
Abstract
A 12-y-old Shetland Pony was presented with a mucus-secreting fistula in the right paralumbar fossa. Surgery was performed to unravel the origin of the fistula. The horse died under anesthesia and was forwarded to autopsy. The right kidney was markedly atrophic and fibrotic, consistent with unilateral end-stage kidney. The right ureter was markedly thickened, but with luminal continuity leading into the urinary bladder where a partial obstruction caused by nodular para-ureteral fat necrosis was evident. The lumen of the cutaneous fistula was continuous with the right ureter; therefore, we diagnosed the lesion as a ureterocutaneous fistula. Anomalies of the ureter are uncommon, and ureterocutaneous fistula formation in equids has not been reported previously to our knowledge.
A 12-y-old Shetland pony mare was presented to the Department for Horses (Faculty of Veterinary Medicine, Leipzig University, Germany) for the treatment of a fistula in the right flank secreting gray clear viscous mucus, which had been encountered starting ~6 mo before referral. Attempts to flush the fistula had not led to the resolution of secretion, and anatomic localization and direction of the fistula were the reasons to refer the case for surgery.
Clinical examination upon referral revealed a fistula in the center of the right paralumbar fossa. Physical parameters and routine blood analysis were within physiologic norms. Ultrasonography and probing revealed a tract at least 10-cm deep directed axially in a horizontal plane; however, the origin of the fistula could not be defined. Surgery was performed under general anesthesia in left lateral recumbency to excise the fistula. Preparation of the fistula canal revealed that the cutaneous fistula was connected with the thickened right ureter. The right kidney had an untypical, uneven surface, was firm and fibrotic, and appeared atrophic. Distally along the ureter towards the bladder, the thickened ureter entered a ball-like, firm, fibrotic lesion, which was directly attached to the bladder wall. To remove the fistula, the tract was transected at the T-junction with the ureter, and an outflow of gray clear viscous mucus was observed; such mucus is typically seen in the renal pelvis of horses. We assumed that the firm lesions adjacent to the bladder might have led to ureteral obstruction triggering the fistula formation. Therefore, the conversion from fistula surgery to nephrectomy was decided to prevent further production of mucus, and the atrophic right kidney was excised.
Upon completion of nephrectomy the mare suddenly developed cardiac arrest, died despite attempts at resuscitation, and was referred to the Institute for Veterinary Pathology (Leipzig University) for autopsy. The excised fistula tract, kidney, and ureter specimens were immediately fixed in 4% formaldehyde for histologic examination.
An autopsy was performed with special emphasis on the urogenital tract. After opening the abdominal cavity, the left kidney measured 13.5 × 11.2 × 6.3 cm. The left ureter was 0.7 cm in diameter and within normal limits (ureteral diameter of mid-sized horse = 0.6–0.8 cm). 9 Histologic examination of the left kidney revealed no pathologic alterations.
Alterations of the urogenital tract consisted of a markedly thickened right ureter (2.1 cm diameter) and an 11.2 × 5.4 × 5.2-cm para-ureteral mass near the ureteral junction with the urinary bladder (Fig. 1A). The surgically removed right ureter had a sutured edge, and a fistula remnant was identified (Fig. 1B). The complete urogenital tract was fixed in Klotz solution containing 0.42% formaldehyde to stop autolysis and to enable postmortem radiographic analysis before trimming tissue samples. First, a radiographic image was taken prior to contrast agent application (Imeron 300 M; Bracco). By this approach, we confirmed radiodense accumulations in the para-ureteral mass indicating mineralization within the lesion that severely obstructed the ureteral lumen (Fig. 1C). Next, contrast agent was applied with a syringe into the ureteral lumen at the site of surgery. A continuous ureteral lumen was seen, resulting in accumulation of contrast material in the urinary bladder (Fig. 1D), suggesting that a minimal luminal connection to the urinary bladder was maintained.
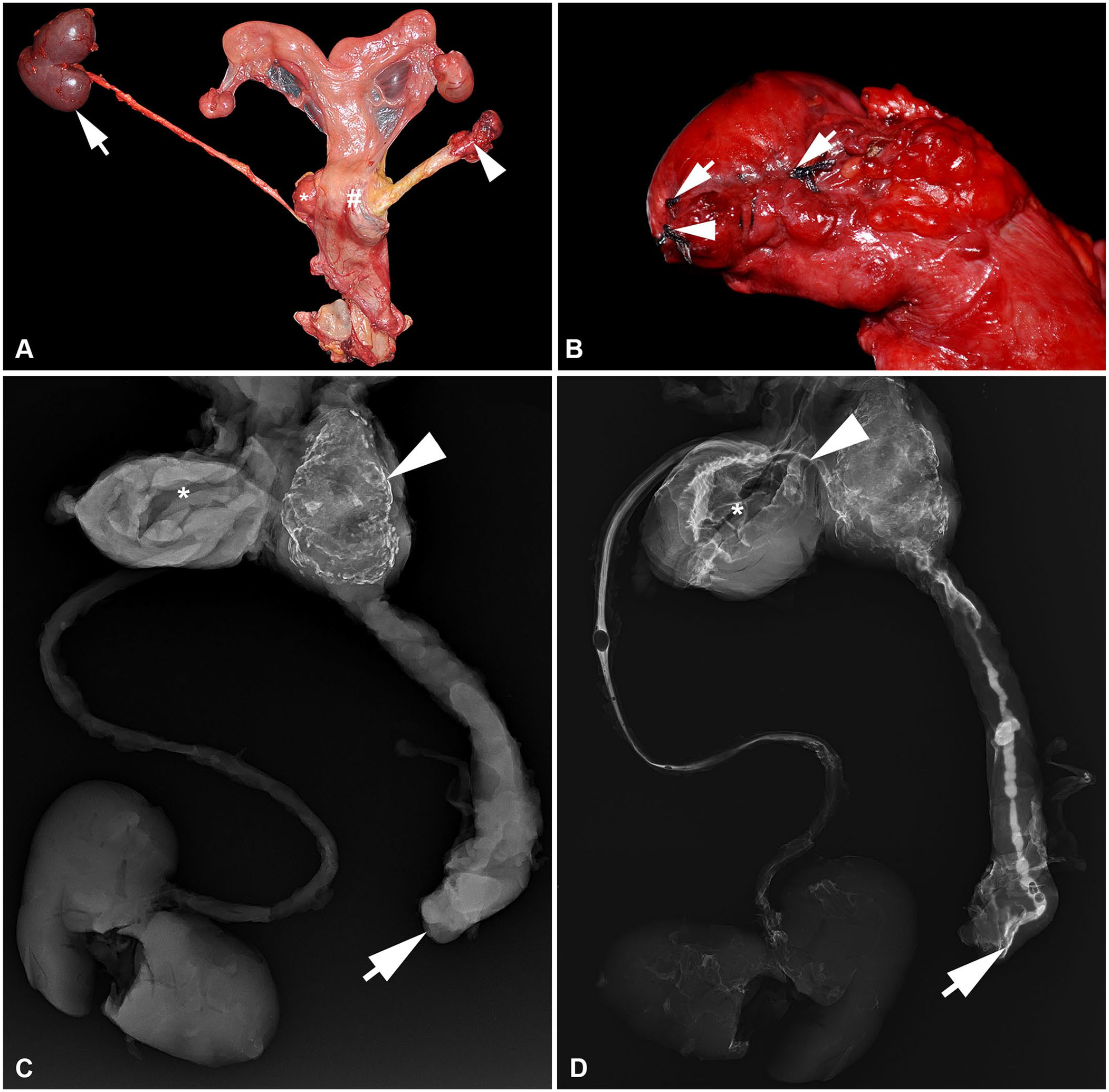
Thickened right ureter and para-ureteral mass with postmortem radiographic findings in a female Shetland pony.
The right ureter was subsequently bread-loafed for assessment of continuity and luminal diameter. The lumen was variably dilated (0.4–1.4 cm diameter) and filled with opaque mucus (Fig. 2A). Histologic examination of the right ureter revealed variable fibrosis of the mucosal lamina propria and tunica adventitia (Fig. 2B), as well as mild-to-moderate lymphohistioplasmacytic ureteritis (Fig. 2C). The para-ureteral mass consisted predominantly of necrosis with extensive mineralization surrounded by a dense fibrous connective tissue capsule that enclosed the distal part of the right ureter (Fig. 2D).
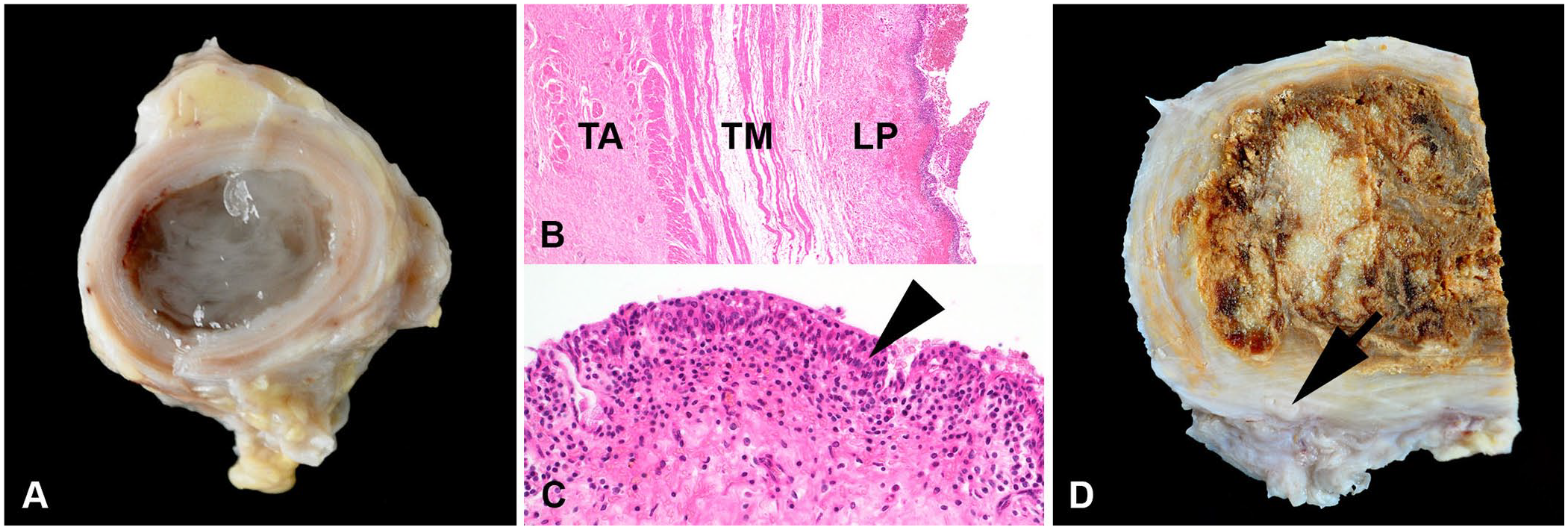
Mucus-filled, thickened right ureter and para-ureteral mass of fat necrosis in a Shetland Pony.
The 11.5 × 7.0 × 3.5-cm right kidney was markedly atrophic and fibrotic and consisted of a markedly thickened capsule, a non-identifiable corticomedullary junction, and the proximal part of the right ureter was identified (Fig. 3A). The fistula remnant was equally inflamed and lined by an attenuated-to-flattened (pressure atrophy) epithelium. Severe glomerular and tubular atrophy with interstitial as well as intimal and medial fibrosis of numerous blood vessels was evident (Fig. 3B). Furthermore, lymphohistioplasmacytic- (Fig. 3B, inset) to-granulomatous pyelonephritis with a few dilated and amorphous protein-rich secretion–filled tubules (thyroidization) were seen (Fig. 3C, 3D). In the cortical region, atrophic, sclerotic, and hyalinized glomeruli were evident (Suppl. Fig. 1).
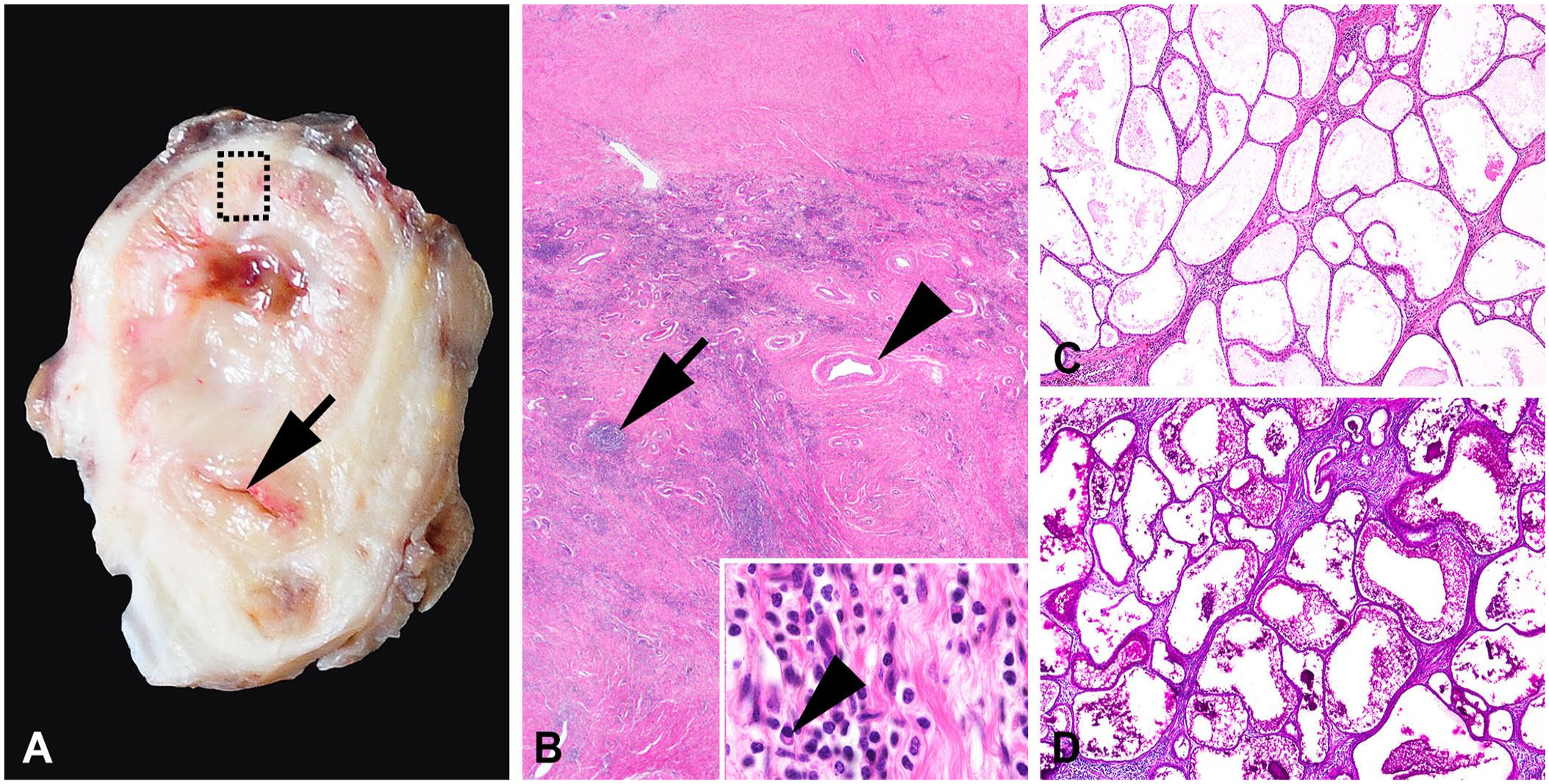
Pyelonephritic end-stage kidney in a Shetland pony.
Fistula formation in the urogenital tract is occasionally seen post-surgery and started as early as 12 d after iatrogenic injury of the urethra in a porcine experimental model of urethrocutaneous fistula formation. 2 Aside from experimental settings, ureterocutaneous fistulae have been reported rarely in human medicine as surgery-associated lesions 7 ; one case report describes a similar entity in a dog that developed a fistula 3.5 y after ureteral stenting. 6 In addition to surgery-associated lesions of the ureter, trauma during dystocia and urolithiasis can cause para-ureteral pseudocysts (urinomas) as a result of urine leaking into the peritoneum and inciting severe fibroblastic inflammation.5,8 We cannot rule out that the para-ureteral fat necrosis that we noted near the urinary bladder orifice of the right ureter was initially a urinoma.
Leaking urine into the ureteral tunica adventitia may have further acted as a chemical irritant inciting severe fibrosis along the entire length of the right ureter. We found no evidence of an ongoing infectious or neoplastic process nor urolithiasis that could have been causative for the para-ureteral fat necrosis, nor was a preexisting gynecologic condition or gynecologic treatment or surgery recorded in the mare’s clinical history. We retrieved no cases of a ureterocutaneous fistula in horses in a search of Google, PubMed, CAB Direct, Web of Science, and Scopus, suggesting that no descriptions of this condition have been reported in equids.
We further assume that the para-ureteral fat necrosis had caused obstruction of the ureteral lumen, as indicated in the postmortem radiograph. Furthermore, the obstruction could have caused hydroureter, which would explain the prominent luminal dilation we observed and could have led to pyelonephritis (PN). As inflammation progressed, macrophages and lymphocytes replaced the initial neutrophils, and marked fibrosis indicates the progression to chronic PN. The obstruction of the right ureter is the most plausible cause, given that chronic PN frequently develops further to predisposing factors that impede the outflow of urine.1,3 In our case, fibrosis was marked and the kidney was severely atrophic compared to the left kidney. In particular, the microscopic evidence of numerous blood vessels with intimal and medial fibrosis, the thyroidization of remaining tubules, 1 as well as atrophic hyalinized glomeruli, are all features of chronic PN.1,3 However, identification of the initial step in this progressive renal disease is virtually impossible. Therefore, albeit less likely, primary renal disease by the hematogenous route must be considered; glomerulonephritis would occur bilaterally, and can hence be ruled out.
We hypothesize that the fistula formation was temporally not associated with the para-ureteral fat necrosis, given that the fistula did not develop there. It is obvious that the proximal ureter gave rise to fistula formation in conjunction with severe inflammation. Ureteral glands are especially numerous in the proximal ureter and are unique to the equine urinary tract. 4 The glands produce the light-gray opaque mucus observed in the fistula at surgery and in the ureter at autopsy. Prolonged mucus production in combination with spatially adjacent inflammation was the nidus for the subsequent ureterocutaneous fistula formation.
Supplemental Material
sj-pdf-1-vdi-10.1177_10406387231186134 – Supplemental material for Pyelonephritic end-stage kidney and ureterocutaneous fistula in a Shetland pony
Supplemental material, sj-pdf-1-vdi-10.1177_10406387231186134 for Pyelonephritic end-stage kidney and ureterocutaneous fistula in a Shetland pony by Jan Schinköthe, Kerstin Gerlach, Reiner G. Ulrich and Walter Brehm in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank Ralf-Peter Dobroschke, Jessica Frese, Lars Riesche, Elfi Quente, Hilke Gräfe, Peggy Schleinitz, Christiane Pleitz, and Brigitte Uhlemann for excellent technical assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.