
Abstract
The objective of the current review is to provide the reader with an overview of the bovine hematological profile. Sample collection, bovine reference ranges, and cattle-specific characteristics of erythrocyte, leukocyte, and platelet parameters are reviewed. Furthermore, diseases associated with abnormalities in the complete blood cell count of cattle are discussed.
Introduction
Hematologic analysis is not only relevant for diagnosing disorders of the hematologic system but also helpful in the diagnosis of many organ and systemic diseases. Although the diagnosis of a disease can only occasionally be based solely on a complete blood cell (CBC) count, the hemogram may contribute valuable information in the diagnosis, surveillance, and formulation of a prognosis regarding the future progression of a disease in an individual. The objective of the current review is to provide bovine clinicians and laboratory technicians with an overview of the sample collection process, bovine reference ranges, cattle-specific properties of blood cells, and diseases associated with abnormalities in the hematological profile of cattle. Because automated cell counters have become more and more popular in veterinary practice, the focus of the present review is on abnormalities detectable by automated cell counters (i.e., abnormalities in the number, volume, and hemoglobin concentration of blood cells rather than on abnormal morphology). However, if pathological or irregular results are discovered, or abnormal morphology or blood cell function impairment is suspected, an additional microscopic blood smear evaluation is strongly recommended.
Blood sampling and storage
The most accessible and commonly used vessels for blood collection in cattle are the external jugular vein and the coccygeal vessels. If possible, animals should be calm to avoid stress-related changes of the hemogram.22,39 For hematologic analysis, samples must be collected in tubes coated with anticoagulant agents, preferably potassium–ethylenediamine tetra-acetic acid (EDTA/K3) with a concentration of 1.27 mg EDTA/K3 per ml of blood, or disodium–ethylenediamine tetra-acetic acid (EDTA/Na2) with a concentration of 1.5 mg EDTA/Na2 per ml of blood. Heparin is not recommended for general hematological use in cattle because it results in deviations of leukocyte counts. 13 Mixing should occur by carefully inverting the tube several times. The correct blood quantity should be collected in the sample tube, because an inappropriate ratio of sample blood to anticoagulant might cause erroneous results for red blood cell (RBC) parameters and indices. Samples can be stored up to 24 hr at 4°C. Platelet counts should be conducted within 4 hr after venipuncture.22,39,47
Bovine hematological reference ranges
The most appropriate reference range is generated from a group of healthy animals with environmental and physiological characteristics as similar to the patient as possible. As in all species, a certain amount of physiological variability is observed in hematologic profiles of cattle. Variables that contribute to the thresholds and width of reference intervals include age, sex, stress, diet, body condition, reproductive status, recent activity, hydration, ambient temperature, and altitude.28,50 Reference intervals for bovine hematologic parameters from 3 sources are summarized in Table 1.
Bovine hematology reference intervals according to 3 sources.*
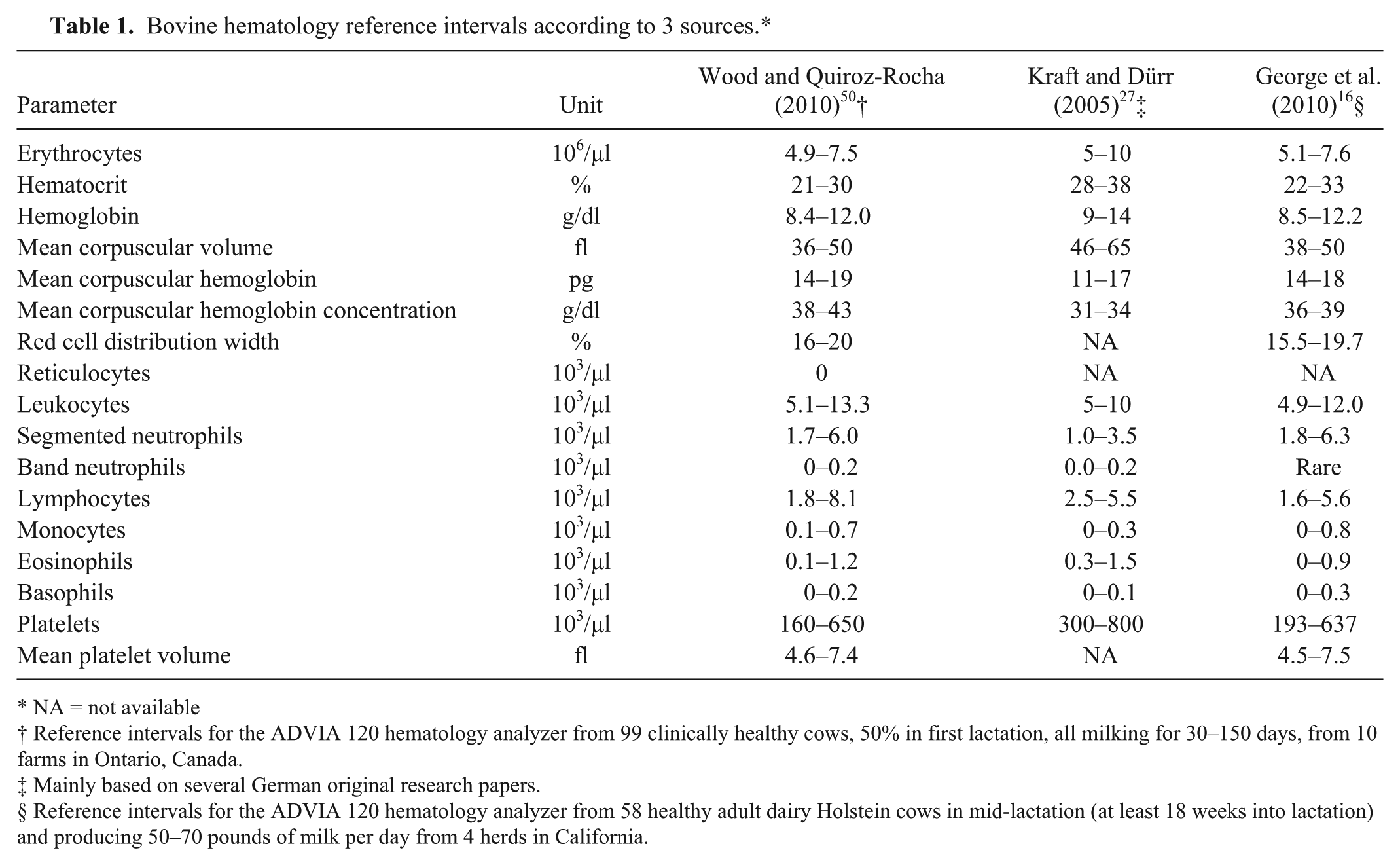
NA = not available
Reference intervals for the ADVIA 120 hematology analyzer from 99 clinically healthy cows, 50% in first lactation, all milking for 30–150 days, from 10 farms in Ontario, Canada.
Mainly based on several German original research papers.
Reference intervals for the ADVIA 120 hematology analyzer from 58 healthy adult dairy Holstein cows in mid-lactation (at least 18 weeks into lactation) and producing 50–70 pounds of milk per day from 4 herds in California.
Many commonly used hematology reference intervals originate from research undertaken in the 1960s. A 2010 study 16 compared reference intervals of healthy North American cows from 1957 to 2006 to account for changes in the CBC count during the past 50 years. The main findings included a significant increase in reference ranges for neutrophil counts over the study period, whereas reference intervals for lymphocyte, monocyte, and eosinophil counts as well as hemoglobin concentration had decreased. Genetic selection and decreased prevalence of bovine virus diarrhea were suggested as possible reasons for higher neutrophil counts. 16 Animals persistently infected with Bovine viral diarrhea virus (BVDV) exhibit significant neutropenia, 35 thus the absence of persistently infected animals in the study might have contributed to increased neutrophil numbers. The reduced eosinophil count was assumed to be caused by decreased exposure to parasites due to modern husbandry and parasite control programs. The authors recommended that laboratories should establish their own reference ranges to reflect current cattle populations. 16
Red blood cell parameters and their interpretation
Erythrocytes have an average diameter of 5–6 μm in cattle, which is small compared to other species. The key function of erythrocytes is the transport of oxygen, which is bound to hemoglobin. Erythropoiesis, which takes approximately 5 days, is stimulated by erythropoietin and occurs in the bone marrow parenchyma. Bovine erythrocytes have a relatively long life span of 130–160 days.7,50
An RBC count typically includes the total number of RBCs, hematocrit (HCT), hemoglobin (HGB), erythrocyte indices, and occasionally the red cell distribution width (RDW). Erythrocyte indices include mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). 7
In general, beef cattle breeds have higher RBC counts than dairy cattle, bulls have greater RBC counts than cows, and nonlactating cows have higher RBC counts than lactating cows. 50 In calves, HGB, MCH, and MCHC decrease during the first month and then start to increase during the first 3 months of life. 31 In young calves, RBC counts might be higher, and MCV and MCHC might be lower than in adults.9,22
Common indications for RBC analysis are clinical anemia or hemorrhage. In absolute anemia, RBCs, HGB, and/or HCT are decreased. Relative anemia is caused by an increase of plasma volume (e.g., during pregnancy or after fluid therapy). Anemia can be categorized into regenerative and nonregenerative anemia according to the bone marrow response, and can also be classified with regard to the cell size (normocytic, macrocytic, and microcytic, indicating normal, increased, and decreased MCV, respectively) and hemoglobin concentration (normochromic, hypochromic, and hyperchromic, indicating normal, decreased, and increased HGB, respectively).7,27
Causes for regenerative anemia are hemorrhage or hemolysis. With acute blood loss, the RBC parameters are initially within the reference ranges because cells and plasma are lost in the same proportion. Diminished RBC count and HGB can be found only after several hours, when fluid in the blood vessels is replaced and dilutes the blood. In cattle, regeneration of erythrocytes begins after approximately 2 days, and takes weeks to be fully accomplished. In chronic hemorrhage, RBC count, HCT, and HGB are decreased while reticulocytes as well as MCV are increased. In ruminants, only a moderate rise in reticulocytes is observed in responding anemia. If regenerative capacity is depleted, chronic bleeding anemia can become nonregenerative. 7 Causes for hemorrhage include trauma, abomasal ulcers, hemorrhagic enteritis, vena cava syndrome, blood-sucking parasites (e.g., Haemonchus spp., lice, or ticks), hemostasis defects, and vessel erosion or rupture. Hemolytic anemia is caused by blood parasites, toxins, electrolyte imbalances, hypoosmolality,7,19,22 or autoimmune reactions. 40 In cattle, common causes for hemolysis include unsuitable food and toxic plants, such as cabbage (Brassica spp.), onions (Allium cepa), rye grass (Lolium spp.), or red maple (Acer rubrum).2,7,19,21,50 Microorganisms infecting ruminant RBCs include rickettsia (Anaplasma marginale),1,20,26 protozoa (Babesia spp., Theileria spp., Trypanosoma spp., and Sarcocystis spp.),1,7,20,22,34,53 or bacteria (Mycoplasma wenyonii, Leptospira spp., and Clostridium spp.).1,22,37 Further factors are copper deficiency or chronic copper intoxication,22,30,50 hypophosphatemia (postparturient hemoglobinuria),7,19,29 and water intoxication.19,27,41
Nonregenerative anemia generally occurs in the following combinations: normochromic and normocytic, normochromic and macrocytic, or hypochromic and microcytic.7,27 Normochromic, normocytic anemia is seen in nonspecific disease, especially during chronic inflammation. It is also observed in connection with erythropoietin deficiency due to chronic renal disease or endocrine disorders, as well as bone marrow depression, certain drugs (e.g., estrogen, chloramphenicol, or cytotoxic cancer medication), toxins (e.g., lead poisoning), abscesses, and neoplasia.7,15,22 Normochromic, macrocytic anemia occurs with deficiencies in vitamin B12, folic acid, or cobalt.7,19 It is also found in polled Hereford dyserythropoietic anemia, a congenital anemia accompanied by dyskeratosis and progressive alopecia. 49 Hypochromic, microcytic anemia is commonly caused by iron deficiency as observed during chronic hemorrhage or in calves raised solely on milk,19,22 but microcytes are also observed in copper deficiency, pyridoxine deficiency, or lead toxicosis. 7
The term polycythemia is used to describe increased RBC, HCT, and/or HGB. Relative and absolute polycythemia are differentiated. Relative polycythemia is triggered by a reduction in plasma volume in dehydrated individuals or by splenic contraction. Absolute polycythemia is caused by an increased number of erythrocytes. Primary polycythemia or polycythemia vera is a myeloproliferative disorder resulting from autonomous stem cell proliferation. Secondary polycythemia is triggered by increased erythropoietin production. It occurs under hypoxic conditions, which can be of physiological (e.g., high altitude) or pathological (e.g., pulmonary or cardiac disorders) origin. It is also observed with renal tumors and cysts.7,22,27 A bovine hereditary polycythemia is known in Jersey and Hereford cattle. 19
The RDW is the coefficient of variation of the RBC volume distribution and is a measure of anisocytosis. 7 The RDW can be presented as a diagram with the cell volume on the x-axis and the number of cells on the y-axis. The presence of macrocytosis or microcytosis results in abnormal peaks and a wider distribution. In healthy calves, MCV is decreased, resulting in a wider RDW. Further examples of conditions associated with an increased RDW include iron deficiency, or other trace mineral deficiencies associated with macrocytic or microcytic anemia.4,9,24,27
The small size of ruminant erythrocytes might cause falsely low results for RBC counts if automated analyzers are not calibrated correctly for cattle. Erroneous results for RBC parameters and indices might also occur due to in vitro hemolysis or inadequate blood sample–to–anticoagulant ratio, which might cause erythrocyte shrinkage or dilution. 22
White blood cell parameters and their interpretation
White blood cells (WBCs) or leukocytes play an essential role in immune defense, and include different subpopulations: neutrophil, eosinophil, and basophil granulocytes, monocytes, and lymphocytes. Leukocytes are produced and mature in the bone marrow, and, in the case of lymphocytes, in the lymphoid tissues. The number of leukocytes in the blood constitutes only a small percentage of the total population and undergoes wide fluctuation. In the vasculature, a marginal pool and a circulatory pool of neutrophils are differentiated. The marginal neutrophils are attached to the endothelial cells, but detach and join the circulatory pool if blood pressure rises and the blood flow velocity increases. Therefore, every change in blood pressure can result in a change in the amount of leukocytes present in the blood.27,48
A complete WBC count is composed of the total number of leukocytes, the relative differential blood count, and the absolute differential blood count. Usually, the different subpopulations, as well as band and segmented neutrophils can be distinguished.27,50
In cattle, the total number of WBCs decreases with age. 19 Lymphocytes are the dominant subpopulation, but the lymphocyte proportion varies with age. The newborn calf has more granulocytes than lymphocytes.22,50 During the first month of life, calves exhibit a decrease in the overall number of WBCs, neutrophils, and lymphocytes, followed by an increase thereafter. 31 Within approximately 3 months, the lymphocyte percentage increases up to 80% of the total circulating WBC population. In the adult, the lymphocyte concentration decreases progressively but remains the dominant cell type. The neutrophil-to-lymphocyte ratio in adult cattle is approximately 1:2, which is low compared to other domestic animals.22,46,50 Eosinophils are below adult reference ranges after birth and increase with age.9,27,50
Compared with other species, cattle have a small bone marrow reserve for granulocytes. This results initially in a neutropenic rather than a neutrophilic reaction in an early inflammatory process. Neutrophilia and a left shift might be observed only after the speed of granulopoiesis is increased. After 3–5 days, immature and mature neutrophils might rebound.19,22,46,50 Cattle neutrophil counts rarely exceed 30,000 cells/μl.46,48 Neutrophil numbers decrease in the postpartum period, 18 and lactating cows have lower WBC counts than nonlactating cows. 50
Indications for a leukogram include diagnostics, general health assessments, monitoring of a disease, or monitoring of therapeutic actions. However, it is seldom possible to come to a definite diagnosis based solely on a WBC count. 27 Sequential leukograms can help establish a prognosis. The return of the leukogram within normal limits together with clinical improvement can be interpreted as a favorable sign, whereas a rapid fall in leukocytes without clinical improvement is regarded as a grave prognostic sign. Guarded or poor prognoses should be formulated with persisting neutropenia, a degenerative left shift, or severe persistent leukocytosis.19,22,48
The mechanisms underlying leukocytosis include increased release from the bone marrow, decreased emigration into the tissues, and a shift of cells from the marginal into the circulatory pool. 48 Physiologic leukocytosis is seen in association with stress, excitation, fear, exercise, or parturition. A stress leukogram is characterized by neutrophilia, lymphocytopenia, eosinopenia, and occasionally monocytosis. It is triggered by endogenous or exogenous corticosteroid exposure.22,25,27,46 A short-term physiological leukocytosis is also observed after epinephrine release.22,46 Causes for pathological leukocytosis include infectious diseases, endogenous or exogenous intoxication, endocrine conditions, central nervous disorders, anaphylactic shock, leukemia, and bovine leukocyte adhesion deficiency (BLAD). 27
Leukopenia is caused by decreased production, increased tissue demand, and consumption combined with marginalization. In general, it is observed in connection with viral infections, circulatory shock, peracute inflammation, cytotoxic substances, as well as hematopoietic stem cell disorders and bone marrow atrophy. 27 In cattle, leukopenia often occurs with metabolic disorders, liver disease, and infectious diseases (e.g., mucosal disease, paratuberculosis, or salmonellosis). Panleukopenia, a depression of all WBC subpopulations, is observed in viral disease (e.g., mucosal disease, infectious bovine rhinotracheitis), rickettsiosis, bacterial septicemia, and purulent splenitis. 19
The most common causes for neutrophilia are chronic inflammation and stress. Chronic inflammation has been reported among other infections of the udder, urogenital tract, gastrointestinal tract, liver, respiratory tract, heart, and central nervous system. In bovines, neutrophilia is also commonly observed with acute purulent processes, such as endometritis or metritis, retained placenta, acute bacterial mastitis, and foreign body peritonitis.19,46 Inflammatory neutrophilia is seen in viral, bacterial, protozoal, parasitic, and fungal infections.46,48 Additionally, neutrophilia is observed with noninfective inflammation (traumatic injuries, necrosis, infarction, burns, thrombosis, etc.), neoplasia, intoxication, endocrine disorders, hemorrhage, and hemolysis.27,48 In cattle, stress-induced neutrophilia is also associated with abomasal displacement, ketosis, indigestion, and dystocia.48,51,52 Severe leukocytosis, exceeding 40,000 cells/μl and sometimes even 100,000 cells/μl, based on a marked increase in neutrophils may be a sign of BLAD in Holstein Friesians. BLAD is usually diagnosed in calves, and most affected calves die within 1 year of age.17,32,33,48
Neutropenia occurs in ruminants during the first 1 or 2 days of severe, acute inflammation, including sepsis, mastitis, peritonitis, metritis, enteritis, and pneumonia. It can be caused by viral (BVDV, Bluetongue virus, Border disease virus), 46 rickettsial (Anaplasma phagocytophilum,43,46 Ehrlichia ruminantium), protozoal (Theileria sp.),34,46 and fungal infections, as well as bone marrow disease, toxins, neoplasia, or idiosyncratic drug reactions.27,48
Conditions commonly associated with eosinophilia include type I (immediate)23,45 hypersensitivity reactions and parasitic infection.22,27,46 Additional causes are neoplasia, infections, and drug reactions. 48 Eosinopenia might also occur in the early phase of infectious diseases, uremia, and acute hemolysis. 27 Extreme eosinopenia has been associated with Theileria infections.34,46
Basophilia has been linked to hyperlipidemia and occasionally to allergies, ulcerations, 27 and parasitic infections (ticks).8,46 Basopenia is not commonly reported in the literature because basophil reference intervals often include zero.46,48
Lymphocytosis can occur in the healing phase of infectious diseases, during chronic antigenic stimulation due to infectious agents, neoplasia, and hypoadrenocorticism.27,48 Reactive lymphocytosis is observed during chronic purulent diseases, such as hepatitis, peritonitis, pericarditis, nephritis, mastitis, or bronchopneumonia. 19 Bovine leukemia virus (BLV) is the causative agent of enzootic bovine leukosis. Infection with BLV results in a persistent lymphocytosis driven by an increase in B cells with abnormal lymphocyte morphology in up to 30% of affected cattle. Only a small percentage of animals with lymphocytosis develop bovine lymphoma. In some cases, WBC counts may exceed 100,000 cells/μl.3,12,22
Reasons for lymphocytopenia include acute stress, viral or bacterial infection, immune suppression, chronic renal insufficiency, and application of corticosteroids.22,27 It is also induced by loss of lymph and disruption of lymph node architecture (e.g., in paratuberculosis, inflammation, or neoplasia). 48
Monocyte numbers are variable in cattle and are thus not a sensible indicator for a specific disease. 22 Monocytosis has been observed during acute stress and in the healing phase of acute as well as chronic infections. It is further caused by hemolysis, hemorrhage, exudative inflammation, necrosis, ulceration, and corticosteroid therapy.27,48 Monocytosis was also found to be a successful marker of bacteremia and bacterial endocarditis 48 as well as puerperal infections. 19 Monocytopenia may be associated with endotoxemia, 46 viremia, and inflammation, 22 but has so far not been proven to have much clinical relevance. 48
With automated cell counters, falsely low WBC counts might occur due to clumping of leukocytes, and falsely high WBC counts might be caused by nucleated red blood cells, insufficient lysis of erythrocytes, excessive Heinz bodies, or clumping of platelets. 48
Platelet parameters and their interpretation
Platelets are anuclear cytoplasmic fragments of megakaryocytes, and play an essential role in hemostasis.6,38 With an average mean platelet volume (MPV) of 4.0–4.8 femtoliters, bovine platelets are small compared to those of other species. 5 Up to 30–40% of platelets are sequestered in the spleen and enter circulation in response to epinephrine release. Thrombocytes are also stored in the liver and bone marrow.6,38 Bovine platelets survive up to 10 days in peripheral blood. 50 In intact blood vessels, platelets circulate predominantly in the marginal pool. 27 The total number of platelets is influenced by the amount of production, consumption, sequestration, and loss.6,38
Platelet numbers increase significantly during the first 2 weeks of age and more slowly thereafter during the first 3 months. Platelet counts in calves might be within 31 or above adult reference intervals. 9 The following parameters can be estimated: total number of platelets, MPV, thrombocrit or plateletcrit, and platelet distribution width.6,38
In practice, a count of platelets might be indicated with severe hemorrhage or increased bleeding tendency. This includes clinical signs such as petechia, ecchymosis, hematuria, epistaxis, melena, hematemesis, and hyphema.38,44
Thrombocytosis occurs physiologically as a consequence of epinephrine-induced splenic contraction. Essential or primary thrombocytosis is an uncommon myeloproliferative condition. Reactive or secondary thrombocytosis is triggered by cytokine release and is observed in connection with stress, chronic blood loss, inflammation, neoplasia, or iron deficiency. Enhanced thrombopoiesis is also seen with inherited megakaryocyte disorders.6,42 An increased platelet count might be associated with an increased risk for thrombosis.6,27
Thrombocytopenia is found in excessive consumption (e.g., with blood loss, disseminated intravascular coagulation, or thrombocytopenic thrombotic purpura), decreased platelet production (e.g., in myelophthisis or bone marrow hypoplasia linked to toxins), destruction (e.g., due to infections, toxins, drugs, neoplasia, or immune-mediated), or distribution disorders (e.g., splenomegaly).6,27,38,44 Examples for infectious diseases causing thrombocytopenia include salmonellosis, leptospirosis, babesiosis, theileriosis,34,44 anaplasmosis, 43 and BVDV infection.6,10,36,44 Examples for toxins leading to platelet destruction are bracken fern (Pteridium aquilinum), mycotoxins (trichothecene), black fly (Simuliidae spp.) toxin, and coumarin rodenticides.19,44 Thrombocytopenia associated with leukopenia and bone marrow depletion is observed in bovine neonatal pancytopenia, a hemorrhagic disease of newborn calves observed since 2006, which is thought to be linked to an inactivated vaccine against BVDV in dams.11,14
Enlarged platelets are associated with accelerated production as well as myeloproliferative disorders and hyperthyroidism. 38 Decreased MPV or platelet fragments are observed in iron-deficiency anemia, bone marrow failure, and immune-mediated thrombocytopenia. 6
Automated cell counters should be calibrated adequately to account for the small size of bovine platelets. Falsely elevated platelet counts might be flagged if fragmented RBCs or WBCs are erroneously counted as platelets by an automated analyzer. 42 Platelet clumping might be a reason for indication of thrombocytopenia in automated cell counters. Platelet clumping can result from exposure to EDTA exceeding 4–6 hr or from use of heparin as an anticoagulant.22,44 Storage of blood in EDTA tubes over 4 hr at room temperature or refrigerated might cause platelet swelling, resulting in falsely increased MPV. Storage over 24 hr can result in fragmentation of platelets.6,38
Conclusions
Physiological and pathological characteristics of the bovine hemogram were discussed. The results of a CBC count are often helpful in the diagnosis, monitoring, and prognosis of a disease. If automated cell counters are used to obtain a CBC count, results should be interpreted with care to avoid false-positive or false-negative outcomes. If in doubt, a manual microscopic evaluation of the blood sample should be carried out. In cattle, changes in the CBC count, especially in the leukogram, might not be as pronounced as in other species even during severe illness. Therefore, a diagnosis or prognosis should not be based on hematologic results solely, but should also take findings from the clinical examination or other diagnostic procedures into consideration. 19
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.