
Abstract
A 21-year-old male African elephant (Loxodonta africana) died suddenly with no previous medical history. Grossly, there were severe multifocal epicardial and endocardial hemorrhages of the atria and ventricles, hydropericardium, multifocal pleural hemorrhages, and severe pulmonary congestion and edema. Histologically, there was fibrinoid vasculitis and thrombosis in the heart and lung and myocardial necrosis. Citrobacter freundii was isolated in abundance in pure culture from liver and heart samples. Low levels of multiples types of elephant endotheliotropic herpesvirus (EEHV-6, EEHV-2B, and EEHV-3A) were detected in spleen samples, but not in heart samples. The levels of EEHV DNA found were much lower than those usually associated with acute EEHV hemorrhagic disease, and many other genomic loci that would normally be found in such cases were evidently below the level of detection. Therefore, these findings are unlikely to indicate lethal EEHV disease. Polymerase chain reaction for encephalomyocarditis virus (EMCV) and toxicology for oleander (Nerium oleander) were negative. Stress, resulting from recent transport, and antimicrobial therapy may have contributed to the death of this animal.
A 21-year-old captive-born male African elephant (Loxodonta africana; European Endangered species Programme studbook #9201) was sent to Bioparc Valencia (Spain) from Cantabria (Spain), where he had been on breeding loan since 2009. No previous diseases were reported in this animal, and results of blood work carried out 4 days before transport were within normal limits for the species. One superficial wound on the right hind limb resulting from chaining during transport was noted, and preventive treatment with enrofloxacin was given orally for 3 weeks before the death of the animal. On January 23, 2013, the animal was found lying on the floor at 7:00
The autopsy was performed immediately after the death of the elephant by pathologists from the Veterinary School of the University CEU Cardenal Herrera (Valencia, Spain). The animal was thin with reduced fat deposits. There was an 8 cm × 4 cm skin wound on the cranial aspect of the right hind foot. The surface of the wound was white and firm (granulation tissue), and no exudate or necrotic tissue was observed. There were ~10 L of clear fluid (ascites) in the abdominal cavity. The pleura had >50 multifocal to coalescing, irregular-shaped, dark-red to black areas that were well-circumscribed, and 1–10 cm in diameter (Fig. 1). The lungs were diffusely red and heavy, and white foam oozed from the bronchi on cut surface. The pericardial sac contained ~250 mL of clear fluid. On the endocardial and epicardial surfaces of both atria and ventricles, there were >50 irregular-shaped dark-red lesions, ranging from pinpoint to 4 cm in diameter (Fig. 2). The lesions were especially extensive and marked in the endocardium around both atrioventricular valves, reaching the papillary muscles of both ventricles (Fig. 3). On cut section, these dark plaques barely penetrated the myocardium. The cecum contained >100 white, round worms identified as Murshidia hadia. 14 Histologic sections from the skin, lung, heart, stomach, small and large intestine, liver, spleen, kidney, adrenal gland, pancreas, lymph nodes (submandibular, retropharyngeal, mediastinal, mesenteric), brain, and eye were examined. The main histologic findings were observed in heart and lung. The heart showed epicardial and endocardial hemorrhages with myocardial necrosis (Fig. 4), fibrinoid vasculitis, and thrombosis. There was severe pulmonary congestion and edema with hyaline membranes in the alveolar spaces (Fig. 5). Also, fibrinoid vasculitis and thrombosis (Fig. 6) and mild granulomatous pneumonia with intralesional fungal hyphae (morphology consistent with Aspergillus sp.) were observed. Granulomatous typhlitis was present, likely because of the intraluminal nematodes.

African elephant (Loxodonta africana). Multifocal subpleural hemorrhages in the lung.
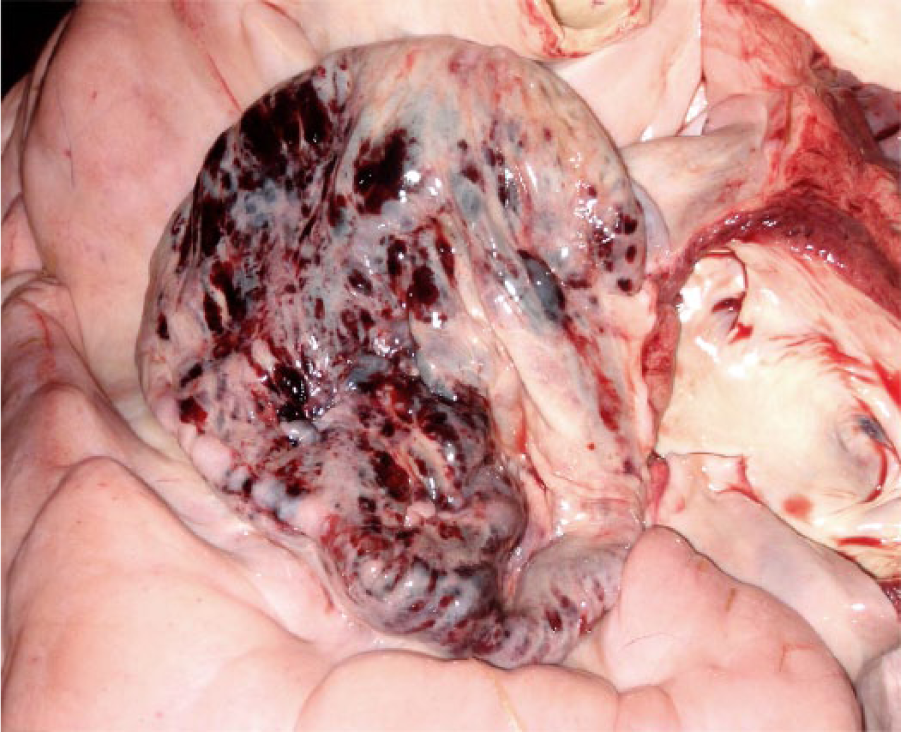
Epicardial petechiae and ecchymoses in the right atria of the heart.
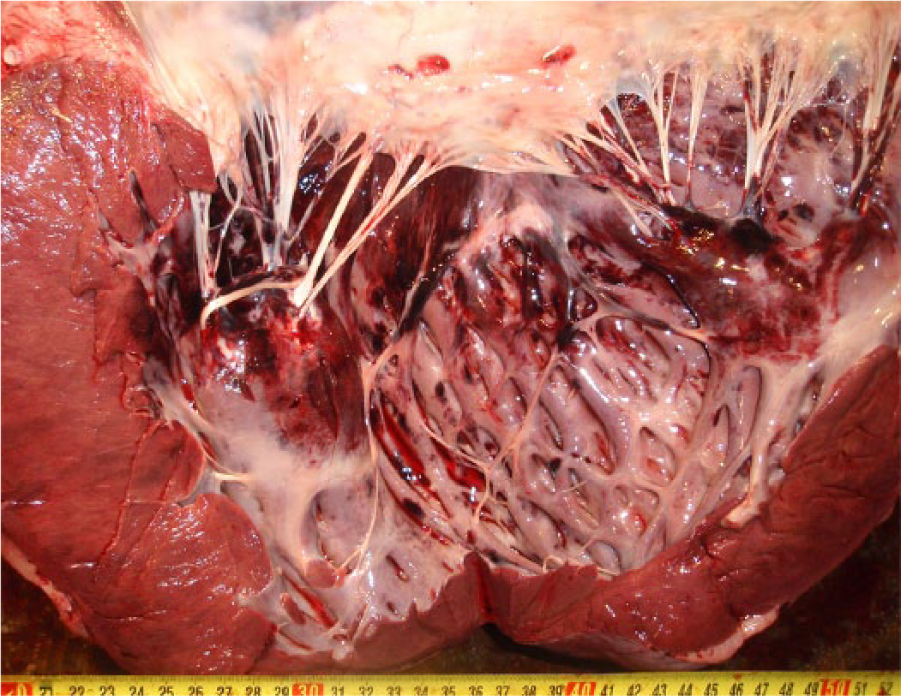
Multifocal to coalescing hemorrhages of the endocardial surface of the left ventricle.
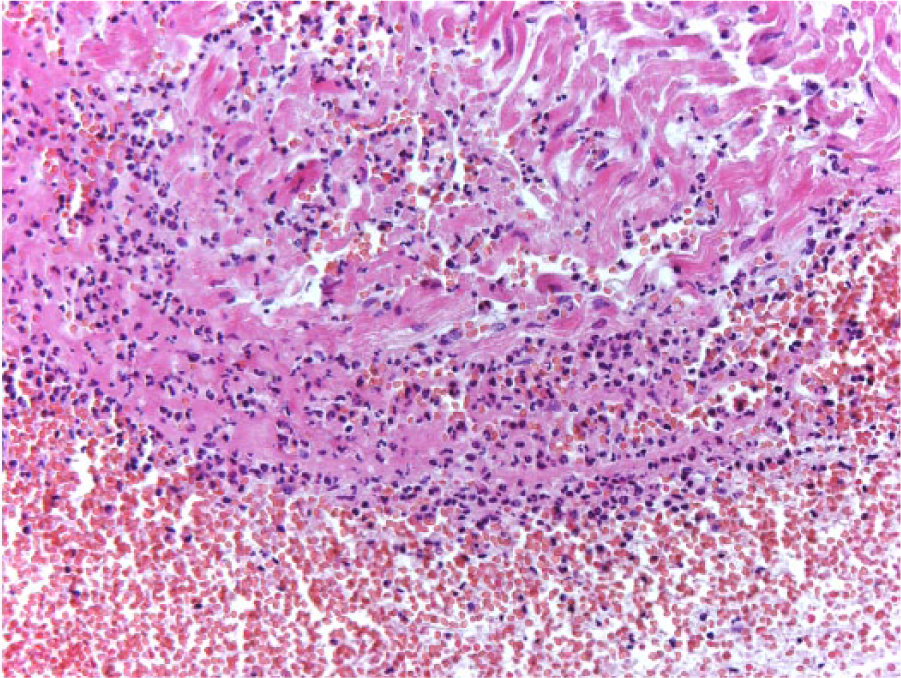
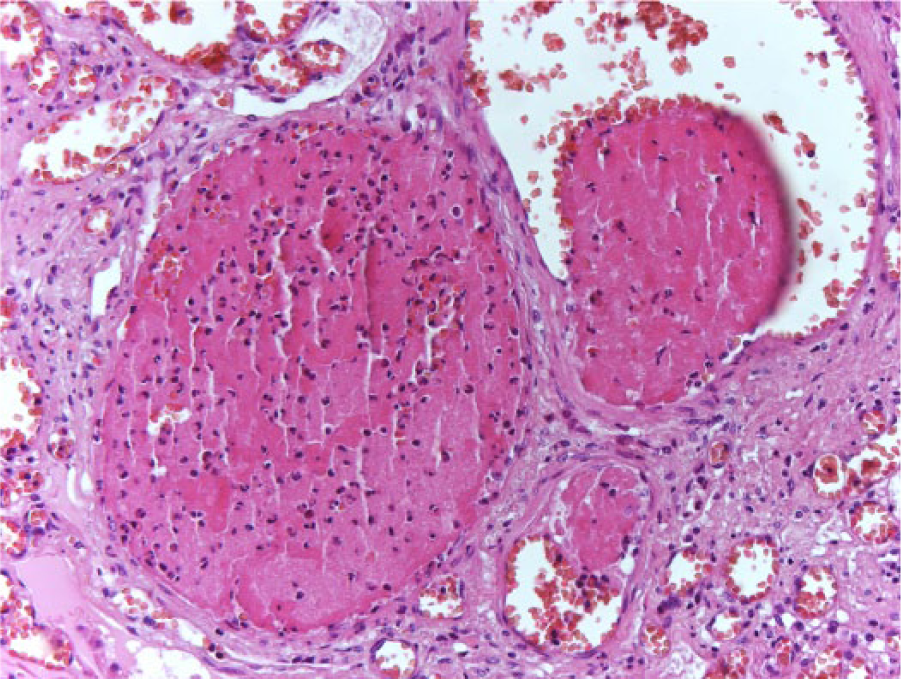
Hemorrhage and acute necrosis of the papillary muscle of the left ventricle. Hematoxylin and eosin.
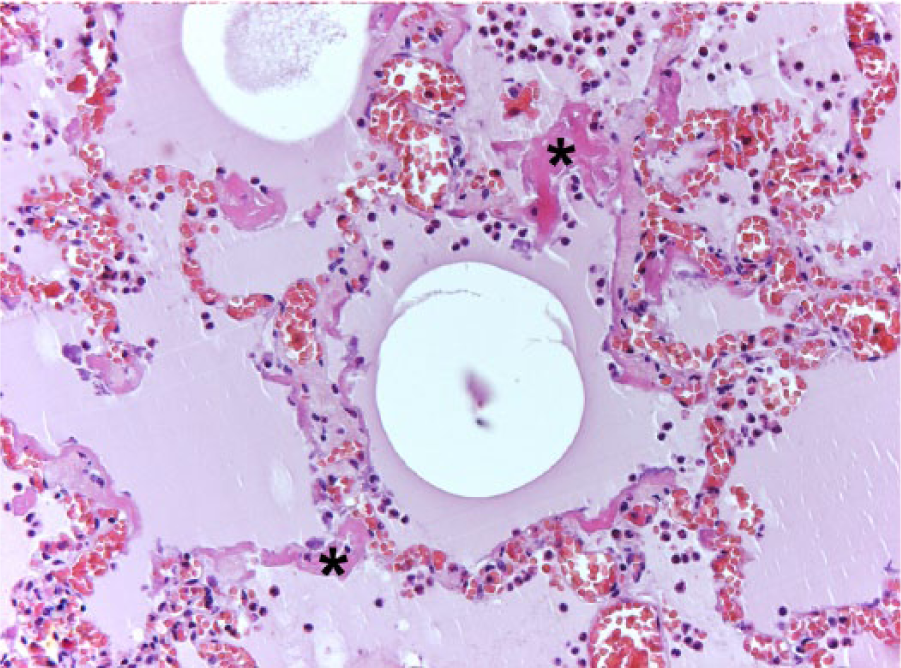
Congestion, hypercellularity, alveolar edema, and hyaline membranes (asterisk) in the alveolar spaces of the lung. Hematoxylin and eosin.
Venous thrombi in the lung. Hematoxylin and eosin.
Samples from the liver and heart were cultured on blood agar and MacConkey agar. The intestinal contents were cultured on blood agar, MacConkey agar, Salmonella–Shigella agar, campylosel agar, and selenite broth under aerobic conditions, and on blood agar, chocolate agar, and thioglycollate broth under anaerobic conditions. All culture media were provided from a commercial source a and were incubated at 37°C for 72 hr before they were judged negative. Citrobacter freundii was isolated in abundance in pure culture from the liver and heart and in low numbers from intestinal content. Identification of the isolates was carried out using a commercial microbial identification system. b The isolates from the liver and heart showed resistance to penicillin, ampicillin, amoxicillin + clavulanic acid, cephalothin, cefazolin, cephalexin, cefoxitin, oxytetracycline, nalidixic acid, and enrofloxacin. C. freundii isolates were screened for mutations in the quinolone resistance–determining region of the gyrA and parC genes by polymerase chain reaction (PCR). 18 Both isolates had a single amino acid substitution in the GyrA protein (Thr-83→Ile), which is sufficient to decrease susceptibility to fluoroquinolones. 18
Spleen and heart samples were evaluated for encephalomyocarditis virus (EMCV) and elephant endotheliotropic herpesvirus (EEHV) using PCR. For EMCV detection, total RNA was extracted from tissue samples using a kit for automated purification of viral RNA from cell-free body fluids c and an automated machine, d according to the manufacturer’s recommendation. Briefly, after lysis in an optimized buffer and adjustment of binding conditions, the sample was loaded directly onto a spin column. Viral RNA bound to the silica membrane, and contaminants were completely removed in 2 wash steps. A one-step real-time reverse transcription (RT-)PCR for EMCV detection was performed using RT-PCR reagents. e The RT-PCR enzyme mix included in the kit was composed of a mutant Moloney Murine leukemia virus (M-MLV) RT capable of producing high complementary DNA yields and hot-start DNA polymerase for target amplification. e The included RT-PCR buffer contained optimized reagents for efficient and robust reverse transcription and PCR; it also contained the passive reference dye, ROX (5-carboxy-X-rhodamine), for quantitative fluorescent signal normalization. The primers and TaqMan probe used are located in the conserved sequence of the EMCV 3D gene. 3 All of the tested samples were found to be negative.
For EEHV detection, DNA was isolated from frozen samples of both spleen and heart using a commercial kit. f Conventional PCR was performed, using degenerate EEHV-type common pol and multiple type-specific primers. EEHV-2, EEHV-3, and EEHV-6 viral DNAs were detected at low levels from spleen samples. To evaluate which subtypes of these 3 viruses were present, as well as to exclude the possibility of laboratory contamination from previously analyzed cases, all positive amplified bands of the expected size were subjected to Sanger cycle DNA sequencing. The results revealed a novel strain of EEHV-6 (hel locus, GenBank accession KM282203), a novel subtype of EEHV-2B (pol, tk loci, KM282198, KM282199), and 2 slightly different strains of EEHV-3A (pol, ter, obp loci, KM282200–KM28202). Many other PCR loci that were tested for these and other EEHV types were negative. All positive loci required second- or third-round PCR amplification to obtain bands of sufficient abundance to be sequenced, indicating far lower levels of viral DNA than in autopsy tissue DNA from all previous lethal cases of EEHV disease that have been examined, which were usually positive after first-round PCR (E Latimer, unpublished information).
Samples of the intestinal content and tissue samples of the heart and liver were analyzed by high-performance liquid chromatography (HPLC) for pesticides and poisons, including cardiotoxic glycosides (oleandrin). First, samples were screened for the heart glycoside oleandrin using an HPLC apparatus g connected to highly sensitive triple quadrupole with an ion trap h operated in multiple reaction monitoring (MRM) mode. Second, systematic toxicological analysis (STA) for other drugs, poisons, pesticides, and their metabolites using an HPLC apparatus connected to a high-resolution mass spectrometer. The time-of-flight mass spectrometry (TOF MS) library encompassed 1,318 substances with their intact masses and a highly resolved tandem mass spectrometry (MS/MS) library with 521 entries. In none of the samples could oleandrin be detected. The limit of detection for oleandrin was estimated to be at 0.5 ng/g organ by the MRM approach and at 5 ng/g organ by the STA approach. The STA approach revealed enrofloxacin and metamizole in heart tissue samples. Both medications were part of the emergency treatment. No other drug, pesticide, or poison that could explain the lesions and death of the elephant was detected in the samples.
The main lesions were observed in the heart and lungs, and consisted of multifocal hemorrhages with fibrinoid necrosis and thrombosis, hyaline membranes in alveoli, and acute myocardial necrosis. The presence of hyaline membranes has been associated with diffuse alveolar damage occurring in the acute exudative phase of interstitial pneumonias. 4 However, none of these lesions were specific, thus differential diagnoses such as plant poisoning (mainly by Oleander sp.), viral infection (by EEHV or EMCV), or septicemia were considered.9,10 Only 2 small fungal granulomas were observed histologically in the lung (in 1 of the 10 sections examined), which was interpreted as an incidental finding.
Oleander toxicosis has been described in several species. There is a single report of plant poisoning in elephants in the veterinary literature involving the death of 2 African elephants by ingestion of Cryptostegia grandiflora, a plant that contains cardiac glycosides, 2 and the possibility of oleander poisoning in elephants is also mentioned by Fowler. 10 However, oleander poisoning was ruled out. EMCV, which has been implicated in the acute deaths of elephants both in captivity24,26 and in the wild, 13 was ruled out by PCR techniques.
EEHV should be included in the differential diagnosis in cases associated with sudden death and heart hemorrhages such as in our report. 22 The EEHV DNA types detected by targeted second- and third-round PCR approaches included EEHV-2, EEHV-3, and EEHV-6. Each of these virus types have been found previously at high levels in blood samples from rare cases of acute symptomatic viremia in young elephants in North America.12,15,23 The only known EEHV-2 case was lethal in a 1-year-old African elephant calf, 23 and the EEHV-6 case was in a surviving 1-year-old African elephant calf. 15 Multiple examples of mixed infections with several strains of EEHV-2, EEHV-3, and EEHV-6 together have also been found in localized lung nodules or skin nodules from asymptomatic healthy adult elephants both in the wild in South Africa and in Kenya, as well as in a zoo elephant in the United States. 27 In our case, low levels of several types of EEHVs were detected in DNA extracted from the spleen, and none was detected in DNA extracted from the heart. The levels of EEHV DNA found were much lower than those usually associated with acute EEHV hemorrhagic disease, and many other genomic loci that would normally be found in such cases were evidently below the level of detection. Therefore, these findings are unlikely to indicate lethal EEHV disease. The lymphoid lung nodules that have been observed to carry EEHVs in many otherwise healthy adult African elephants in the wild 16 as well as in at least 1 zoo African adult 27 resemble enlarged reactive hyperplastic lymphoid follicles.
Citrobacter freundii, a Gram-negative bacterium of the family Enterobacteriaceae, is a ubiquitous and opportunistic pathogen. In humans, bacteria of the genus Citrobacter are infrequent causes of infections in neonates, infants, and immunocompromised adults.7,25 In animals, it has been associated with septicemia in American alligators (Alligator mississippiensis), 19 a patas monkey (Erythrocebus patas), 20 dogs, 11 Australian king parrots (Alisterus scapularis), 5 and in a stranded newborn Cuvier’s beaked whale (Ziphius cavirostris). 8 In all of these cases, there were obvious immune-compromising factors associated with septicemia, or the animals were in poor body condition. It has also been reported to be associated with an epizootic infection in a colony of guinea pigs. 21 In our case, no other pathogenic bacteria were isolated from the intestinal contents.
In the present case, the elephant was recently transported from northern Spain to Valencia, a road distance of ~700 km. Transport is an important stressful factor that is associated with both acute and long-term stress. 6 Elevated fecal glucocorticoid metabolites as an indication of stress have been detected in domesticated African elephants in South Africa within 1–2 months after transportation, and a period of at least 3 months is recommended in order to allow translocated elephants to acclimate to their new surroundings. 17 Thus, we cannot rule out that the elephant transported 2 months before was still under the effect of post-transport stress, and this may have interfered with its immune competence. 9 It can also be speculated that the previous antimicrobial treatment may have triggered a subsequent overgrowth by C. freundii. Dysbacteriosis was also suspected as a predisposing factor in an outbreak of fatal enterocolitis in Asian elephants caused by Clostridium difficile. 1
Our report describes the association of C. freundii with acute septicemia in an elephant. Although C. freundii is an uncommon pathogen, its role as cause of death has been described both in humans and in other animal species. No evidence of clinically relevant infection by any other agents was found in the present case. The results suggest that this multidrug resistant strain of C. freundii played a main role in the disease process, although we cannot rule out that some other agents, not detected by the performed tests, could also be present. The source of infection remains unknown. C. freundii was isolated in low numbers from intestinal content, but no active enteritis or colitis with presence of bacteria (which could lead to septicemia) was observed in the sections examined from the intestine. However, no Citrobacter was cultured in fecal samples obtained from the remaining elephants of the herd. The elephant developed the disease 2 months after transportation, and immediately after initiation of an antimicrobial, suggesting that the enrofloxacin treatment may have produced a microbial imbalance and the overgrowth of this particular strain of C. freundii due to its low susceptibility to fluoroquinolones. The clinical significance of the herpesvirus in this case is unknown.
Footnotes
Acknowledgements
We thank D Viana, L Selva, A Barragan, M Penadés, and A García for helping during autopsy, M Garijo and J Cardells for parasite identification, and F Uzal, L Lowenstine, and P Pesavento for histology review. We appreciate the assistance and interest of the following colleagues: B Puschner, JM Sánchez-Vizcaino, C Rubio, A Dastjerdi, and T Hildebrandt.
Authors’ contributions
J Ortega, JM Corpa, MD Carbonell, and M Casares contributed to conception and design of the study. J Ortega, JM Corpa, and M Casares contributed to acquisition, analysis, and interpretation of data. MD Carbonell and AC Gerique contributed to acquisition and analysis of data. A Roemmelt and A Romey contributed to analysis of data. JA Orden, J Blanco, E Latimer, and GS Hayward contributed to analysis and interpretation of data. T Kraemer and LB Kassimi contributed to interpretation of data. J Ortega, JM Corpa, JA Orden, and M Casares critically revised the manuscript. All authors drafted the manuscript, gave final approval, and agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
bioMérieux SA, Marcy l’Etoile, France.
b.
VITEK 2 system, bioMérieux SA, Marcy l’Etoile, France.
c.
QIAamp viral RNA mini kit (ref. 52926), Qiagen GmbH, Hilden, Germany.
d.
QIAcube, Qiagen GmbH, Hilden, Germany.
e.
AgPath-ID one-step (ref. 4387424), Applied Biosystems, Foster City, CA.
f.
Generation column kit, Qiagen GmbH, Hilden, Germany.
g.
Ultimate 3000, Thermo Fischer, Dreiech, Germany.
h.
5500 QTrap, ABSciex, Toronto, Ontario, Canada.
i.
5600 TripleTOF, ABSciex, Toronto, Ontario, Canada.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.