
Abstract
Objective
Investigate the treatment patterns and prescribers of stimulants for attention deficit hyperactivity disorder (ADHD) in young people in New South Wales (NSW).
Method
Longitudinal cohort study of persons born after 1983 and prescribed stimulants for ADHD as per the NSW Ministry of Health Controlled Drugs Data Collection. Results were analyzed descriptively: a) treatment prevalence by year; age; sex; b) speciality of prescribers over time; c) rate of transition from paediatrics to adult psychiatry. The main analysis covered 2003–2015, with data on general practitioner prescribing to 2023.
Results
Treatment prevalence rates were highest at age 10 (22.8 per 1000 person years), declining among teenagers and stabilizing in adulthood at 2.5 per 1000. The childhood male treatment predominance (4:1) resolved to 1.6:1 in adulthood. Paediatricians were the main prescribers until age 20. The average annual percent increase in prescribers was: adult psychiatry – 13%, general practice – 20%, paediatrics – 2.6%. Only 6.3% of treated children had transitioned to adult psychiatrists by age 25; 50% starting treatment with adult psychiatrists had no previous treatment records.
Conclusions
The proportion on treatment and the male predominance declined substantially with age. Future studies may determine whether increased prescribing by general practitioners and psychiatrists reduces treatment attrition during adolescence.
Attention deficit hyperactivity disorder (ADHD) is a major public health problem in Australia. In 2019, the total social and economic costs of ADHD in Australia were estimated to be $20.4 billion. 1 There is ample evidence that while treatment with medication is effective for improving symptoms in people of all ages with ADHD, 2 resources available for people seeking treatment are inadequate.3,4 In 2023 a senate inquiry supported by 700 submissions from all over Australia highlighted inadequate services, 3 particularly for adults seeking treatment within the public sector. In 2019 the Review of Health Services for Children, Young People and Families within the NSW Health System (Henry Review) identified increasing rates of diagnosis of ADHD had led to unmanageable workloads within the public sector and that new models of care were needed.3,4 A survey of general practitioners (GPs) published in 2023 highlighted ongoing issues with referral pathways in NSW for children and adults with ADHD. 5
Treatment usually involves a combination of medication and non-medical management such as psychological counselling. 6 The most frequently prescribed medication for ADHD in Australia is methylphenidate for children. 7 In 2022 lisdexamfetamine replaced dexamfetamine as the preferred medication for adults following changes to the Pharmaceutical Benefits Scheme listing in 2021 that supported its use in adults.7,8
Australian data document relatively short periods of treatment (2–2.5 years in South Australia 9 ) and in NSW a growing proportion with intermittent treatment. 10 This means that the population prevalence of ADHD cannot be estimated reliably from the treatment prevalence.
The transition from paediatric to adult mental health services is a critical time when continuity of care is important11,12; for young people with ADHD in NSW this transition occurs between ages 16 and 25. 13 However, some adult psychiatrists may not accept referrals for individuals aged less than 18 and public mental health services may exclude ADHD.3,14 A 2015 national survey found that only 34.6% of Australian adolescents aged 12–17 years with mental disorders (including ADHD) had their needs fully met. 15 More recent data emphasizes an Australia-wide deficiency in specialist services for people with ADHD and a perception of inadequate training for GPs to be able to close this gap.5,16 A 2020 survey of South Australian psychiatrists found that 32.9% felt that their training was deficient for managing adults with ADHD and 58.9% would not accept such referrals. 14
The aim of this database study was to investigate the patterns of treatment and prescribers of stimulants for ADHD in young people in NSW from childhood to early adulthood, with particular focus on evidence that might be consistent with a treatment bottleneck at transition to adult services. This has not been fully covered in previous studies and is currently highly topical. The specific aims were to analyze descriptively a) the treatment prevalence by year, age and gender ratio; b) rate of change in number of prescribers by medical speciality over time; and c) rate of transition from paediatrics to adult psychiatry.
Methods
Study population and setting
All individuals born from 1st January 1984 with records of stimulant treatment for ADHD in NSW, Australia.
Stimulant prescribing in NSW
The NSW Pharmaceutical Regulatory Unit allowed two methods of prescribing of stimulants for ADHD: prescribing using general authorization or the prescriber applying for an individual patient authority. General authorization was provided for paediatricians to initiate stimulants for ADHD in children aged 4 to 18 years and to continue treatment up to age 25. 17 Psychiatrists were allowed general authorization to treat patients up to age 70 years. Until 2016, to use this general authorization, prescribers submitted a monthly report to the NSW Ministry of Health detailing each prescription written. Doctors permitted to prescribe stimulant treatment for ADHD, but without general authorization (such as GPs), or those prescribing outside criteria 17 (such as outside the specified dose or age ranges), applied for an individual patient authority.
Data sources
Data on stimulant medication authorizations and prescriptions are recorded in the NSW Ministry of Health’s Controlled Drugs Data Collection (CoDDaC) database. This includes clinician applications to prescribe medications and their reporting of individual prescriptions written. Records of individual patient authorizations were available from 1985 up to December 2019. CoDDaC includes information on patient age, sex, the stimulant drug and dose prescribed and the speciality of the prescriber. Records include a unique patient study number to track treatment longitudinally to the end of follow-up and a unique prescriber study number to identify prescribers and potential patient transitions between providers. General authorization commenced in 1996 and ceased being recorded in CoDDaC in May 2016, therefore the main analysis covered only the period 2003–2015. Analysis of GP prescribing was extended until 2023 using individual prescription authorization data and additional summary data, on GP prescribing, available until December 2023.
Patients were considered ‘covered’ by a given stimulant authorization from its issue date to its expiration date: six months for a general authority and twelve months for an individual patient authority. Four specialities were examined for this study: paediatrics, child and adolescent psychiatry, adult psychiatry, and general practice. The transition from paediatrician to adult psychiatrist was identified as the primary transition pathway of interest.
Data analysis
Treatment prevalence rates were calculated by treatment year, patient age and sex, and by prescriber speciality using single year population estimates by age from Australian census data as denominators. At the prescriber level, the number of unique prescribers treating patients each year as well as the median annual ADHD patient caseload, defined as the number of unique patients per prescriber per year, were calculated by prescriber speciality.
Transitions were examined two ways: (1) comparing rates of new patients and former paediatric patients aged 16 or over beginning care with an adult psychiatrist; and (2) calculating the percentage of patients ending paediatric treatment who transitioned to an adult psychiatrist by age 25. This final analysis required restricting to patients with follow-up to at least 25 years of age.
Trends over time were examined using joinpoint analysis to fit multiple continuous linear segments to the study data, calculating the annual percent change (APC) for each identified segment and an average APC (AAPC) for the full time period. The best fitting number of segments and location of their joinpoints were identified using the grid search method and weighted BIC measure for model selection. 18
All analyses were performed using SAS 9.4 software (SAS Institute, Cary, North Carolina, USA) and Joinpoint 5.0.2 software (National Cancer Institute, Maryland, USA). Ethics approval was granted by the NSW Population and Health Services Research Ethics Committee (ref 2020/ETH00931).
Results
A total of 113,387 unique individuals (77% male) had recorded stimulant treatment for ADHD between 1986 and 2019 from a total of 2723 unique prescribers. Paediatricians, psychiatrists and GPs comprised 89.6% of prescribers, with the remainder either being unrecorded or from another speciality. The modal age for starting treatment was 7 years and for ending treatment was 14 years. Figure 1 shows the treatment rates for children (aged 2–17 years) and adults (aged 18 years and older) based on individual and general authority. The majority of patients were identified from general authority prescription records until 2016 when such recording ceased. Given the cohort definition including only individuals born from 1984, adult patients were not identified in the dataset until 2002/2003. We have therefore limited the main body of our analyses to treatment in years 2003–2015, apart from the GP prescribing data which was available to 2023. Treatment rates for children (aged 2–17 years) and adults (aged 18 years and older) based on individual and general authority 1986–2019. Given the date of birth from 1984 onwards, there were no adults in the cohort until 2002.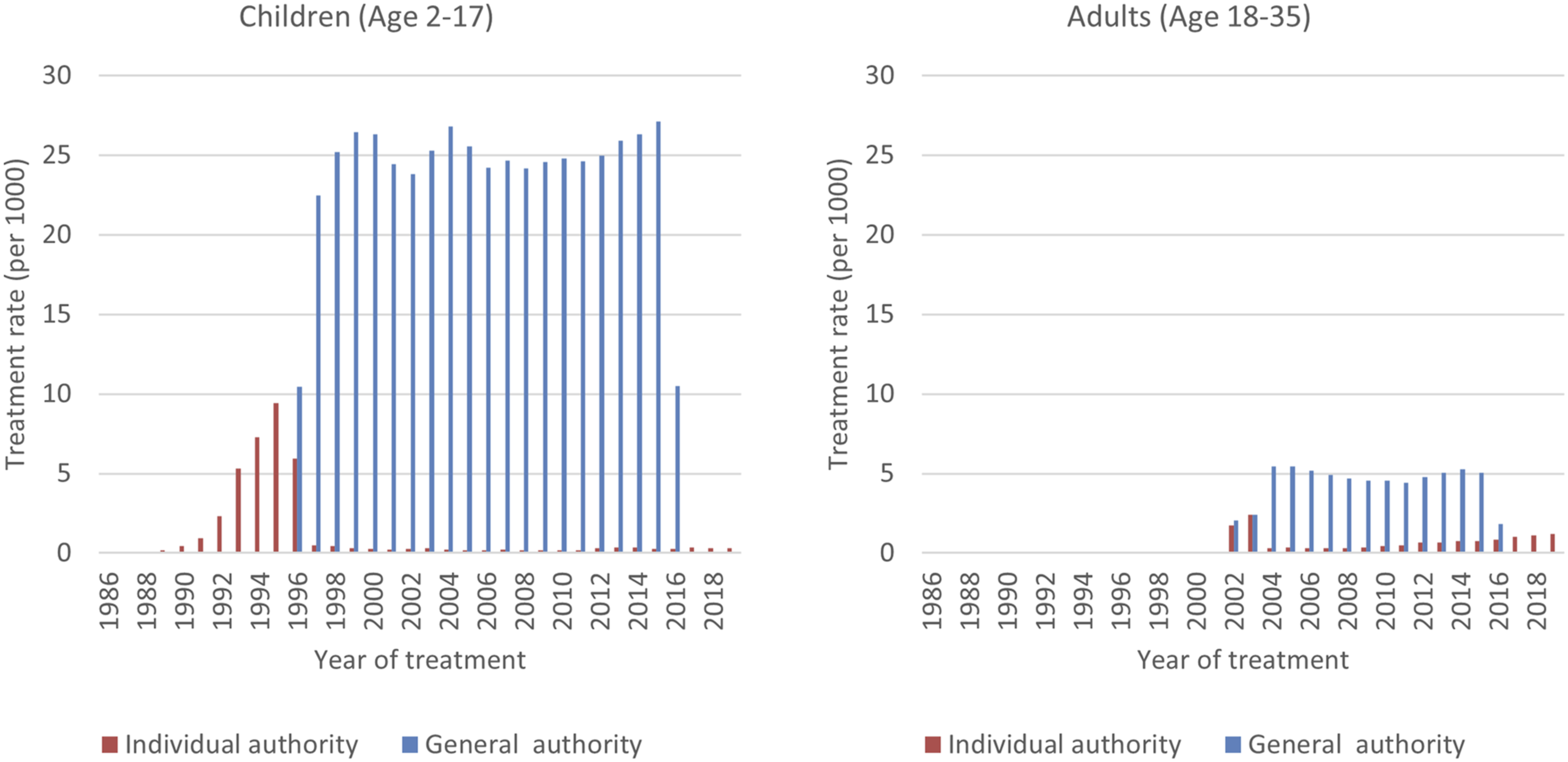
Between 2003 and 2015, the highest treatment prevalence was 22.8 per 1000 person years at age ten (Figure 2) with a predominantly male cohort (>3.5:1). The treatment prevalence declined rapidly during the high school years, stabilizing in adulthood at around 2.5 per 1000 person years. The ratio of males to females declined from more than 4:1 in the preschool years to 1.6:1 by age 25. Treatment prevalence did not increase among children during this time period, but did increase among adults, particularly those aged 19–21 (AAPC 6.9%) and 22–24 years (AAPC 12.4%) (Table S1). Treatment prevalence by age: 2003–2015.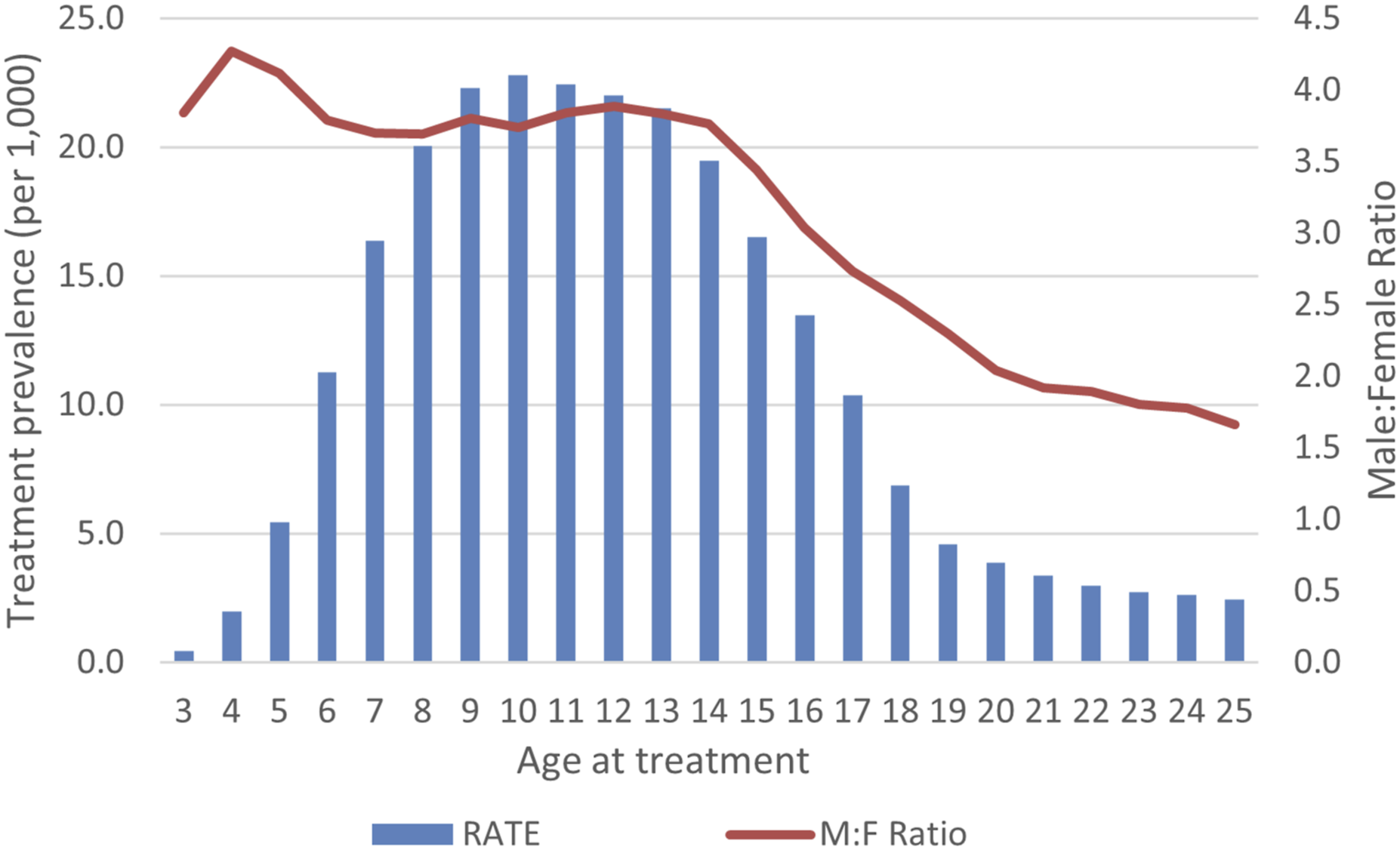
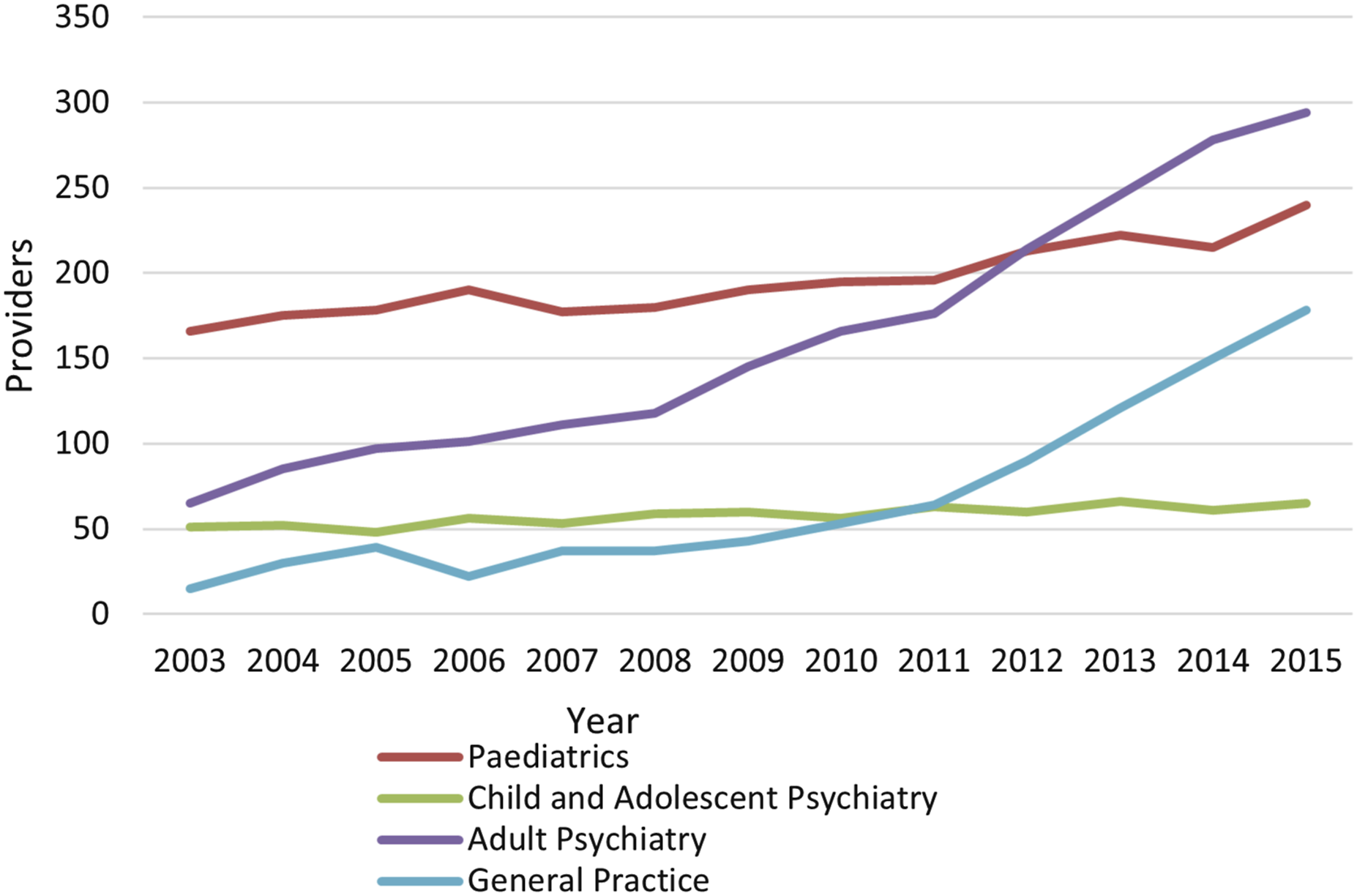
Between 2003 and 2015, the number of unique prescribers increased in all specialities (AAPC adult psychiatry 13%, general practice 20%, paediatrics 2.6%, child and adolescent psychiatry 2.2%) (Figures 3 and 4, Table S2). GP prescribers by year: 2003–2023. Average annual percent increase (AAPI) in number of prescribers by speciality: 2003–2015.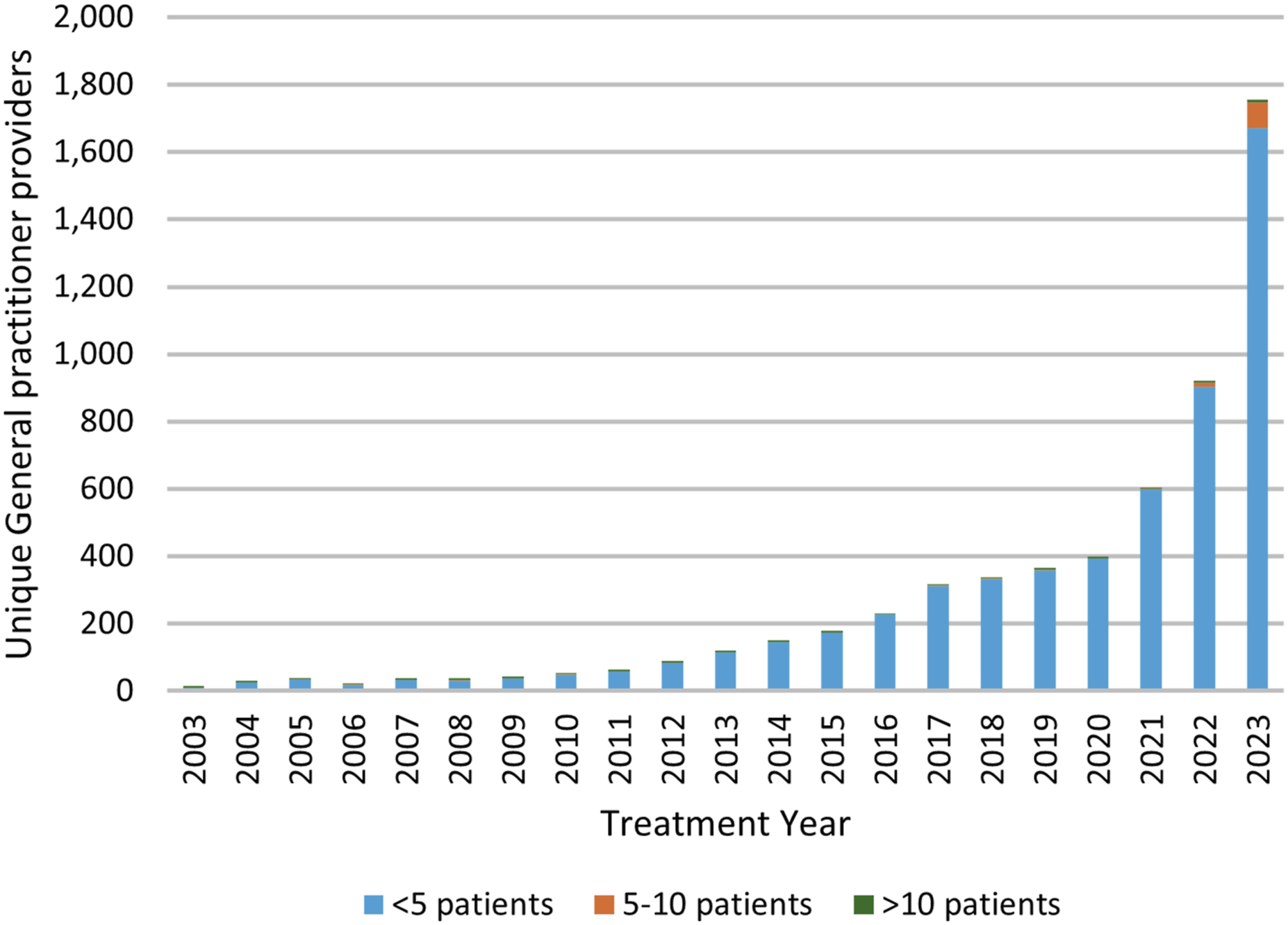
The additional data on GP prescribing gave an APC of 21.5% unique prescribers for the period 2003–2021, accelerating to 75.8% from 2021–2023. The number of GPs in NSW with an ADHD caseload of more than 10 patients increased to 9 in 2023, having remained stable at 3–5 for two decades (APC 46.8% 2021–2023) (Figure 3, Table S3, Table S4).
Paediatricians treated more unique ADHD patients than other prescribers, with a median caseload of 46 patients (interquartile range (IQR) 12, 133) per prescriber per year. By contrast, child and adolescent psychiatrists and adult psychiatrists treated a median caseload of only 7 patients (IQR 2, 26) and 3 patients (IQR 1, 7) per year, respectively. General practitioners had the smallest average median caseloads of only 1 patient (IQR 1, 3). These caseloads remained stable over the study period, except for those of adult psychiatrists which increased an average of 14% per year from 2007 to 2015 (Table S4). Paediatricians were the predominant prescribers overall and treated more patients at all ages up to 20, after which adult psychiatrists were the predominant prescribers (Figure 5). Treatment prevalence by patient age showing speciality of the prescribers: 2003–2015.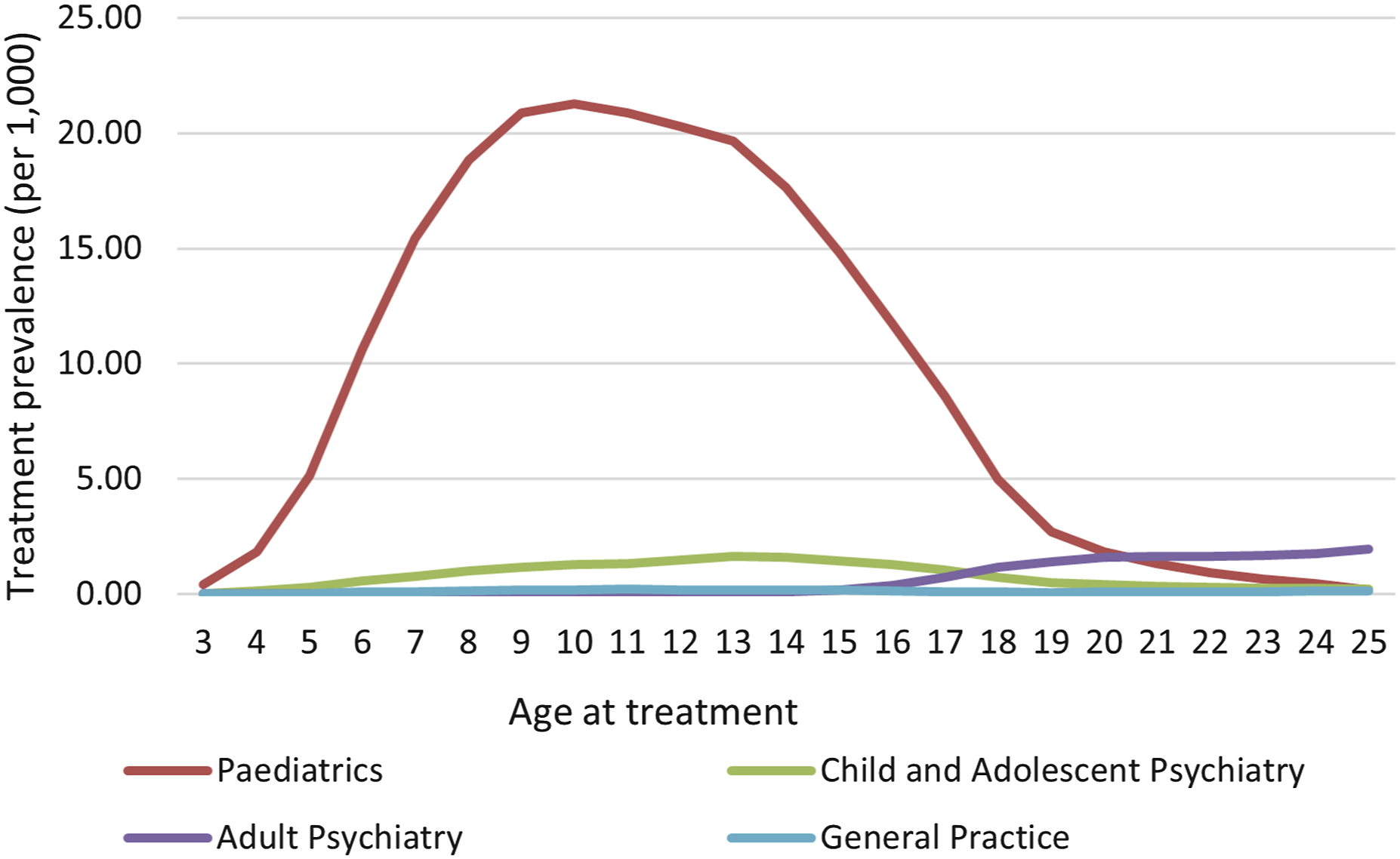
Between 2003 and 2015, a total of 6781 patients aged 16 or over commenced receiving treatment from adult psychiatrists (Figure S1). Half of these (50.4%) had previous recorded treatment; 46.1% had previously been treated by a paediatrician. Out of a total of 25,324 patients treated for ADHD by a paediatrician, the majority (23,589, 93.1%) had not transitioned to adult psychiatric care by age 25 years (Figure 6). The 1735 who did transition represented 6% of the males and 9% of the females treated by paediatricians, giving a transitioning cohort that was 75% male. Of those newly treated by adult psychiatrists, 62% were male. The percentage of patients who transitioned to adult psychiatrist care increased with the age of last paediatric treatment, from 4% at age 12, to 13% at age 18 and 35% at age 25 years. The percentage of patients transitioning to adult psychiatric treatment remained stable over time in all age groups apart from those ending paediatric treatment aged 19–21, where the percentage increased an average of 11.4% (95% CI 6.5, 16.7) per year (from 12.2% in 2009 to 24.2% in 2015) (Table S3). Of the 2298 patients who had transitioned to adult psychiatrists by age 25, only 28% had either continuous treatment or a gap in treatment of no more than 1 year. Transition to adult psychiatry by age (year) at last paediatric treatment: 2003–2015.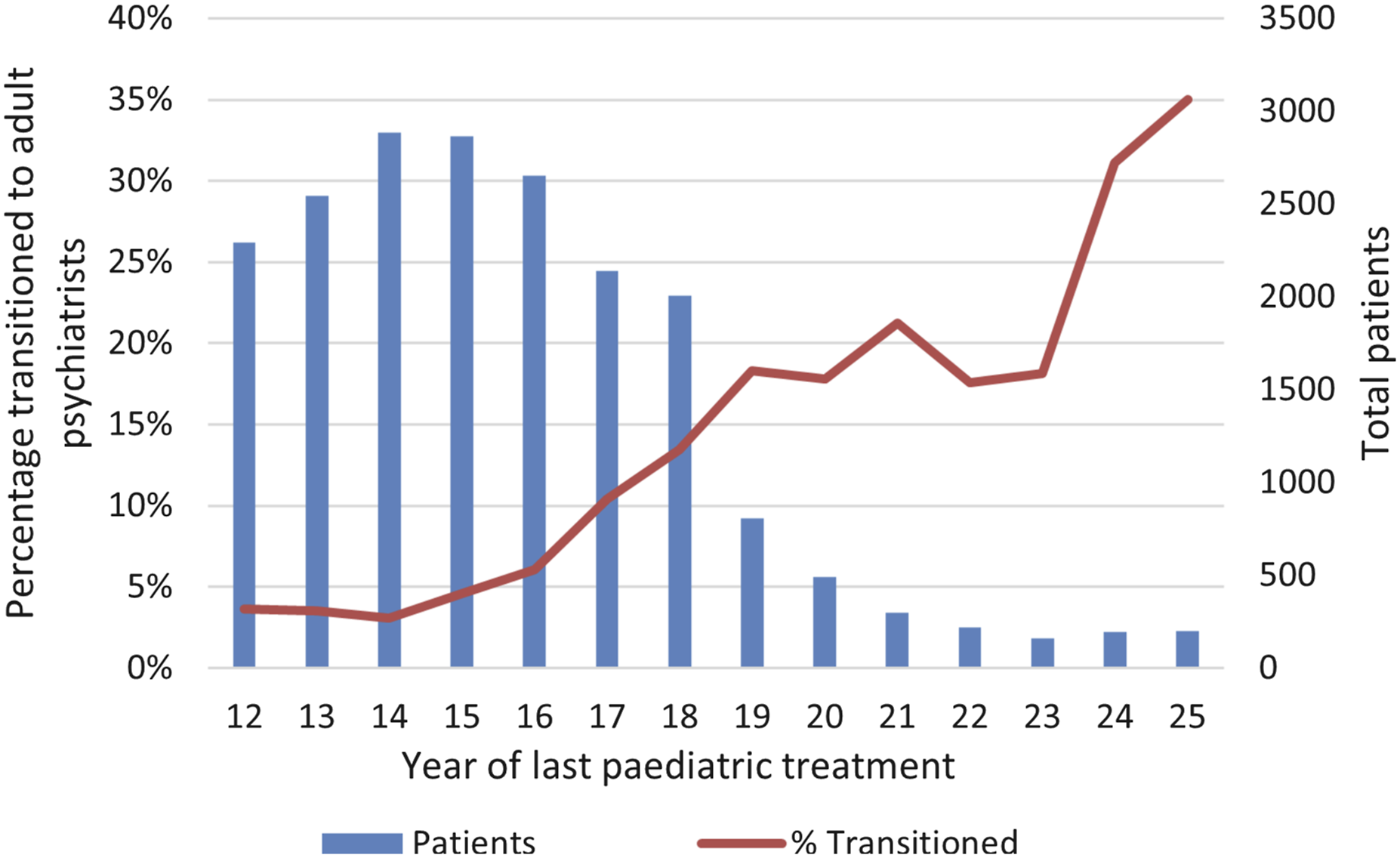
Discussion
The modal age of ADHD treatment initiation in NSW was 7 years. The highest treatment prevalence was 22.8 per 1000 person years at age 10, declining among teenagers and stabilizing in adulthood at 2.5 per 1000 person years. The male predominance in early childhood resolved to almost parity in adulthood. Despite an increasing number of GP and adult psychiatrist prescribers over time, paediatricians treated the majority of patients, even in early adulthood to age 25. It was only once people were aged over 20 that they were more likely to be treated by an adult psychiatrist. Only 6% of those treated in childhood had transitioned to adult psychiatrists by age 25; half of those starting treatment with an adult psychiatrists had no previous treatment records.
The doubling in ADHD treatment prevalence from 2013–2020 documented from Australian population-based prescribing data 8 was not observed in our study as the main analysis only went up to 2015. However, the age of the highest treatment prevalence was comparable (children aged 6–12).
Previous analyses of the CoDDaC database from 1990–2000 documented that treatment was typically intermittent and relatively brief.10,19 The mean duration of treatment declined from 3.8 years in 1993 to 0.9 years in 2010. 10 The median treatment survival time from 1990–2000 was 1.96 years 19 ; the median gap between treatment episodes was 3.03 years. 10 Our study includes more recent prevalence data and includes the medical speciality of the prescribers, up to 2015 for specialists and 2023 for GPs.
The substantial variation in treatment prevalence and gender balance with age, together with the substantial proportion of treated adults who were apparently newly diagnosed with ADHD in adulthood, appears inconsistent with the concept of ADHD as a neurodevelopmental disorder that is continuous across the lifespan. However, the clinical presentation of ADHD is variable, and depends on a complex interaction of a person’s ADHD-related deficits, their cognitive strengths and their social environment.20,21 It has been suggested that the diagnosis of ADHD is skewed towards hyperactive boys, with relative under-diagnosis of girls. 22 The decline in treatment prevalence in adolescence may be related to a reduction in the expression of the symptoms of ADHD, particularly hyperactivity which often diminishes with maturation. 23 Therefore a person with a childhood diagnosis may no longer meet the diagnostic criteria as they approach adulthood and this, coupled with the development of skills and coping strategies, may lead to symptomatic improvement and treatment cessation. This improvement is sometimes considered remission of ADHD. 24 However, as the responsibilities and functional expectations increase into adulthood, there is more scope for the appearance of ADHD-related functional impairment. Those first diagnosed as adults tend to have a higher IQ 24 and to be predominantly female. 25 This suggests that higher ability and being female might reduce the expression of ADHD in childhood, such that a greater proportion of females are diagnosed as adults.
Our longitudinal data showed that 93.7% of the cohort treated for childhood ADHD were untreated as adults, at least to the age of 25 years. This would conflict with longitudinal clinical data suggesting that 41% of those diagnosed in childhood are still impaired as adults. 26 The observed changes in treatment prevalence at different ages could relate to under-treatment and/or discontinuous treatment,8,10,19 due either to choice (including medication refusal by oppositional adolescents) or to limited access to ADHD treatment. Until November 2023, NSW legislation mandated involvement of a psychiatrist in the treatment of adults with ADHD, with paediatricians unable to transition young adults to their GPs for ongoing treatment. A shortage of psychiatrists treating adult ADHD 14 might explain the anomaly of paediatricians continuing to treat adults, sometimes up until age 25.
A strength of the study is the statewide population-level data on a large cohort followed longitudinally from childhood to adulthood. We were also able to track a young person’s course between different prescribers over time. However, we were unable to determine whether the dramatic increase in GP prescribing from 2020–2023 was replicated among paediatricians or psychiatrists.
In common with other database studies, it was unknown which patients actually took the authorized medication. Treatment that was started (or restarted) after the age of 25 and treatment prescribed in other states was not included. Although we had data on GP prescribing up to 2023, data entry of general authority prescriptions ceased after May 2016, which prevented examination of subsequent trends in treatment by paediatricians and psychiatrists. Lack of information on whether treatment was prescribed by public or private specialists meant that we were unable to comment on relative treatment capacity in public and private settings. Treatment using non-stimulant ADHD medications was not recorded; however, it is likely that the number of individuals missed for this reason would be small: ADHD treatment guidelines recommend that the first medication should be a stimulant unless medically contra-indicated. 6 In keeping with this, a study of community dispensing noted that of the non-stimulant ADHD medications, guanfacine and clonidine were mainly prescribed concurrently with stimulants and atomoxetine was rarely used. 8
The finding that paediatricians continued to treat ADHD into adulthood up to age 25 (the maximum age paediatricians were permitted to prescribe stimulants in NSW), together with the low rate of transition from paediatrics to adult psychiatry, could be consistent with a treatment bottleneck. Although our data cannot determine whether lack of accessibility contributed to the low rate of transition to adult psychiatrists, the recent Senate Inquiry reported families waiting for 2 years to see a psychiatrist for ADHD. 3
The number of prescribing GPs showed a dramatic increase, accelerating to an AAPC of 75.8% from 2021–2023. It is possible that some of this increase may relate to recommendations from the Henry Review (published 2019) being implemented with pilot studies involving GP prescribing for ADHD. 4
The marked increases in the number of prescribers among GPs and adult psychiatrists may in due course rectify the treatment bottleneck. However, it is important that doctors are adequately trained. We recommend that ADHD management should be considered essential to the curricula of the professional colleges. For those who are already practicing and whose training in ADHD may not have been adequate, we recommend regular use of the ADHD Prescribing Guide for Australian Healthcare Professionals. 27
Conclusions
In this longitudinal cohort of persons treated for ADHD, the proportion on treatment and the composition of the treated cohort changed substantially with age, with little overlap between those treated in childhood/adolescence and adulthood. Over time the predominant role of the paediatrician has been supplemented with more prescribers among psychiatrists and GPs. Future studies will determine whether this increased capacity enhances the rate of transition of adolescents and young adults to psychiatrists and GPs who can continue their treatment into adulthood.
Supplemental Material
Supplemental Material - Changing patterns of treatment and prescribers of stimulants for children, adolescents and young adults with attention deficit hyperactivity disorder in New South Wales, Australia: evidence for a treatment bottleneck? - A database study
Supplemental Material for Changing patterns of treatment and prescribers of stimulants for children, adolescents and young adults with attention deficit hyperactivity disorder in New South Wales, Australia: evidence for a treatment bottleneck? – A database study by Timothy C Nielsen, Ralph Nanan, Tony Butler, Natasha Nassar and Alison Poulton in Australasian Psychiatry
Footnotes
Acknowledgements
New South Wales Ministry of Health Pharmaceutical Services; CoDDaC Data Custodian
Author contributions
A.P. and R.N. conceived the study, N.N. contributed to the study design, A.P. and N.N. organized funding, A.P. organized the ethics with support from R.N., N.N. and T.B., T.N. analyzed the data with support from N.N., A.P. wrote the paper, all authors reviewed and contributed to the final version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Research Development Grant from the University of Sydney Brain Mind Centre and by a National Health and Medical Research Council (NHMRC) investigator grant (APP1197940). Prof. Nassar was supported by the Financial Markets Foundation for Children.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Poulton discloses personal fees and non-financial support from Shire/Takeda, outside the submitted work; and book royalties from Disruptive Publishing (ADHD Made Simple).
Ethics statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.