
Abstract
Muscular pseudohypertrophy was diagnosed in the cervical musculature of a full-term crossbred Simmental fetus delivered by fetotomy. Only head and cervical regions were submitted for pathologic examination; the rest of the fetal body was reportedly normal. The neck musculature of the fetus was markedly deformed by 23 cm and 18 cm in diameter, firm, spherical masses that consisted of enlarged and pale left splenius and right serratus ventralis cervicis muscle, respectively, covered by intact skin. Additionally, lipomatous masses were present within the cervical vertebral canal, compressing the spinal cord. Microscopically, the prominent muscular enlargement was due to massive adipose and fibrous connective tissue replacement of atrophic muscle. Focal myelodysplasia and astrocytosis affecting the grey matter was detected in the mid-cervical region of the spinal cord, accompanied by degeneration in the ascending and descending tracts of the remaining cord segments. Abnormal spinal cord development as a result of severe spinal cord compression by the lipomatous masses within the spinal canal leading to replacement of muscle by fat and fibrous tissue was considered to be the cause of the muscular malformation in this fetus.
Muscle atrophy typically leads to reduction in size of the affected muscle. 11,15,19 Less commonly, macroscopic enlargement of the atrophic muscle occurs due to replacement of muscle by fat and fibrous tissue, a condition known as muscular pseudohypertrophy. 19,21 Muscular pseudohypertrophy is well known in human medicine, but is poorly documented in veterinary medicine. Muscular pseudohypertrophy due to a localized muscular defect known as steatosis is recognized in livestock, especially cattle and pigs, and is most often found as an incidental finding at slaughter. 11,15,19 Microscopic findings of myofiber atrophy admixed with hypertrophy in steatosis have been attributed to denervation, 19 but associated nervous system lesions are not described. This report describes the gross and histologic aspects of congenital muscular pseudohypertrophy characteristic of steatosis in a full-term crossbred Simmental fetus, attributed to localized lack of innervation/denervation secondary to abnormal spinal cord development.
The calf had been conceived through artificial insemination and was delivered by fetotomy due to dystocia caused by marked enlargement of cervical musculature. The head and neck were submitted to the Animal Disease Diagnostic Laboratory at Purdue University for gross and histologic examination. The remainder of the body was reportedly normal.
Grossly, the neck of the fetus was deformed due to large (23 cm and 18 cm in diameter), firm, spherical masses covered by intact skin (Fig. 1). The masses consisted of markedly enlarged left splenius and right serratus ventralis cervicis muscle, respectively. The affected muscles were diffusely pale yellow and doughy, with prominent perimysium on cut section. In addition, two 2.0 × 2.5 × 4.5 cm, ovoid, soft, well-delimited masses with a homogeneous white and slightly gelatinous cut surface were present within the cervical vertebral canal, compressing the spinal cord. These masses were adhered to the periosteum and protruded outward through the right lateral vertebral foramen in the axis and through the right intervertebral foramen between C6 and C7. The interspinous ligament between the latter vertebrae was soft and poorly defined. Masses similar to those within the vertebral canal were also present between some of the transverse processes of the cervical vertebrae on either side of the vertebral column.
Specimens of multiple tissues, including tongue, masseter, various epaxial and hypaxial cervical muscles, the masses in the vertebral canal, brain and the first 5 cervical spinal cord segments, were fixed in neutral buffered formaldehyde (10% formalin), embedded in paraffin, sectioned, and stained with hematoxylin-eosin (HE). Sections of skeletal muscle were also stained with Masson's trichrome and alcian blue, and spinal cord sections were also stained with Luxol fast blue and a polyclonal rabbit antibody against glial fibrillary acidic protein (GFAP). a
Microscopically, the enlarged cervical muscle had marked loss and atrophy of myofibers with massive replacement by adipose and fibrous connective tissue. In some of the fields examined, the majority of the muscle fibers was absent and was replaced by abundant adipose tissue as well as occasionally by pale basophilic, alcian blue-positive ground substance. The myofibers that remained in these areas had considerable variation in cross-sectional diameter: many were markedly thin and poorly defined, with lack of cross-striations (atrophy); others were round and large, with increased eosinophilia and/or sarcoplasmic vacuoles (hypertrophy) (Fig. 2). Occasional cleft fibers were noted. Sarcolemmal nuclei were numerous, often vesicular and of a bizarre shape; some were internalized and in rows. In other areas of the grossly enlarged muscle only isolated myofiber fascicles were affected, and were present next to fascicles of relatively normal myofibers (Fig. 3). The perimysium of affected muscle fascicles was expanded by an increased amount of connective tissue. Multiple small foci of hemorrhage and extramedullary hematopoiesis were also present. Intramuscular nerves were not identified. Other muscles of the deeper layers of the dorsolateral cervical region were also affected, but to a much lesser degree. Tongue, masseter, and muscles forming the ventral cervical group were microscopically normal. The masses located within the spinal canal and on either side of the vertebral column were microscopically composed primarily of adipose tissue, multifocally inter-mingled by fibrous connective tissue septa, blood vessels, and clusters of hematopoietic precursor cells. A thin capsule of fibrous tissue surrounded these masses. In the central nervous system, microscopic lesions were confined to the cervical spinal cord. Focally in the mid-cervical region, there was overall increase in fibrous astrocytes in many spinal cord tracts, accompanied by profound fibrous astrocytosis of the grey matter, areas of gemistocytic astrocytosis, and apparent overall loss of myelinated nerve fibers in many areas. The normal architecture of the grey matter in this location was markedly distorted, with absence of the normal “butterfly” pattern and abnormal location of the motor neurons (Fig. 4). Primarily within the grey matter and to a lesser degree within the white matter there was also prominent perivascular sclerosis. The remaining spinal cord sections had fibrous astrocytic scarring in dorsal, ventral and ventromedial tracts, as well as loss of myelinated nerve fibers.

Muscular pseudohypertrophy in a bovine fetus. Note the cervical deformity due to striking enlargement of the left splenius and right serratus ventralis cervicis muscle. The skin was intact, and has been dissected off of the underlying muscle.
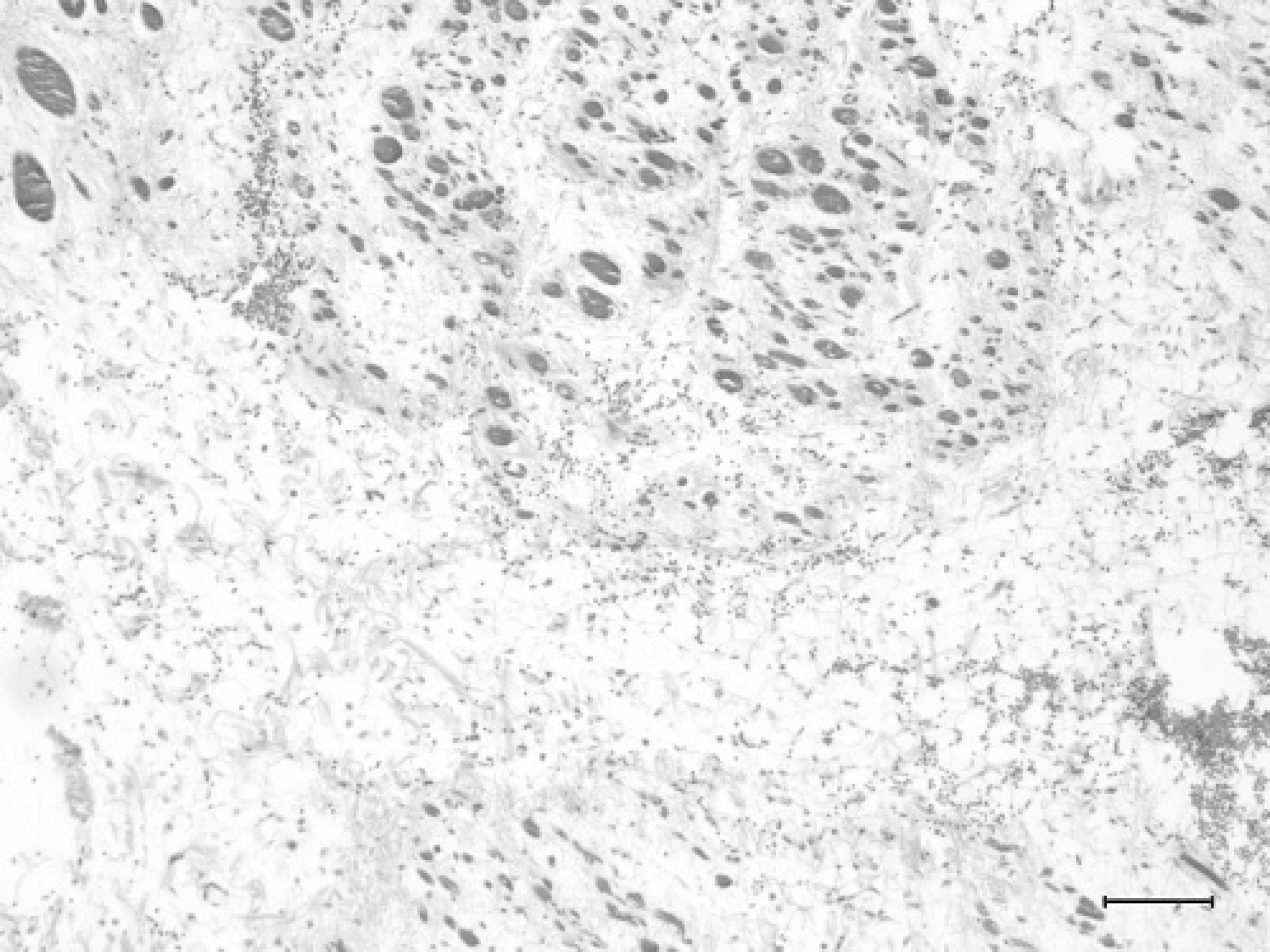
Left splenius muscle of a bovine fetus with muscular pseudohypertrophy. Massive accumulation of adipose and fibrous connective tissue replaces almost entirely the affected muscle. Note the marked variation in size (atrophy and hypertrophy) of the few remaining myofibers. Masson's trichrome. Bar = 100 μm.
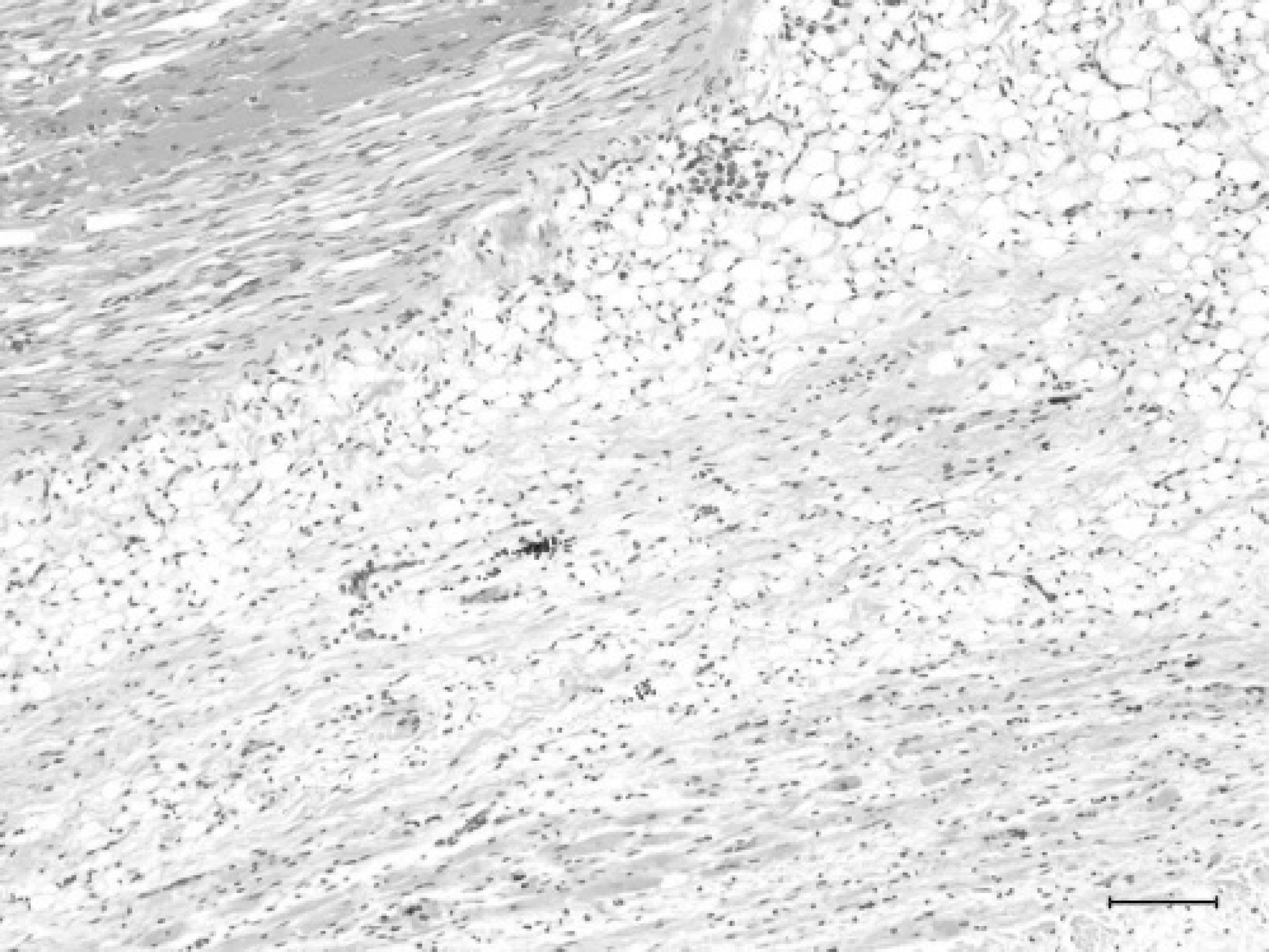
Left splenius muscle of a bovine fetus with muscular pseudohypertrophy. An area with marked loss of muscle fibers and replacement with adipose tissue is located next to an area with relatively normal muscle fibers. Hematoxylin and eosin. Bar = 100 μm.
The marked deformity of the neck of this fetus was determined to be due to massive adipose and fibrous connective tissue replacement of the markedly atrophic left splenius and right serratus ventralis cervicis muscle. The resultant macroscopic enlargement of these muscles is characteristic of muscular pseudohypertrophy. Muscular pseudohypertrophy is most commonly seen in people with chronic (end-stage) dystrophic conditions or with severe chronic denervating lesions. 3,21 The severity and the selective involvement of the musculature in association with the degeneration of the grey matter in the cervical spinal cord in this fetus are supportive of neurogenic muscle atrophy and subsequent development of muscle pseudohypertrophy. Absence of inflammatory response and lack of myofiber regeneration further support a neurogenic condition as the underlying mechanism of the muscle atrophy. 14 However, based only on the histomorphologic features, it cannot be determined whether the alterations are due to failure of innervation or due to denervation. While innervation does not play any part in the initial muscle morphogenesis, at about the time of conversion of myotubes to myofibers the muscle becomes increasingly dependent on neural stimulus. 11,14 In the absence of innervation, muscle differentiation is arrested and the myotubes are replaced by fibrous and adipose tissue. 17

Spinal cord of a bovine fetus with muscular pseudohypertrophy. The grey matter is asymmetric and contains abnormally distributed motor neurons. The pallor of staining in the ventral tracts of the white matter reflects decreased density of myelinated fibers. Central canal (arrow), ventral fissure (F). Masson's trichrome. Bar = 250 μm.
Similar myopathic changes characterized by muscle atrophy and interstitial fibrous and/or adipose tissue proliferation are frequently observed with embryologic defects of the central nervous system that affect the function of motor neurons. 10,14 The majority of these cases have cerebral defects such as hydranencephaly and cerebellar hypoplasia or agenesis, accompanied by arthrogryposis characterized by permanent joint contracture due to neurogenic muscle fiber atrophy. 10,14 The brain in this fetus was grossly and histologically unremarkable. Instead, the myopathic alterations were associated with focal dysplastic and degenerative changes in the spinal cord thought to be the result of severe spinal cord compression by lipomatous masses in the vertebral canal.
Lipomatous hamartomas or lipomas in cattle are infrequent and generally affect either body cavities or subcutaneous tissue. 9 Intracranial and spinal lipomatous masses are reportedly rare in this species. An extradural spinal lipoma was determined to be the cause of progressive paresis of the hind limbs in a 10-month-old bull 1 and a 9-year-old cow, 5 and a lipomeningocele was reported as a presumptive congenital lesion in a 3-month-old calf. 8 The lipomatous mass in the latter animal extended from the corpus callosum into the subcutis of the forehead through a cranial defect. There are only a few other reports on congenital lipomatous masses in bovine. They either formed large masses located within the abdomen, 4,12,16 or infiltrated muscle and lymph nodes of the face. 2 None of them involved the central nervous system directly. In the present case, the lipomatous masses were located in the extradural space of the spinal canal and appeared to represent overabundance of tissue regarded as normal for the site. On this basis they were considered to be a non-neoplastic, hamartomatous, malformative lesion. Consequent pressure onto and deformation of the cervical spinal cord likely led to lack of innervation/denervation of the affected cervical musculature.
A distinct feature of the case described here is the severity of the muscle lesions. The critical initiating event in this case likely occurred early in gestation. Tongue, masseter and muscles forming the ventral cervical group were microscopically unremarkable, and deeper muscles of the dorsolateral cervical region were only mildly affected. This likely reflects differences in nerve supply. The muscles of the head are innervated by branches of cranial nerves, whereas the cervical nerves supply the muscles of the neck. 6 The splenius muscle in ruminants is innervated by the third to eighth cervical nerves, and the serratus ventralis cervicis muscle is innervated by the third to fifth cervical nerves and the long thoracic nerve; other cervical muscles are innervated by the first 2 cervical nerves. 6 The first cervical nerve in ruminants communicates in a variable manner with the hypoglossal nerve (cranial nerve XII), and the second cervical nerve connects with the dorsal branch of the accessory nerve (cranial nerve XI). 7 The collateral innervation from nerves arising in the brain of the fetus may have been responsible for the reduced severity and lack of alterations in the other cervical muscles.
The extent of the spinal cord lesions in this fetus could not be determined since only the proximal portion of the cervical segment was available for histologic examination. The limbs of the fetus were reportedly grossly unremarkable. A decreased number of α-motor neurons in the cervical intumescence is described in calves with arthrogryposis multiplex congenita. 20 Had alterations similar to those observed in the proximal spinal cord of this fetus been present in the remaining spinal cord, the associated musculoskeletal lesions should have been evident to the referring veterinarian.
Many different congenital defects of genetic and environmental cause (including viruses and toxins) have been reported in cattle, 10,13,14,18 but the specific cause of the spinal extradural lipomatous masses leading to focal myelodysplasia and myelodegeneration accompanied by pseudohypertrophy of the innervated musculature in this case is not known. This case illustrates the importance of careful evaluation of the central nervous system and peripheral nerves as well as of muscle in cases of pseudohypertrophy due to steatosis in livestock.
Acknowledgement. We thank Dr. J. F. VanVleet (School of Veterinary Medicine, Purdue University, West Lafayette, IN) for helpful discussion and review of this manuscript.
Footnotes
a.
Dako (Z0334), Carpinteria, CA.