
Abstract
Objective:
The COVID-19 pandemic has had a profound effect on global mental health, with one-third of infected individuals developing a psychiatric or neurological disorder 6 months after infection. The risk of infection and the associated restrictions introduced to reduce the spread of the virus have also impacted help-seeking behaviours. Therefore, this study aimed to determine whether there was a difference during the COVID-19 pandemic in the treated incidence of psychotic disorders and rates of admission to hospital for psychosis (including involuntary admission).
Methods:
Incident cases of first-episode psychosis in young people, aged 15 to 24, at an early intervention service in Melbourne from an 8-month period before the pandemic were compared with rates during the pandemic. Hospital admission rates for these periods were also compared.
Results:
Before the pandemic, the annual incidence of first-episode psychosis was 104.5 cases per 100,000 at-risk population, and during the pandemic it was 121.9 (incidence rate ratio = 1.14, 95% confidence interval = [0.92, 1.42], p = 0.24). Immediately after the implementation of restrictions, there was a non-significant reduction in the treated incidence (incidence rate ratio = 0.80, 95% confidence interval = [0.58, 1.09]), which was followed by a significant increase in the treated incidence in later months (incidence rate ratio = 1.94, 95% confidence interval = [1.52, 2.49]; incidence rate ratio = 1.64, 95% confidence interval = [1.25, 2.16]). Before the pandemic, 37.3% of young people with first-episode psychosis were admitted to hospital, compared to 61.7% during the pandemic (odds ratio = 2.71, 95% confidence interval = [1.73, 4.24]). Concerning the legal status of the admissions, before the pandemic, 27.3% were admitted involuntarily to hospital, compared to 42.5% during the pandemic (odds ratio = 1.97, 95% confidence interval = [1.23, 3.14]).
Conclusion:
There was a mild increase, which did not reach statistical significance, in the overall incidence of first-episode psychosis; however, the pattern of presentations changed significantly, with nearly twice as many cases presenting in the later months of the restrictions. There was a significant increase in both voluntary and involuntary admissions, and the possible explanations for these findings are discussed.
Background
The COVID-19 pandemic has had a profound impact on mental health across the world (The Lancet, 2020). The infections can be associated with neuropsychiatric complications (Nakamura et al., 2021), and one-third of affected individuals develop a psychiatric or neurological condition within 6 months after infection (Taquet et al., 2021). During previous epidemics, such as Middle Eastern Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS), it was found that between 4% and 11% of individuals can experience psychotic symptoms following infection (Brown et al., 2020). In addition to this, social factors associated with an increased risk for psychotic disorders have increased during the pandemic, specifically unemployment, social isolation and stress (Reininghaus et al., 2008). However, for some individuals, there may be a reduction in risk factors, such as the reduction in stress associated with not having to attend education or work settings for those with social anxiety disorder. There may also have been a reduction in the use of illicit substances as a result of less social gatherings. Given these factors, it is important to evaluate whether the COVID-19 pandemic has had an impact on the incidence of psychotic disorders.
In addition to the possible neuropsychiatric and psychosocial impact of COVID-19, the pandemic has also been associated with a significant change in help-seeking behaviours. In the initial period of the pandemic, individuals were hesitant about attending emergency departments or general practitioners. In some jurisdictions, people were actively discouraged from attending these services unless they were extremely unwell (Sless et al., 2021). Therefore, it is possible that referral rates for psychotic disorders during the pandemic may initially have declined due to a delay in help seeking, but may have been followed by a subsequent upswing in presentations characterised by a longer duration of untreated psychosis. As longer delays to treatment are associated with more severe psychotic symptoms (Howes et al., 2021), the need for admissions to hospital could also have increased (O’Donoghue et al., 2014).
Therefore, this study aimed to determine whether there was a difference during the COVID-19 pandemic compared to the previous year in (1) the treated incidence of psychotic disorders and (2) rates of admission to hospital (including involuntary admission). In addition, we aimed to determine whether the incidence rate of first-episode psychosis (FEP) was correlated with the admission rate (total and involuntary admission rate).
Methods
Participants and setting
The Early Psychosis Prevention and Intervention Centre (EPPIC) is an early intervention (EI) for psychosis service within Orygen, a state-funded youth mental health service covering a defined catchment area within Northern and Western Melbourne. This study included all young people diagnosed with a first episode of psychosis between 1 March 2019 and 31 October 2020. To be eligible to receive treatment at EPPIC, clients must be aged between 15 and 24 years, be residing within the defined catchment and be diagnosed with a first episode of psychosis, operationalised as experiencing full threshold psychotic symptoms daily for at least 1 week. Sources of referral include local mental health services, general practitioners, law enforcement agencies, community support services, family members and friends, and self-referral.
Catchment area
The EI service has a geographically defined catchment area that encompasses the Northwestern areas of Melbourne that covers a total population of over 1 million. From the 2016 Australian Census, it was determined that there were 191,356 people aged 15 to 24 within the catchment area (Australian Bureau of Statistics, 2016). The incidence rate of FEP is high within this catchment area, with a treated incidence study identifying that there were over 100 cases per 100,000 of the at-risk population (i.e. those aged 15–24 years; Eaton et al., 2019).
Instruments and sources of information
All cases of FEP were recorded at the time of entry to the service, and demographic data were captured. Any admission to the Orygen inpatient unit was recorded in the clinical notes, and if an admission occurred in a different inpatient unit prior to referral, this was documented in the referral letter and the initial assessment. All of these documents were reviewed to determine whether an admission occurred at the time of presentation and the legal status of the admission. A structured clinical risk assessment is conducted at time of entry to the service and it contains three questions about self-harm and suicidality. A single variable was created that indicated whether an individual scored positive on any of these three items. Furthermore, within the risk assessment, an item indicated whether the individual had any current difficulties with illicit substance abuse. Demographic information, such as living arrangements and employment status, was collected at the initial presentation in a registration document.
Statistical analysis
Incidence rate ratios (IRRs) were determined by comparing the incidence of FEP for the period 1 March 2019–31 October 2019 (pre-COVID-19) to the period 1 March 2020–31 October 2020 (during the pandemic) using the Poisson term with Stata version 15.1 (StataCorp, 2019). The IRR controlled for age and sex, and the at-risk population was determined from the 2016 Australian Census. Binary logistic regression was used to determine the odds ratio (OR) for admission at the time of presentation, and in total, six models were performed. The first model examined the risk of admission across the two periods. The second model controlled for demographic factors (sex, age, living arrangements and employment/educational status). The third model controlled for clinical factors, specifically any self-harm or suicidality at presentation or illicit substance abuse. These models were repeated with the outcome of involuntary hospital admission. Finally, Spearman’s correlations (rs) were performed to determine whether the number of cases per month correlated with the proportion of cases admitted to the inpatient unit during that month, either voluntarily or involuntarily.
Ethical approval
Ethical approval was received from the Melbourne Health Human Research Ethics Committee (HREC). The study aimed to examine the incidence rates and therefore all cases were needed to be included, and as a result, a waiver for individual consent was granted by the HREC.
Results
Treated incidence of FEP
The number of new cases of FEP diagnosed per month between 1 March 2019 to 31 October 2020 is presented in Table 1, and a visual representation of this treated incidence rate is presented in Figure 1. In the 8 months between 1 March 2019 and 31 October 2019 (pre-COVID-19), a total of 150 young people presented with an FEP from an at-risk population of 191,356, equating to an estimated annual treated incidence of 117.6 per 100,000 at-risk population. In the 8-month period during the pandemic of 1 March 2020 to 31 October 2020, 175 cases of FEP presented and this equated to an annual treated incidence of 137.2 per 100,000 in the at-risk population. When comparing the two time periods, there was no statistical difference in incidence rates when controlling for age and sex (IRR = 1.14, 95% confidence interval [CI] = [0.92, 1.42], p = 0.24). The monthly treated incidence rates for FEP are presented in Table 1 and show that there was a non-significant decrease in April 2020, the month after restrictions were introduced (IRR = 0.80, 95% CI = [0.58, 1.09]), which was followed by an increase in the treated incidence in July (IRR = 1.94, 95% CI = [1.52, 2.49]) and August (IRR = 1.64, 95% CI = [1.25, 2.16]). The monthly incidence rate is also displayed visually in Figure 1. A comparison of the demographic characteristics of the young people who presented with an FEP before the pandemic (1 March 2019–31 October 2019) to the period during the pandemic (1 March 2020–31 October 2020) is presented in Table 2.
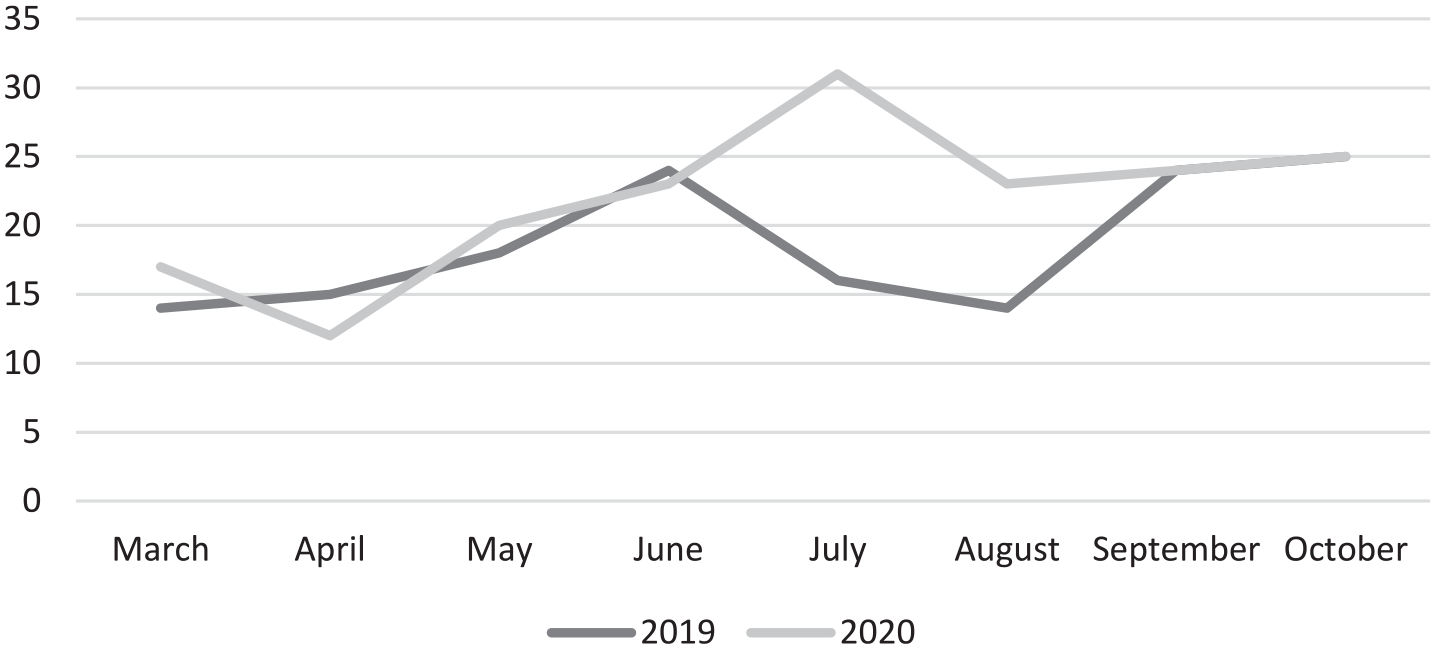
Monthly incident cases of FEP before and during the pandemic.
Number of new cases of FEP diagnosed per month, incidence rates, proportion admitted and incidence rate ratio of pre-pandemic versus during the pandemic.
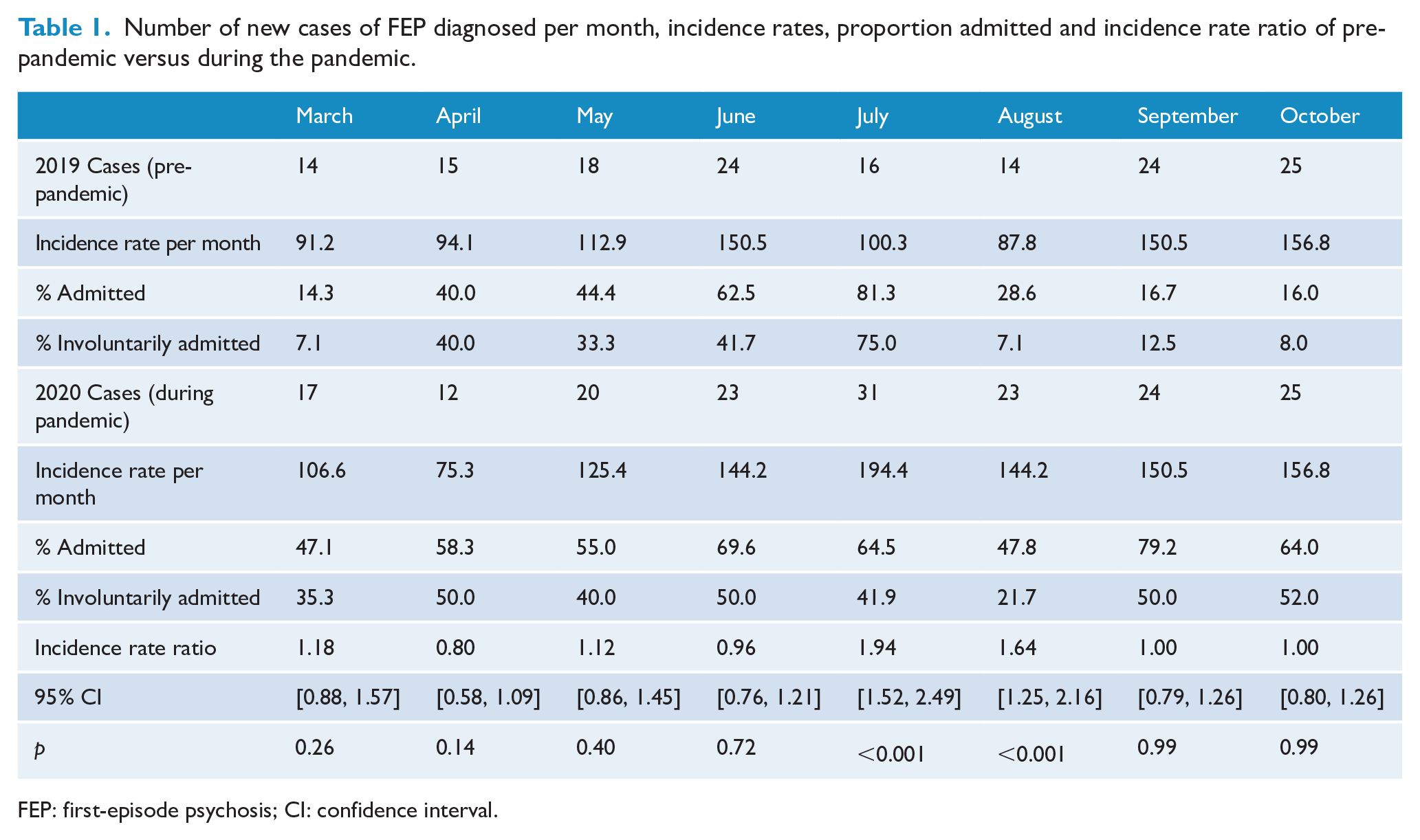
FEP: first-episode psychosis; CI: confidence interval.
Demographic characteristics of young people presenting with an FEP before and during the pandemic.
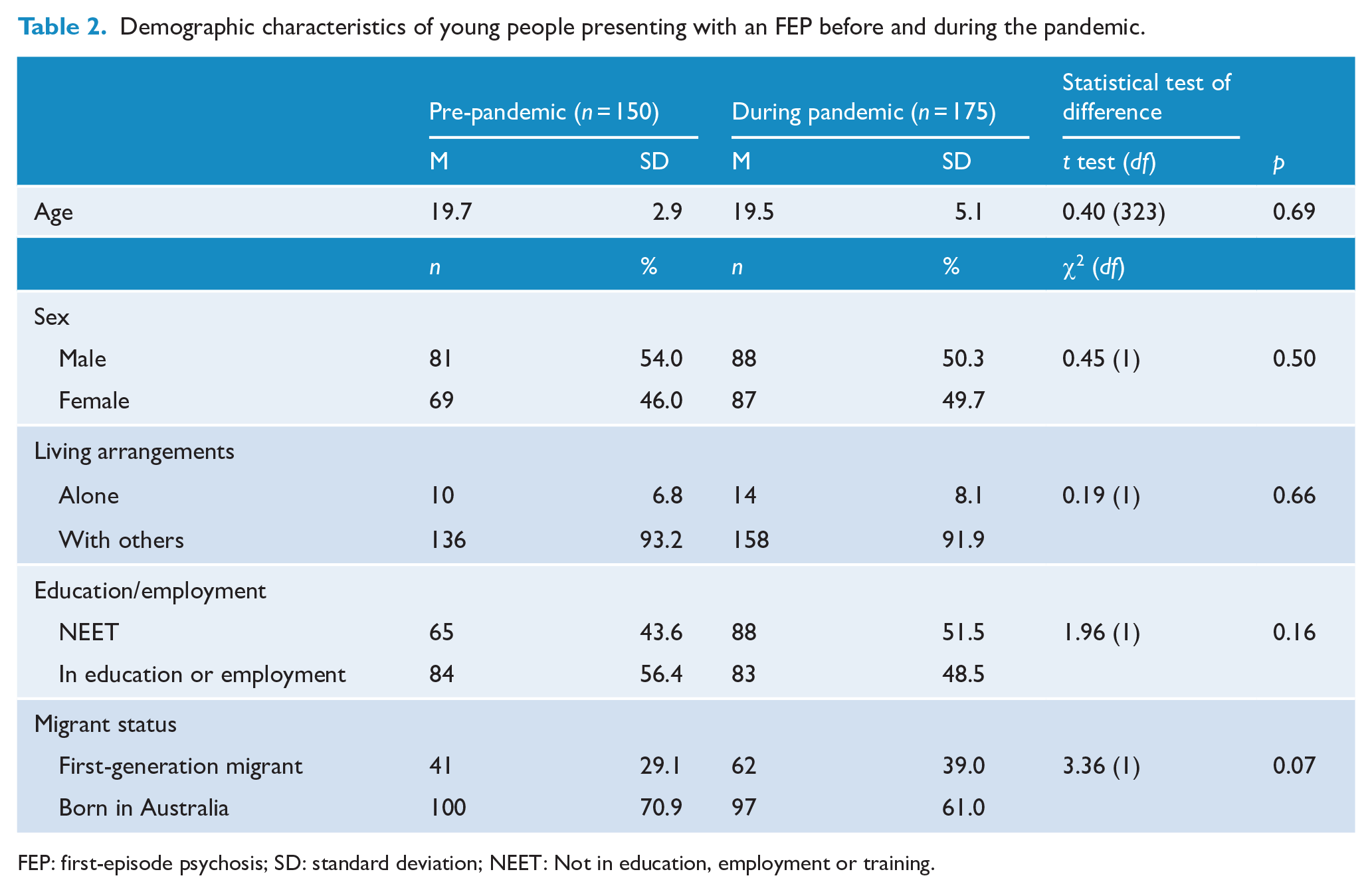
FEP: first-episode psychosis; SD: standard deviation; NEET: Not in education, employment or training.
Admission rate and legal status of admissions
In the period of 1 March 2019 to 31 October 2019, 37.3% (n = 56) of young people presenting with an FEP were admitted to hospital, compared to 61.7% (n = 108) during the pandemic and period of 1 March 2020 to 31 October 2020 (OR = 2.71, 95% CI = [1.73, 4.24]). This finding remained consistent when controlling for demographic factors (sex, age, living arrangements and employment/educational status). However, the OR reduced to 2.09 (95% CI = [1.23, 3.56]) when controlling for clinical factors, specifically self-harm or suicidality and substance abuse (Table 3).
ORs for admission to hospital before and during the COVID-19 pandemic.
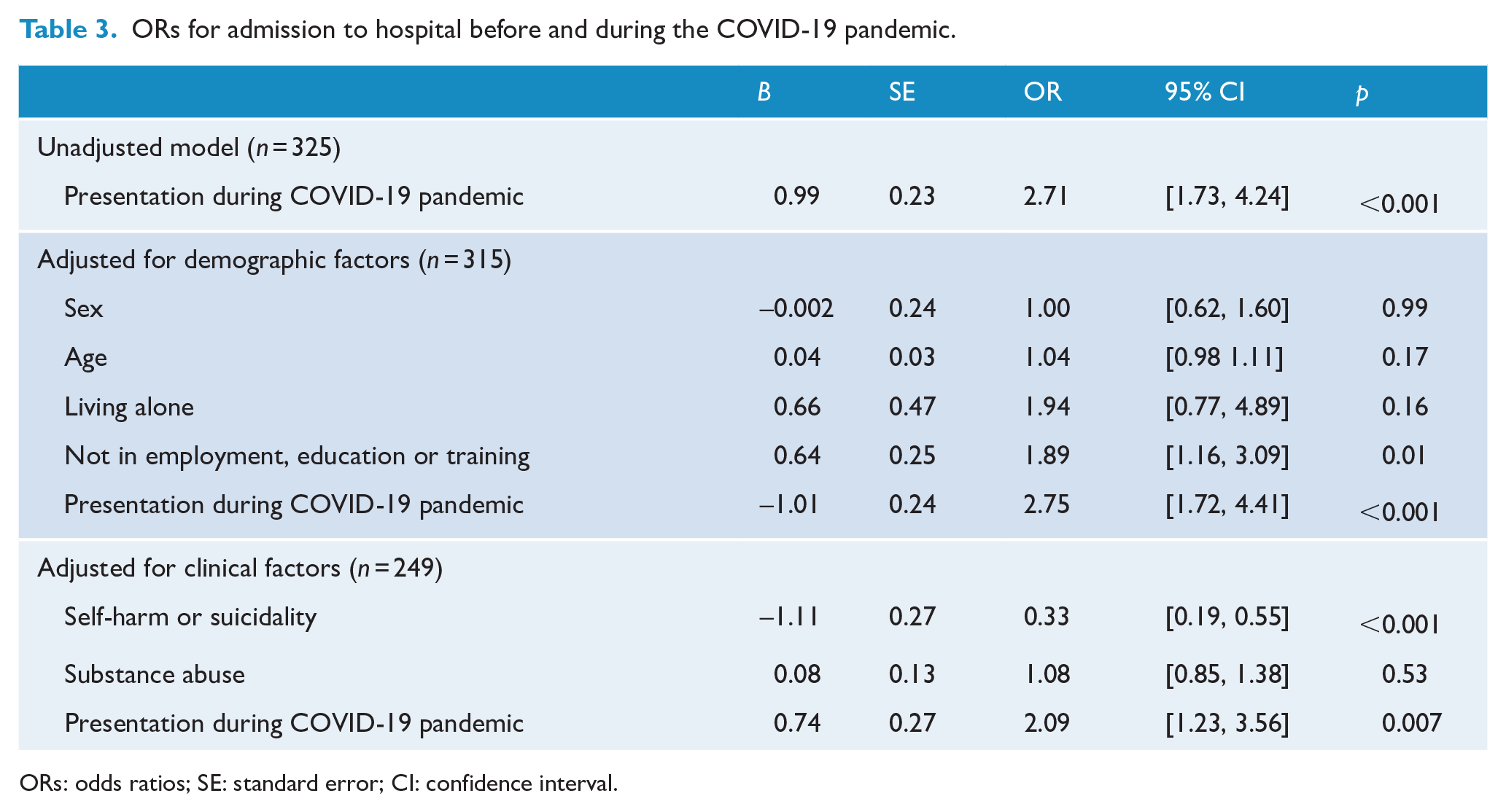
ORs: odds ratios; SE: standard error; CI: confidence interval.
In relation to the legal status of the admissions, in the period of 1 March 2019 to 31 October 2019, 27.3% (n = 41) of young people presenting with an FEP were admitted involuntarily to hospital, compared to 42.5% (n = 74) in the period of 1 March 2020 to 31 October 2020 (OR = 1.97, 95% CI = [1.23, 3.14]). This finding did not attenuate when controlling for demographic factors; however, the OR reduced when controlling for suicidality and substance abuse (OR = 1.56, 95% CI = [0.89, 2.76]).
The number of new cases per month was not correlated with the proportion of cases who were admitted to hospital (rs = 0.26, p = 0.33) or the proportion who were admitted involuntarily (rs = 0.19, p = 0.49) in the same month.
Discussion
Summary of findings
The main findings of this study are that while the overall incidence of FEP did not statistically significantly change during the pandemic, there was a change in the pattern of presentation of cases, with an immediate decrease in detection of cases followed by a subsequent upswing in presentations, in later months. There was also an increase in the proportion of young people admitted to the service’s inpatient unit at the time of presentation with an FEP, including involuntary admissions.
Possible explanation of findings
The findings of a decrease in the number of presentations immediately after the pandemic restrictions were put in place in Victoria are not surprising, as there was a decrease in attendance at the typical places where psychosis is detected, namely, emergency departments (Mitchell et al., 2020), schools and universities (Graves et al., 2021)and general practitioners (Homeniuk and Collins, 2021). While not statistically significant, there was a higher number of cases detected during the pandemic compared to the corresponding period in the previous year. There were approximately 14% more cases over this time period, which is substantial, but as this study was confined to one clinical service, it is likely to be underpowered to detect a statistical difference. Furthermore, the incidence of psychotic disorders is relatively low and therefore it would be unlikely to observe a large change in a short period of time, within one service. It also needs to be considered that the incidence of FEP is not temporally stable, as we have found increases of up to 33% in the incidence of FEP in this catchment area when comparing the incidence across different years (Pignon et al., 2021). Therefore, even if statistical differences had been observed, we could not have attributed them solely to the COVID-19 pandemic or the associated restrictions.
Perhaps the most striking finding is the much higher proportion of young people with an FEP at presentation being admitted, both voluntarily and involuntarily, during the pandemic. The odds of being admitted were nearly threefold during the pandemic and nearly twofold for involuntary admissions compared to the pre-pandemic period. While the study design could not identify the reasons for higher admission rates, there are several possible explanations. First, the severity of psychotic symptoms may have increased during the pandemic, possibly because of delays in help seeking and referral (and therefore longer duration of untreated psychosis (DUP)). Interestingly, risk to self is one of the clinical indications for admission to hospital, but in this study, the presence of either self-harm or suicidality reduced the odds for admission during the pandemic (Tables 3 and 4). Again, it cannot be determined with this study design, but this finding lends support to the theory that the increased rate of admission was due to severity of symptoms (rather than symptoms being associated with risk).
ORs for involuntary admission to hospital before and during the COVID-19 pandemic.
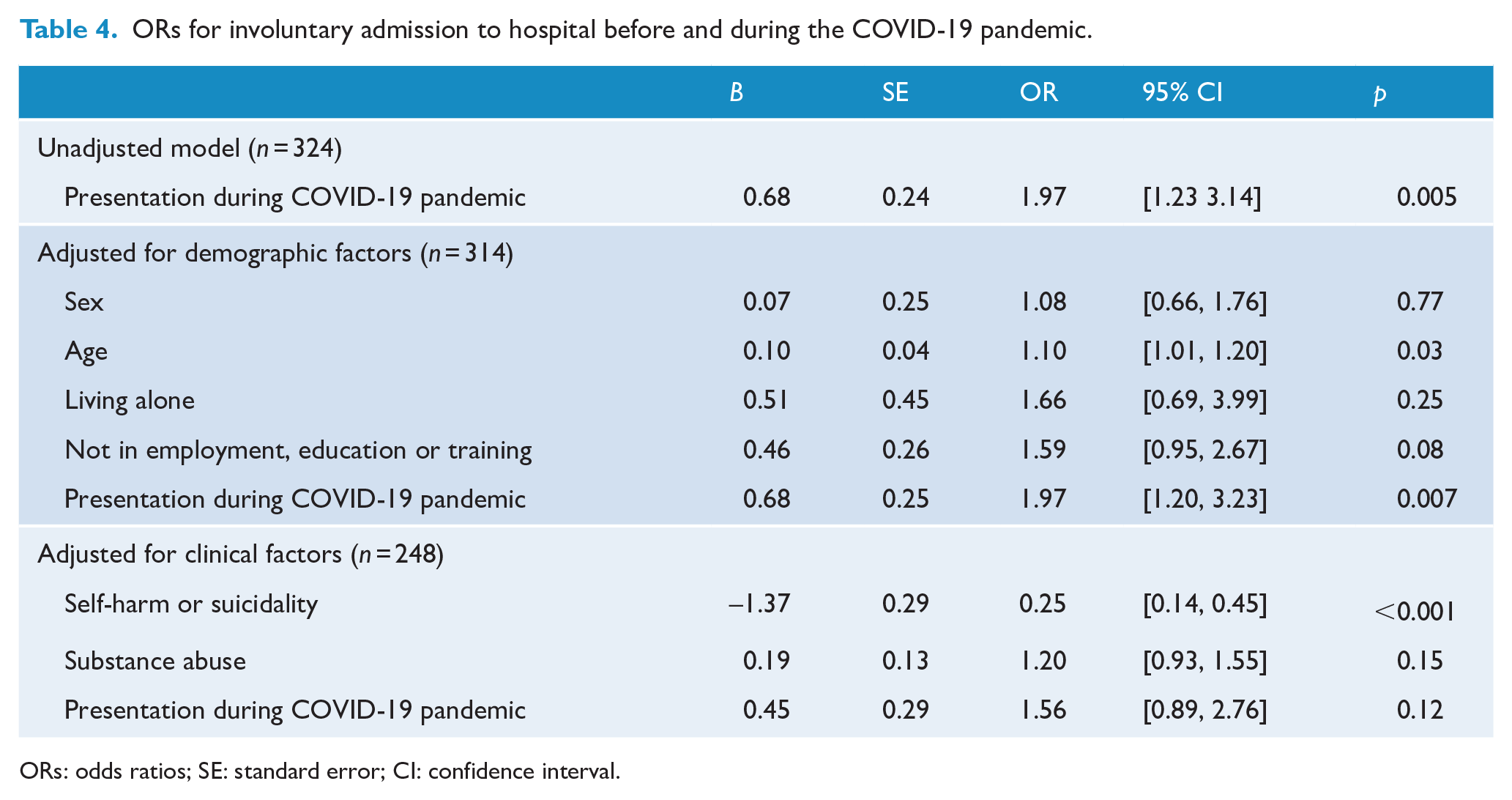
ORs: odds ratios; SE: standard error; CI: confidence interval.
Second, during the pandemic, there was a change in how the clinical service delivered treatment, which may have led to higher rates of admission. Telehealth facilities were introduced across the clinical service and there was also a higher threshold to conduct home-based treatment, due to the potential risks it posed to both staff and patients. Furthermore, the quarantining of staff who were close contacts of COVID-19 cases and the grouping of staff into separate teams to reduce contact among staff also led to a reduction in the ability to conduct home visits. Therefore, it may have been required to admit young people with an FEP to hospital, who may otherwise have received intensive home treatment. In addition to this, as observed in Figure 1, there was an initial decrease in presentations in April 2020, after the pandemic restrictions had been introduced and there was a subsequent upswing in presentations, which peaked in July and August 2020. While there was no significant increase in the overall incidence, the clinical services still had to provide care for up to twice as many cases in some months compared to the previous year. With the already reduced staff load available, this is a further reason why intensive home-based treatment could not be provided, which may also have contributed to the higher hospital admission rate. In addition, these figures represent the treated cases of FEP and it is possible that during the periods of heightened demand upon the clinical services, it is possible that young people with an FEP were directed towards private providers.
It is also possible that during the pandemic, families and caregivers may not have been able to provide the intensive support that is required for home-based treatment due to other commitments, such as homeschooling or their own increased stress during the pandemic.
Finally, it is understandable that during a pandemic, young people would be reluctant to be admitted to hospital, as the nature of an admission would result in coming in close contact with other patients and staff. Hence, it may have been more difficult to persuade a young person to be admitted to hospital and this may explain the higher rate of involuntary admission.
Clinical implications
The location and context of the service need to be considered when interpreting these results. While the State of Victoria, which has a population of nearly 7 million, recorded just over 20,000 cases of COVID-19, this is a small proportion of the overall population, in comparison to the proportion of populations infected in other countries during the pandemic (Department of Health and Human Services, 2021). However, in order to achieve this low infection rate, a strict lockdown was imposed that, at the time, was one of the longest in the world (Scott et al., 2021). Therefore, the results of this study reflect this situation. We did not observe a significant increase in the incidence of FEP. However, if it is expected that the cause of an increase in incidence would be from post-infection cases, then it is unsurprising the incidence did not increase, as the case numbers of COVID-19 were relatively low. In addition, the overall risk of a psychotic disorder post-COVID-19 is relatively low, with 1.40% (95% CI = [1.30, 1.51]) of individuals developing a psychotic disorder within 6 months of COVID-19 infection (Taquet et al., 2021). Conversely, the admission rate is more likely to be a result of help-seeking behaviour, access to care and the ability of the health service to respond in a timely manner with intensive inputs, all of which were impacted by the restrictions imposed to control the spread of the virus. As the restrictions were intensive and prolonged in the jurisdiction in which study was conducted, it may be less surprising that the main findings of this study relate to the dramatically increased admission rates and involuntary admission orders. This study also replicates the findings from Switzerland and Germany, which also found that involuntary admission increased during the COVID-19 pandemic, although this related to all psychiatric presentations and not just psychotic disorders (Ambrosetti et al., 2021; Fasshauer et al., 2021).
While it is hoped that further severe restrictions, such as lockdowns, will not be necessary following successful vaccination programmes, they may still occur in the future. In the event of such restrictions, EI for psychosis services should anticipate that help seeking may be affected and examine local means by which to ensure that any delays are reduced, in order to have a continuous pattern of referrals. At the EPPIC EI service, where this study was set, a ‘hospital in the home’ service was being established and was operational from the time just after the study period ended. This ‘hospital in the home’ service aims to deliver an equivalent level of care as an inpatient setting, such as being seen at least twice a day, in the young person’s home and offers a realistic alternative to an inpatient admission.
Strengths and limitations
The findings of this study need to be considered within its limitations. First, we were limited in the comparisons we could make between time periods, as we could only compare the routinely collected demographic and clinical information that had been collected prior to the pandemic. Second, we did not have a measure of the duration of untreated psychosis, which would have informed us whether there had been help-seeking delays during the pandemic. Third, we could only access data relating to the at-risk population from the 2016 census, and it is likely that the population had changed in the years after this census; we could also not account for any changes in the at-risk population between 2019 and 2020. In addition, the incidence of psychotic disorders is relatively low, and therefore this study was underpowered in order to observe even a modest change in this incidence. Furthermore, as the rate of COVID-19 in the general population in the study setting was relatively low in this period, it would have been unlikely to change in the incidence of psychotic disorders as a result.
Conclusion
There was a mild increase, that did not reach statistical significance, in the incidence of FEP, and the pattern of presentation changed substantially, with twice as many cases presenting in the later months of the restrictions as would have been expected. There was also a significant increase in both voluntary and involuntary hospital admissions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.