
Abstract
Objective
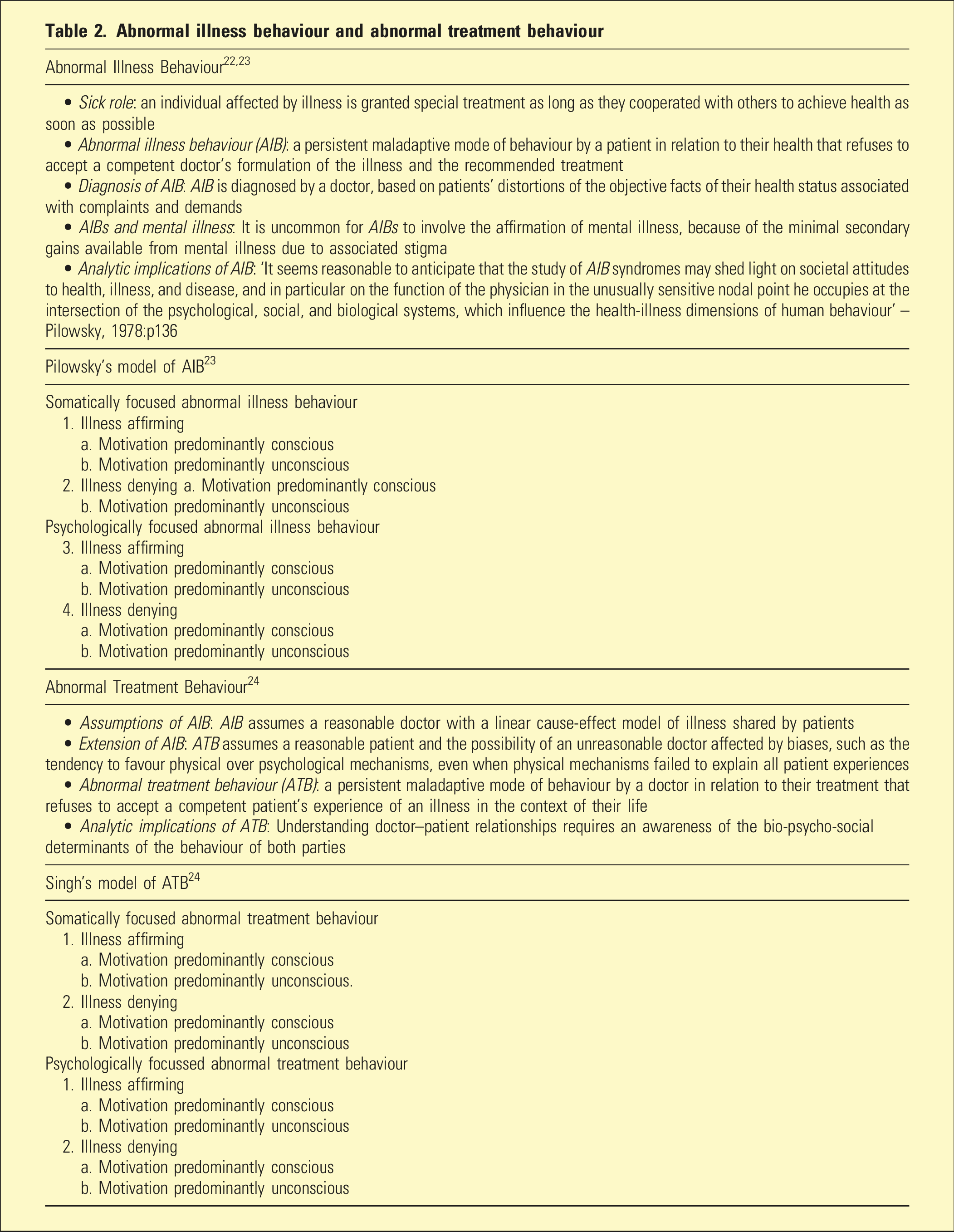
To describe the increasing number and changing demographics of patients presenting with gender dysphoria and provide an account of patient- and clinician-related factors which may have contributed to these changes. The concept of abnormal illness behaviours introduced by Pilowsky, and its extension to the concept of abnormal treatment behaviours by Singh, provides a framework for understanding healthy and pathological interactions between gender dysphoria patients and their doctors.
Conclusions
Abnormal illness behaviours driven by the reinforcing contingencies of gender-affirming care may explain, in part, the increasing number and changing demographics of gender dysphoria, as well as the increasing incidence of desistance and detransition. The under-diagnosis and under-treatment of mental health disorders by clinicians treating these patients are examples of abnormal treatment behaviours. Uncritical affirmation of patient reported gender identity appears likely to conceal unconscious motivations of some patients and clinicians, increasing the risks of harm to both.
Keywords
Definitions in gender medicine
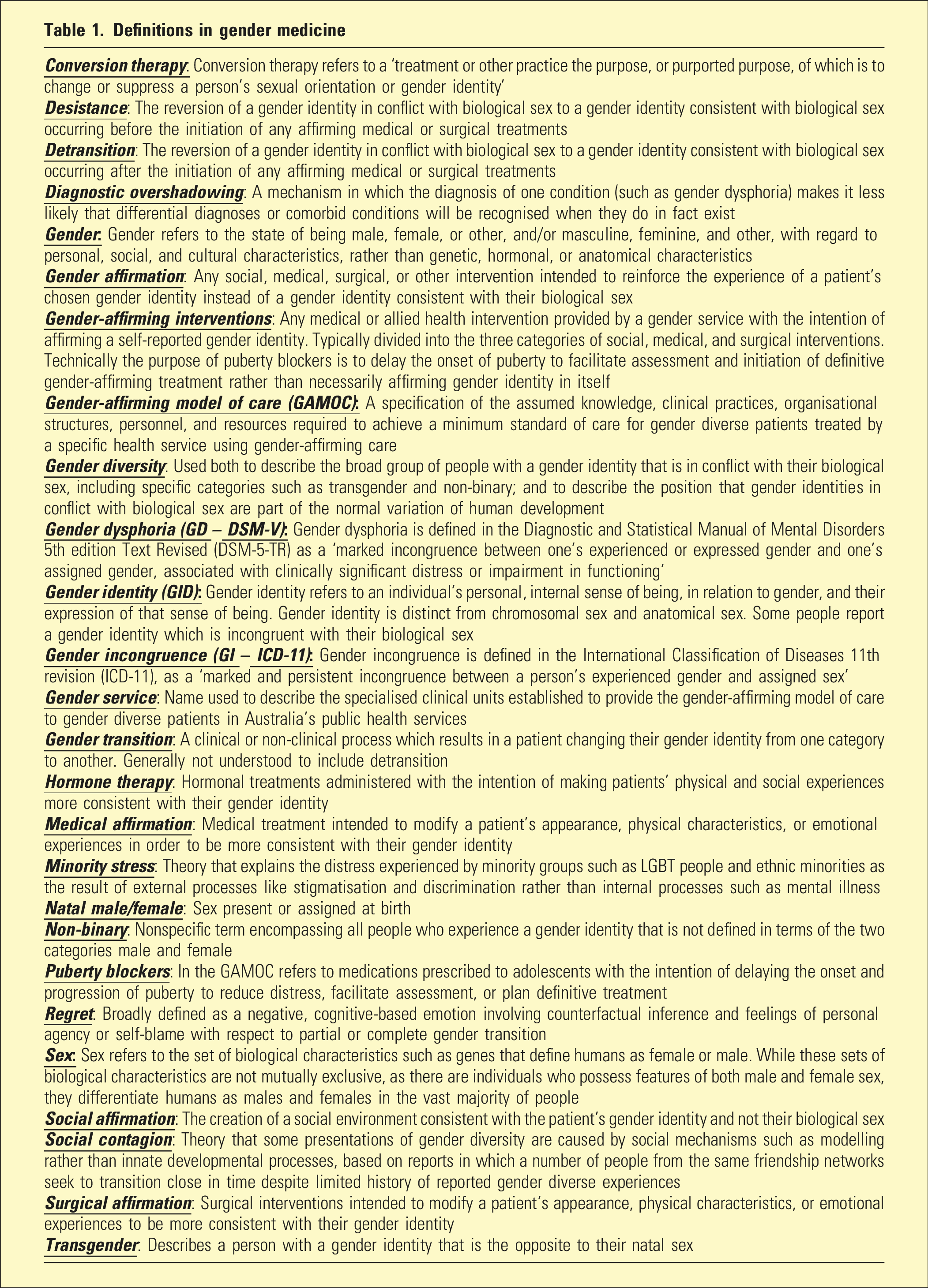
These changes accompanied the growing influence of the gender-affirming model of care (GAMOC) on Australian and New Zealand gender services. The GAMOC was pioneered in the Netherlands 3 and is promoted by an international network of groups including the Australian Professional Association for Trans Health (AusPATH) 4 and the World PATH (WPATH). 5 The GAMOC assumes that all people have a gender identity that is not determined by biological sex; assumes that patients are unquestionable experts about their gender identity, regardless of age; and recommends that professionals, family, and community always affirm patient reported gender identity.
Alongside puberty blockers intended to increase the time available to make decisions about the management of gender dysphoria, the GAMOC includes three modes of intervention affirming gender identity by social, medical, or surgical means. The most ambitious claim presented by GAMOC advocates in support of affirming interventions is that they are potentially lifesaving, citing the increased risk of suicide in gender diverse patients, which they associate with minority stress and societal prejudice.4,5 However, methodological limitations in this literature prevent the conclusion that GAMOC has a causal role in reducing suicide.6–11
In addition, a NICE review found no reliable evidence that puberty blockers improve gender dysphoria, mental health, body image, or psychosocial functioning. 11 The reviewers cautioned that all available studies had ‘very low’ certainty due to biases and confounds. The NICE review of hormone therapy in minors with gender dysphoria identified similar shortcomings, concluding there was very low certainty of benefits that must be weighed against the largely unknown long-term safety profile of these treatments. 10
After initial support for the GAMOC, international medical authorities have started to remove their endorsements. In 2020, Finland revised its GAMOC guidelines based on a systematic review of the evidence to prioritise psychological interventions over medicine and surgery, particularly for youth with no childhood history of gender dysphoria. 9 In 2022, the Karolinska Hospital in Sweden, following its own systematic review of the evidence, 8 issued a new policy statement ending puberty blockers and hormone therapy for minors. Hormone therapy is still allowed after 16 but only in research settings.
Historically, alternative approaches to the treatment of minors presenting with gender dysphoria included watchful waiting 12 and psychotherapy. Watchful waiting is predicated on high resolution of gender dysphoria after puberty and focuses on the treatment of psychiatric comorbidity and personality pathology. 13 A representative psychotherapeutic approach to gender dysphoria is Gender Exploratory Psychotherapy (GED), 14 which considers diverse aetiologies of gender dysphoria, including trauma, internalised homophobia, and comorbid psychiatric conditions such as autism spectrum disorder, borderline personality disorder, and eating disorders. GED provides a supportive approach to clarifying and addressing underlying aetiological factors and dynamics. GED has been erroneously conflated with conversion therapy by critics. 15
Abnormal illness behaviour and abnormal treatment behaviour
Discussion
It may be anticipated that those who insist that gender diversity does not involve psychopathology will argue that abnormal illness behaviours (AIBs) and abnormal treatment behaviours (ATBs) should not be applied to the GAMOC. However, gender dysphoria remains a DSM-5-TR diagnosis, gender incongruence is an ICD-11 diagnosis within the chapter on sexual disorders and sexual health, and the doctor–patient relationship is a core component of the GAMOC. Thus, AIB and ATB are relevant to the GAMOC whether it is assumed that gender diversity involves psychopathology or not.
Applying the ideas of abnormal illness and abnormal treatment behaviours to the context of gender dysphoria allows the insight that the diagnosis, formulation, and management of patient presentations by doctors can be subverted by unconscious dynamics affecting patients and clinicians. AIB provides a framework for understanding why so many young people now regard lifetime medicalisation as an attractive solution to potentially transitory gender dysphoria, regardless of trauma, internalised homophobia, and other comorbid psychopathologies. ATB provides a framework for understanding why some doctors and health professionals are so committed to the GAMOC despite the limited evidence of benefits, and poorly researched but certainly significant risks of adverse effects and complications, including loss of fertility, loss of sexual function, reduced life expectancy, and regret/desistance/detransition.
Clinical Case with features of AIB and ATB
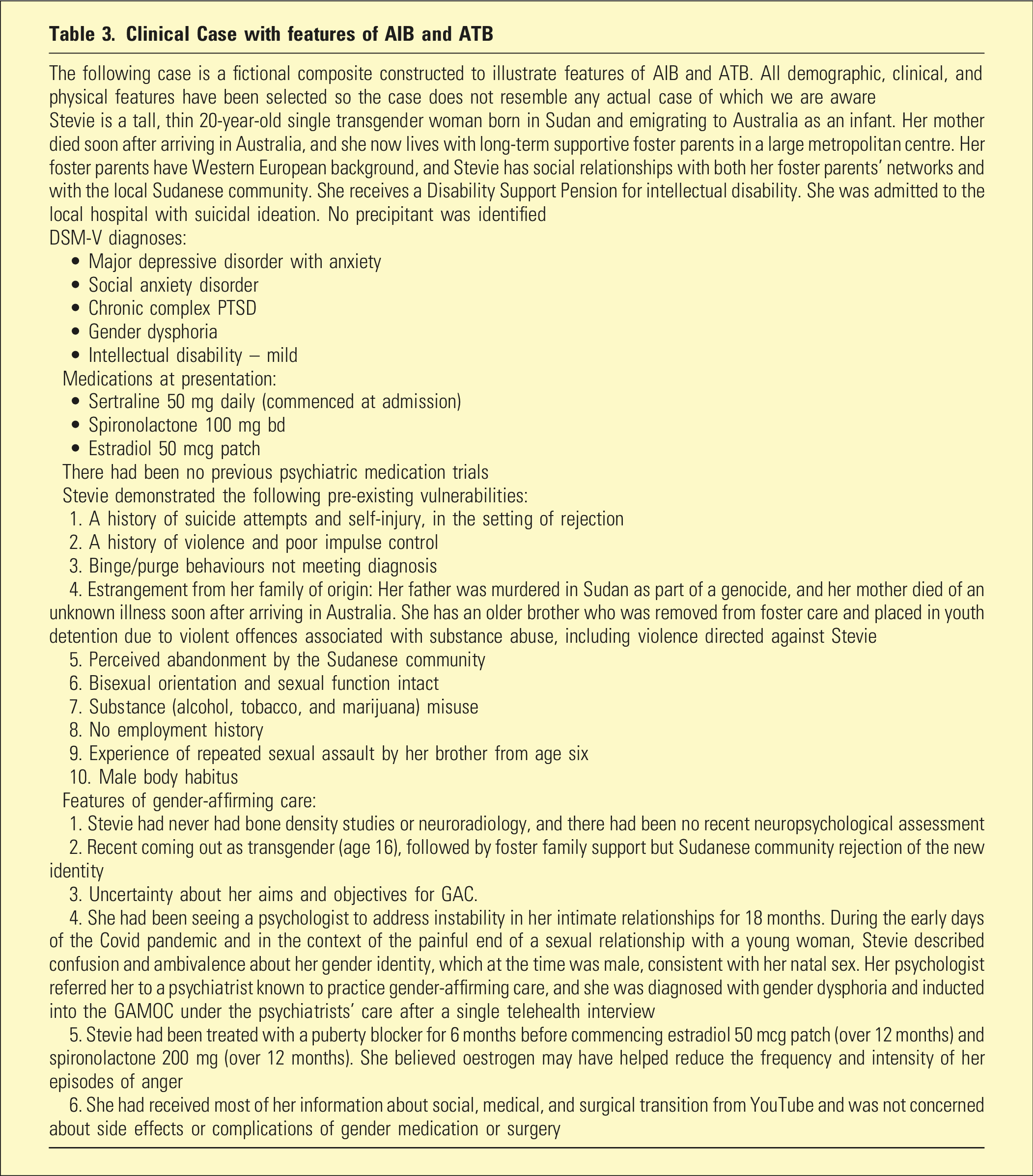
Let us consider fictional patient Stevie through the lenses of AIB and ATB.
The history includes repeated sexual trauma as a young boy at the hands of the brother; manifest in chronic complex PTSD; intellectual disability associated with concrete thinking; disrupted attachment and abandonment, with the early death of her mother and murder of her father; and perceived rejection from her culture as the result of bisexual orientation, pre-existing her current gender confusion and possibly associated with cognitive dissonance and the search for a meaningful identity which is developmentally consistent with her age.
Embracing a new identity affirmed by professionals, foster family, and gender-affirming social networks appears likely to allow Stevie to receive validation and support in a socially accepted way and deny male aspects of herself that she associates with violence, rejection, and death. It may also be satisfying to substitute the validation of the dominant culture for the rejection of the male-dominated Sudanese minority. The expression of gender diversity has provided Stevie with peer support often difficult for children with intellectual disability to access. On the other hand, this new identity and its powerfully reinforcing social contingencies might distract Stevie from conscious awareness of the underlying causes of her distress and therefore perpetuate her depression and anxiety by focussing on the relief of symptoms rather than the treatment of pathology.
The competent interpretation of such psychodynamic processes makes unquestioning affirmation impossible, because it must consider whether the self-reported identity is mistaken, misleading, or frankly factitious. For example, an exploration of the possibility that a gender identity has been reported for the purposes of secondary gain would violate the principle of unquestioning affirmation.
Among the ATBs expected due to uncritical gender affirmation, the most serious are a great reduction in the likelihood that clinicians will robustly assess, diagnose, and treat psychopathological factors that may contribute to gender dysphoria. For example, in Stevie’s case, the inability to explore her reported gender identity would prevent exploration of the psychic effects of her early abuse by her brother and the association between maleness, violence, and the loss of control.
It is useful to consider how Stevie’s case fits into Singh’s nosological framework for ATBs (Table 2). 24 The initiation of puberty blockers and hormone therapy instead of a psychotherapeutic approach such as Gender Exploratory Psychotherapy suggests the possibility of somatically focussed, illness affirming ATB. The question whether the psychiatrist’s motivation is conscious, unconscious, or a mix of both is a complicated one that depends upon their level of self-awareness.
It is instructive to consider how the different diagnostic approaches taken in the ICD-11 and DSM-5-TR might influence the probability of ATBs in Stevie’s treatment. While the DSM-5-TR still considers gender dysphoria to be a mental illness, the ICD-11 treats gender incongruence as a normal feature of human development. Thus, the diagnosis of gender incongruence could redirect affirming clinicians away from the psychopathological factors outlined above leading to under-diagnosis of Stevie’s depression, anxiety, and failure to recognise mechanisms such as compromised identity formation. This focus on gender incongruence to the exclusion of other causes of distress is called diagnostic overshadowing and can have undesirable effects including under-referring (e.g. for trauma focussed psychotherapy and exploratory psychotherapy), under-treating (with delay of and then inadequate trial of antidepressant medication), and consequent prolongation of illness behaviour. Diagnostic overshadowing was one of the serious problems with the GAMOC revealed by the Cass Review which led to the suspension of the gender service at the Tavistock Institute in the United Kingdom. 21
In addition, it may be argued that if medical affirmation becomes the primary treatment modality, that there is overtreating of the gender identity (with consequent risks of metabolic disorder and subsequent cardiovascular disease), while relatively ignoring other significant diagnoses and dynamics. In Stevie’s case, there had been no bone density or neurological radiology and no recent neuropsychological update, perhaps in keeping with under-investigation associated with ATB.
Additionally, this case could be argued as an example of psychologically focussed ATB, illness denying, motivation conscious (collusion with patient) and motivation unconscious (countertransference, judgemental attitude towards psychiatry, and identification with patients with an overinclusive view of normality). In the GAMOC, the patient is idealised as the unquestionable gender identity expert, and the clinician has the subordinate role of uncritical affirmation to facilitate social, medical, and surgical support. As a form of unconscious collusion, this encourages medical and surgical over-treatment, 22 under-treatment of psychiatric disorders, under-investigation of other factors, and may prolong illness over and above the probability of the lifelong trajectory of affirmation interventions. Whatever the causes, it is certainly true that there have been exponential increases in gender-affirming interventions in Australian and New Zealand minors, including puberty blockers and hormone therapy, since 2010. 22
Conclusion
This paper explores abnormal illness behaviours (AIBs) and abnormal treatment behaviours (ATBs) that may arise in the context of the gender-affirming model of care (GAMOC) by reinforcing the expression of gender diverse identities, overshadowing differential diagnoses, and redirecting clinician attention away from psychopathological contributions to gender diversity. This paper does not propose that AIB and ATB are exclusive or even preferred models of gender diversity, but merely that they contribute to understanding such patients and improving their care.
Pilowsky and Singh emphasise the impact of social, political, and cultural forces upon the doctor–patient relationship.23–25 Singh acknowledges that economic factors influence diagnostic and prescribing patterns, as well as patient’s families. Adopting the GAMOC may have significant potential financial and career consequences, including industry sponsorship, academic advancement for those who subscribe to progressive politics, and public recognition.
When Pilowsky and Singh wrote their articles, mainstream medical ethics balanced the principles of autonomy, non-maleficence, and beneficence. It can be argued that the rise of the GAMOC over the last 10 years mirrors the growing dominance of the principle of autonomy over the broader society. Over the same period, the GAMOC has been imbued with the status of a human rights issue, reflecting the significant influence of political and social movements over patients and physicians. However, while we acknowledge that adults can choose to prioritise autonomy over safety by exercising human rights that might include risky behaviours, we believe that doctors continue to have an ethical responsibility to balance autonomy and safety on behalf of their patients. This is particularly true for minors, who have widely varying ability to balance autonomy, safety, and other goods.
In our opinion, the uncritical affirmation by clinicians of the self-reported gender identity of all patients irrespective of their history, personality, comorbidities, and circumstances carries a high risk of concealing the unconscious motivations of patients and clinicians alike. If the medical profession does not urgently address this problem, it will be responsible for any harms that result, and risk loss of public confidence.
Footnotes
Acknowledgements
The Authors wish to acknowledge Dr A. Clayton and Dr R. D’Angelo for editing assistance with an earlier draft of this paper.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The second author is Deputy Editor of Australasian Psychiatry.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.