
Abstract
Objectives
This perspective examines the role of psychiatrists in section 10 assessments under the Mental Health Act (MHA) in Aotearoa New Zealand, focusing on their involvement, concordance with preliminary assessments, and implications for service delivery. It also explores the potential impact of a capacity-based model.
Methods
Data was requested from all 20 District Health Boards (DHBs) on section 10 assessments completed between July 2022 and July 2023, including how many resulted in a section 11 certificate. Response rates and concordance between section 8(b) and section 10 assessments were analyzed.
Results
Data from six DHBs showed over 95% of section 10 assessments led to a section 11 certificate, demonstrating high concordance. Psychiatrists conducted most section 10 assessments. However, approximately 1 in 20 cases involved non-concordance, suggesting psychiatrist-led assessments serve as a critical safeguard.
Conclusions
High concordance rates suggest inefficiencies, yet the 1 in 20 non-concordance highlights an important safeguard. Given psychiatrist shortages and after-hours workload, reconsideration of the MHA process is warranted. Possible reforms include streamlining assessments, enabling non-psychiatrist practitioners to conduct final evaluations in some cases, and adopting a capacity-based model to optimize service delivery while maintaining safeguards.
Introduction
The Mental Health (Compulsory Assessment and Treatment) Act 1992 (MHA) governs involuntary treatment in New Zealand. It provides the legal framework under which individuals experiencing severe mental illness may be assessed and treated without their consent if they meet specific statutory criteria. The act aims to balance individual rights with public safety and clinical necessity.
Under the MHA, the process of involuntary assessment begins with a Section 8(a) application, typically completed by a concerned party such as a general practitioner (GP), family member, or police officer. This is accompanied by a Section 8(b) certificate from a medical practitioner (often a GP or emergency doctor), which provides clinical justification for further psychiatric evaluation. If the Section 8(b) assessment supports the need for further assessment, a psychiatrist conducts a Section 10 assessment to determine whether compulsory treatment under Section 11 is warranted. The two-stage assessment process under Sections 8(a) and 8(b) is intended to act as a safeguard, ensuring that individuals are not subject to psychiatric detention without sufficient justification. However, the requirement for a psychiatrist-led Section 10 assessment after an 8(b) assessment raises questions about efficiency, particularly given the high concordance between the two steps.
The mental health sector in Aotearoa New Zealand (NZ) has long grappled with challenges related to insufficient resourcing, particularly for inpatient and secondary mental health and addiction services. A recent study by Every-Palmer et al. 1 highlighted that psychiatrists and trainee psychiatrists (registrars) regard after-hours work being a significant cause of this concern. Notably, 90% of those working on acute on-call rosters reported an increase or substantial increase in demand for their after-hours services. One of the sources of this on-call demand is the assessment of patients under the Mental Health Act (MHA), which currently enshrines the need for a psychiatrist to undertake section 10 assessments “if reasonably available.” It determines that, in the event of a psychiatrist being reasonably unavailable, “a medical practitioner or nurse practitioner… who, in the opinion of the Director of Mental Health, is suitably qualified” can be used in their stead. Ergo, the requirement and involvement of a psychiatrist, on-site, undertaking the assessment, hinges on what counts as “reasonably available.” This terminology is not currently interpreted uniformly across NZ which then creates room for a psychiatrist to not be necessary in the process. “Reasonably available” is defined as being readily able to be contacted without undue effort and willing and able to act in a timely manner considering the urgency of the individual's health care needs. 2 However, there is a paucity of published data available to assess the impact of specialist psychiatrist involvement in this process.
The Ministry of Health (MoH) is currently reviewing the MHA with a probable decision to move towards a capacity-based model, aligning with frameworks in other developed countries such as the UK. 3 Notably, the proposed Mental Health Bill expands the role of mental health practitioners as assessors, potentially reducing the reliance on psychiatrists for compulsory assessment processes. This shift reflects an effort to address workforce constraints and improve accessibility while maintaining clinical safeguards. However, the implications of this change for service delivery, professional responsibilities, and patient rights remain key areas for examination. 4
Methods
Data regarding the use of section 10 assessments (and the involvement of psychiatrists in such a process) is not collected centrally which is unusual compared to other Sections of the MHA. 5 Therefore, the Directors of Area Mental Health Services (or their administrative counterparts) of the 20 New Zealand Districts 6 were contacted on three distinct/separate occasions to optimize responsiveness. The information requested was the number of Certificates of Preliminary Assessment (Section 10 (2) (b)) completed between July 2022 and July 2023. Of these, information was requested regarding how many section 10 assessments proceeded to the issuing of a section 11 certificate.
Where a Section 8(a) was not followed by the completion of a Section 8(b), these were not analyzed or included in this analysis as the further evaluation via specialist review was not required.
Results
Number of Section 10 assessments and discontinuation of the mental health act by district. Absolute numbers over a 12 month period (percentage)
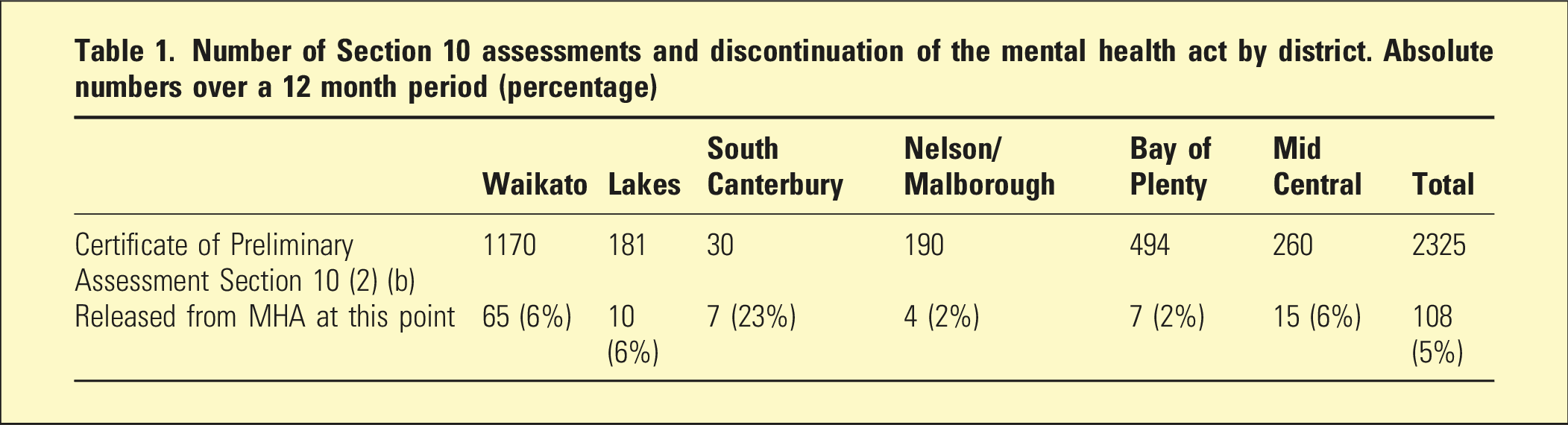
This indicates that, in most cases, psychiatrists agreed with the initial assessments made by those completing the 8(b) and continued the involuntary process. Of those providing the data, it was noted that the completion of Section 10 assessments was completed by psychiatrists in more than 98% of cases (as opposed to the official MHA terminology of a “mental health practitioner”—a nurse practitioner, a medical practitioner, or a registered nurse practising in mental health).
Discussion
Notably, only 1 out of every 18 patients did not require further assessment and treatment by a psychiatrist (i.e., the Section 10 did not proceed to an 11) after an initial assessment by whoever completed the 8(b), which is perhaps a low rate considering the expectation regarding psychiatric expertise in assessing risk and making decisions regarding involuntary treatment. An immediate limitation with the data is that it does not distinguish who did the 8(b); that is, a psychiatrist could have completed the 8(b). However, it can be inferred that most were seeing a psychiatrist for the first time during this process by virtue of resourcing. In any event, the purpose of a Section 10 assessment is a protective measure for the proposed patient; it is a procedure involving formal assessment which addresses the criteria of the legislation and, as such, it cannot be based on the Section 8(b) assessment. Furthermore, a Section 11 does not definitively mean an in-patient admission; data from the MHA office of the author’s District Health Board (DHB) over a 2 month period demonstrated that only 4% were not admitted.
The Royal Australian and New Zealand College of Psychiatrists (RANZCP) considers psychiatrists responsible for assessing the risk of self-harm, suicide, and harm to others [REF]. However, under the MHA, other practitioners, such as medical practitioners, nurses, and psychologists, can also initiate the involuntary treatment process. Another way of stating this is that 95+% of the time, those completing the 8(b) could be interchangeable with the role of the psychiatrist completing the Section 10 assessment without altering the assessment outcome. That said, this paper falls short in considering other aspects outside the medico-legal requirement such as consulting with the family and the reassurance for family and patient that they have been seen by a senior doctor.
With the introduction of the Mental Health Bill, the scope of compulsory assessment is expected to expand beyond psychiatrists, incorporating mental health practitioners in assessment roles. While this adjustment aims to alleviate workforce pressures and ensure timely evaluations, it raises concerns regarding the consistency and rigor of clinical decision-making. Given the findings in this study—where over 95% of Section 10 assessments confirmed initial Section 8(b) determinations—it remains unclear whether this shift will meaningfully alter patient outcomes. A key question is whether empowering a broader workforce to complete these assessments will enhance service efficiency or introduce variability in assessment standards.
The findings of this study must be considered within the wider context of defensive practice and the prevailing culture of risk aversion in New Zealand’s mental health system. The high concordance rate (95%) between Section 8(b) and Section 10 assessments suggests that, in most cases, psychiatric assessment merely confirms an existing risk-based determination rather than offering a fresh, independent clinical judgment. While psychiatrist involvement is often justified as a safeguard against wrongful detention, the lack of variance suggests that decisions are shaped more by systemic risk-aversion than by meaningful risk stratification. The Ministry of Health’s 2022 discussion paper “Reviewing Risk” acknowledges this issue, highlighting that psychiatric risk assessment in New Zealand remains inconsistently applied and overly influenced by medico-legal concerns rather than clinical need. 7 Furthermore, the 2018 He Ara Oranga report 8 called for a national conversation about mental health and risk, but this has yet to materialize. The absence of such a discussion continues to leave clinicians in a position where they default to defensive decision-making, potentially reinforcing the reliance on involuntary treatment rather than promoting less restrictive alternatives. This raises fundamental questions about whether the proposed changes to the MHA—particularly the introduction of non-psychiatrist assessors—will reduce unnecessary detentions or simply redistribute liability and defensive practice across a broader workforce.
One of the arguments for psychiatrist involvement is therefore to manage the risk and provide the highest level of assessment to unwell patients. Furthermore, another argument could be that registrars (often completing the Section 8(b)) are more prone to practise defensive practice. The He Ara Oranga report, 8 stated that “clinicians working under the MHA, particularly psychiatrists and mental health nurses whose decisions have been subject to criticism from DHB reviews, coroners’ inquests and Health and Disability Commissioner investigations, have unsurprisingly developed a culture of risk aversion and defensive practice.” It could be argued that the high concordance of Sections 8(b) and 10 are indicative of this, that is, if one person believes the MHA is required, it is more difficult (and risky) for another to disagree. Defensive practice is generally defined as health professionals' deviation from sound medical practice motivated by a desire to reduce exposure to malpractice litigation. However, in many studies, this takes on a broader definition and can be grouped into four categories: fear of patient dissatisfaction, fear of overlooking a severe diagnosis, fear of negative publicity, and unconscious defensive practice. 9 Despite New Zealand’s no-fault compensation model, the country has not been immune to claims of defensive practice, 10 often linked to doctors changing their usual practice to avoid complaints rather than litigation. 11 Certainly, cases whereby no prosecution has been brought can still result in subsequent reputational damage. 12
One of the practices most frequently perceived as defensive is when psychiatric admission is used as a means of mitigating risk and subsequent negative publicity, with at least 34% of admissions thought to be defensive decisions, 13 a finding that has been replicated internationally. 14 For the psychiatrist to prove meaningful in protecting against the defensive action of those undertaking the previous assessment, a wider disparity would be anticipated.
Even less information is available regarding the other likely contributing factors to the infrequent discontinuation of the MHA by psychiatrists: local data from internal research suggests that two-thirds of admissions occur outside of working hours. It is logical to presume that “less restrictive interventions” such as respite or home-based treatments are therefore unavailable at the time of assessment, 15 which effectively results in a binary option: home or admission. The other option of an informal or involuntary admission on locked wards is a violation from a human rights perspective, 16 which unfortunately can result in the MHA almost becoming a prerequisite for a given admission (and ergo, involvement of a psychiatrist in the assessment).
These findings suggest that while psychiatrists provide an essential safeguard in the involuntary treatment process, the high concordance rate raises important questions about the necessity and efficiency of current procedures. It remains unclear whether this high concordance reflects true clinical agreement, defensive practice, a lack of alternative treatment options, or systemic pressures leading to conservative decision-making. Future research should explore how changes to the Mental Health Act—such as expanding assessment roles to non-psychiatrist mental health practitioners—might influence decision-making processes, workforce demands, and patient outcomes. In particular, a key question for service planners is whether more structured training for non-psychiatrist assessors at the Section 8(b) stage could improve efficiency while maintaining safeguards.
Research into the determinants of the MHA continuation by psychiatrists following Section 8(b) assessments and its potential for a negative impact on patient’s recovery and wellbeing needs to be expanded to include and account for demographics of those assessing and those being assessed as well as qualitative information gathering examining the culture and perceptions of psychiatrists assessing. Similarly, data on the impact of whom is completing the 8(b) might offer further insights. Meanwhile, considering the well-documented specialist shortage in the mental health workforce and the distress related to the on-call roster for psychiatrists, the evidence provided by this research suggests that the current process of mandatory psychiatric assessment following Section 8(b) assessment is hardly cost-effective within a fiscal or wellbeing context. Furthermore, arguments suggesting the sequential process of the MHA is there to protect the rights of the patient simply do not apply for the vast majority of patients assessed (as the outcome is unaltered by the sequential step of a Section 10 assessment). The results from South Canterbury are comparative outliers, and further investigation into this might yield further interesting factors such as who is completing the Section 8 and 10 assessments and what options are available beyond their small 12-bed unit. It may also suggest that higher concordance amongst other districts is secondary to later presentation of illness or other upstream factors.
Conclusion
The proposed changes under the Mental Health Bill represent a significant policy shift that could reshape the workforce structure for compulsory psychiatric assessments. While this may address psychiatrist shortages, further investigation is needed to determine whether expanding assessment roles to mental health practitioners will lead to meaningful improvements in efficiency and patient care or simply redistribute risk management responsibilities. A nuanced approach that incorporates workforce realities, legal safeguards, and empirical assessment of outcomes will be critical in determining the long-term impact of these legislative changes.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All sources for this article are included as references with an absence of data beyond this.