
Abstract
A postpartum mare and foal were presented for evaluation of fever and lethargy in the mare. The mare was diagnosed with endometritis and initially responded well to treatment. On the second day of hospitalization, the mare developed renal insufficiency characterized by oliguria, azotemia, hemolysis, and thrombocytopenia. Concurrently, the foal developed rapidly progressive central nervous system signs culminating in refractory seizures. Both animals failed to respond to treatment and were euthanized. Thrombotic microangiopathy involving glomeruli was evident on microscopic examination of the mare's kidneys. Microscopic evidence of brain edema was the principal postmortem finding in the foal. No specific etiology was confirmed in either case. Notably, Escherichia coli 0103:H2 was isolated from the mare's uterus and the gastrointestinal tracts of both animals. To the authors' knowledge, this is the first report in which an organism implicated as a cause of hemolytic-uremic syndrome was isolated from an animal with clinical signs and postmortem findings consistent with the disease.
Thrombotic microangiopathy (TMA) is characterized by thrombocytopenia, microangiopathic hemolysis, and organ ischemia resulting from platelet thrombosis within the arterial microvasculature and capillaries. 4,8,13 The kidneys and brain are most prominently affected, and acute renal failure and/or neurologic signs are the predominant clinical manifestations. Hemolytic-uremic syndrome (HUS) and thrombotic thrombocytopenic purpura (TTP) are the renal and neurologic forms, respectively, of TMA described in the human literature. Hemolytic-uremic syndrome occurs most commonly in children as a postdiarrheal complication of enteritis caused by Escherichia coli 0157 and other Shiga toxin-producing E. coli (STEC). Thrombotic thrombocytopenic purpura is considered a systemic TMA with prominent neurologic manifestations, and it is attributable to immune-mediated, heritable, viral, and toxic origins. In veterinary medicine, edema disease of weanling pigs is a systemic TMA caused by specific strains of STEC and characterized by central nervous system dysfunction. 10
Reports of naturally occurring conditions compatible with HUS appear infrequently in the veterinary literature and include several cases in dogs with gastroenteritis, three horses, and a postpartum cow. 3,7,9,12 This report describes a syndrome of acute oliguric renal insufficiency, hemolysis, and thrombocytopenia that developed in a postpartum mare subsequent to treatment for endometritis. Thrombotic microangiopathy involving the kidneys was identified on postmortem examination, and E. coli 0103:H2 carrying the gene for Shiga toxin-1 (Stx1) was isolated from the uterus and gastrointestinal tract. To the authors' knowledge, this report is the first in which an E. coli strain associated with HUS was isolated from an animal with spontaneous clinical signs and pathologic lesions consistent with HUS.
An 8-year-old American Paint Horse mare and neonatal colt were presented for evaluation after the mare experienced lethargy and fever for approximately 24 hr. The mare had given birth 36 hr before admission: the gestational period and parturition were reported as uneventful, the foal was seen to nurse vigorously after parturition, and there were no reported signs of systemic illness in the foal since birth. The mare had clinical signs and laboratory abnormalities consistent with endotoxemia, including depression, fever (39.1°C), injected mucous membranes, mild diarrhea, marked leukopenia with a degenerative left shift, acidosis, and slight elevations in hepatic enzyme activities. There was a hemorrhagic vaginal discharge, the uterus was firm and fluid filled, and uterine lavage yielded a dark, sanguineous fluid containing flocculent debris; these signs indicated a clinical diagnosis of endometritis. Examination of the foal revealed a strong, vigorous, apparently healthy neonate. The vital signs and complete blood count were within normal limits, and semiquantitative IgG testing indicated that the foal had received adequate passive transfer of maternal antibodies.
The mare was treated with intravenous fluids, potassium penicillin, gentamicin, and flunixin meglumine. The clinical signs of endotoxemia subsided, and the mare's attitude and appetite improved substantially over the next 24 hr. Thirty-six hours after admission to the hospital, however, the mare began exhibiting stranguria and passing small amounts of blood-tinged urine. Clinical pathology data indicated a systemic inflammatory response characterized by a left shift in the leukogram, hyperfibrinogenemia, thrombocytopenia, and azotemia. Gross hemolysis was evident in the plasma, and the urine test strip indicated hemoglobinuria (3+). Microscopic hematuria (5–10 red blood cells/high-powered field [hpf]) and granular tubular casts (2–3/hpf) were observed in the urine sediment. Despite aggressive treatment with intravenous fluids and diuretics, the oliguria persisted, the azotemia worsened, heart and respiratory rates increased progressively, and mental status deteriorated. The mare was euthanized approximately 12 hr after treatment for the renal dysfunction was initiated.
Coincident with the clinical deterioration of the mare, the foal became lethargic and suckling activity was reduced. Vital signs were within normal limits, but the oral mucous membranes appeared mildly injected. Clinical laboratory testing showed moderate toxic changes in the peripheral neutrophils, lymphopenia, and mild azotemia. Treatment was initiated with intravenous fluids, dextrose, plasma, broad-spectrum antibiotics, and corticosteroids. The foal produced adequate volumes of urine in response to fluid therapy, and the urinalysis was within normal limits. However, central nervous system dysfunction became evident with disorientation and generalized motor dysfunction. Over time, the foal became increasingly tachycardie, and the neurologic signs progressed rapidly to recumbence and nonresponsiveness, eventually culminating in generalized seizures that were refractory to anticonvulsant drugs. The foal was euthanized approximately 12 hr after clinical signs were first noted.
Complete postmortem examinations were conducted on both the mare and colt within 12 hr and 6 hr of death, respectively. Tissue samples for histopathologic examination were preserved in 10% neutral-buffered formalin, embedded in paraffin, sectioned at 5 μm, and routinely stained with hematoxylin and eosin. Additional sections of paraffin-embedded kidney were stained according to the Fraser-Lendrum method. Blocks of formalin-fixed kidney cortical tissue were trimmed into 1–2 mm cubes, postfixed in osmium tetroxide, embedded in epoxy resin (Epon), a sectioned at 1 μ, and stained with toluidine blue. Blocks were retrimmed, and ultra-thin (60–100 nm) sections were prepared, mounted on copper grids, stained with lead citrate and uranyl acetate, and examined on a JEOL JEM2000EX-II 200 keV transmission electron microscope. b
Blood, intestinal contents, uterine fluid, and tissue samples were collected from the mare and colt, and standard culture methods were used to isolate bacterial pathogens. Escherichia coli organisms isolated from the animals were serotyped according to standard methods for determining the O antigen. 11 Flagellar (H) antigens were determined by amplifying the fliC gene by polymerase chain reaction (PCR) and further digesting the amplified fragment by restriction enzyme. 6 Virulence attributes of the isolates were identified by an independent laboratory c using PCR analysis as previously described. 2
On gross examination, the mare was found to be in good overall body condition. The mucosa of the cecum and ventral colon were reddened, and the submucosa had mild edema. The kidneys were edematous and pale bilaterally. The lungs were diffusely reddened and edematous.
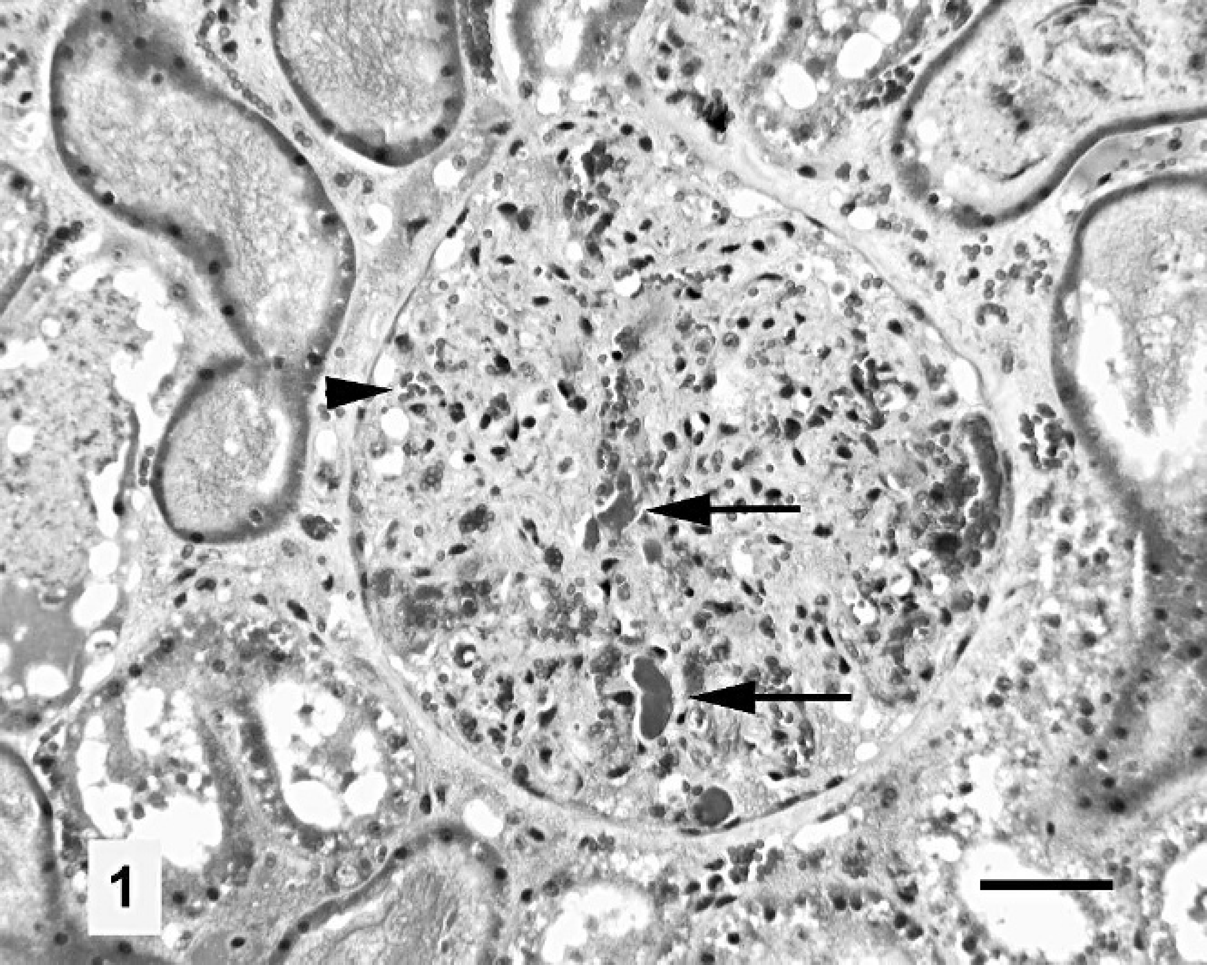
Renal cortex, mare. Glomerular capillaries are filled with dark, elongated deposits of fibrin (arrows), and pale, nonnucleated material indicative of platelets. The capillary lumina are not evident. A few erythrocytes are present (arrowhead). Fraser-Lendrum stain. Bar = 50 μm.
Hematoxylin and eosin-stained sections of the mare's kidneys revealed a number of pathologic changes. There was abundant homogeneous, eosinophilic material (plasma protein) and more granular, eosinophilic material (hemoglobin) in both cortical and medullary tubules. Occasional tubules exhibited epithelial necrosis, particularly in the proximal tubules. Epithelial regeneration was not evident. Tubular epithelial vacuolation and apical blebbing and detachment were also evident. In sections of kidney stained according to the Fraser-Lendrum method there was obliteration of the glomerular structure (Fig. 1). Capillary lumina were not evident, as they were obscured by varying proportions of fibrin, scattered erythrocytes, and amorphous material with staining properties of pale cytoplasm. Neutrophils were occasionally present in mesangial areas. A mild neutrophilic infiltrate accompanied by hemorrhage was found in the endometrium. The endometrial glands contained accumulations of neutrophils and necrotic debris. Mild edema was present in the lamina propria and submucosa of the colon. Histologic sections of brain revealed widening of perivascular spaces within the neural parenchyma, but extravasated proteinaceous material was absent.
Sections of the mare's kidney prepared for transmission electron microscopy revealed prominent glomerular changes. Podocytic processes were partially effaced and condensed. Only occasional electron-dense remnants of glomerular capillary endothelial cell cytoplasm were evident. Elongated electron-dense deposits indicative of fibrin were scattered in glomerular capillaries. Rounded, pale, cytoplasmic profiles consistent with platelets were numerous within glomerular capillaries and often adhered to the exposed basement membrane (Fig. 2). Sparse alpha granules were in their cytoplasm. Bowman's space often had moderately electron dense, homogeneous material consistent with plasma protein.
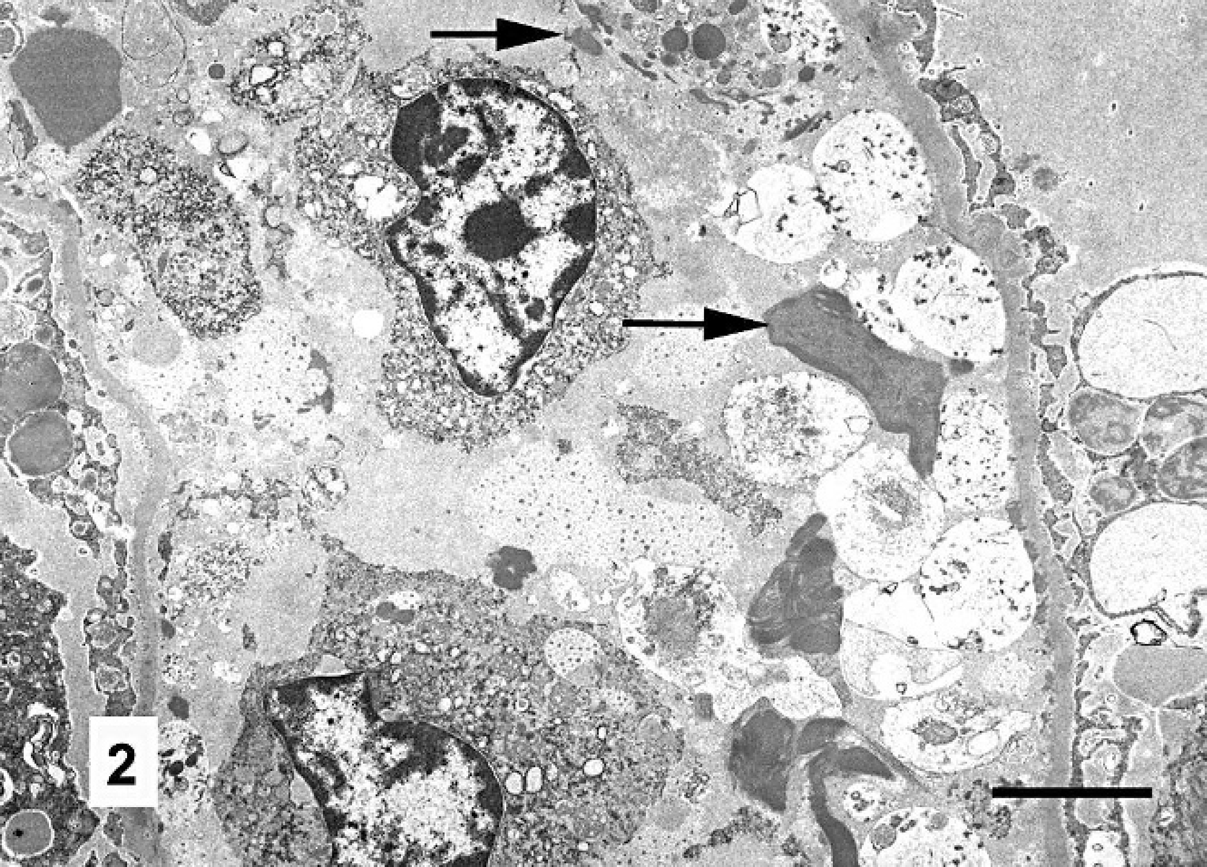
Glomerular capillary, mare. The endothelial lining is largely absent. Swollen, degranulated platelets are associated with the denuded capillary basement membrane (right side). Linear and irregularly shaped accumulations of electron-dense fibrin (arrows) are intermingled with the platelets and two leukocytes. Transmission electron micrograph. Bar = 3 μm.
Escherichia coli, Klebsiella pneumoniae, and Enterococcus faecalis were cultured from the small intestinal contents in heavy growth, and E. coli was isolated from the cecal contents in heavy growth. Escherichia coli, Enterobacter agglomerans, and Pseudomonas spp. were cultured from the uterus. The E. coli isolates were identified as belonging to serotype O103:H2, and were found to carry alpha hemolysin (hlyA) and stx1 virulence attributes as determined by PCR analysis.
On gross pathologic examination, the colt was in normal body condition. There was mild mucosal reddening of the ventral colon. Mesenteric and cardiac vessels were congested. There were no other macroscopic changes. The cranial vault and brain were normal and lacked evidence of brain herniation. Microscopic lesions in the foal were confined to the brain and consisted of a widening of the perivascular spaces with perivascular accumulations of homogeneous, eosinophilic material (plasma protein) in deep gray matter areas of the corpus striatum and thalamus (Fig. 3). Other regions, including cerebral cortex, midbrain, cerebellum, and medulla oblongata, were not affected.
Klebsiella pneumoniae and Enterococcus spp. were isolated in heavy growth from the small intestinal contents of the foal, and E. coli, K pneumonia, and Enterobacter cloacae were isolated in heavy growth from the cecal contents. Light growth of Clostridium perfringens Type A was also obtained from the cecal contents. The E. coli isolate was identified as serotype 0103:H2 and carried the genes hlyA and stx1.
The clinical signs, clinical laboratory abnormalities, and postmortem findings observed in the mare are consistent with HUS as described in the medical literature. 3,4,7,8,9,12,13 Although specific measures of disseminated intravascular coagulation (DIC) were not performed, the characteristic glomerular lesion and absence of systemic involvement, fibrinogen depletion, and hemorrhagic diathesis appear to distinguish the pathology observed in this case from DIC. An apparent inconsistency with HUS is the lack of evidence of microangiopathic hemolysis on the blood smear. A lack of demonstrable schistocytes has been reported in several cases of HUS, bringing the sensitivity of this observation into question. 1 Hematologic examination was performed on blood collected soon after the clinical signs of renal insufficiency became apparent. Schistocytes, as well as anemia, may have become evident with time.
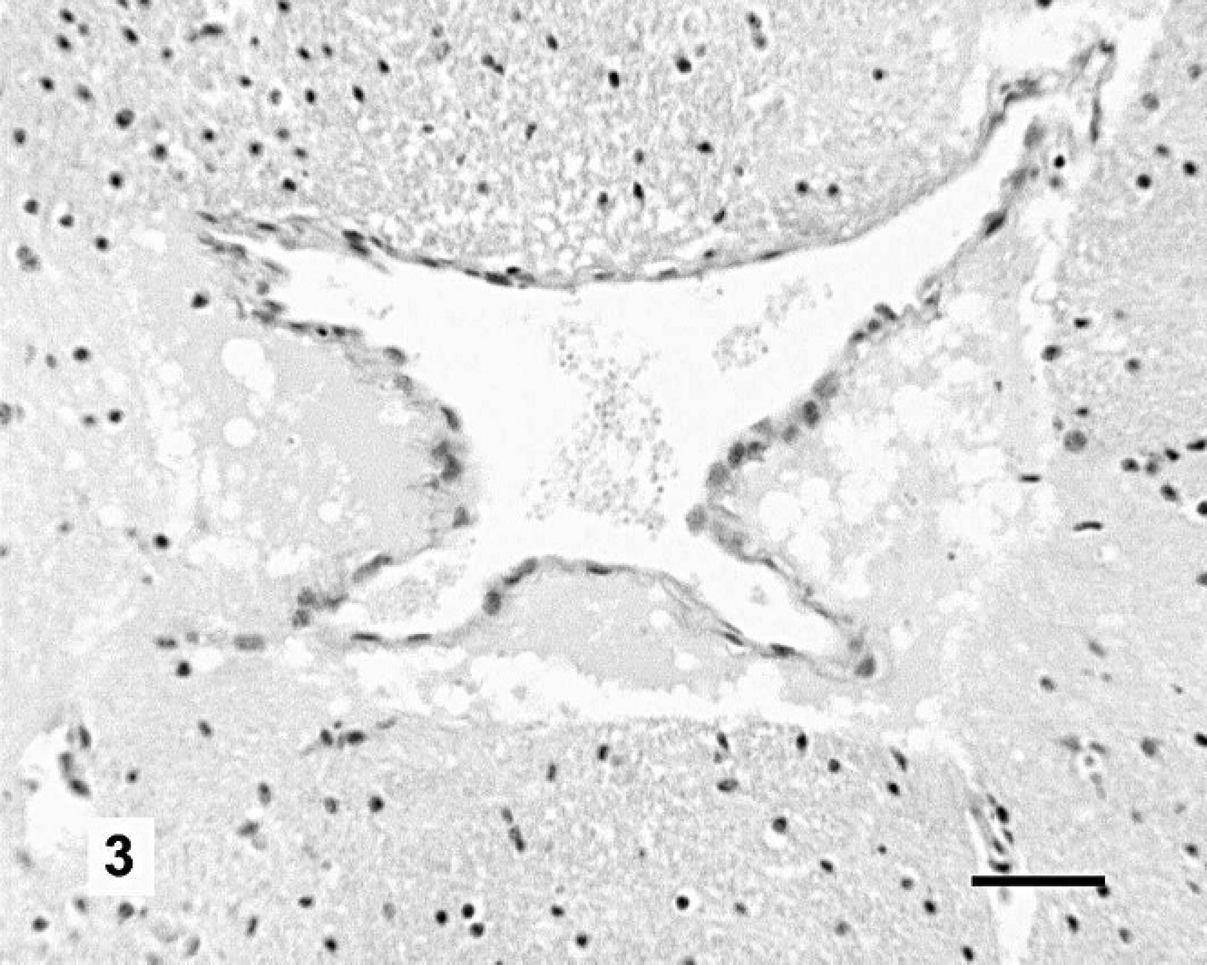
Brain, corpus striatum, foal. The venular perivascular space is filled with eosinophilic, homogeneous material indicative of extravasated plasma protein. Hematoxylin and eosin. Bar = 50 μm.
Escherichia coli 0103:H2, cultured from the uterine contents, is one of the more common non-0157 E. coli serotypes implicated in human cases of HUS, 2 and it must be considered as a possible pathogen associated with the HUS observed in this case. However, direct assays for Shiga toxins, the demonstration of which would be essential in establishing a causal relationship, were not performed. Other pathophysiologic mechanisms of TMA involve genetic defects in complement regulatory proteins, heritable deficiency of the von Willebrand factor-cleaving metalloprotease ADAMTS13, and acquired autoantibodies to ADAMTS13. 4 Additional risk factors include endotoxemia, pregnancy, parturition, neoplasia, viral infections (such as HIV1), antibiotics, antineoplastic agents, immunosuppressive drugs, antiplatelet drugs, radiation, and bone marrow transplantation. 5,8,13
That the disease processes of the mare and foal shared a common etiology cannot be discounted. The clinical presentation was unusual, and the foal's condition is not otherwise readily explained. Encephalopathic signs in newborn foals are most commonly attributable to cerebral hypoxia associated with perinatal asphyxia, which occurs as a consequence of placental insufficiency, premature placental separation, dystocia, prematurity, and/or sepsis. 14 Given the maturity, vigor, absence of sepsis, age of onset, and postmortem findings, neonatal hypoxic-ischemic encephalopathy seems unlikely as a singular explanation for the clinical signs observed in the foal. Other possible causes of seizures in neonatal foals—such as trauma, meningitis, congenital brain malformations, hypoglycemia, hypocalcemia, hyponatremia, and hyperbilirubinemia—are not supported by the clinico-pathologic data. Intravenous fluid administration may have aggravated the underlying neurologic condition.
This report documents HUS after treatment for endometritis in a postpartum mare. Escherichia coli 0103: H2 carrying the gene for Stx1 was identified as a possible pathogen in the disease process, but the true significance of this finding is unclear. The etiopathogenesis of this and similar cases remain unknown. Clinicians and diagnosticians are encouraged to identify and investigate such cases in the future.
Acknowledgements. The authors would like to thank Gayle Thompson of the Colorado State University Diagnostic Laboratory, and Dennis Sylvain and Robert Gore of the library at the James L. Voss Veterinary Teaching Hospital for their invaluable assistance. The authors are grateful for the electron microscopy technical assistance provided by Suzanne Royer.
Footnotes
a.
Hexicon Specialty Chemicals, Houston, TX.
b.
Jeol Ltd., Tokyo, Japan.
c.
Gastroenteric Disease Center, The Pennsylvania State University, University Park, PA.