
Abstract
A 27-y-old Anglo-Arabian gelding with bay coat color was presented with a swelling of the left maxillary region. Fenestration on the left maxilla revealed that the left maxillary sinus was filled with black-red tissue. A portion of the tissue was excised and diagnosed histologically as malignant melanoma. Genotyping of the STX17 gene for gray coat color revealed that the horse did not have the “gray” factor. The horse was euthanized ~3 mo after first presentation. During autopsy, a black-to-gray mass extended from the left nasal cavity to the surrounding paranasal sinus and invaded the hard palate, cribriform plate, and the cranial portion of the left olfactory bulb. Moreover, identical black nodules were present in lymph nodes from the mandible to the larynx, and in the spleen, liver, kidney, and adrenal glands. However, masses were not found in the skin, perineal region, or pelvic cavity. All of the black-to-gray nodules were malignant melanomas that were histologically identical to the initial biopsy; tumor emboli were also found in the kidney. Sinonasal mucosal melanoma is a rare disease in horses.
There are 2 types of melanocytic neoplasms: melanocytoma and malignant melanoma. 4 In horses, melanocytomas are benign neoplasms that are frequently found in the perineal region, the ventral surface of the tail, and on the head and neck region of gray horses.15,20 Melanocytoma in gray horses occurs most frequently in older animals, with very few cases < 5-y-old. 15 Breeds that are predisposed to melanocytomas are Arabian, Thoroughbred, Lipizzaner, Camargue, and Percheron. 15
In general, melanocytomas in gray horses tend to progress to malignancy in the long term.6,15,20 Malignant melanoma exhibits invasive growth and frequent metastasis.3,4,8,13,20,21 Melanocytic tumors in non-gray horses tend to be malignant melanomas. 6 Reports of 17 cases of malignant melanomas in non-gray horses > 8-y-old noted that stallions or geldings were more often affected;3,8,13,19–21 the most common tumor site was the tail.3,8,13,19–21
In human medicine, “mucosal melanomas” are a recently established category of melanocytic neoplasms and are a rare aggressive malignancy. They originate primarily in the mucosa of the respiratory, alimentary, and urogenital tracts, which contain melanocytes.10,11 In veterinary medicine, typical mucosal melanomas are canine oral melanomas, 14 yet very few cases of primary sinonasal melanoma have been reported in dogs.1,5,9 In horses, there are only 2 case reports of suspected mucosal melanomas.2,19 We detail here a case of malignant melanoma in a non-gray horse that appeared to originate from the sinonasal region with systemic metastasis.
A 27-y-old Anglo-Arabian gelding with a bay coat color was presented to the primary veterinarian because of a swelling of the left maxillary region (Fig. 1A) with suppurative nasal discharge. Two weeks later, the horse was referred to the Kagoshima University Veterinary Teaching Hospital (Kagoshima, Japan) because of these signs. Upon endoscopic examination, a mass was observed protruding into the left nasal cavity (Fig. 1B). On radiographic examination, a deposit with a sharp horizontal line was observed in the left maxillary sinus and was suspected to be fluid-like material (Fig. 1C). Trephination of the left maxilla revealed that the left maxillary sinus was filled with black-red tissue; a portion of the tissue was excised for histologic examination. Histologically, the collected tissue was composed of neoplastic cells containing intracytoplasmic melanin pigment, with infiltration of melanophages (Fig. 1D). The neoplastic cells exhibited nuclear and cellular atypia and many mitotic figures with the destruction of adjacent bone.
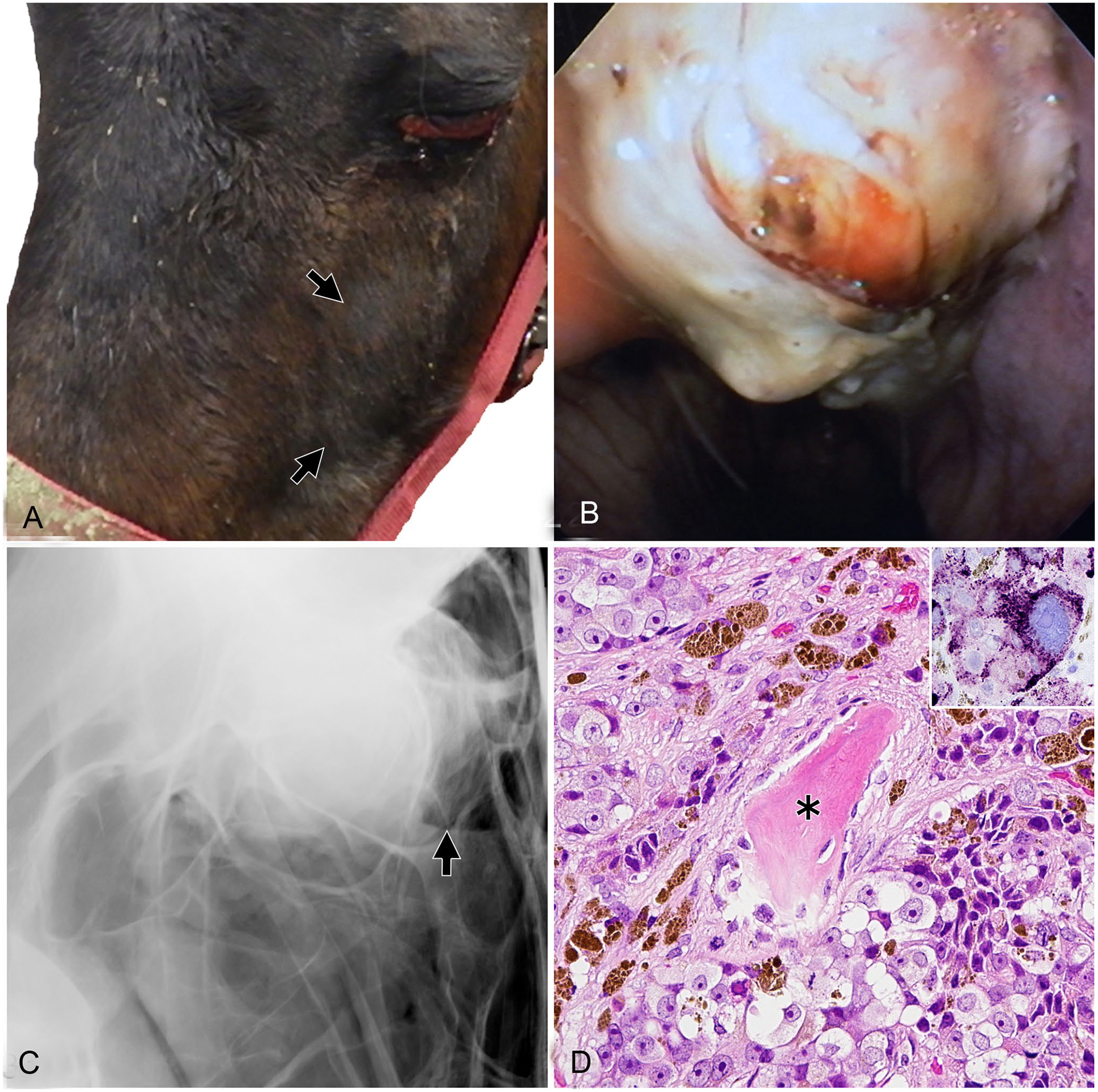
Clinical and biopsy findings of sinonasal malignant melanoma of a horse.
Immunohistochemistry using the anti-melanoma marker antibody (clone PNL-2; Santa Cruz Biotechnology) showed a positive reaction in the cytoplasm of the neoplastic cells (Fig. 1D, inset). Based on these findings, the mass was diagnosed as malignant melanoma. To genotype the gray coat color gene (syntaxin-17, STX17), we made minor modifications and followed a previous report. 16 Briefly, we performed long-range PCR using genomic DNA and DupForward primer, DupReverse-N primer, and DupReverse-D primer that amplified intron 6 in the STX17 gene under the following conditions: initial denaturation at 92°C for 2 min, followed by 35 cycles of denaturation at 92°C for 10 s, annealing at 55°C for 15 s, and extension at 68°C for 6 min. After final extension for 7 min at 68°C, PCR products were stored at 4°C. PCR products were subsequently measured by 0.8% agarose gel electrophoresis. Positive (gray) and negative (non-gray) controls for this test were obtained from Thoroughbred racehorses. We obtained the same PCR result as the negative control, thus confirming its non-gray color genotype.
Because the owner did not agree to aggressive therapeutic approaches (e.g., complete excision of the tumor), the horse was treated several times with irrigation, systemic administration of antibiotics, and oral administration of cimetidine; clinical signs did not improve. The horse returned to our hospital 2 mo later because of 10 d of anorexia. On physical examination, an intraoral black mass protruded from the hard palate, and black tissue proliferated on the gingiva around the left maxillary first molar, which was loose and markedly tender. One month later, the horse was euthanized given the poor prognosis.
Postmortem computed tomography revealed occlusion of the left sinonasal cavity by soft tissue, which partially invaded the right nasal cavity and oral cavity (Fig. 2A). During autopsy, a black-to-gray mass occupied the left nasal cavity and the surrounding paranasal sinus and invaded the hard palate (Fig. 2B), cribriform plate, and the cranial portion of the left olfactory bulb. Moreover, identical black nodules were present in lymph nodes from the mandible to the larynx, and in the spleen, liver, kidney, and adrenal glands (Fig. 2C). Similar masses were not found in the skin, perineal region, or pelvic cavity. Other lesions were found in the thyroid and pituitary glands. Both thyroid lobes had multiple white solid nodules, the largest of which was 1.5 cm diameter and in the left lobe. The pars intermedia of the pituitary gland was enlarged and contained several small nodules.
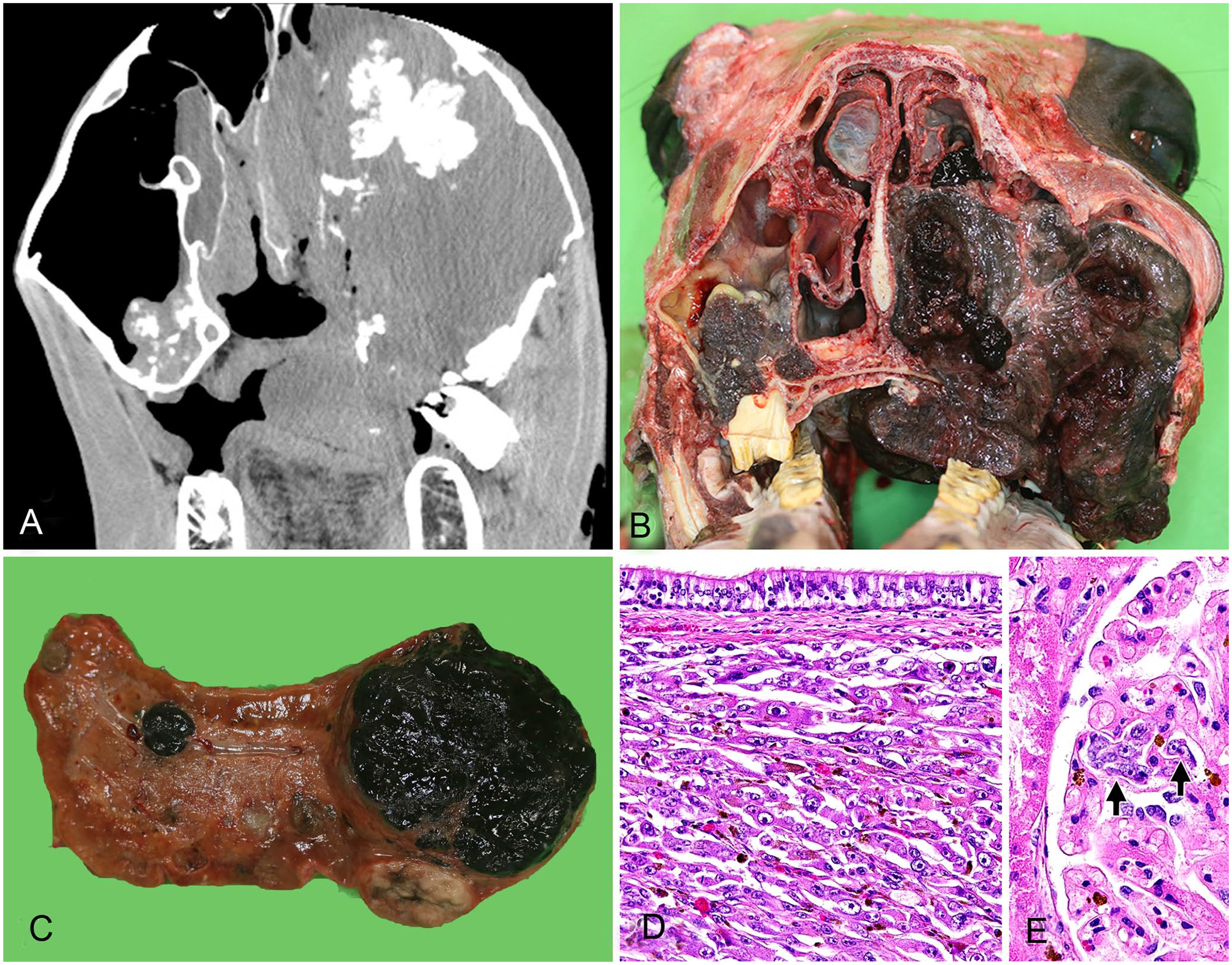
Postmortem findings of sinonasal malignant melanoma in a horse.
Histologically, all of the black-to-gray nodules were diagnosed as malignant melanomas, identical to the biopsy (Fig. 2D). Tumor emboli were also found in the kidney (Fig. 2E). The thyroid masses were diagnosed as C-cell adenoma and hyperplasia. The nodule in the pars intermedia was diagnosed as microadenoma with hyperplasia.
Our case was a mucosal melanoma that originated from the sinonasal mucosa, although we could not determine definitively if the maxillary sinus or nasal cavity was the original site. The most common site of mucosal melanomas in horses is not clear, given that only a few cases have been reported.2,19 However, the 2 previous suspected cases affected the head, consistent with our case. Additionally, a case of nasal melanoma has been reported in a pony. 2 However, information was not provided regarding coat color, precise site of melanoma, and metastasis. Moreover, the histologic diagnosis of the case was only described as melanoma, not distinguished as benign or malignant. In a case in a 9-y-old gelding, the masses extended from the left guttural pouch to the pharynx, and there were no other localizations of melanoma and no metastatic lesions. 19 Considering the size and extent of the major mass, the malignancy in our case may have existed for a long time prior to clinical signs and thus resulted in widespread metastasis.
There may be a genetic component to the development of malignant melanomas. Gray horses have a 4.6-kb duplication in the intron 6 of the STX17 gene, and the duplication is a dominant trait. 16 However, non-gray horses do not have this duplication. In addition, STX17 and the neighboring gene NR4A3 are overexpressed in several organs and especially in melanocytic tumors in gray horses. 16 STX17 is a member of the syntaxin family, which participates in vesicle transport, including the transport of melanosomes. NR4A3 is one of the cell cycle regulators and is linked to carcinogenesis. Thus, the 4.6-kb duplication in STX17 may enhance the expression of STX17 and NR4A3, and can contribute to the gray phenotype and accompanied melanocytic tumors in horses. 16 Genetic analysis of our case showed no duplication, and thus this result is consistent with the coat color phenotype. Therefore, the formation of malignant melanoma in our case likely differs from the pathogenesis of melanocytic tumors in gray horses.
Thyroid C-cell adenoma and nodular hyperplasia are common in older horses and are well known as incidental lesions at autopsy.7,12,17,18 Nodular hyperplasia of C cells may be initiated by hypercalcemia and is thought to be a preneoplastic change. In our case, the multiple nodules that formed in both thyroid lobes consisted of proliferation of well-differentiated C cells. According to the current pathology criteria, 18 the large tumors were adenomas because they had a capsule and compressed the surrounding tissue. The small nodules were hyperplasia given that there was no capsular formation and an ambiguous boundary.
Adenomas and hyperplasia of the pituitary pars intermedia are also frequently found in older horses.7,12,17,18 Hyperplasia of the pars intermedia is defined as extensive growth without a clear border. 7 Compressive proliferation with a capsule and fine fibrovascular septa are characters of adenoma, and small tumors (1–5 mm diameter) are termed microadenomas.7,12,18 Lesions in the pars intermedia of our case were determined to be microadenoma and hyperplasia.
In general, pituitary pars intermedia dysfunction (PPID) of horses is brought about by a pars intermedia adenoma leading to functional changes and upregulation of peptides, and typically gives rise to clinical manifestations of hirsutism, polydipsia, polyuria, muscular atrophy, and increased appetite.12,17,18 We did not conduct a hormone examination in our case because the horse did not display either typical lesions or signs of PPID. Thus, the functional effects of the changes in the pars intermedia were unclear; adenoma and hyperplasia of the pars intermedia are not always functional. 12 The hypophysial lesions found in our case appear to have been nonfunctional.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.