
Abstract
Two separate incidents of monensin exposure in horses resulting in toxicosis provided insight into the diagnostic value and interpretive criteria of various biological samples. In case 1, 25 horses broke into a shed and ingested feed that was supplemented with 800 g/ton (880 µg/g) of monensin. Within 48 hr, 1 horse had died, 2 developed cardiac arrhythmias, lethargy, and recumbency, and another was euthanized due to severe deterioration. Minimal histologic lesions were noted in the horse that died peracutely, while another showed characteristic lesions of acute cardiomyocyte degeneration and necrosis. Stomach content, heart, liver, urine, and serum revealed various detectable concentrations of monensin in clinically affected and unaffected horses with known exposure. In case 2, a pastured horse had access to a mineral mix containing 1,600 g/ton (1,760 µg/g) of monensin. Within 48 hr, the horse became symptomatic and was euthanized because of severe respiratory distress. Histologic cardiac lesions were minimal but detectable amounts of monensin were found in blood, heart, liver, and stomach contents. In both cases, monensin toxicosis was confirmed with toxicological analysis. These cases demonstrate an overall lack of correlation of monensin concentrations in various biological samples with clinical outcome. However, serum, urine, blood, liver, heart, and stomach content can be tested to confirm exposure. More importantly, the consistently higher concentrations found in heart tissue suggest this is the most useful diagnostic specimen for postmortem confirmation of toxicosis in horses especially in cases in which associated feed cannot be tested for monensin or in cases with no histologic lesions.
Monensin, a monovalent carboxylic polyether ionophore antibiotic, is approved for use by the U.S. Food and Drug Administration as a feed additive for certain classes of ruminants and poultry. Unfortunately, unintended exposure can and does occur in other species with dire consequences. Horses are exquisitely sensitive to monensin; a reported median lethal dose (LD50) of 2–3 mg/kg for horses 10 is substantially lower than the LD50 of 21.9–80 mg/kg that has been estimated for cattle. 9 Several cases of monensin toxicosis in horses have been reported in the veterinary literature.1,2,7,13,14 In all these cases, a diagnosis of monensin poisoning was based on finding high levels of monensin in the feed in association with appropriate clinical or histologic evidence of myopathy. To the authors’ knowledge, a fatal monensin poisoning in horses has not been confirmed based on detection of monensin in tissues or blood. Furthermore, no data has been established in previous investigations as to the most appropriate antemortem or postmortem sample for confirmation of monensin exposure and/or toxicosis. Thus, the current case series describes the discernible toxicological and pathological findings in horses with confirmed exposure and poisoning from monensin, provides recommendations on specimen collection for toxicological testing, and illustrates the limitations of monensin concentrations as prognostic indicators.
Case 1
A group of 25 horses broke into a shed and had access to feed that was supplemented with 800 g/ton (880 µg/g) of monensin. Approximately 6–8 hr later, a 7-year-old American Quarter Horse gelding (horse A) became lethargic and tetraparetic; an irregular heart rate was noted by the veterinarian on physical examination. Clinical biochemistry showed elevations in aspartate aminotransferase, creatine kinase, and creatinine. The horse was treated symptomatically with intravenous fluids, but died 3–4 hr later. A field necropsy revealed epicardial hemorrhages with white and red streaking of the ventricular myocardium. Heart tissue was submitted to the California Animal Health and Food Safety Laboratory System (CAHFS; Davis, California) for histological examination. Minimal pathology was observed. Cardiomyocytes encircled by infiltrating neutrophils where occasionally seen, in addition to degenerate-looking neutrophils expanding the lumens of multiple myocardial vessels. Generalized marked congestion was also noted.
Approximately 24 hr after exposure to the monensin-supplemented feed, 2 more geldings (horses B and C) developed severe cardiac arrhythmias, lethargy, and recumbency. Treatment with intravenous fluids, selenium, vitamin E, flunixin meglumine, and activated charcoal was initiated. In addition, all remaining horses were administered activated charcoal orally 36 and 60 hr postexposure. Horse B was euthanized approximately 48 hr after exposure due to severe clinical deterioration, and heart and liver tissues were submitted to CAHFS for histologic and toxicologic evaluation. Histologically, the heart revealed distinct areas of pallor outlining groups of cardiomyocytes undergoing acute degeneration and necrosis (Fig. 1). Lesions diffusely throughout the liver were consistent with a moderate midzonal vacuolar hepatopathy. The other clinically affected horse (horse C) remained lethargic but started eating and drinking 4 days after exposure and eventually recovered. Another horse (horse D) collapsed suddenly and died 4 days after monensin exposure; no postmortem examination was performed.
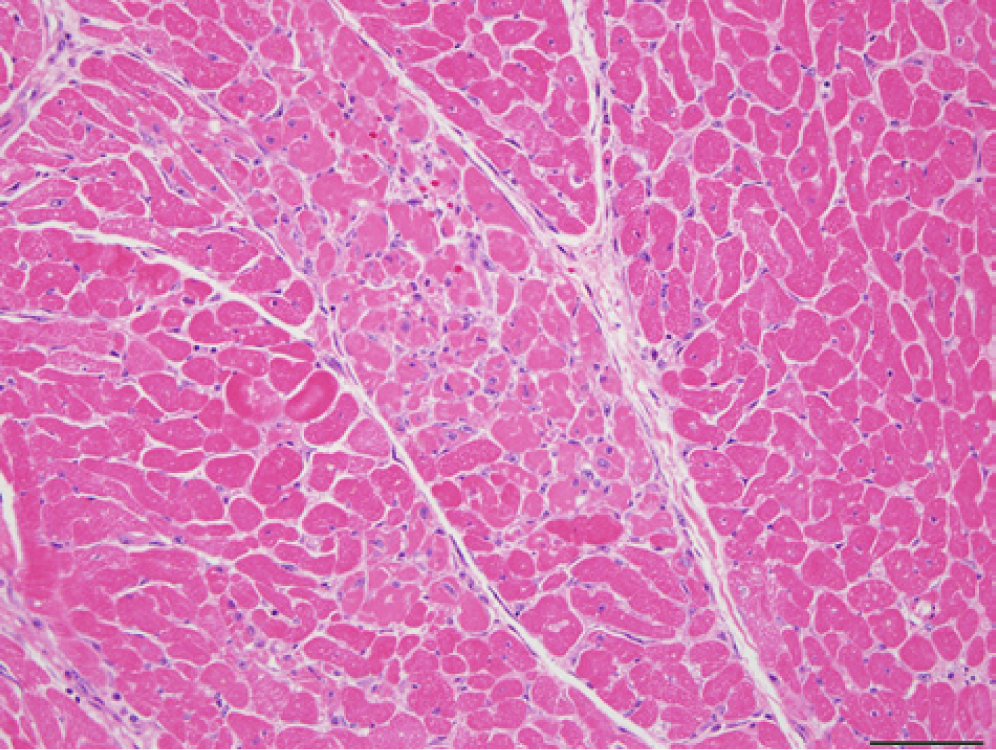
Myocardium; horse B (case 1). Prominent foci of acute necrosis; well-demarcated groups of cardiomyocytes demonstrate loss of cellular detail and cross-striations, with infiltrating stromal cells, histiocytes, and occasional neutrophils. Hematoxylin and eosin. Bar = 50 µm.
Stomach content, heart tissue, and serum from horse A; stomach content, heart tissue, liver tissue, urine, and serum from horse B; and serum from horse D and 2 clinically unaffected horses (horses E and F) were submitted for ionophore analysis. Briefly, 1 g of urine and serum were extracted with ethyl acetate (serum) or methylene chloride (urine). After centrifugation, aliquots of the supernatant were evaporated to dryness under nitrogen and reconstituted in methanol:water (1:1 v/v), filtered through a 0.22-µm filter c and transferred into autosampler vials. All controls and fortified samples were prepared in the same manner. For tissue samples, 3 g were extracted by homogenization with methylene chloride. After centrifugation, aliquots of the supernatant were evaporated to dryness under a gentle nitrogen stream. The residue was reconstituted in 200 µl of methylene chloride and 800 µl of hexane. The reconstituted residue was then subjected to solid phase extraction (SPE). The SPE cartridges d were conditioned with 10 ml of hexane. Extracts were applied to SPE cartridges and filtered gravimetrically. The cartridges were washed with 10 ml of 100% hexane, 10 ml of 20% methylene chloride in hexane, and 10 ml of 100% methylene chloride, discarding all washes. The analyte was eluted with 10 ml of 100% methanol into disposable glass tubes and evaporated to dryness. The residue was reconstituted in 0.5 ml of methanol:water (1:1 v/v), filtered through a 0.22-µm filter, c and then transferred into an autosampler vial. Extracts were analyzed using a triple quadrupole–linear ion trap mass spectrometer b equipped with a high-performance liquid chromatograph a (HPLC). The HPLC separation was performed by a 150 mm, 4.6 mm i.d. 5-µm particle size column e with a mobile phase consisting of 0.1% formic acid in water and 0.1% formic acid in methanol. The injection volume was 20 µl. Mass spectral data was acquired in the positive ion electrospray ionization mode. Tandem mass spectrometry analysis of the precursor ion at m/z 693 was used to identify monensin. Spectra and retention times obtained from sample analyses were compared with those obtained from the analysis of a certified monensin analytical standard. f Quantification was performed using an external, 4-point calibration curve in matching matrix with linear regression. The limits of detection for monensin for the method used were 0.5 ng/ml for serum and urine, 2 ng/g for heart and liver (wet weight), and 0.1 μg/g for stomach contents (wet weight).
Stomach content collected from the 2 horses (horses A and B) that died 12 and 48 hr after exposure contained 1 and 6 µg/g of monensin, respectively, while the heart tissue contained 45 and 5.2 ng/g, respectively. The 5 sera, composed of serum from 2 clinically unaffected (horses E and F) and 3 affected horses (horses A, B, and D), contained between 5.3 and 52 ng/ml of monensin. The single liver and urine samples from horse B contained 2 ng/g and 5.6 ng/ml of monensin, respectively. Table 1 provides a summary of the toxicological findings. Based on the history and the clinical presentation and toxicological findings, a diagnosis of monensin toxicosis was confirmed in horses A, B, and D and monensin exposure in horses E and F.
Monensin concentrations detected in various biologic equine samples following oral exposure.*
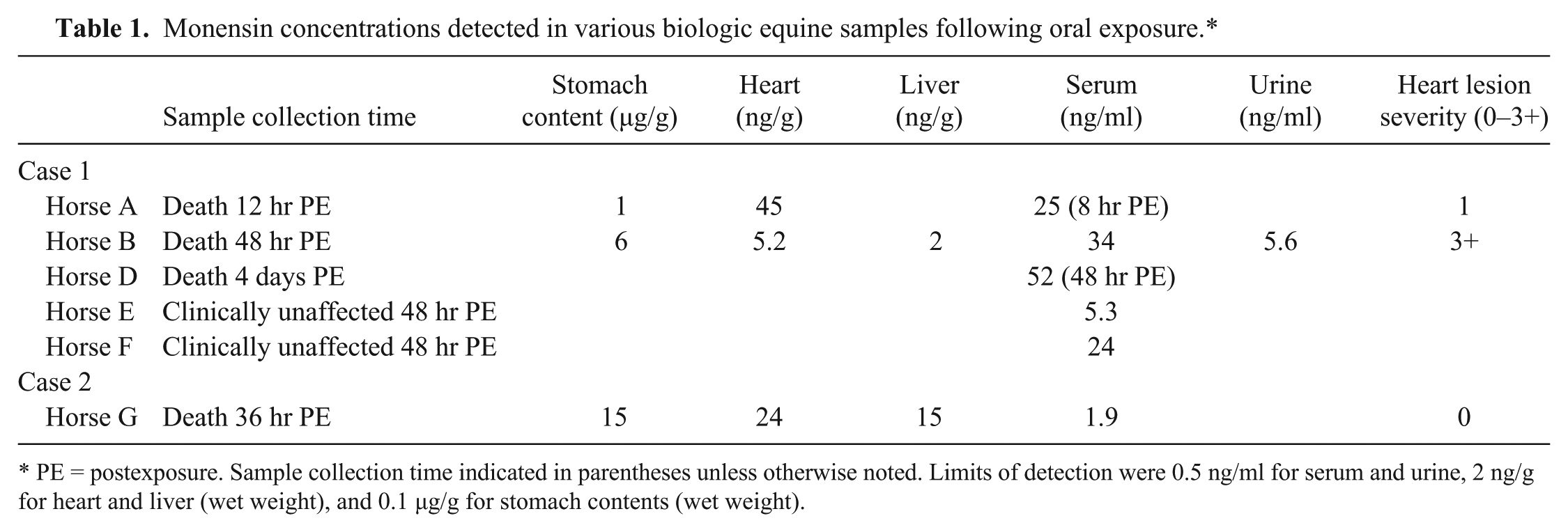
PE = postexposure. Sample collection time indicated in parentheses unless otherwise noted. Limits of detection were 0.5 ng/ml for serum and urine, 2 ng/g for heart and liver (wet weight), and 0.1 µg/g for stomach contents (wet weight).
Case 2
An 8-year-old male, 493-kg American Quarter Horse (horse G) and 2 ponies were placed in a cattle pasture adjoining a dry lot. A high magnesium mineral mix containing 1,600 g/ton (1,760 µg/g) of monensin had been placed in a dry lot feeder 1 month prior. The owner assumed that the cattle had consumed all of the mineral mix. The next afternoon, the owner noticed that the horse was in the dry lot, but no obvious clinical problems were noted. However, the following morning the horse was restless, lying down and getting back up repeatedly, and showing weakness in the hindquarters. The horse was transported to a local veterinary clinic for examination. The horse was in severe respiratory distress with fluid coming from the nostrils and collapsed in the trailer on arrival to the veterinary clinic. The horse was subsequently euthanized that afternoon. The owner realized that evening that the horse might have had access to the mineral mix containing monensin. On checking the feeder in the dry lot, the owner found a large amount of the mineral mix still present.
The horse was submitted to the University of Kentucky Veterinary Diagnostic Laboratory (Lexington, Kentucky) for postmortem examination. The horse was in fair postmortem preservation with good body condition. The mucus membranes were moderately pale, and there was moderate pulmonary edema and congestion. A moderate amount of red-tinged froth was noted within the tracheal lumen and nares. Numerous bot larvae were attached to the margo plicatus of the stomach. No other significant gross lesions were observed. Histological examination revealed variable numbers of eosinophils admixed with proteinaceous fluid within the alveoli and bronchioles. There was mild cytoplasmic vacuolation of hepatocytes, primarily within centrilobular and midzonal regions. Multifocally, there were regions of mild to moderate perivenular fibrosis of central and portal veins with bile duct hyperplasia. Low to moderate numbers of eosinophils and an occasional cross-section of adult nematodes were observed within the intestinal mucosa. The heart, spleen, and kidney were devoid of any significant histological lesions. Stomach content from this horse (horse G), along with portions of heart and liver tissue and heart blood, were submitted for toxicological ionophore testing based on the case history of possible monensin exposure.
Stomach content contained 15 µg/g of monensin approximately 36 hr after exposure. The heart and liver tissues contained 24 and 15 ng/g of monensin, respectively. The heart blood contained 1.9 ng/ml of monensin. Based on the history, clinical presentation, and toxicological findings, a diagnosis of monensin toxicosis was confirmed in this horse. The 2 ponies that had been in the pasture together with horse G did not show any abnormal clinical signs at any time, and no diagnostic testing was performed for either pony.
Diagnostic work-up for possible monensin toxicosis has relied heavily on postmortem histologic findings.18,19 Typically, pathologic evidence of skeletal and cardiac myopathy along with a clinical history of possible or known exposure to monensin is used to confirm toxicosis.8,13,16,17,20 However, several studies have shown individual variations in the severity of cardiac and skeletal muscle pathology, with some horses having no detectable histological changes1,2,14 as shown in the current report. In those cases, diagnosis was made based on clinical signs of tachycardia, ataxia, depression, anorexia, and/or profuse sweating in conjunction with detection of high concentrations in the feed and/or stomach content.1,2,14 In cases in which associated feed cannot be tested for monensin or in cases with no histologic lesions, detection of monensin in postmortem tissues, blood, or serum may aid in diagnosis.
In the present report, monensin was detected in various biological samples. There was a lack of correlation with stomach content monensin concentrations and clinical progression or outcome. Horse A had only 1 µg/g of monensin detected in the stomach content and died acutely (<12 hr) after exposure; in contrast, horse G, which had 15 µg/g of monensin in the stomach content, died after 36 hr. Differences in concentrations measured could have been due to several factors, including variable volumes of ingesta because of dietary differences, individual differences in absorption rate and/or gastric transit times, variation in postmortem sampling strategies for collection of stomach contents, and postmortem redistribution of monensin. 15 Nonetheless, based on this data, stomach content monensin concentrations should be interpreted with caution, but are a reliable tool for confirming monensin exposure. Varying concentrations of monensin were also detected in serum up to 48 hr after exposure in clinically affected and unaffected horses. Horse A died peracutely with a serum concentration of 25 ng/ml in contrast to horse F, which had a similar serum concentration (24 ng/ml) at 48 hr and appeared clinically unaffected and survived. Thus, while serum monensin concentrations do not indicate severity of clinical disease or probable outcome, they can be used antemortem or postmortem to confirm monensin exposure.
There is a lack of data about useful postmortem biological diagnostic specimens in suspect or known monensin exposures in horses. A 2001 case report of accidental lasalocid poisoning in horses used clinical signs, histological cardiac lesions, and detection of lasalocid in the liver tissue of 2 affected horses to confirm the diagnosis of ionophore toxicosis. 5 In oral dosing studies, monensin has been detected in plasma, liver, heart, and gastrointestinal content of horses. 6 Horses that received a LD50 of 2 mg/kg body weight 10 had plasma concentrations of 50–150 ng/ml at 24 hr after dosing; another horse that received 3 mg/kg body weight had a plasma concentration of 200 ng/ml 3.5 hr after dosing and died directly thereafter. 6 One horse in the oral dosing study that died within 24 hr had a liver monensin concentration of 100–200 ng/g. Another horse had no detectable monensin (<50 ng/g) in the liver even though this horse also died. Detected concentrations of monensin in heart tissue were less than 100 ng/g, and concentrations in stomach content ranged from 1 to 2 µg/g. 6
In the veterinary literature, plasma monensin concentrations in horses receiving a LD50 dose of monensin were higher than many of the serum concentrations detected in the 2 cases reported herein, with the exception of horse D (52 ng/ml monensin detected in serum 48 hr postexposure). 6 Horses A and B had serum concentrations well below the 50 ng/ml reported in the dosing study, providing further evidence that serum or plasma monensin concentration cannot be used to accurately determine clinical outcome. In most diagnostic toxicology investigations, accurate information on amount of toxicant ingested is not available. This must be taken into account when interpreting diagnostic test results based on data established in toxicokinetic studies. Concentrations of monensin in stomach content from horses A, B, and D were comparable or higher than previously reported values. 6 In the present report, monensin was detectable in the liver and heart up to 48 hr after exposure. The concentrations detected were indeed lower than those reported in the LD50 dosing study; however, more sensitive methods have been developed and were used to detect monensin in tissues in the present case series (Dick CP, Vessie GH, Moran JW, Coleman M: 1996, The determination of monensin residues in cattle following the administration of two monensin controlled release capsules. In: World Buiatrics Congress, p. 254. Edinburgh, UK).3,11,12 Lower concentrations may have been found in earlier studies had methods with lower detection limits been used. In the present case series report, heart monensin concentrations were consistently higher than those detected in the liver. Therefore, heart tissue may serve as a more useful postmortem diagnostic specimen to confirm exposure especially in cases with no salient histologic lesions. Of notable interest was the finding of detectable concentrations of monensin in urine 48 hr postexposure. In a radio-labeled dosing study, detectable amounts of radioactively labeled monensin were found in the urine up to 96 hr following oral administration of 1 mg/kg body weight of monensin to 2 ponies. 4 Thus, although urine is not the major route for elimination of monensin, it could be used to determine exposure antemortem, especially in cases involving horses with mild or absent clinical signs. The major route of excretion is in bile and elimination in feces.4,6 Although, analysis of bile and feces was not conducted in the reported cases, such specimens could be useful in determining monensin exposure.
The pathologic findings in the present report did not correlate well with detected tissue concentrations of monensin, similar to other case reports.1,2,14 In case 1, horse A had the highest detected monensin concentration (45 ng/g) in the heart, but only mild histologic cardiac changes were noted. In contrast, horse B, which had a much lower concentration (5.2 ng/g) of monensin detected in the heart, had more severe cardiac lesions on histology. In addition, no lesions were noted in case 2 (horse G) even though 24 ng/g of monensin was detected in the heart. Thus, in the absence of cardiac lesions one should not rule out monensin toxicosis and more important, tissue concentrations do not correlate with histological lesions.
The present report is important in that it documents the detection of monensin in biological samples in clinically affected and unaffected horses with known exposure to monensin. In addition, it highlights the difficulty in identifying an appropriate diagnostic work-up of suspected monensin toxicosis cases. There was an overall lack of correlation of monensin concentrations in the various biological samples that were tested with clinical progression or outcome. However, serum, blood, liver tissue, heart tissue, stomach content, and urine can be tested to confirm exposure. More important, the consistently high levels found in heart tissue suggest that this is the most useful diagnostic specimen for postmortem confirmation, especially in cases in which associated feed cannot be tested for monensin or in cases with no histologic lesions.
Footnotes
Acknowledgements
The authors wish to thank Dr. Arthur Sutfin for providing clinical information and Elizabeth Tor for valuable technical assistance.
a.
HPLC Model 1100, Agilent Technologies, Santa Clara, CA.
b.
4000 Q Trap Mass spectrometer, Applied Biosystems/MDS Sciex, Concord, CA.
c.
0.22 µM Millex-EIMF 13 mm diameter, PES membrane filter, EMD Millipore, Billerica, MA.
d.
Sep-pak Vac 6 cc (1 g) Silica cartridges, Waters Corp., Milford, MA.
e.
Luna 5 µm C18(2) 100 Å, LC Column 150 x 4.6 mm, Phenomenex, Torrance, CA.
f.
Monensin sodium salt, Sigma-Aldrich, St. Louis, MO.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.