
Abstract
A conventional dairy farm, housing 19 Austrian Simmental cows, experienced a spontaneous outbreak of a Mycoplasma bovis infection, showing severe clinical signs of respiratory tract disease, clinical mastitis, and tremendous drop in milk production. Despite intensive therapy, 5 cows died within 2 weeks or were euthanized. From the remaining cows, bacteriological culture and polymerase chain reaction revealed M. bovis in 10 of 14 milk samples. Mycoplasma bovis was found in 1 of 5 randomly collected nasal swabs. Autopsy of 1 cow revealed infection of the lungs and the udder with M. bovis. The 13 M. bovis isolates from milk samples, nasal swabs, lungs, and udder were genotyped by multilocus variable number of tandem-repeat analysis, and indicated that described infections were caused by a single M. bovis strain. The virulent M. bovis strain resulted in dramatic economic loss to the farmer. To control the disease, culling of all animals, including heifers and calves, was recommended, and strict hygienic measures were implemented before introducing new animals to the farm.
Mycoplasma bovis was first isolated in 1961 in the United States from cattle with severe mastitis 10 and has been detected in many other countries worldwide since then. 15 Cattle trade, transport stress, and growing herd size increase the risk of introducing the pathogen into herds, resulting in higher prevalence of bovine Mycoplasma diseases.5,8 In Austria, the first cases of Mycoplasma-associated mastitis (M. bovis and M. bovigenitalium) were reported in 2006, 2 followed by the emergence of the disease in successive years predominantly caused by a single endemic strain. 20 Mycoplasma bovis has not only been identified as a major pathogen for respiratory tract disease and polyarthritis in beef cattle worldwide,6,12 but it has also been implicated in other clinical manifestations, such as mastitis, otitis, and reproductive disorders. 15 Infections with M. bovis often predispose the respiratory tract, particularly of calves, to other pathogens (e.g., Mannheimia haemolytica and Trueperella pyogenes). 4 The association with virus infections is less clear, but the immunosuppressive effect of Bovine viral diarrhea virus 1b and 2 is suspected to play a synergistic role in M. bovis pathogenesis. 26
Conventional culture procedures for the identification of M. bovis infections are expensive and time-consuming and often produce false-negative results caused by overgrowth with bacteria or fast-growing commensal mycoplasmas or previous antibiotic use. Culture of mycoplasmas, however, is still a widely performed standard test providing isolates and strains for genotyping in order to evaluate the epidemiology of mycoplasma infections. Today, highly sensitive species-specific polymerase chain reaction (PCR) systems are also widely used in the diagnosis of mycoplasma-associated diseases including M. bovis infections. 25 In contrast, combining generic PCR with denaturing gradient gel electrophoresis enables the simultaneous detection of multiple mycoplasma species involved in mixed infections. 13 Alternatively, DNA microarray technology also offers highly specific detection of many different species. 24 For both latter technologies, however, laboratory costs for equipment and performance do not allow for routine use. An inexpensive and rapid screening method is serology (e.g., indirect ELISA), measuring a host’s antibody response against M. bovis. 17 Although M. bovis strains can exhibit multiple antigenic membrane configurations, 22 which may affect the reliability of these screening tests, 23 medium to high antibody titers have suggested an active infection in a suspicious herd. 16 Furthermore, culture of bulk tank milk samples on a regular basis has been recommended to monitor the herd mycoplasma mastitis status. 20
Our case report describes a spontaneous outbreak of a M. bovis infection with a strain isolated in Austria for the first time, which resulted in severe clinical signs and dramatic economic losses. In February 2014, a dairy herd experienced a sudden increase in the incidence of clinical respiratory tract diseases and a tremendous drop in milk production. The conventional dairy farm was family managed and located in the Austrian province of Styria. This area is characterized by a low concentration of farms, which are predominantly small- to medium-sized with <50 cows. 18 The described herd consisted of 19 Simmental dairy cows. Within the last 5 years, no animals were purchased and introduced to the herd. All animals (dairy cows, heifers, and calves) were housed in 1 free-stall barn, separated by fences. The mean daily milk production was 28 kg per cow. The dairy producer reported that within 4 days, 8 cows developed severe dyspnea with fever (39.2–40.6°C), coughing, nasal discharge, and drooling (Table 1). Despite therapy by the local veterinarian with antibiotics and non-steroidal anti-inflammatory drugs (Table 1), the respiratory tract disease progressed and affected 13 of 19 cows, 5 of which died within 2 weeks. In the next 3 weeks, the local veterinarian diagnosed and treated clinical mastitis in 10 of the 14 remaining cows (Table 1). Affected quarters were swollen and firm. The secretions were yellow and flaky. In the clinical course, some affected quarters showed reduction in volume and indurated tissue. Quarter milk samples from 4 cows were sent to a laboratory for bacteriological examination. In 2 samples, T. pyogenes or Streptococcus agalactiae were isolated, and 2 samples were negative for microbial growth.
History, clinical signs, rectal temperature, and treatment of the remaining cows, heifers, and calves, recorded by the dairy producer and the local veterinarian.
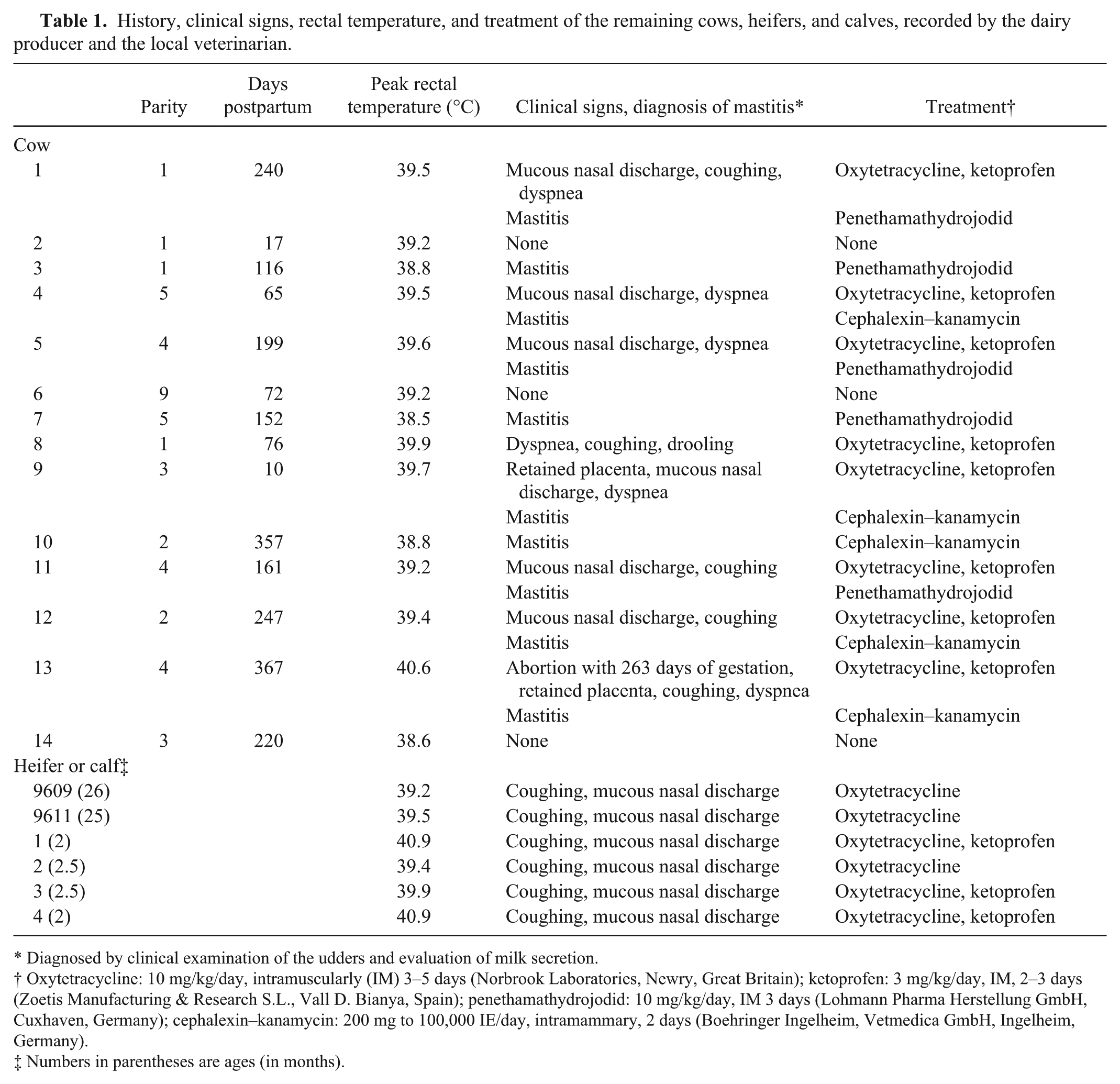
Diagnosed by clinical examination of the udders and evaluation of milk secretion.
Oxytetracycline: 10 mg/kg/day, intramuscularly (IM) 3–5 days (Norbrook Laboratories, Newry, Great Britain); ketoprofen: 3 mg/kg/day, IM, 2–3 days (Zoetis Manufacturing & Research S.L., Vall D. Bianya, Spain); penethamathydrojodid: 10 mg/kg/day, IM 3 days (Lohmann Pharma Herstellung GmbH, Cuxhaven, Germany); cephalexin–kanamycin: 200 mg to 100,000 IE/day, intramammary, 2 days (Boehringer Ingelheim, Vetmedica GmbH, Ingelheim, Germany).
Numbers in parentheses are ages (in months).
The average herd somatic cell count in milk increased from 138,000/mL in January to 352,000/mL in March. The dairy producer estimated that herd milk production dropped by 60% and dry matter intake by 30–40%. In the end, milk could be delivered from only 4 cows, whereas 7 cows developed chronical mastitis; milk had to be withdrawn or milk production ceased almost completely and the cows were not milked any further (n = 3).
Furthermore, 2 of 8 heifers and 4 of 5 calves showed reduced appetite or elevated temperature and were treated as shown in Table 1. All heifers and calves recovered from clinical signs within 1 week after treatment.
In cooperation with the Clinical Unit for Herd Health Management (Clinic for Ruminants, Vetmeduni Vienna, Austria), clinical examinations of all 14 remaining cows were performed 4 weeks after the first clinical case of respiratory disease (Table 2). These cows showed almost no interest in fresh feed, the environment, or people in the barn, and were depressed. The average body condition score of the cows was low (mean 2.5 on a 5-point scale). At the clinical examination of the udders, in 4 cows, 1 or more quarters were small and indurated on palpation. During the entire course of clinical disease, no udders were painful on palpation. No other abnormalities, such as nodules or abscesses, were detected in the quarters. In 9 cows, secretion from 1 or more quarters was watery with flakes, but odorless (Table 2). At the time of clinical examination, signs of a respiratory tract disease were detected only in 3 cows, but not in heifers or calves. These 3 diseased cows were separated from the herd and moved to an area outside the stable.
Results of California Mastitis Tests (CMTs), clinical examination of the quarters, bacteriological results of milk samples, clinical examination of respiratory tract, and further examinations performed 4 weeks after the first clinical case on the farm.
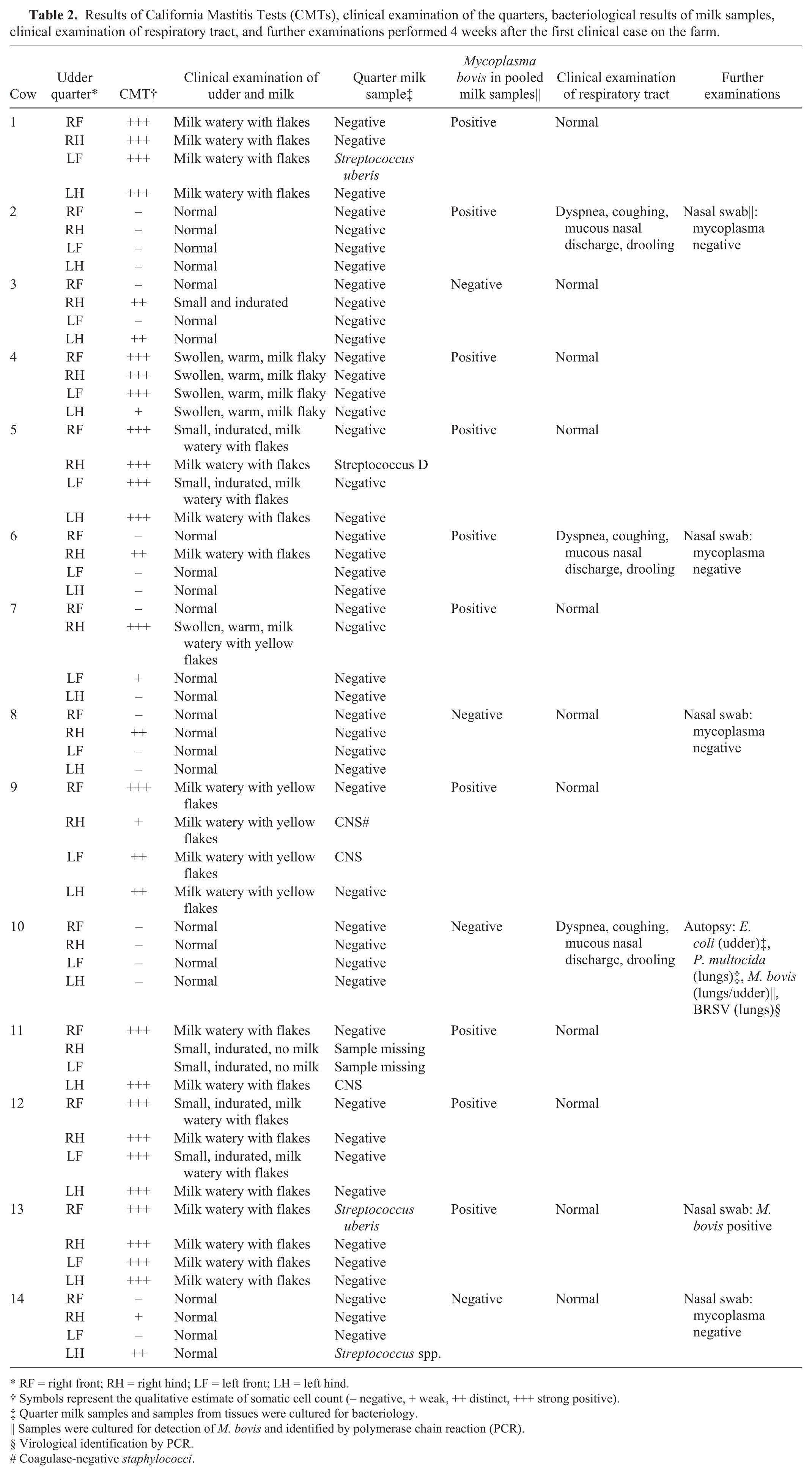
RF = right front; RH = right hind; LF = left front; LH = left hind.
Symbols represent the qualitative estimate of somatic cell count (– negative, + weak, ++ distinct, +++ strong positive).
Quarter milk samples and samples from tissues were cultured for bacteriology.
Samples were cultured for detection of M. bovis and identified by polymerase chain reaction (PCR).
Virological identification by PCR.
Coagulase-negative staphylococci.
From all 14 cows, quarter milk samples were taken for bacteriological culture, and pooled milk samples of each cow were taken for detection of mycoplasmas. Five randomly selected cows were sampled for bacteriological and virological analyses of nasal swabs. Nasal swabs were taken with a sterile, unguarded cotton swab after cleaning the nares with a sanitary wipe. The swabs were inserted deep (~15–20 cm) into 1 naris of each animal and then placed in a holder containing charcoal-free Amies transport medium before transferring to the laboratory. All samples were sent to the Institute of Microbiology, Vetmeduni Vienna, Austria.
One cow was euthanized because of severe signs of respiratory tract disease and treatment failure (Fig. 1). Autopsy was performed on this cow at the Institute of Pathology, Vetmeduni Vienna, Austria.
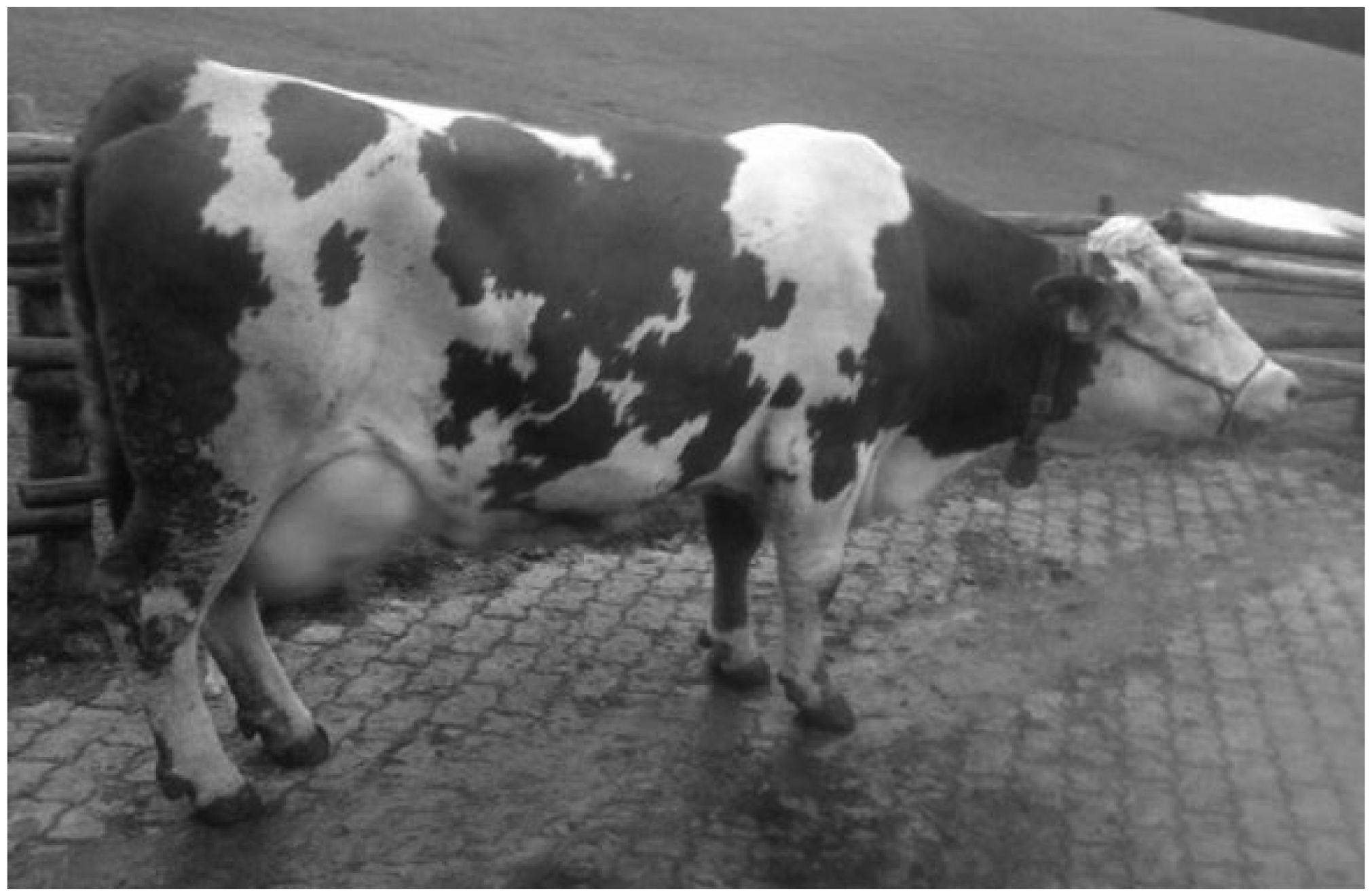
Cow with severe dyspnea. This cow was euthanized and autopsied.
Mycoplasma bovis was isolated from 10 of 14 pooled milk samples by culture using modified Hayflick agar at 37°C under microaerophilic conditions 25 followed by identification employing PCR targeting the uvrC gene. 28 The latter described technique was performed to analyze nasal swabs, in which 1 of 5 was positive for M. bovis, as well as the lungs and the udder of the autopsied cow, which revealed an infection with M. bovis. All results of bacteriological and virological examinations are summarized in Table 2.
In summary, M. bovis was identified in 10 milk samples, in 1 nasal swab, and in the lungs and in the udder of the autopsied cow. To evaluate the epidemiology of the presented case, all 13 M. bovis isolates were genotyped applying multilocus variable number of tandem-repeat (TR) analysis targeting 10 M. bovis–specific TR loci (TR29, TR30, TR31, TR35, TR40–41, TR49–51, TR59, TR147, TR148, and TR427) as described previously.1,29 Multilocus variable number of TR analysis generated identical profiles for all 13 M. bovis isolates differing from those produced by previously isolated Austrian and geographically unrelated M. bovis strains. 27 This finding strongly suggests that the presented outbreak arose from a single source and was caused by a single M. bovis strain. Histologic examination of the lung and the udder of the autopsied cow revealed necrotizing bronchopneumonia, chronic pleuritis, and pyogranulomatous galactophoritis, with marked fibrosis (Fig. 2).

Bovine lung showing necrotizing bronchopneumonia from which Mycoplasma bovis was isolated.
Because of the severity of signs, the unresponsiveness to treatment, the persistence of the infection, and the permanent risk of new infections via contact between the animals in the same barn,3,19 culling of all animals, including young stock, was recommended to eradicate M. bovis. Furthermore, cleaning and disinfection of the stables and all equipment (disinfectant based on 5% iodine or 0.2% peracetic acid) was recommended as essential to eradicate mycoplasma from the farm. The dairy producer waited 14 days after depopulation before new animals were introduced to the farm. 20
It can be surmised that this outbreak was associated with dramatic economic losses caused by milk loss in the beginning and the final cessation of milk delivery, loss of animals, and costs for treatment and diagnosis. Mycoplasma spp. is considered to be one of the major mastitis pathogens, causing high economic losses per case per lactation of ~$350 result of decreased milk production. 30 In the longer term, however, the risk of transmission was demonstrated to be a major determinant of the cost of clinical mastitis. 7 In the present outbreak, culling of all cattle, in particular before they achieved the best body condition for slaughtering, and costs for purchasing new animals increased the total costs. Furthermore, current costs for the farm (e.g., costs for feeding animals, electricity, bank loans, and several other cost factors) must be included in a full financial calculation.
Our report on an acute infection in dairy cattle with dramatic economic losses demonstrates the virulence of the M. bovis strain involved. M. bovis has been identified as the most pathogenic mycoplasma species in bovine respiratory tract disease also causing a variety of other clinical manifestations. 16 Because of its ability to vary the expression of certain membrane surface proteins, which may enable M. bovis to adapt to changing environmental conditions and to evade the host’s immune response, associated diseases are often chronic in nature. 14 Certain mycoplasmas including M. bovis strains are able to form biofilms, which may also account for chronicity and the lack of response to chemotherapy. 14 It is well known that β-lactam antibiotics such as penicillin and cephalosporin are not effective, as mycoplasmas lack a cell wall. Resistance of M. bovis in vivo against macrolides, oxytetracycline, spectinomycin, and florfenicol has been determined in a 2014 study. 9 The primary concern with the treatment of mycoplasma infections, however, is persistence of the bacteria, regardless of susceptibility to antimicrobials. 8
In this particular mycoplasma outbreak, severe signs of respiratory tract disease were detected in cows, whereas signs of disease in younger cattle, as described elsewhere,6,8,16 were less pronounced. Reasons for this remain unclear. Mycoplasma spp. associated with mastitis is spread primarily from cow to cow during milking.8,21 Mycoplasma bovis, however, can also spread to the udder via the hematogenous route following respiratory tract disease. 11
Footnotes
Acknowledgements
We acknowledge the involved farm manager and local veterinarian for their excellent cooperation.
Authors’ contributions
H Pothmann, J Spergser, and M Drillich contributed to conception and design of the study. J Elmer and M Iwersen contributed to analysis of data. I Prunner and D Klein-Jöbstl contributed to analysis and interpretation of data. H Pothmann drafted the manuscript. All authors gave critically revised manuscript; final approval; and agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared that they received no financial support for their research and/or authorship of this article.