
Abstract
Renal papillary necrosis was diagnosed during postmortem examination of a juvenile white-tailed deer (Odocoileus virginianus) from Oklahoma. The deer was surgically treated for a Salter Harris type II fracture of the proximal tibia of the left hind limb. The animal was administered multiple nonsteroidal anti-inflammatory drugs (NSAIDs), including meloxicam, flunixin meglumine, and ketoprofen for pain management. At postmortem examination, gross lesions included a proximal tibial Salter Harris type II fracture with an associated fibrinonecrotizing myositis and bilateral renal papillary necrosis. Histologically, the kidneys exhibited coagulation necrosis of the renal medulla and renal papilla, thrombosis of renal blood vessels, and interstitial medullary edema. The gross and microscopic lesion coupled with the clinical history of multiple NSAID administration suggests NSAID-induced renal papillary necrosis.
A juvenile, 9.6-kg, female white-tailed deer (Odocoileus virginianus) was presented to Oklahoma State University Boren Veterinary Medical Teaching Hospital (Stillwater, Oklahoma) for suspected vehicle trauma. On admission, the deer had a heart rate of 168 beats/min, showed signs of discomfort, and was mildly dehydrated. Physical examination indicated a fracture of the left hind limb, and radiographs confirmed a Salter Harris type II fracture of the proximal tibia. The left hind limb was bandaged, and the animal was given a single intravenous dose of 2.2 mg/kg of ketoprofen. a
The following day, the animal was in pain, and surgical repair of the fracture was performed. The left hind limb was aseptically prepared according to standard hospital procedure. A 10-cm incision was made over the medial aspect of the proximal tibia centered over the fracture site. Open reduction of the fracture was performed, and the fracture was stabilized with the use of a cross-pinning technique with Kirschner wires. After pin placement, the fracture was deemed to be stabilized by manual manipulation of the fracture site. The subcutaneous tissues were sutured in a simple continuous pattern with 3-0 PDS* II. b The skin was then closed with 3-0 nylon suture material b in a cruciate pattern. Postoperative radiographs revealed that the pin placement was satisfactory, and the fracture was reduced. Recovery from anesthesia was uneventful.
Postoperatively, the deer was given a single intravenous dose of 1.1 mg/kg of flunixin meglumine c and a constant-rate infusion of 3.0 μg/kg of fentanyl per hour b ; the fentanyl was discontinued the next day. Additional pain medications administered to the deer for the 2 days after surgery included 1 daily oral dose of 0.2 mg/kg of meloxicam d and multiple subcutaneous doses of 0.3 mg/kg of morphine. d Various drugs were given for pain management in this case because of the availability of drugs and changes in administration route, depending on the stress level of the animal. The deer did not show any clinical signs of improvement postoperatively. The patient remained anorexic and lethargic and eventually became obtunded. The animal was humanely euthanized given the poor prognosis for recovery and submitted for postmortem examination.
Significant postmortem examination findings were limited to the kidneys and the left hind limb. Both kidneys were slightly enlarged and had a smooth capsular surface. On sagittal section, bilaterally well-demarcated foci of medullary and papillary necrosis appeared yellow to orange and occupied more than 75% of the right renal medulla (Fig. 1) and 25% of the left renal medulla. Lesions of the left hind limb included a Salter Harris type II fracture of the proximal tibia with edema, hemorrhage, and necrosis of the surrounding connective tissue.
A set of tissues (brain, lung, heart, spleen, liver, kidney, skeletal muscle, and bone from the fracture site) were collected and fixed in 10% buffered neutral formalin for histologic examination. Formalin-fixed tissues were processed routinely, sectioned at 4 μm, and stained with hematoxylin and eosin. Bone was decalcified before processing.
Histologic examination was performed, and lesions were observed in both kidneys and at the tibial fracture site. The normal renal medullary architecture of both kidneys was disrupted by coagulation necrosis of the inner renal medulla and renal papilla (Figs. 2, 3). Ghosts of the medullary tubules were identified. There was a rim of intense congestion of the renal blood vessels at the margin of the necrotic and viable renal parenchyma. Multiple small-caliber renal blood vessels that contained secondary thrombi were located within, and restricted to, the necrotic tissue. A mild to moderate number of neutrophils were within the regions of necrosis, with moderate interstitial medullary edema.

Deer (Odocoileus virginianus) kidney. Section of kidney showing a large area of necrosis extending from the renal pelvis to the central medulla (arrows).
Multifocal degeneration, necrosis, and mineralization of myocytes of the musculature adjacent to the fracture site were observed. The interstitium was moderately edematous, contained a moderate amount of fibrin, and had a moderate accumulation of neutrophils, macrophages, and lymphocytes. Decalcified sections of bone revealed a minimal amount of periosteal proliferation. All other tissues examined were within normal limits. The clinical history and postmortem examination findings of the present case are supportive of the diagnosis of nonsteroidal anti-inflammatory drug—induced renal papillary necrosis.
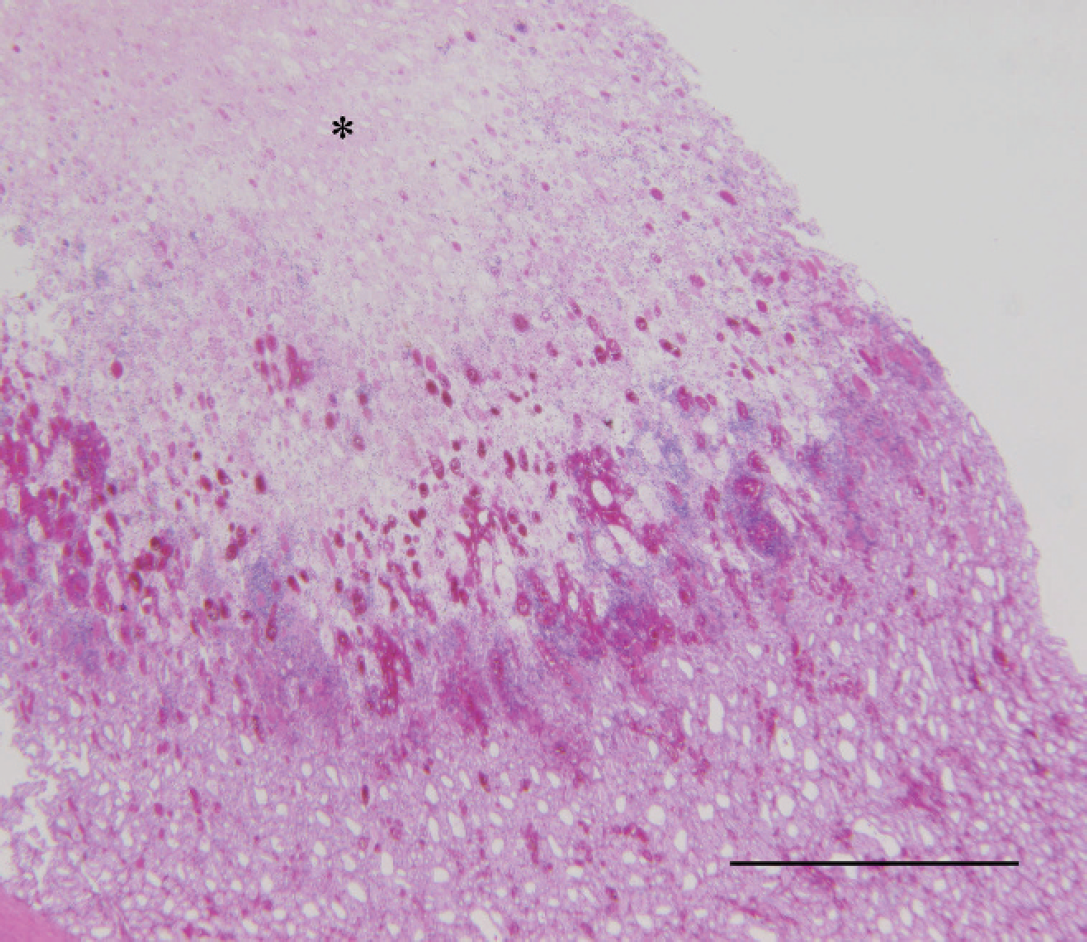
Deer (Odocoileus virginianus) kidney. Photomicrograph of kidney showing locally extensive necrosis involving the renal medulla (asterisk). Hematoxylin and eosin. Bar = 200 μm.
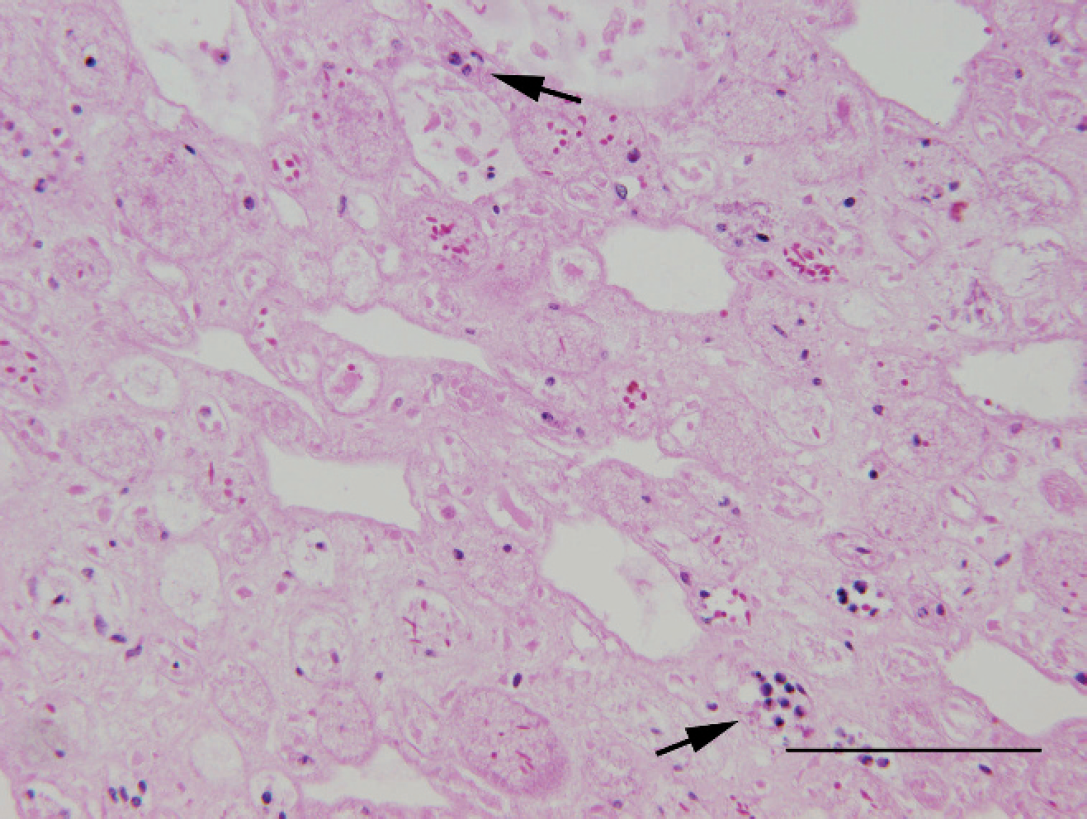
Deer (Odocoileus virginianus) kidney. Photomicrograph of the kidney showing the renal medulla showing ghosts of medullary tubules with accumulation of interstitial medullary polymorphonuclear cells (arrows). Hematoxylin and eosin. Bar = 50 μm.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used analgesic drugs in human and veterinary medicine. The principle therapeutic effect of NSAIDs, whether inhibiting both cyclooxygenase (COX)-1 and COX-2 enzymes or selectively inhibiting the COX-2 enzyme, is to inhibit the production of prostaglandins to interrupt the inflammatory cascade. 1,4 In veterinary medicine, adverse affects associated with NSAID administration include gastrointestinal ulceration, renal toxicity, hepatotoxicity, and platelet dysfunction. 4 In humans, analgesic nephropathy is a condition caused by excessive intake of NSAIDs, which results in renal papillary necrosis with a secondary chronic tubulointerstitial nephritis due to inhibition of urine flow. 2 A similar condition called NSAID-induced renal papillary necrosis has been reported in veterinary medicine either naturally or experimentally. 5,6,9,14,17 Patients predisposed to NSAID-induced renal papillary necrosis include patients in hypovolemic states (dehydration or shock); patients receiving nephrotoxic or nephroactive drugs; and patients with renal, hepatic, or cardiac disease. 4
Renal papillary necrosis by NSAID administration is a commonly reported side effect in horses administered phenylbutazone 6,14 and has also been reported in dogs 9,17 and Syrian hamsters. 5 Other NSAIDs associated with renal papillary necrosis include phenylbutazone, 6,14 deracoxib, 15 piroxicam, 4 and mefenamic acid. 5 Flunixin meglumine administered in combination with methoxyflurane has resulted in medullary tubular necrosis in several dogs. 9 Medullary interstitial cells are the primary target of various NSAIDs, which have a major role in the synthesis of prostaglandins. 13 The result of administration of excessive amounts of NSAIDs is a decrease in the synthesis of prostaglandins such as prostaglandin (PG)E2 and PGI2 by the inhibition of cyclooxygenase. Renal prostaglandins such as PGE2 and PGI2 are important mediators of vasodilation during periods of renal hypoperfusion, 16 and these prostaglandins modulate the vasoconstrictor effects of angiotensin II, vasopressin, and norepinephrine. 3 Decreased synthesis of the renal prostaglandins results in a loss of vasodilatory effect on vascular smooth muscle, 3 which reduces the normal medullary blood flow and results in ischemia and renal papillary necrosis. 13
Renal papillary necrosis can also result from reduced blood flow in the vasa recta because of glomerular amyloidosis or compression of the vasa recta because of interstitial fibrosis. 13 Other causes include interstitial renal medullary amyloidosis or pyelonephritis. 10,13 Extrarenal renal disease such as calculi or lower urinary tract obstruction could also result in papillary necrosis. 10,13 Renal papillary necrosis has also been associated with periods of dehydration. 7,11
In the current case, the diagnosis of renal papillary necrosis was based on multiple clinical and postmortem examination findings. The deer had a clinical history of administration of multiple NSAIDs, including flunixin meglumine, ketoprofen, and meloxicam for pain management. No calculi formation, other renal disease, or urinary tract obstruction was evident on gross or histopathologic examination, thus ruling out other potential secondary causes of renal papillary necrosis. The significance of the initial dehydration of this animal is not known, and it could have played a role in the pathogenesis of the papillary necrosis. Another possible cause for the renal lesions in the present case could have been associated with possible capture myopathy, as this animal was captured by a good Samaritan; however, reported lesions in cases of capture myopathy include myoglobinuria, renal tubular necrosis, glomerular degeneration, and necrosis in association with a monophasic multifocal myositis, 8,12,13 of which none were identified in this animal. On the basis of the clinical history and pathologic lesions in the deer, it was speculated that NSAID administration caused a marked decrease in synthesis of renal prostaglandins, ultimately resulting in renal papillary necrosis. Given that multiple NSAIDs were administered to this animal, it was not possible to associate the renal papillary necrosis with a specific drug. To the authors' knowledge, NSAID-induced renal papillary necrosis has not been previously reported in white-tailed deer.
Acknowledgements The authors thank Mr. Curtis Andrew and the Oklahoma Animal Disease Diagnostic Laboratory histotechnologists for their technical assistance. The authors also thank Dr. John Gilliam, Jill Murray, and the students of the Zoo, Exotic, and Wildlife Medicine Service for their great efforts in the surgical management and medical care of this animal.
Footnotes
a.
Fort Dodge Animal Health, Fort Dodge, IA.
b.
Novartis Animal Health, Greensboro, NC.
c.
Intervet/Schering-Plough Animal Health, Kenilworth, NJ.
d.
Baxter Healthcare Corporation, Deerfield, IL.