
Abstract
We investigated 2 outbreaks of osteomalacia as a result of phosphorus (P) deficiency in herds of lactating beef cows grazing subtropical native pastures in Uruguay. Cows exhibited pica, difficulty to stand and walk, rib fractures, and body weight loss even with adequate forage availability. Osteopenia and severe osteomalacia were observed on gross and histologic examination. The concentrations of bicarbonate-extractable P in soil (4.0, 4.1 mg P/kg), total P in pasture (0.9, 1.1 g P/kg), inorganic P in serum (1.0, 0.71 mmol P/L), and P in bone (73 mg P/mL) were all low. Although injectable and mineral salt supplements provided additional P in both outbreaks, these supplementary amounts were insufficient to prevent P deficiency. The P ingested by the cows from the pasture and supplements would have provided 20–55% of their daily P requirements of ~21 g P/d. Osteomalacia occurred in cattle at the 2 ranches as a result of severe P deficiency in the soil and forage, and inadequate P supplementation. Following diagnosis, control of P deficiency in beef cattle requires estimation of the amount of pasture P ingested and provision of sufficient additional supplementary P to meet the animals’ requirements.
Osteomalacia is a mineral deficiency disease that occurs in many animal species and is associated with failure in bone tissue mineralization. Osteomalacia is usually caused by dietary phosphorus (P) deficiency. 4 The main clinical manifestations of osteomalacia in cattle are pica (eating or licking bones and/or stones), body weight (BW) loss, difficulty in standing and walking, and bone fractures.3,17 However, the main production losses associated with the disease are subclinical as a result of weight loss and reduced fertility of the herds, leading to reduced economic viability of the ranches. 6 Osteomalacia in grazing beef cattle associated with P deficiency occurs on native pastures containing < 1.5–2.0 g P/kg growing on soils containing <4–5 mg P/kg.3,6 Such P deficiencies are most common in low-input tropical native pasture systems, such as in regions of South Africa, 15 Brazil, 18 or Australia. 6 Osteomalacia has long been recognized in Uruguay, usually affecting lactating cows grazing subtropical native pastures 16 that comprise ~11.2 million ha supporting ~5.9 million cows and heifers. These native pastures typically have low P concentrations in soil (2.5–9 mg P/kg) 1 and forages (0.2–4.2 g P/kg). 19
In endemic P-deficient areas, effective supplementation with P and/or P fertilizers can prevent osteomalacia and improve cattle production.2,3,6 However, mineral supplementation is sometimes not effective because of inadequate intake of supplementary P and/or inappropriate timing of supplementation. 14 Nevertheless, despite the evidence of the benefits of P supplementation in Uruguay, 20 osteomalacia outbreaks still occur. We describe here 2 outbreaks of osteomalacia in beef cows on commercial ranches in Uruguay. Both outbreaks occurred on native grassland paddocks dominated by C4 perennial grasses that had never been fertilized with P and thus were associated with inadequate P supplementation.
Outbreak 1 occurred in February 2019 on a ranch in the Department (Province) of Cerro Largo in a herd of 350 lactating primiparous and multiparous Hereford and Aberdeen Angus crossbred cows (3–8 y old) grazing 700 ha of native grassland paddocks. From April 2017 to December 2018, all of the cows had been given a monthly injectable supplement providing 0.7–1.0 g P (Suppl. Table 1). In addition, from September 2018 until February 2019, the herd was offered feed-blocks containing 40–55 g P/kg (Suppl. Table 1) and ingested 0.4–0.6 g P/cow daily. Additionally, from January to February 2019, cows with clinical signs were given 10 mL of injectable P supplements (Suppl. Table 1) every 3–4 d.
Outbreak 2 occurred in January 2020 on a ranch in the Department of Tacuarembó in a herd of 205 lactating multiparous Hereford crossbred cows (5–6 y old) grazing a 470-ha native grassland paddock. In September 2019 and January 2020, cows were given the injectable P supplements described above, and for 45 d from December 2019 to January 2020 were fed a loose mixed mineral supplement containing 36–44 g P/kg (Suppl. Table 1) and ingested 2.3–2.8 g P/cow daily.
Representative samples of soil at a depth of 150 mm and of forage (n = 30 each of soil and forage) were collected. Forage samples obtained by hand-plucking 5 were sorted manually into green and senescent forage fractions. The forage initially available was measured using a comparative yield method. 8 The concentrations of bicarbonate-extractable P (PB) in the soil and the total P concentration in the forage were determined colorimetrically by an ammonium molybdate method 11 using a spectrophotometer.
Blood samples were collected by jugular venipuncture from cows selected randomly at outbreak 1 (12 with and 14 without signs) and outbreak 2 (11 with and 11 without signs). The blood samples were transferred into 5-mL tubes with a clot accelerator and stored for 5–7 d until centrifugation (2,450 × g, at 4°C, 10 min). The concentrations of inorganic P (Pi) and calcium (Ca) in serum were determined colorimetrically by the phosphomolybdate and o-cresolphthalein complexone methods, respectively, using an automatized spectrophotometer (Dimension RxL Max integrated chemistry system; Siemens). Mineralization of the lumbar bones of the cows (outbreak 1: 43 with and 14 without clinical signs; outbreak 2: 11 with and 11 without signs) was evaluated using a needle test. 18 The cows were classified as “deficient” (i.e., with osteopenia) if the apophysis could be easily penetrated by the needle (hypodermic 18 ga), or “adequate” (no osteopenia) if not.
Autopsies were performed on 2 cows from outbreak 1. Several tissue samples were collected, fixed in 10% neutral-buffered formalin, processed routinely, and stained with hematoxylin and eosin (H&E) for histopathology. After fixation, rib and humerus samples were cut into 5-mm slices and demineralized with 12% EDTA (pH 7.0) for 20–30 d, processed routinely, and stained with H&E and the Masson variation of the Goldner trichrome for histopathology. Samples of the 12th left rib bone from each cow were weighed, dried at 100°C, ashed at 700°C, and the ash dissolved in 5N HCl. 10 The concentrations of P and Ca were measured by inductively coupled plasma–emission spectroscopy (MP4200; Agilent) and calculated per unit volume of fresh bone. Bones from a cow grazing in a pasture containing 2 g P/kg and with serum P concentration of 2.3 mmol P/L were used as controls.
Analysis of variance was performed to compare the BW, Pi, and Ca to the presence or absence of signs and to outbreaks. The animal was considered the experimental unit, and data were analyzed using Stata v.14.0 (StataCorp).
In outbreak 1, 59 (43 in February, 16 in March) of 350 cows in the herd had clinical signs, and 5 died. Of the 43 cows, only 22 were classified as “deficient” according to the needle test. In outbreak 2, 11 of 205 cows had clinical signs, and 8 of these 11 were classified as “deficient” according to the needle test. In neither outbreak were any of the cows without clinical signs classified as “deficient” according to the needle test. In both outbreaks, affected cows had one or more of the following signs: pica (Fig. 1A); BW loss; kyphosis; refusal to walk; stiff and unsteady gait with slow, short steps; spent most of the time lying down; and after getting up, rested for 1–3 min on their carpi (Fig. 1B). In outbreak 1, 11 of 43 cows had fractured ribs.
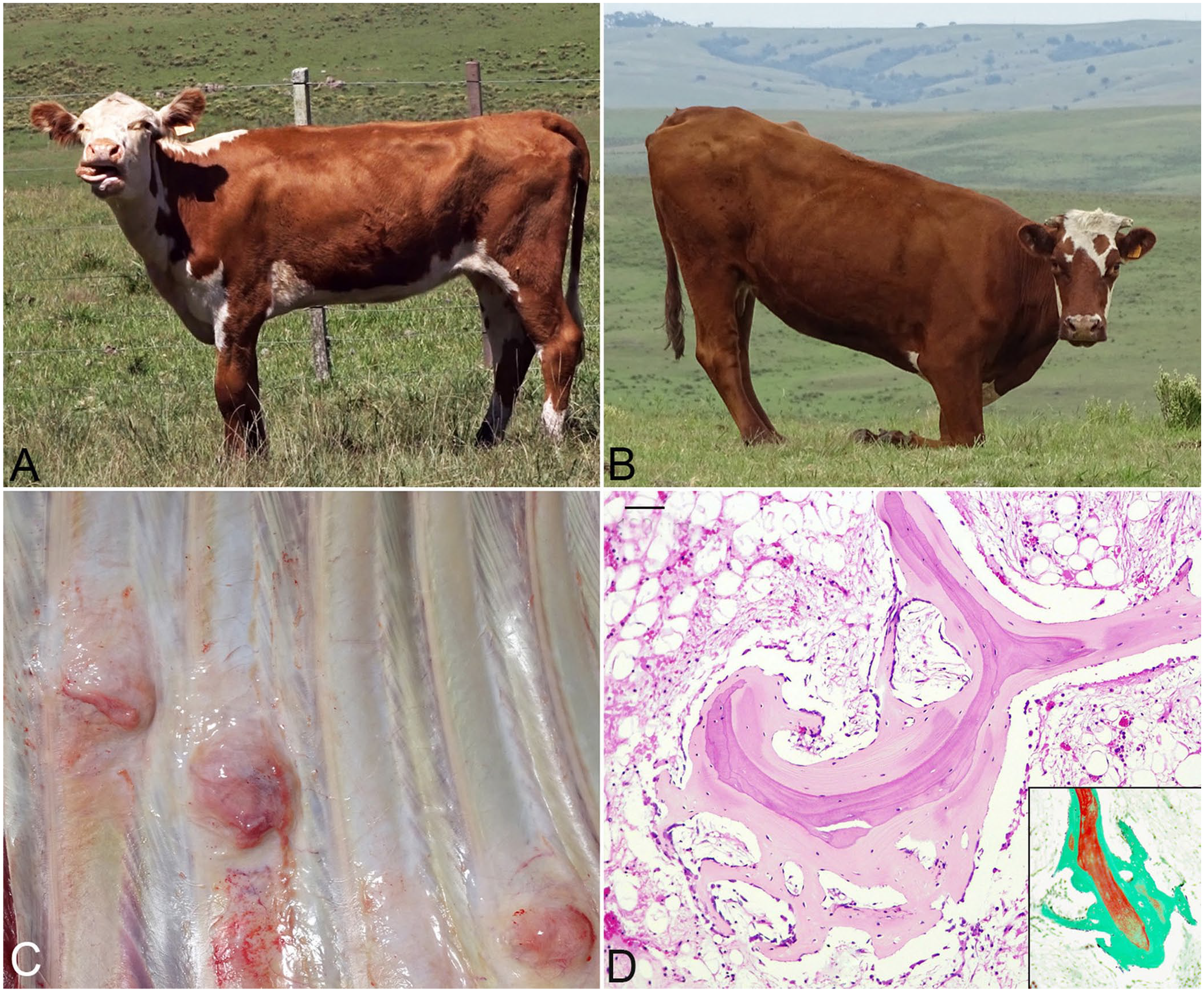
Beef cattle with osteomalacia.
At autopsy, 1 cow had 5–8-cm bone calluses in each of 4 fractured ribs (Fig. 1C). In both cows, the cortical bone of the ribs and the bone in the diaphysis of the humerus were thinner than normal bone. Histologically, the ribs of both cows had severe thinning of the cortical and trabecular bone tissue, and unmineralized osteoid covered the trabecular surfaces (Fig. 1D) and the osteonic canals.
The concentrations of PB in soil, P in forage, Pi in serum, and P in rib bone were all low (Table 1). The concentrations of Ca in blood were adequate in cattle in both outbreaks. The BW (mean ± SD) of cows with clinical signs (281 ± 29 kg and 330 ± 46 kg, for outbreaks 1 and 2, respectively) was lower (p < 0.001) than of cows without signs (411 ± 27 kg and 421 ± 35 kg, for outbreaks 1 and 2, respectively). However, neither the concentrations of serum Pi (0.84 ± 0.36 mmol/L vs. 0.87 ± 0.39 mmol/L) nor Ca (2.40 ± 0.23 mmol/L vs. 2.50 ± 0.17 mmol/L) were different (p > 0.05) between cows with and without signs in either outbreak.
Measurements in the 2 outbreaks of soil bicarbonate-extractable phosphorus (PB) concentration, amounts and components of pasture available, total P concentration of this pasture, inorganic P and Ca concentrations in serum of blood, and ash, P, and Ca concentrations of the 12th left ribs of 2 cows autopsied.
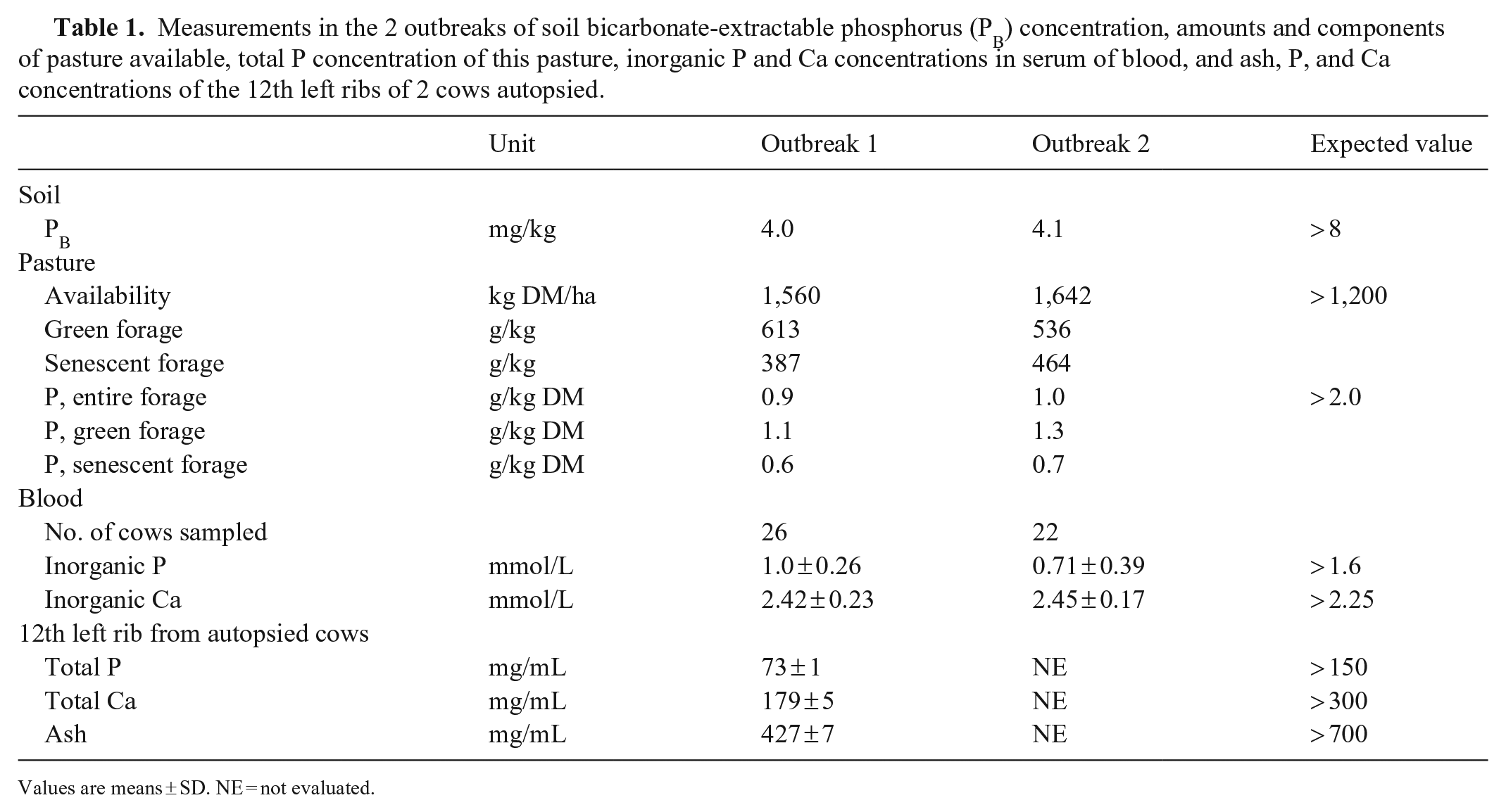
Values are means ± SD. NE = not evaluated.
More than a century after the early reports in Uruguay, osteomalacia continues to occur in extensive beef cattle production systems,16,19 even on ranches on which management has included P supplementation to address P deficiency, such as both outbreaks described here. The reasons that the management of mineral supplementation was not effective in avoiding osteomalacia included providing only small amounts of P as subcutaneous injectable supplements, insufficient amounts of mineral salt supplements or adequate amounts but for short periods, and mineral supplements with low P concentrations (40–50 g P/kg). Calculations from the P concentrations in forage and expected forage intakes (4–9 g P/d) and the P provided in injections or supplements (0.2–3 g P/d) together would have provided 20–55% of the expected P requirements of the cows (~21 g P/d).6,13 Furthermore, a national agricultural census in Uruguay reported that ~27% of ranches used mineral salt supplements, 12 and from market information, the amounts of supplements sold (~6,000 tonnes) 20 would have provided ~30% of the amount needed to supplement all cows on all ranches. Hence, the use of mineral salts has been insufficient.
As reported previously in Uruguay, 16 both outbreaks occurred during the summer (January–March). One reason for the higher incidence of the disease during summer may be the higher content of senescent forage in the pasture (38.7% in outbreak 1; 46.4% in outbreak 2). Senescent forage contains ~50% less P than green forage (Table 1). A higher frequency of osteomalacia has been related to the occurrence of drought years.3,6,9,16 This situation occurred in outbreak 2 (171 mm vs. 316 mm in long-term average for the summer) but not in outbreak 1 (369 mm), suggesting that osteomalacia may also occurs in years with normal rainfall. However, in outbreak 2, which occurred during a drought, the Pi in serum was lower (p < 0.01) than in outbreak 1. Osteomalacia may be the result of lower forage availability; however, both outbreaks had adequate forage availability (Table 1) and low stocking rates (0.5 and 0.44 cows/ha in outbreaks 1 and 2, respectively). Additionally, in Uruguay, summer is the time when beef cows are lactating and have higher P requirements.
In both outbreaks, cows with clinical signs of osteomalacia weighed 20–30% less than cows without signs, and in outbreak 1, 8 of 14 cows with signs were primiparous and weighed 226–285 kg. This was probably associated with low voluntary intake of pasture, which is an important consequence of P deficiency,6,9 and the difficulty for these animals to walk and graze effectively. Poor growth, as a result of lifelong P deficiency, over the longer term may also have contributed to the low weights of these cows.
The measurement of the soils, pastures, and animals in both outbreak herds provided strong evidence that the cows were severely P deficient and that this was the primary cause of the osteomalacia. The concentrations in soil of ~4 mg PB/kg and in forage of ~1 g P/kg were indicative of P deficiency. 6 There is widespread agreement that blood Pi for a group of cattle provides the best simple marker of P deficiency6,15; studies in Australia and South Africa have concluded that growing and lactating beef cattle with Pi concentrations of < 1 mmol/L and consuming diets of at least moderate quality are severely P deficient.7,15 Thus, the low Pi concentrations in both outbreaks provided direct evidence that the cows were severely P deficient.
The needle test of bone 18 has been demonstrated to be a simple and useful field test to evaluate mineral deficiency with osteopenia, such as P deficiency. In both outbreak herds, several affected cows were classified as “deficient” according to the needle test, but it is of some concern that some, and not all, of the cows with signs of osteomalacia were classified as “deficient.” Also, in the 2 cows that were autopsied, the results were consistent with low ash contents (427 mg/mL) and P concentration (73 mg/mL) in the ribs. A similar result has been reported in cows and heifers with P-deficient diets that, in addition, had up to ≥ 30% of unmineralized osteoid tissue, representing true osteomalacia resulting from P deficiency. 7
In our study, the measurements of P in soil, pasture, blood, and bone supported a final diagnosis of P deficiency. However, for routine field diagnosis of osteomalacia caused by P deficiency, the clinical signs, the needle test, and the serum Pi concentration together are excellent tools for the diagnosis of P deficiency. Additionally, to treat and prevent P deficiency, it is necessary to estimate the amount of P ingested from pasture to effectively provide the amounts of additional P needed to meet the P requirements of cows.
Given the occurrence of outbreaks of osteomalacia in some rangelands that are P deficient, and the greater prevalence of subclinical than clinical disease, it is recommended to increase the use of routine field diagnoses of P deficiency, and to improve application of P supplementation technology in regions known, or suspected, of being P deficient for grazing beef cattle.
Supplemental Material
sj-pdf-1-vdi-10.1177_10406387211025828 – Supplemental material for Osteomalacia as a result of phosphorus deficiency in beef cattle grazing subtropical native pastures in Uruguay
Supplemental material, sj-pdf-1-vdi-10.1177_10406387211025828 for Osteomalacia as a result of phosphorus deficiency in beef cattle grazing subtropical native pastures in Uruguay by Carlos O. Schild, Fabiana M. Boabaid, Luiz G.S. Olivera, Mizael Machado, Ana Vildoza, Anderson Saravia, Alejandra Custodio, Carolina Command, Agustín Martinez, Martín Jaurena, Rob Dixon and Franklin Riet-Correa in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank Benjamin Barros, Alejandro Botello, and Dr. Manuel Taño, the ranch owners and managers, for their assistance during the outbreaks. We thank Daniel Basaund, Carolina Ramos, Cecilia Alvarez, and Lucia Barrón for assistance with the laboratory analyses, and Microlab (Nafecor) for loaning the equipment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Our work was funded by grant FMV_1_2017_1_136347 from the Uruguayan “Agencia Nacional de Investigación e Innovación.” A postgraduate scholarship was provided to Carlos Schild by National Institute for Agricultural Research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.