
Abstract
Objectives
Encouraging interest in specialist practice in psychiatry is a key aim of both public psychiatric practice and medical student training. We describe the ongoing development and benefits of an accredited trainee position in academic psychiatry based in public mental health services and a graduate medical school. This is discussed in the context of relevant research evidence on psychiatry training and fostering interest in psychiatry.
Conclusions
The benefits of an accredited trainee position in academic psychiatry extend beyond the skills gained by the trainee, with flow on effects to medical student teaching, attraction to the local training scheme, and fostering a broader culture of academic engagement and activity. The challenges include maintaining funding for a position over nearly two decades, balancing specialist training requirements with clinical and academic service, and also tailoring the roles for the different interests and skills of academic trainees.
There has been longstanding activity to improve interest in psychiatry as a medical specialty career. US research on 29,723 medical students interested in psychiatry indicates that once established, interest is more stable at 50% than other medical specialties, and that a key factor is the clinical placement. 1 There have also been programs to encourage interest in psychiatry among medical students locally 2 and internationally. 3 In most medical schools, clinical academics are involved in teaching the psychiatry curriculum.
Clinical academic training in psychiatry can develop the skills of trainee psychiatrists in medical student teaching and research, and provide a pathway into an academic career. In the US, there have been a number of physician-scientist (MD-PhD) 4 and academic psychiatry training programs 5 designed to bolster the numbers of clinical academics, that have demonstrated effectiveness, including from the perspective of those mentored. 6 There is evidence from other structured, larger-scale training experiences in the US that may also be effective in recruiting interest in academic psychiatry, such as for the first and fourth year of the US psychiatry specialist training program. 7 We describe the development of an academic psychiatry training program.
Background
As part of the establishment of core academic faculty Medical School at the Australian National University, an agreement was struck between the state-funded mental health service in the Australian Capital Territory (ACT), the ACT RANZCP specialist training scheme and the University to enable an academic trainee position in 2006. This was envisaged to provide a pathway for trainee psychiatrists to develop academic skills and experience, and which some might then pursue as a longer-term career. The position was fully-funded by the state health service, and accredited by the ACT Branch Training Committee for advanced trainees (now Stage 3 of the RANZCP training program). 8 This training position was funded continuously until 2024, when it was defunded by the health service for unspecified reasons.
The role was appointed for one year, with the option for a second renewal subject to satisfactory performance, especially with regard to successfully completing training tasks, and examinations. The role was divided into two components. The clinical training component was for 0.5 FTE, and this was reserved for meeting the requirements for clinical advanced training, usually within one of the subspecialty-training certificate schemes, such as Consultation Liaison or Old Age Psychiatry. The academic psychiatry role of 0.5 FTE included curriculum development, with an emphasis on the teaching (of medical students) and research within the university medical school.
The training position necessarily involved clinical and academic training, as the two-year RANZCP fellowship advanced training scheme only permits a maximum of one year of academic research or teaching, with a minimum of one year of clinical training.
Clinical training component
Generally, advanced trainees in psychiatry in Australia undertake the equivalent of two years of full-time clinical training, with options for part-time training. For academic psychiatry trainees in our service, due to the 0.5 FTE employment for clinical training, they will have only one calendar year of clinical attachments to complete their training. The current (like the previous) RANZCP training program for advanced trainees permits up to one year of academic service and research for all specialist training certificates, subject to local Branch Training Committee approval. Therefore, there are challenges to fulfil the requirements for specific clinical placements and supervision for the clinical training component due to the 0.5 FTE commitment. For example, Old Age Psychiatry trainees are required to have a placement of at least 6 months in inpatient care, and 6 months in outpatient care, which would translate in a 0.5 FTE position to one year in each setting. However, trainees are required to complete formative and summative assessments at the same rate at trainees in full-time clinical training. This means that in the most recent version of the RANZCP training curriculum, trainees will need to complete workplace-based assessments and entrustable professional activities, as well as be supervised for the required 4 hours of direct specialist clinical supervision, and also attend a formal educational program within the 0.5 FTE clinical attachment. In practice, as clinical training is necessarily a priority, some of the training requirements will be met in the academic training time.
Academic training component
The role has been designed to embed the trainee as a junior academic in psychiatry. While other trainees can engage with clinical academic supervisors, most do not (being supervised by clinicians who are not academics), and therefore they do not have the enriched access of the academic psychiatry trainee. Similarly, while trainees can teach in the medical student teaching program, only the academic psychiatry trainee is required to have a teaching load, with support from the clinical academic lead.
Over a typical two-year 0.5 FTE attachment, this involves direct involvement in the delivery of medical student teaching for didactic lectures and interactive clinical case and skill-development workshops. Trainees also participate in curriculum and examination development, as well as formative and summative assessments through Objective Structured Clinical Examinations (OSCEs) such as conducting a mental state examination. These teaching and examination aspects are identical, relative to level, to the roles of clinical academic psychiatrists in substantive medical school positions.
It is also essential that trainees have direct involvement in the generation of new scholarly activities in psychiatry, upon which the delivery of modern psychiatric care is based. Accordingly, trainees are encouraged to discuss with their academic supervisor the development of a research project or similar scholarly activity, such as a systematic literature review or quality assurance project. Trainees can discuss, and if of interest, align to existing research streams within the Academic Psychiatry Department in the Medical School. Examples of trainees’ research have included: original experimental research projects such as analysis of mental health data published by the Australian Institute of Health and Welfare, neuroimaging research related to neurodegenerative disease, and mental health policy research.
As an additional benefit for local psychiatric training, the skills of trainees and supervisors in providing research training supervision have translated to support of other local trainees for the successful completion of the research skills-based scholarly project, through supervision by academic psychiatry trainees and departmental staff. 8 Similarly, academic trainees have been involved in supervision of medical students undertaking mandatory research projects for their medical degree.
A qualitative survey of the research needs of 165 advanced trainees in Ireland found that the key themes identified were a ‘collaborative research culture’, ‘choice’, ‘guidance’, and ‘access to resources’. 9 In this context, the academic psychiatry trainee has weekly supervision with their academic mentor, who is usually the head of the academic department, and participates in the weekly teaching and research meetings, with the opportunity to seek supervision and collaboration on research with any of the academic psychiatry staff.
Typical timetable of an academic trainee in psychiatry. a
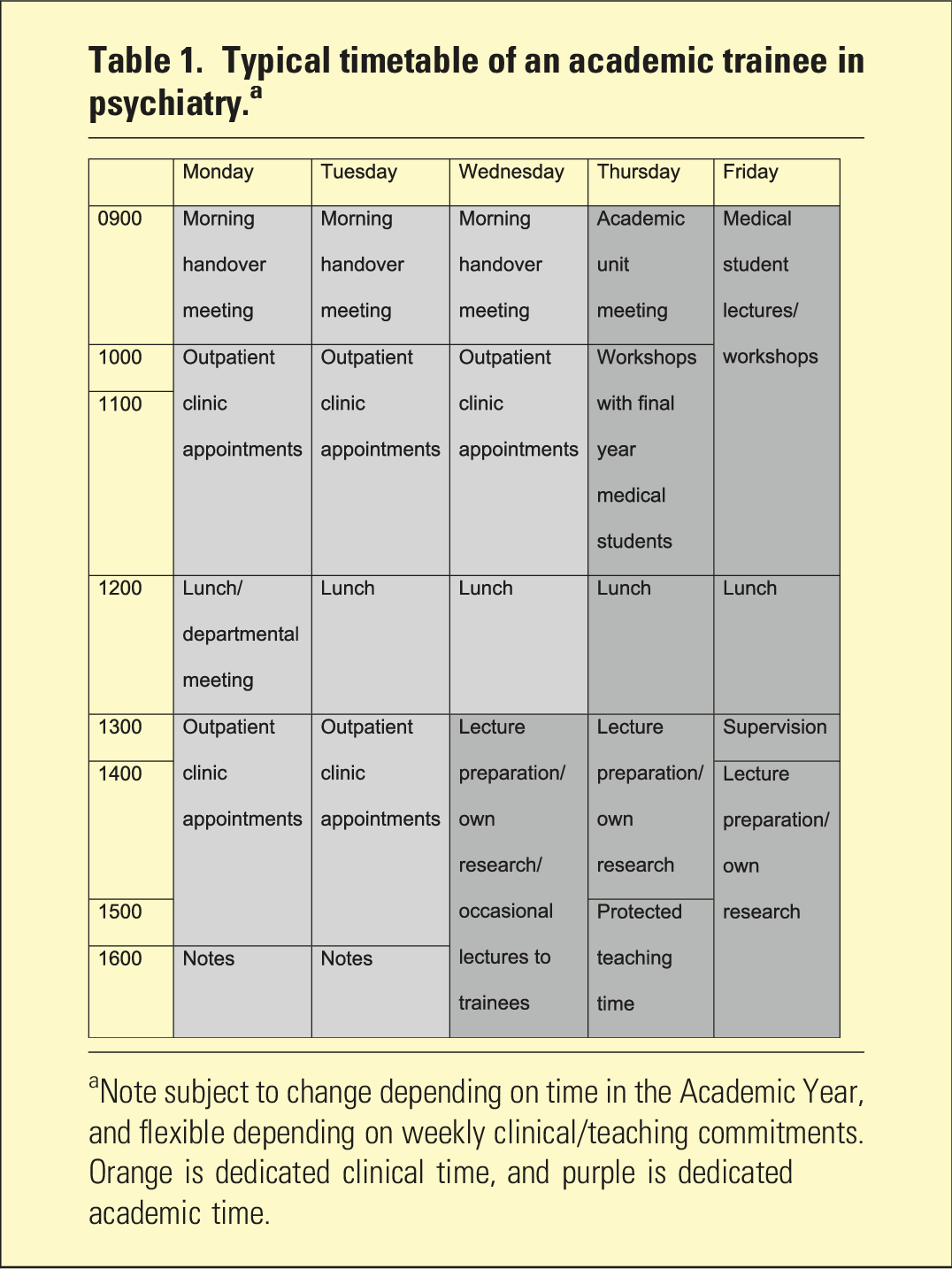
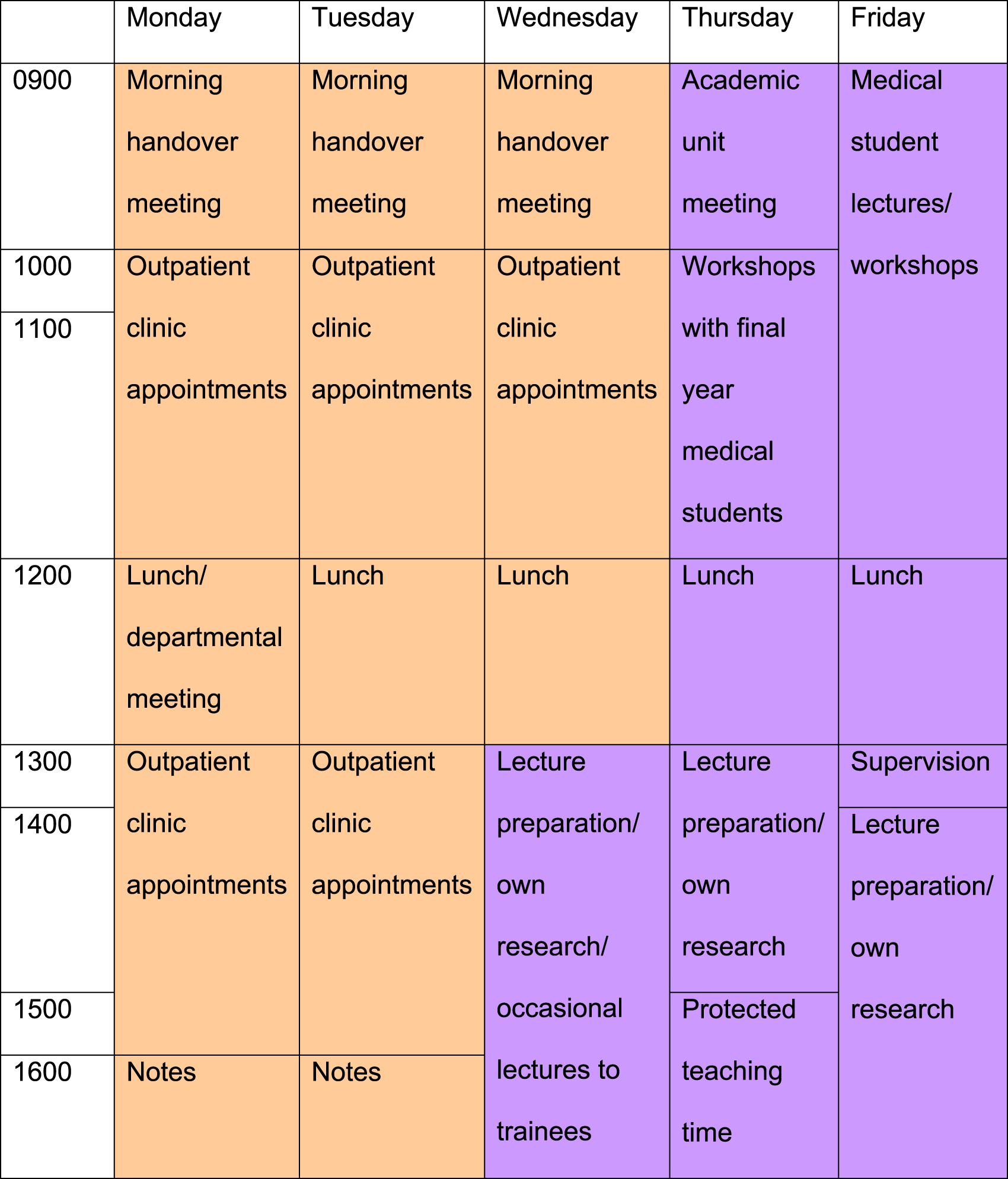
aNote subject to change depending on time in the Academic Year, and flexible depending on weekly clinical/teaching commitments. Orange is dedicated clinical time, and purple is dedicated academic time.
Benefits
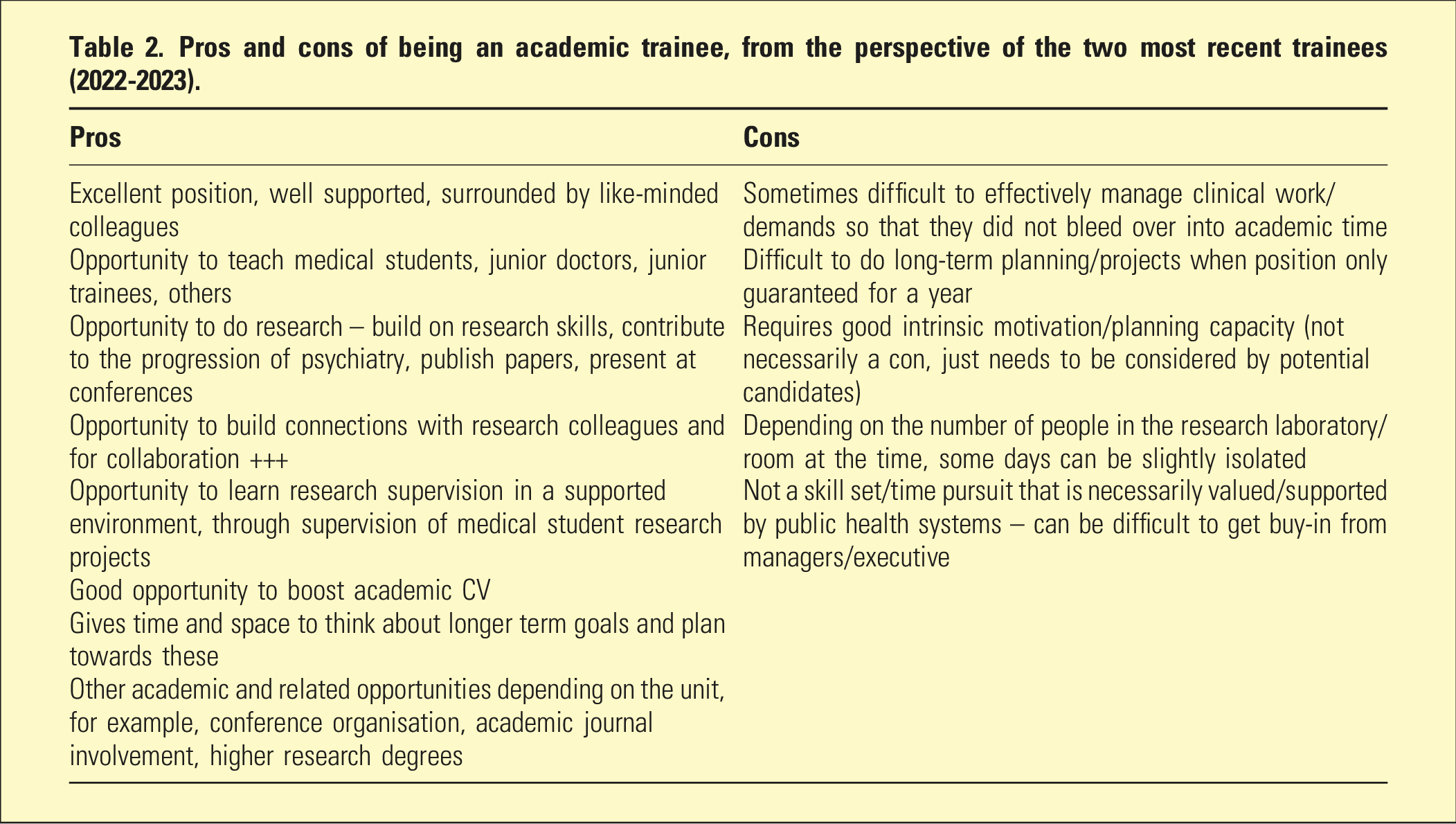
Pros and cons of being an academic trainee, from the perspective of the two most recent trainees (2022-2023).
Notably, there is the opportunity for weekly, high-quality supervision both one-on-one, and in teaching and research staff meetings, as noted as a positive experience for general psychiatric training in a qualitative review. 10 Support from other academic team members, as well as academic freedom, are regarded as a positive training experiences. 10
The program’s impact extended beyond individual trainees in creating broader cultural changes within the service. Academic trainees generated increased interest in academic psychiatry among their peers, with other trainees seeking opportunities to engage in research and teaching even without holding the formal academic position. This ‘academic contagion’ led to increased research collaboration between trainees, more involvement in medical student teaching, and greater engagement with scholarly activities across the whole training program.
The serendipity of local academic developments has permitted trainees to be involved in broader academic roles, such as scientific conference organisation and engagement with medical journals, including peer-reviewing submitted papers, as well as ongoing public mental health research.
Challenges
Among the challenges are that sometimes trainees can struggle with the rather structured and potentially competing workload of a joint academic and clinical training position (Table 2). In local experience, trainees will prioritise based on their training needs. However, it has been essential that academic and clinical supervisors ensure that the trainee meets their training targets for progression through the specialist training program, and that means that clinical training requirements are paramount. In some circumstances, this has meant that there has been lesser involvement in primary research, as trainees may have already completed their mandatory scholarly project for the RANZCP curriculum, and may be interested in curriculum development and teaching.
State-funded academic positions inherently lack long-term funding security. The training position was de-funded by the public mental health service. This is consistent with the gradual decline of academic psychiatry in medical schools, 11 where academic leads are no longer actively appointed, or at least take very long periods to recruit.
Push and pull factors for recruitment of psychiatrists are also important, such as the family and relational roles cited by European trainees, 12 and will affect burgeoning academic psychiatrists.
There are also important challenges in achieving diversity by gender 13 and minority ethnic status 14 that are active considerations in promoting access and advancement of a more diverse community of academic psychiatrists. Advertising for, and consideration of, a broad range of applicants is a start, but perhaps trainees may also be encouraged to apply by mentors. Also, there are worldwide challenges from workplace harassment, incivility, and poor psychosocial milieus in academic medicine. 15
Concluding comments
Once a valued training experience, we have not heard of a similar long-standing program in Australia. The initiative has ultimately proved vulnerable, as when the support from the university and health service declines, and/or key stake-holders have changed. Fundamentally, effectiveness depends on leadership from bona fide clinical academic faculty (i.e. leading in practice, teaching, and research), who are dwindling. This means the program is now effectively shuttered. Nonetheless, perhaps this brief overview may encourage other health services and universities to develop such initiatives. Further development and necessary evaluation will determine if such projects are feasible and effective.
Footnotes
Disclosure
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCLL, FAW, RER, and PAM are editorial staff of the journal and were not involved in the independent peer-review of this paper. This paper represents the views of the authors, not the journal or other organisations they are affiliated with.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Authorship
All authors have satisfied: Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND drafting the work or revising it critically for important intellectual content; AND final approval of the version to be published; AND agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.