal tissue (presumed lymph node), skin and heart (case 3), and intestine and mesentery (presumed lymph node, case 5). In the marrow of case 6, tumor cells displayed myeloid differentiation, and erythroid cells were dysplastic (Fig. 2A). Tumor cells infiltrated the lymph node paracortex predominantly, but were also found in subcapsular and medullary sinuses. Nodal architecture was effaced in all or some nodes in cases 3 and 6, respectively, whereas retention of residual follicles was seen in the other cases (Fig. 2B). Tumor cells diffusely infiltrated splenic red pulp or were multifocal surrounding the white pulp. Moderate infiltrates were found periportally and within hepatic sinusoids. Case 6 also had multifocal centrilobular infiltrates and necrosis (Fig. 2C). Tumor cells were located multifocally perivascularly and interstitially in the renal cortex (mostly) and medulla. Lung infiltrates were around bronchioles or vessels or within alveoli. Tumor cells multifocally infiltrated stomach and large intestinal submucosa in case 5 (Fig. 2D). Case 3 had moderate superficial and deep dermal infiltrates with no epitheliotropism, and multifocal interstitial endocardial, pericardial, and perivascular subpleural infiltrates. Tumor cells distended vessels or were perivascular in the brain (choroid plexus, cerebrum) and spinal cord in cases 3 and 6.
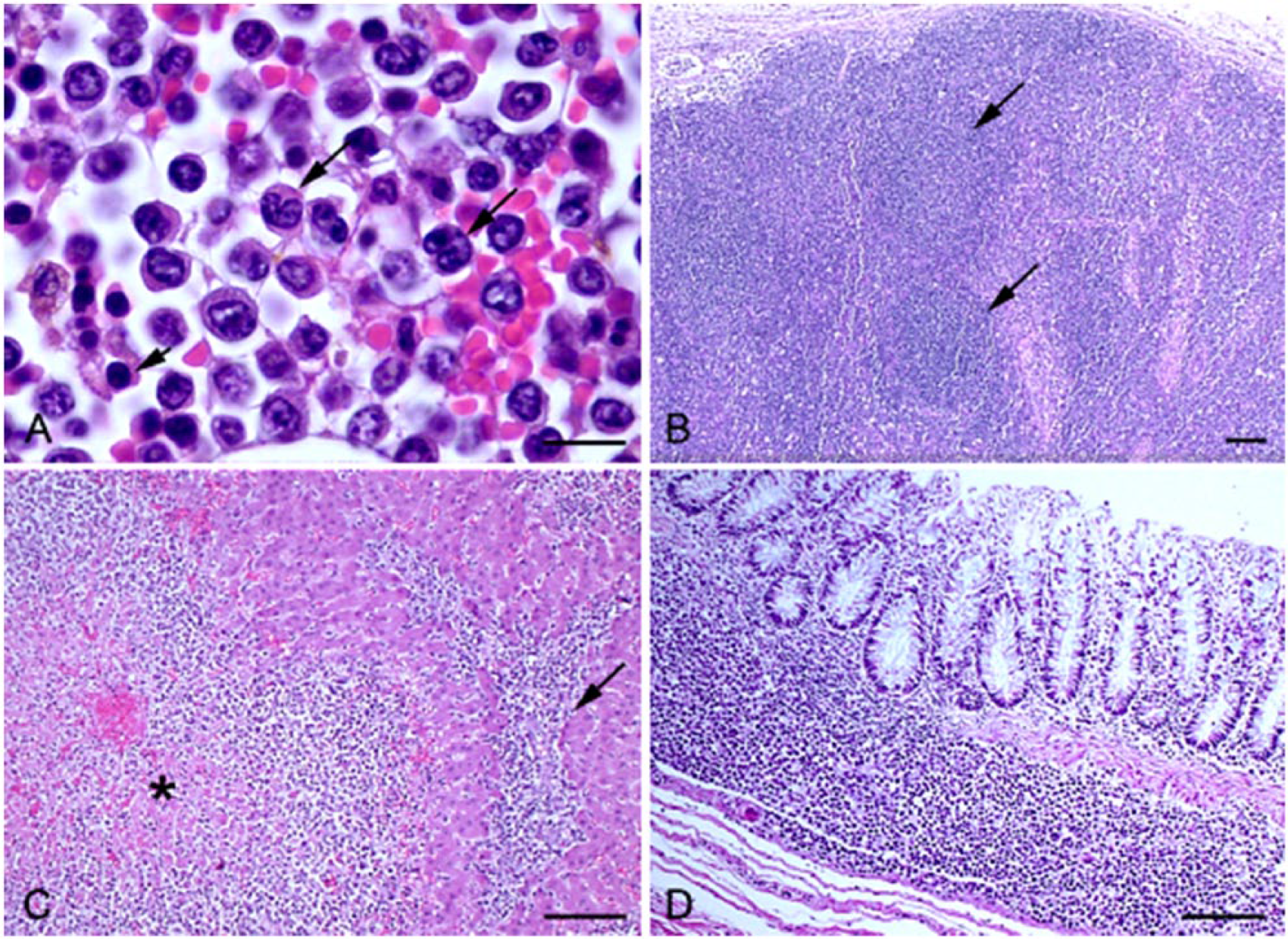
Representative photomicrographs of paraffin-embedded, formalin-fixed tissue sections from horses with acute leukemia. H&E.
Immunohistochemical staining was performed on formalin-fixed tissue sections (Table 3). Based on all of the phenotyping results, the initial diagnosis of T-ALL was revised to B-ALL in cases 1 (which expressed more B than T markers, including CD20; Fig. 3A) and 2 (which expressed 2 B- and 2 T-cell markers; however, CD5 is expressed in a B-cell subset 1 ). Case 3 was modified to B-ALL based on weak CD20 expression. The diagnosis of AML was unchanged, but 2 cases expressed cytoplasmic CD3 (Fig. 3B). We also evaluated Iba-1 expression in normal lymph node and tumor cells. Iba-1, a histiocytic marker, 10 was expressed in macrophages or dendritic cells in normal lymph node (Supplemental Fig. 1) and in tumor cells of 4 cases (Fig. 3C, D; Table 3).
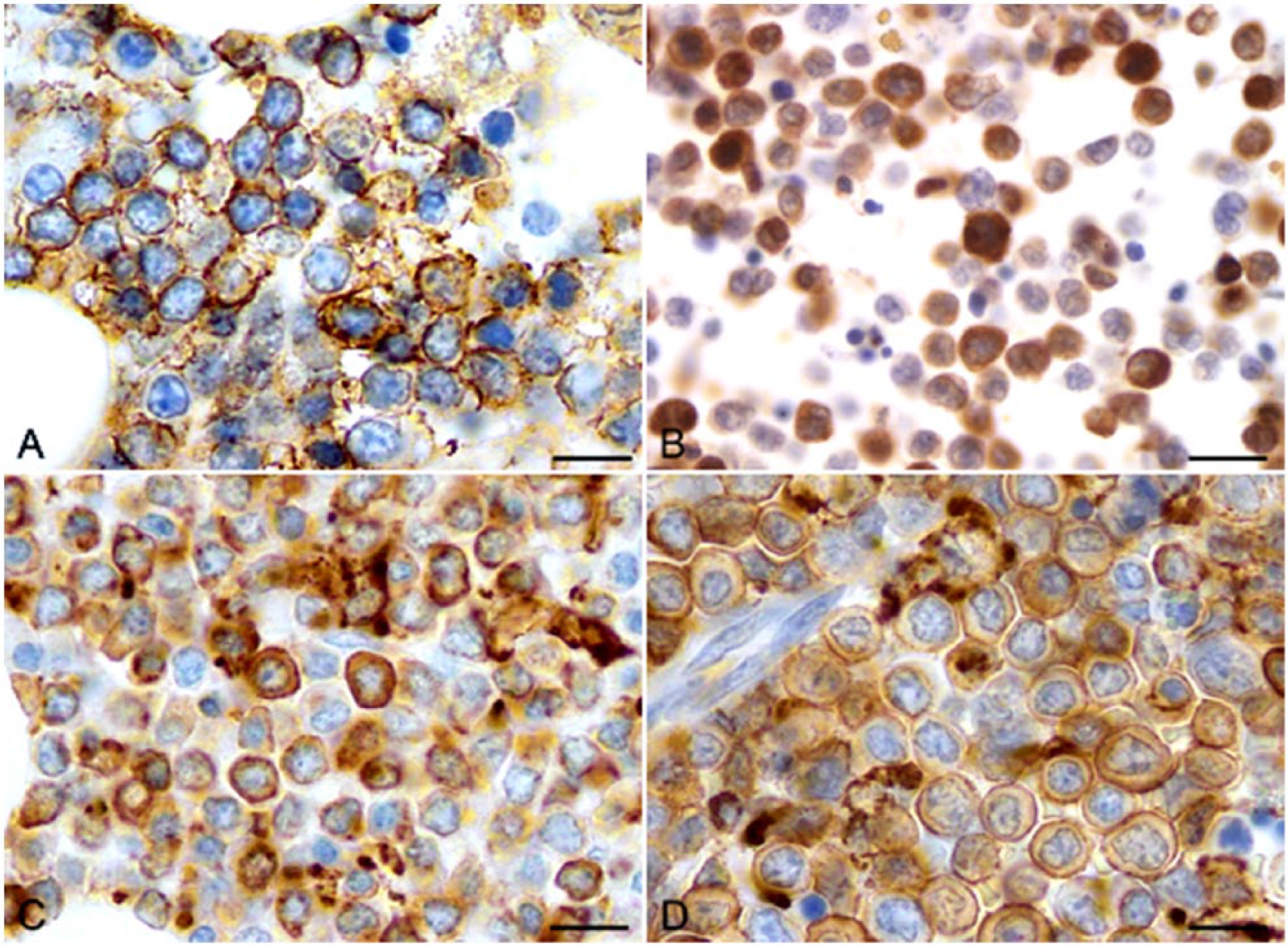
Representative photomicrographs of immunohistochemical staining of paraffin-embedded, formalin-fixed bone marrow sections from horses with acute leukemia.
Hematopoietic neoplasia is uncommon in horses, with lymphoma the most commonly described form.3,6 In contrast, only 1% (2 cases) of 203 lymphoid tumors in a retrospective study were classified as ALL. 3 Such findings are similar to our experience, with only 6 cases of acute leukemia diagnosed over 22 y.
All horses in this case series were young adults with no breed predilection. Clinical signs were acute in onset and nonspecific, but all horses were febrile, either historically or on initial physical examination. Hemogram results were pivotal, and led to a presumptive diagnosis of acute leukemia in all cases. Horses were neutropenic and thrombocytopenic; 2 horses were pancytopenic. Several horses had hematologic evidence of concurrent inflammation. Cytopenias were generally moderate-to-severe and anemias were nonregenerative, with macrocytosis in case 5 attributed to abnormal erythropoiesis versus a regenerative response to the anemia (based on the erythroid dysplasia evident in blood and marrow). Low numbers of neoplastic cells were identified in all blood smears and led to a presumptive diagnosis of acute leukemia, which underscores the need for careful evaluation of smears when severe or multiple cytopenias are detected in horses. Circulating tumor cells are not diagnostic for acute leukemia, because they may be observed in lymphoma, and were documented in 14 of 37 horses with lymphoma in a previous study. 6 However, multiple or severe cytopenias are unusual for lymphoma, and such cytopenias should raise the possibility of acute leukemia, which warrants bone marrow aspiration for confirmation. Biochemical results were unremarkable, and indicated inflammation, stress, and in some cases possible liver involvement. Tumor cells infiltrated extramedullary tissues, which largely followed a vascular pattern. Of note, nodal involvement was extensive, with effacement of architecture, which mimicked lymphoma. However, careful examination revealed residual follicles in 5 horses, which supports an infiltrative process. It is possible that case 3 had lymphoma versus B-ALL, given that the horse had skin nodules and marked lymphadenopathy, with effacement of nodal architecture, findings more typical of lymphoma. Lymphoma can infiltrate bone marrow; marrow myelophthisis was noted in 5 of 12 horses with circulating tumor cells in a previous study of horses diagnosed with lymphoma. 6 However, it is possible that the latter horses had acute leukemia and not lymphoma. These cases highlight the difficulty in histologically differentiating acute leukemia from lymphoma. Indeed, the World Health Organization categorizes ALL and lymphomas as a group of precursor lymphoid neoplasms, distinguished primarily by the main site of tumor involvement. 9
We used cytochemical staining and immunophenotyping to classify the leukemias. Positive cytochemical results or myeloid antigen expression supports an AML classification. Conversely, negative cytochemical results or lymphoid antigen expression supports a diagnosis of ALL.2,4,5 Based on cytochemical and flow cytometric results, 3 horses in our study were initially diagnosed with AML and 3 with ALL, 2 of T-cell origin (expression of CD8 in 1 horse, and CD5 and CD4 in another). However, tumor cells in the latter 2 horses lacked CD3 and expressed B-cell antigens on immunohistochemical staining of postmortem tissue, thus their leukemia classification was amended to B-ALL (based on the majority of marker expression). We also found lineage infidelity in 2 AML cases, which aberrantly expressed CD3 (the negative cytochemical reactions in tumor cells of case 5 was attributed to enzyme deactivation with storage, given that staining was done after 1 y). These results indicate that tumor cells in acute leukemia can aberrantly express antigens as reported for humans 8 and dogs, 7 which makes accurate classification difficult. Our results raise the possibility that tumors diagnosed as lymphoma on single antigen expression3,6 could be AML. Likewise, it is conceivable that some leukemias were misclassified in our study and that some cases with expression of markers of more than 1 lineage could be mixed-phenotype acute leukemia (e.g., B-ALL/AML). Our results illustrate the importance of using all available tools and multiple markers for phenotyping, with the ultimate diagnosis based on the majority of expressed markers, not solitary results.
Iba-1 is used to identify histiocytes, particularly in the brain, 10 but we reasoned it may be a marker of AML, particularly monocytic variants. Tumor cells in 2 AML horses expressed Iba-1, as did cells in 2 B-ALL. Thus, we did not use Iba-1 to classify the leukemia. Because there have been no reports of Iba-1 expression in acute leukemia, to our knowledge, Iba-1 testing may be worthwhile in horses with lymphoma and in other species with hematopoietic neoplasia.
Footnotes
Acknowledgements
We thank Alan Weldon, Simon Peek, Theresa Ollivett, Kathleen Mullen, and Toby Pinn for their case contributions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.