
Abstract
A 3-year-old female spayed domestic ferret (Mustela putorius furo) was presented for evaluation of severely increased liver enzyme activities noted prior to anesthesia. The ferret showed no clinical signs of liver or gall bladder disease. Serum biochemical profile confirmed elevations in alanine aminotransferase and alkaline phosphatase activity and total bilirubin concentration. Abdominal ultrasound revealed a distended and convoluted common bile duct although no obstruction was seen. Upon exploratory laparotomy, a large amount of sediment was found within the bile duct that appeared to be obstructing it, but no other cause for the obstruction was found. A choledochoduodenostomy was performed, and the ferret recovered uneventfully from surgery. Liver enzyme activities returned to normal by 5 days post-operatively. Biopsy and culture results yielded no definitive cause of the bile duct obstruction. Cholestasis is a rarely reported disease in ferrets and generally has been described in connection with neoplasia or parasitism, neither of which was found in the current case.
A 3-year-old female spayed ferret (Mustela putorius furo) weighing 0.744 kg had been examined by the referring veterinarian 3 weeks earlier for a crusted mass on digit 3 of the right rear paw. Antibiotic therapy with an unknown antibiotic was started, but after a week, the mass remained unchanged and surgery was recommended to remove it. A pre-anesthetic biochemical profile revealed significant increases in serum alanine aminotransferase (ALT; >1,000, reference [ref.] interval: 82–289 IU/l) and gamma-glutamyl transferase (GGT; 97 U/l, ref. interval: 0–5 IU/l) activities, and total bilirubin (2.7 mg/dl, ref. range: <1.0 mg/dl) concentration. The ferret was referred to Oklahoma State University Center for Veterinary Health Sciences (Stillwater, Oklahoma) for further evaluation.
On presentation, the ferret was bright and alert with normal temperature, pulse, and respiration rates, and pink mucous membranes. Body condition was also normal. The ferret’s diet consisted mainly of pelletized ferret food, a and she was kept in a multi-level cage with 6 other ferrets. The owners reported that the ferret’s appetite and activity levels were normal and that there were no abnormalities in urination or defecation. Abnormalities on physical examination included crusty, ulcerated lesions on multiple digits of all paws except the left front. An apparent pain response was also elicited on abdominal palpation over the cranial abdomen. Otherwise, the physical examination was unremarkable.
Blood was obtained from the right jugular vein for a complete blood cell count (CBC) and serum biochemical profile. The CBC results were within reference intervals, and the biochemical profile revealed increased ALT (974 IU/l) and ALP activities (361 IU/l, ref. interval: 30–120 IU/l), total bilirubin (6.2 mg/dl, ref. interval: <1), and cholesterol (458 mg/dl, ref. interval: 64–296 mg/dl). Anesthesia was induced and maintained using 2–3% isoflurane b in 100% oxygen administered with a precision vaporizer using a non-rebreathing system and facemask abdominal radiographs and ultrasound. Abdominal radiographs revealed no significant abnormalities. Abdominal ultrasound revealed an enlarged liver with overall echotexture and a markedly dilated and tortuous bile duct with a moderately distended normal gallbladder (Fig. 1). The bile duct measured from 0.27 cm to 0.55 cm in diameter on ultrasound. Sediment and flocculent material could be seen within the bile. The kidneys revealed poor corticomedullary definition with an incidental cortical cyst in the right kidney and possible mild right adrenal enlargement. No specific cause for the bile duct dilation could be determined by ultrasound.
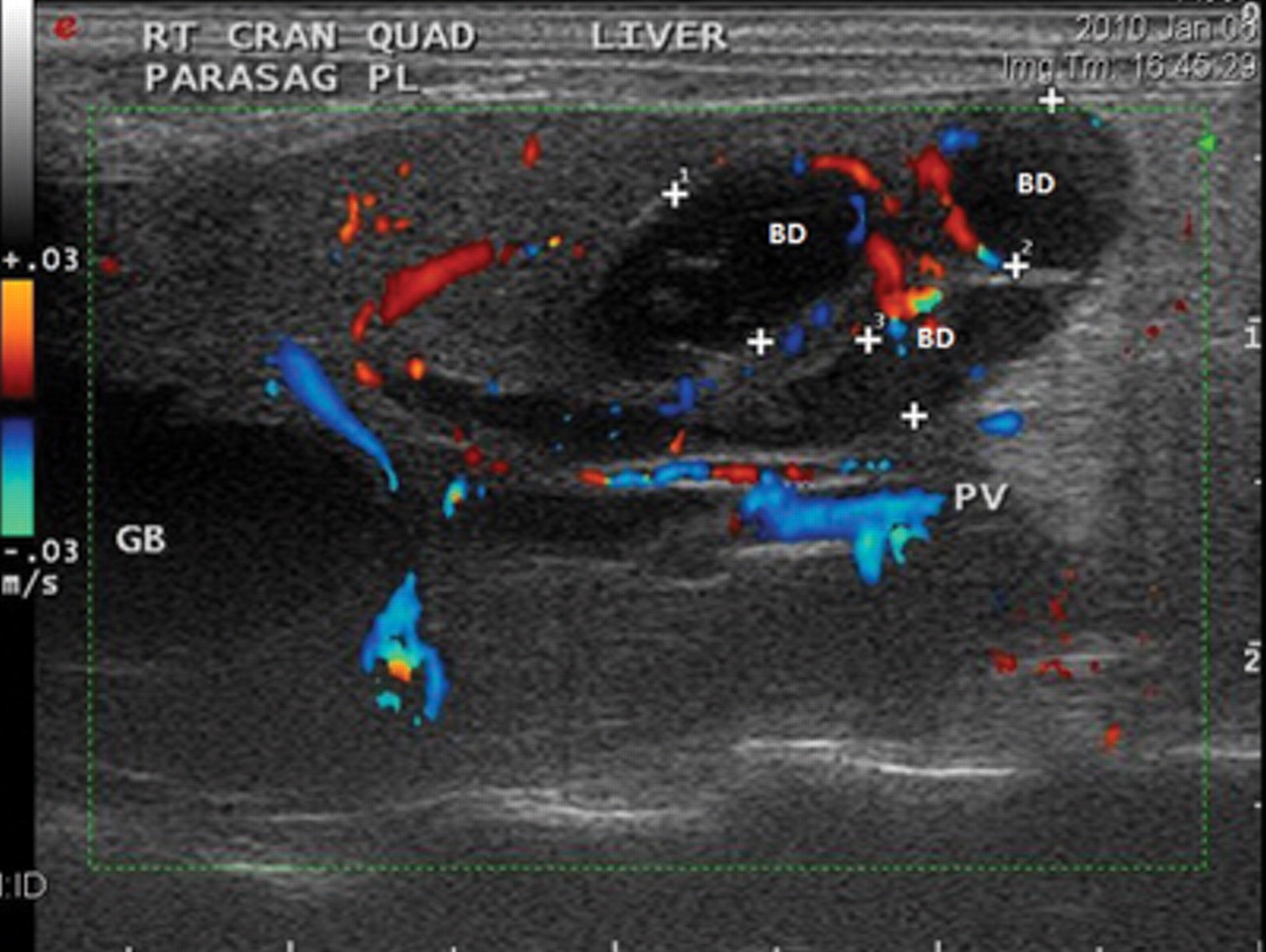
Right parasaggital 2-dimensional abdominal ultrasound view demonstrating the dilated and tortuous common bile duct (BD) and moderately distended gallbladder (GB) in a domestic ferret (Mustela putorius furo). PV = portal vein.
Cholestasis of undetermined cause was presumptively diagnosed in the ferret. Although the ferret exhibited no clinical signs of liver or gall bladder disease despite the biochemical profile abnormalities, an intravenous catheter was placed in the right jugular vein and the ferret was started on maintenance fluids c at 60 ml/kg/day for diuresis. A diet of prescription food specifically for patients with liver disorders d was instituted, and exploratory laparotomy was scheduled for the following day.
The ferret was held off food for 6 hr, and anesthesia was induced e (4.4 mg). The ferret was intubated and maintained at a surgical plane of anesthesia with isoflurane gas at 2–4% administered in 100% oxygen with precision by a non-rebreathing system. Celiotomy revealed a grossly dilated bile duct (Fig. 2) containing large amounts of sediment. The gallbladder could not be expressed, and the bile duct was resected and a choledochoduodenostomy was performed (Fig. 3). Tissue samples of bile duct, duodenum, stomach, mesenteric lymph node, and liver were placed in 10% buffered formalin and submitted for histologic evaluation. Sample of the sediment and bile from the bile duct and gall bladder were submitted for aerobic and anaerobic cultures. The pancreas and adrenal glands appeared grossly normal so no samples of these tissues were submitted. The ferret recovered from anesthesia uneventfully and was maintained on intravenous fluids c (with 2.5% dextrose added) at 60 ml/kg/day and given buprenorphine f subcutaneously at 0.03 mg/kg every 6 hr for pain.
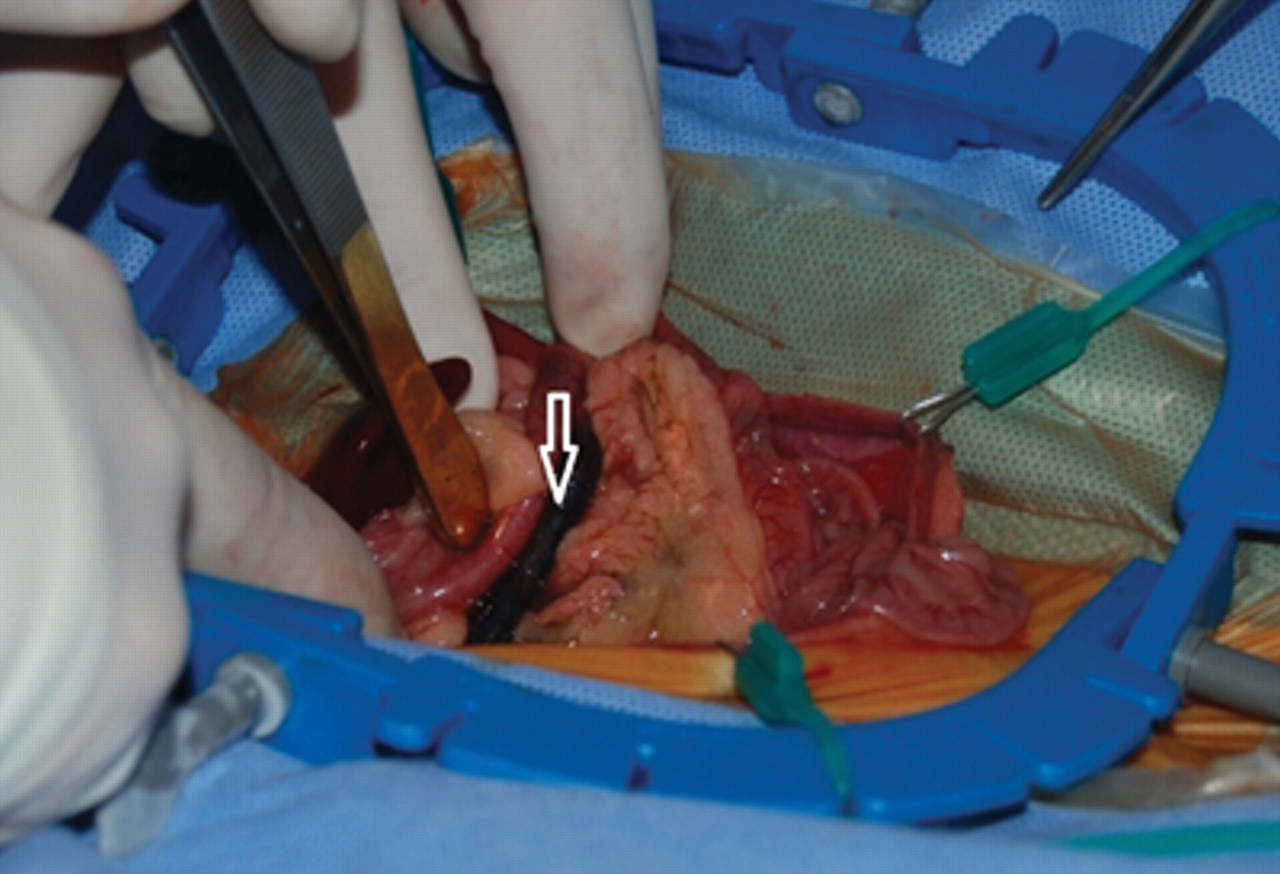
View at ventral celiotomy showing the markedly distended common bile duct (arrow) in a domestic ferret (Mustela putorius furo). The bile duct diameter is nearly equal to the adjacent small intestine.
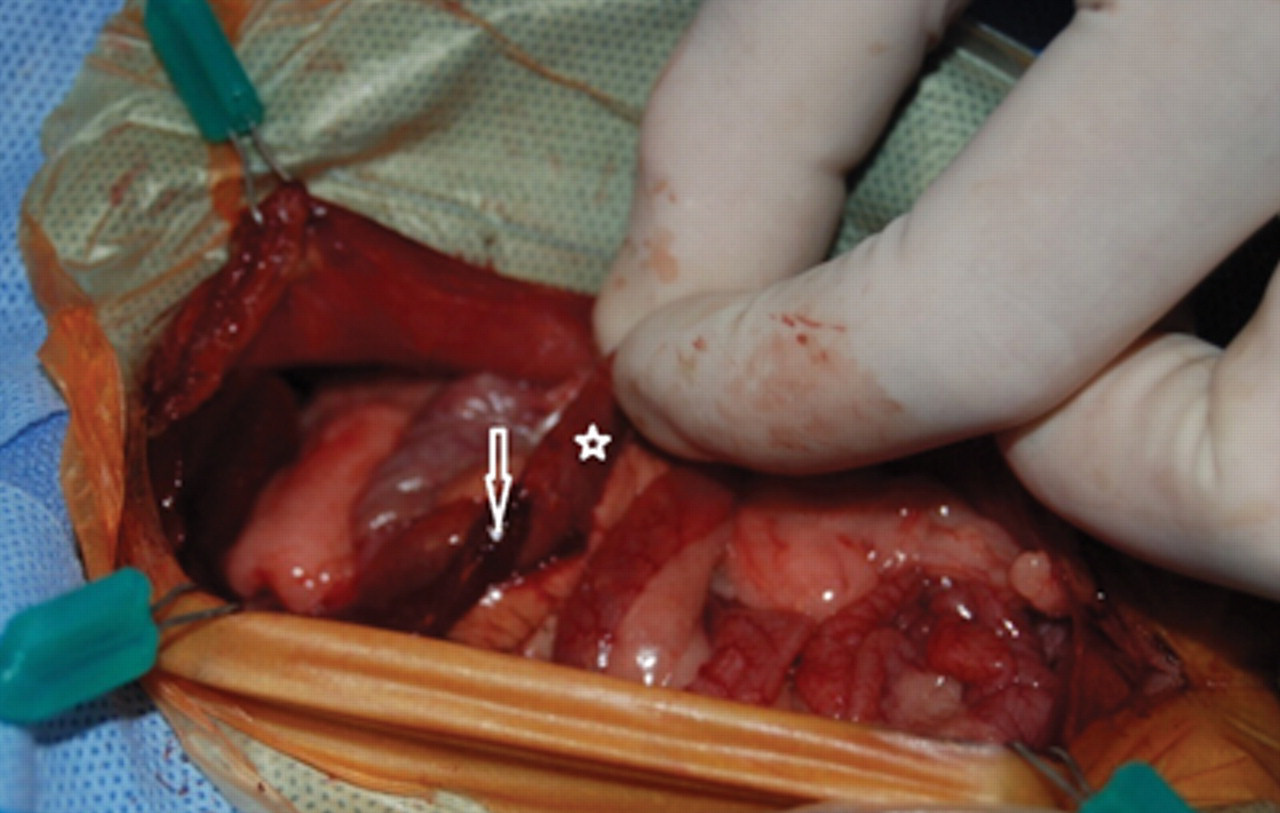
View at ventral celiotomy showing resected common bile duct (arrow) and duodenum (star) in a domestic ferret (Mustela putorius furo) after completion of choledochoduodenostomy.
The first day post-operatively, the ferret was lethargic and unwilling to eat on its own although she appeared to be fully recovered from anesthesia. A blood sample was collected from the left lateral saphenous vein and submitted for follow-up CBC and serum biochemical profile. The CBC was again unremarkable, and the serum biochemical profile revealed decreases in ALT (476 IU/l) and ALP (122 IU/l) activities, and total bilirubin (2.0 mg/dl) concentration. The serum glucose concentration was 74 mg/dl (ref. interval: 63–134 mg/dl). Treatment for pain control was initiated with meloxicam g orally at 0.1 mg/kg every 24 hr, and buprenorphine was decreased to every 8 hr. The ferret became more active throughout the day and a diet of recovery food designed for carnivores that are unwilling to eat their normal diet h when instituted. The postprandial glucose concentration increased to 156 mg/dl. The intravenous 2.5% dextrose-containing solution was discontinued, and the ferret was maintained on fluids c at 2.5 ml/hr for continued diuresis. Two days post-operatively, the ferret was bright, alert, and eating well on her own. Intravenous fluids were discontinued, and the jugular catheter was removed. Five days post-operatively, the surgical incision was healing well, and the ferret was dismissed from the hospital with meloxicam at 0.1 mg/kg orally every 24 hr for an additional 7 days until suture removal. Unfortunately, the owners did not return the ferret for suture removal, and all attempts to contact the owners were unsuccessful.
Histologic examinations of tissues submitted revealed biliary hyperplasia characterized by a convoluted mucosal surface with markedly hyperplasic epithelium of the common bile duct; random hepatic necrosis with neutrophilic inflammation comprised of small foci of inflammatory cells randomly scattered throughout the section of liver; mild lymphoid hyperplasia; and normal stomach and duodenum. There was no growth of aerobic or anaerobic bacteria on cultures of the bile and sediment. Based on these results, an inciting cause of the ferret’s cholelithiasis with cholestasis could not be determined.
In human beings, alcoholism and morbid obesity may result in primary hepatopathies, but in animals, primary hepatopathies are uncommon. This appears to be true for ferrets as well. 3 Neoplasms are one of the reported causes of primary hepatopathies with the most common neoplasia being lymphoma. Other hepatic neoplasias include hemangiosarcoma, adenocarcinoma, and hepatocellular adenoma. 1 Metastatic neoplasias are more common and often due to adrenal cortical adenocarcinomas or lymphoma originating from other sites. 5 Reported causes of primary liver and biliary disease in domestic and black-footed ferrets (Mustela nigripes) include neoplasia 3 and parasites. 1 Biliary adenoma, adenocarcinoma, cystadenoma, and cystadenocarcinoma have all been documented in the domestic ferret. 1 In a retrospective study of a captive population of black-footed ferrets, biliary cystadenoma or carcinoma were some of the most common neoplasms. The unusually high prevalence of this neoplasm was thought to be secondary to the common occurrence of intrahepatic biliary cysts in that population. 4
Most hepatopathies in animals are secondary to preceding or concurrent conditions. Chronic lymphocytic portal hepatitis has been seen and is thought to be related to chronic inflammation such as inflammatory bowel disease (IBD). 5 Suppurative hepatitis is also thought to be related to IBD. 5 Vacuolar hepatopathy is associated with endocrinopathies such as hyperadrenocorticism but may also be found in association with administration of corticosteroids; however, this is rare in ferrets. 5 Hepatic lipidosis has been found in association with long-term anorexia in cats and ferrets. 5
Elevations in ALT, and often GGT, activities most commonly occur in ferrets with liver disease while increased ALP activity is uncommon and increased total bilirubin concentration is very rare. 3 Ferrets clear bilirubin efficiently via the kidneys and often will have bilirubinuria when serum bilirubin concentration is within the reference interval. 5 Elevated total bilirubin concentration may occur with severe suppurative or neoplastic hepatic disease, or hemolysis. In the ferret in the current study, the elevations in ALP activity and total bilirubin concentration suggested biliary pathology and/or obstruction. Primary cholestasis has rarely been reported in ferrets. Since the ALT activity was also increased, liver hepatocellular disease could not be excluded.
The authors find it interesting that the ferret in the present report had a complete lack of clinical signs associated with this disease. The only clinical abnormality seen was the minor crusty lesions on the paws. The origin of these lesions was not determined. Possibilities include trauma with secondary bacterial infection, allergic dermatitis, or a neoplastic process, although none are common in ferrets. Only by performing pre-anesthetic laboratory testing (which revealed increases in total bilirubin concentration, ALP activity, and ALT activity that were repeatable findings over approximately 1-weeks’ time) was a problem detected. Further investigation by ultrasound revealed a severely distended bile duct, which and was considered to be the source of these biochemical abnormalities. Although the ferret continued to eat well, it was started on intravenous fluids and a liver protective diet prophylactically prior to surgery. Exploratory laparotomy performed the following day may have relieved the obstructed bile duct before clinical signs developed.
In domestic ferrets, biliary and hepatic disease has been associated with several conditions: cystic mucinous hyperplasia and papillary hyperplasia of the gallbladder mucosa with the formation of discrete mural mucinous cysts, 6 Aleutian mink disease virus infection in mink (Neovison vison) and ferrets causing bile duct dilatation and proliferation in the liver, 7 coccidiosis extending to the bile duct, 8 and chronic cholangiohepatitis in a group of cohabitating ferrets infected with an argyrophilic bacteria similar to several species of Helicobacter. 2 Biliary cysts and cystadenomas in both domestic and black-footed ferrets rarely result in clinical hepatopathy and generally are incidental findings during laparotomy or at necropsy. 5
At celiotomy, only the severely dilated common bile duct appeared to be affected, and the gall bladder was very difficult to express indicating obstructive disease. Histologically, there was only generalized biliary hyperplasia without mucinous cyst formation. Findings consistent with Aleutian disease of hypergammaglobulinemia, plasmacytic-lymphocytic infiltration in multiple organs, or global membranous glomerulonephropathy and vasculitis were absent. Parasites including the life stages of a coccidian parasite in the epithelium of the hepatic bile ducts or gallbladder epithelium were absent. No evidence of bacteria could be found on either histologic examination or culture. Although the ferret in the current study had increases in both ALT and GGT activities, biliary cysts were ruled out on visual inspection of the gall bladder during laparotomy. Liver biopsies did yield mild but inconclusive inflammatory liver changes on histologic examination that consisted of small foci scattered randomly throughout the liver tissue. Cultures were negative, and these lesions were not severe enough to cause blockage of the bile ducts.
Cholelithiasis causing cholestasis has not been previously reported in the ferret and is an uncommon disease in dogs and cats. 9 In veterinary medicine, causes for this cholelithiasis are not well understood. Diet could potentially play a role; however, the ferret in the present study consumed a common commercial ferret food that has had no reports provoking liver diseases in ferrets. There was a large amount of sediment in the gallbladder and dilated bile duct. While the particles were not large enough to block the bile duct, an accumulation of a large amount of this sediment in the duct could potentially have caused the obstruction.
In the ferret in the current study, reported causes of primary liver and biliary disease from neoplasia 3 or parasites 1 were ruled out. Only biliary hyperplasia was seen on histologic examination with no indication of any neoplastic process. This ferret remained asymptomatic and never developed icterus and this may be due to ferrets’ ability to eliminate conjugated bilirubin through the kidneys. 5 No preceding or concurrent associated conditions were found to explain the severe bile duct dilation and cholestasis. While the definitive cause for the bile duct obstruction in this ferret remains undetermined post-operatively, the ferret’s blood and biochemical test results had returned to reference intervals.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Barh and Dr. Rochet for their assistance in this case and for providing the images used in this article.
a.
Marshall Farms, Marshall Pet Products Inc., Wolcott, NY.
b.
Isoflurane, MWI Veterinary Supply Inc., Meridian, ID.
c.
Normasol-R, Hospira Inc., Lake Forest, IL.
d.
L/D, Hills Pet Nutrition Inc., Topeka, KS.
e.
Propofol, Abbott Laboratories, Abbott Park, IL.
f.
Buprenorphine/Buprenex, Hospira Inc., Lake Forest, IL.
g.
Meloxicam/Metacam, Boehringer Ingelheim Vetmedica Inc., St. Joseph, MO.
h.
Oxbow Critical Care, Oxbow Enterprises Inc., Murdock, NE.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding for the publication of this article was provided by Oklahoma State University Center for Veterinary Health Sciences.