
Abstract
Objective
This paper describes an audit of borderline symptoms, risk factors for maltreatment and types of abuse among parents who completed a parenting capacity assessment at a South Australian health-based child protection service.
Method
A retrospective case note audit within a 28-month period was conducted and included parents (n = 107) who had completed a Mclean’s screening instrument for borderline personality disorder and/or had a psychiatric review with a formal diagnosis. Parents who had a borderline personality disorder diagnosis or endorsed five or more symptoms were categorised into the ‘high’ borderline symptom group. Rates of parental risk factors for maltreatment and type of abuse were compared between parents with low or high borderline symptoms.
Results
Forty percent of parents endorsed at least five borderline symptoms on the screening tool. On average, parents high in borderline symptoms had a greater number of parental risk factors.
Conclusions
These findings highlight the importance of screening for personality pathology among parents presenting to child protection services. Foundational training for staff and making evidence-based interventions available should be considered in such settings.
Keywords
Children in South Australia (SA) are entering and staying in out-of-home care (OOHC) at a concerning rate (2.2 per 1000 children). 1 The societal and financial burden of OOHC and negative mental health outcomes for children are well documented. 2 Whilst there are many risk factors for child maltreatment, several studies have found an association between borderline symptoms and child abuse potential.3,4 Further, elevated borderline symptoms have been identified among parents with child protection (CP) involvement.5–7
Many people with a diagnosis of borderline personality disorder (BPD) are capable parents8,9; however, the prevalence of BPD appears to be over-represented within CP settings with an estimated maternal prevalence of 34% in one international study. 6 Maltreating mothers with a diagnosis of BPD had greater rates of their own childhood trauma and were more likely to have perpetuated physical and multiple forms of abuse compared to maltreating parents without a personality disorder. 5 Prevalence of borderline symptoms among parents presenting to CP settings in Australia has not been established. Gaining a better understanding of borderline symptomology and CP risks may assist in informing future workforce training, assessment, referral and decision-making processes.
This audit aimed to describe rates of borderline symptoms among parents who completed a parenting capacity assessment (PCA). It was hypothesised that parents high in borderline symptoms would experience greater parental risk factors for maltreatment than the low-symptom group. Based on past research, it was anticipated that rates of physical and multiple forms of abuse would also be greater in the high borderline symptom group.
Method
Recruitment and eligibility
Participants included mothers and fathers referred to the outpatient Child Protection Service (CPS) in southern metropolitan SA. CPS receives referrals from the state child protection statutory body requesting PCAs with families post-CP intervention and often following the recent removal of children from their parents’ care. These assessments are used by the statutory authority and court decision-making process regarding the ongoing safety of children and to inform permanency planning. The project was reviewed by the Southern Adelaide Clinical Human Research Ethics Committee (SAC HREC) confirming that it met the criteria for clinical audit.
Participant flow
A retrospective case file audit was undertaken of 150 family units (including both mothers and fathers) whom underwent a PCA (n = 249 parents and n = 388 children) between March 2019 to June 2022. During this time, clinicians were asked to routinely include the Mclean’s Screening Instrument for BPD (MSI-BPD) in their PCAs. Files were reviewed for evidence of parental symptoms of BPD from either an MSI-BPD or documented in a psychiatrist’s clinical report. Across the family units, there was no data available for 142 parents and they were excluded from the analysis. Unfortunately, given the retrospective nature of the review we were unable to quantify reasons for why the MSI-BPD was not offered but anecdotal feedback suggested reasons such as the clinicians ‘forgot’, ‘ran out of time’ or it was not ‘clinically appropriate’.
One-hundred and seven parents had evidence of borderline symptoms reported in their records. This subset of parents were then categorised into a group with high borderline symptoms (defined as a score of 5 or more on the MSI-BPD) and compared to those in the low-symptom group. The MSI-BPD was missing for 15 participants who had a diagnosis of BPD recorded in a psychiatrist’s report. Given a DSM-V diagnosis of BPD requires people to experience at least 5 out of 9 symptoms, these participants were included in the ‘high borderline group’. Parents who had an MSI-BPD score that ranged between four and zero were included in the ‘low-symptom’ group for comparison purposes. The final sample included 52 parents with ‘high borderline symptoms’ compared to 55 parents categorised as ‘low borderline symptoms’. See Figure 1 for a summary of participant flow. Participant flow diagram.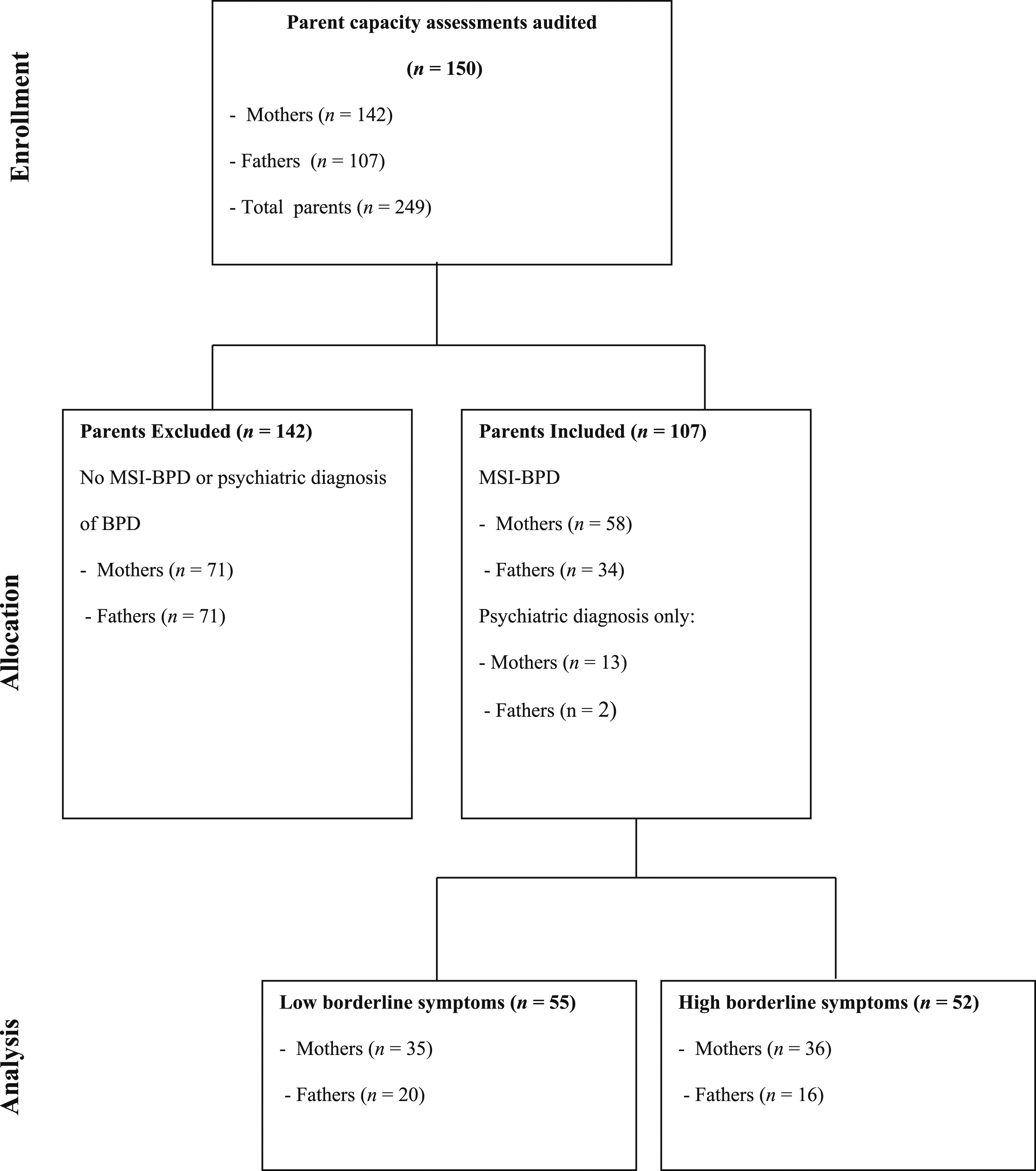
Procedure
A standardised proforma was created in collaboration between the clinical and research teams to identify and collate data from clinical files including demographics of both parents and children, borderline symptoms, parental risk factors for maltreatment and child abuse type identified for subject child/ren.
Measures
The MSI-BPD is a 10-item yes/no self-report questionnaire designed to measure symptoms of BPD. 10 Increased scores indicate a greater number of BPD symptoms with a cut-off score of 7 indicating further diagnostic assessment for a possible BPD diagnosis. 10 Previous research has classified participants as having elevated BPD features using varying criteria ranging between a score of 7 or greater on the MSI-BPD 3 or two symptoms less than diagnostic criteria. 5 In the current study, parents who obtained a score of 5 or higher on the MSI-BPD scale were categorised into the ‘high borderline symptom’ group. For those identified with BPD symptomology via psychiatric assessment report, these assessments were external to the CPS and appeared to be completed via the psychiatrist’s clinical judgement rather than via a standardised measure.
Whilst there is not a universally recognized standard for assessing parenting capacity, the CPS clinicians follow evidence-based guidelines which aim to cover a range of risk factors, for example, alcohol and drug use, mental health and capacity to form relationship. These assessments also focus on parent–child relationship and parents’ capacity to take a reflective stance on their previous parenting practice and alleged maltreatment. 11 At the conclusion of the assessment, clinicians documented the presence of child maltreatment risk factors for parents. These included domestic violence, transience, concerns of current parent–child attachment relationship, alcohol or other drug abuse, parents own history of abuse (including sexual, physical, emotional and neglect) and history of abuse against other children.
Clinicians also identified if any child maltreatment/abuse may have occurred for the subject child/ren based on the information provided during the assessment. Abuse types included emotional, physical, sexual abuse and neglect as defined by the Australian Institute of Health and Wellbeing. 12
Analytic approach
Data were checked for missing cases and cleaned prior to analysis with SPSS v. 27. Chi-square tests of independence (with Yates’ Continuity Correction) were utilised to explore differences between groups with categorical variables. Independent-samples t-tests were undertaken to explore differences between groups with continuous variables. Statistical significance was defined if the difference was p ≤ .05 and all tests were reported two-tailed.
Results
Participant demographics
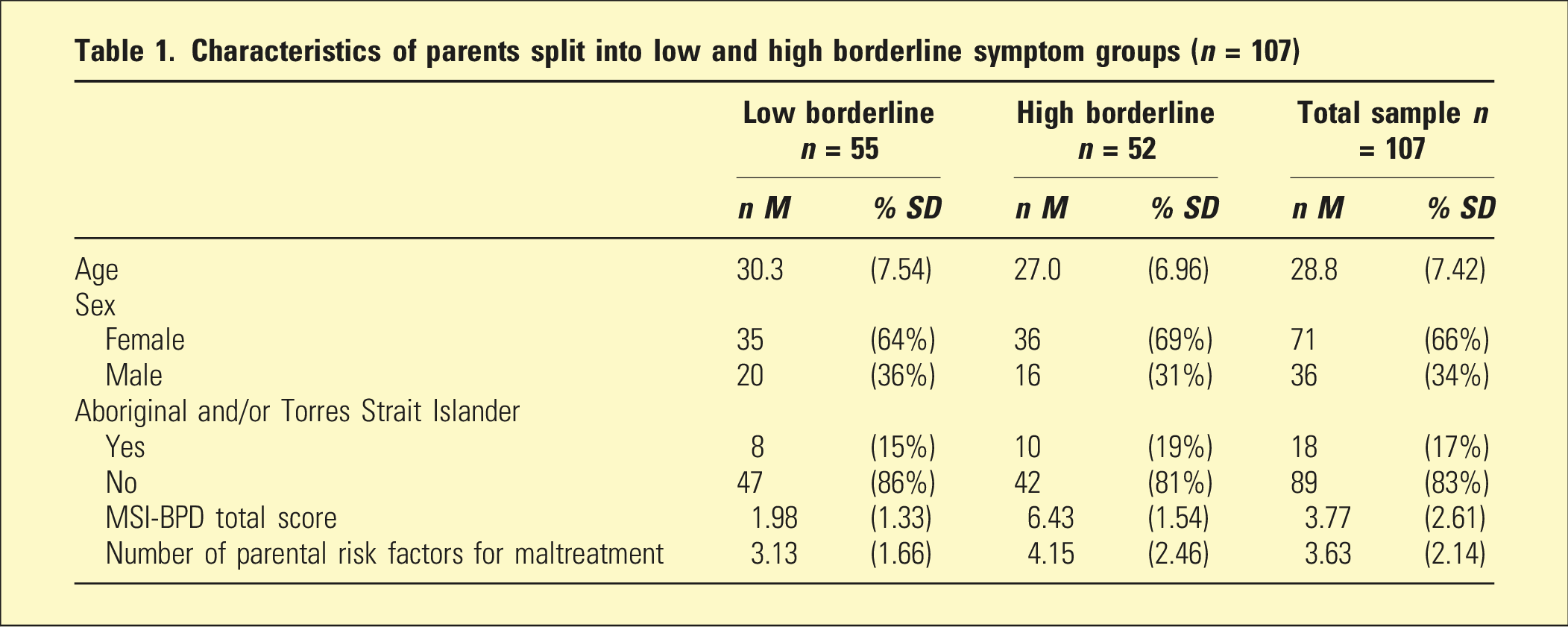
Characteristics of parents split into low and high borderline symptom groups (n = 107)
Parental risk factors for maltreatment
Parental risk factors for maltreatment (n %) split by parent sex and borderline symptom groups (low vs high)
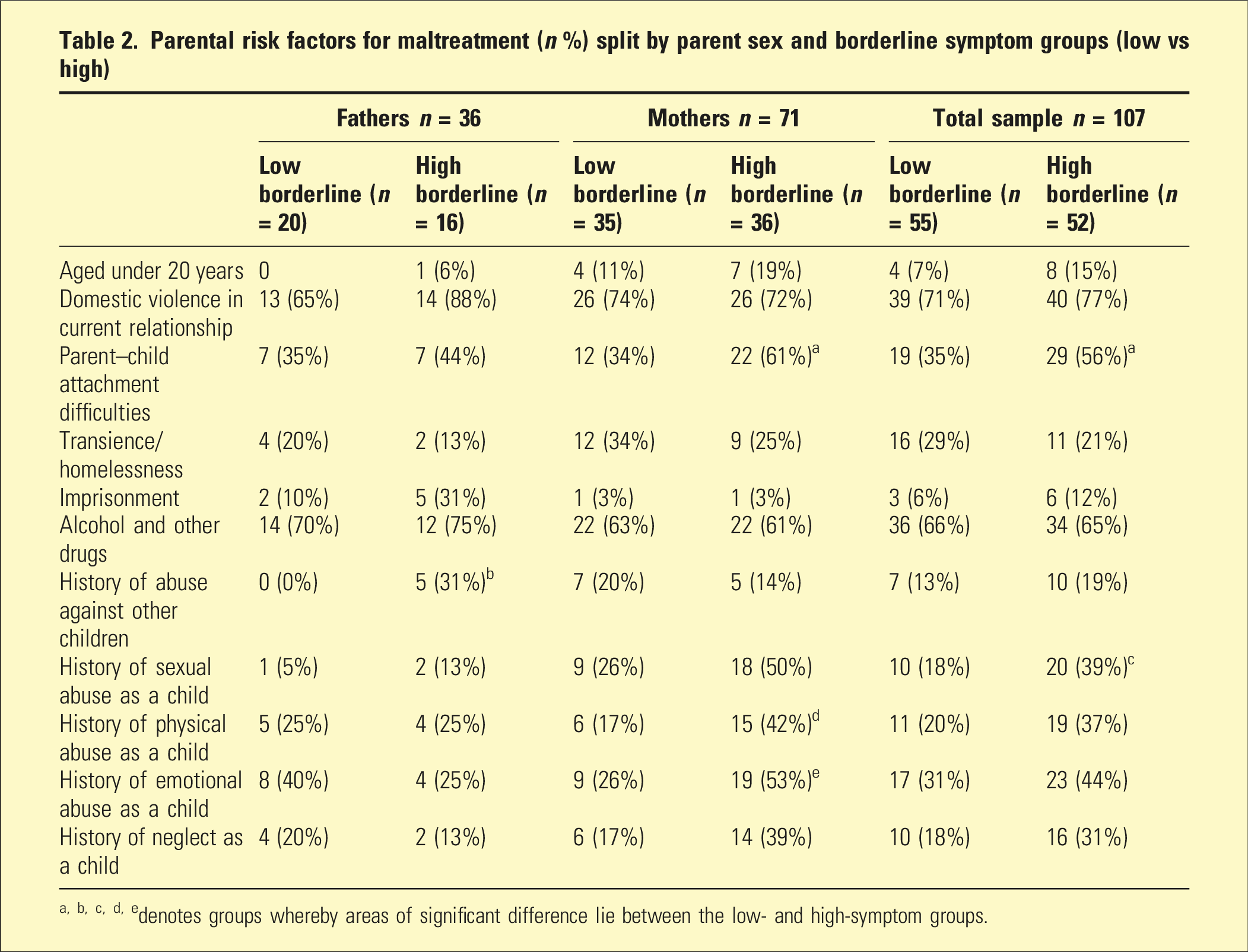
a, b, c, d, edenotes groups whereby areas of significant difference lie between the low- and high-symptom groups.
The total number of parental risk factors were greater in the high borderline symptom group (M = 4.15, SD = 2.46) than in the low borderline symptom group (M = 3.13, SD = 1.66; t (88.7) = −2.52, p = .01). Chi-square tests for independence indicated that compared to mothers in the low borderline symptom group, those in the high borderline symptom group were significantly more likely to experience parent–child attachment difficulties, χ2 (1, n = 71) = 4.10, p = .04, phi = .27; history of physical abuse as a child, χ2 (1, n = 71) = 4.01, p = .05, phi = .27; and a history of emotional abuse in childhood χ2 (1, n = 71) = 4.37, p = .04, phi = .28, suggesting greater complexity in this group. Alternatively, fathers in the high borderline symptom group were more likely to have a history of abuse against other children (Fisher’s Exact = .01). Overall, when considering the total sample, parents in the high borderline group were significantly more likely than those in the low-symptom group to have a history of sexual abuse as a child, χ2 (1, n = 107) = 4. 49, p = .03, phi = .23.
Abuse type
Frequency (percentage) of abuse type identified within the assessment split by parent sex and borderline symptom group (low vs high)
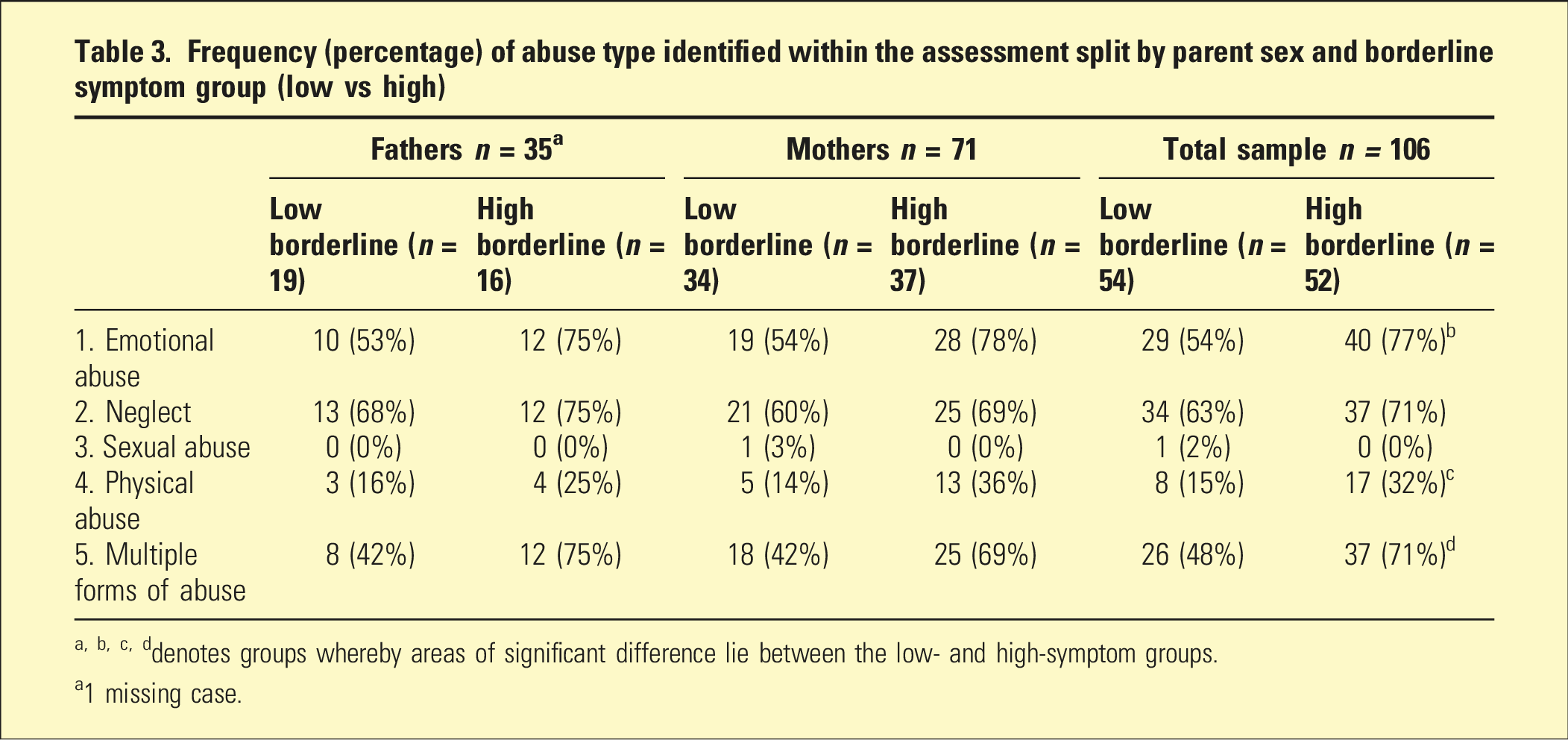
a, b, c, ddenotes groups whereby areas of significant difference lie between the low- and high-symptom groups.
a1 missing case.
No significant differences emerged when comparing high- and low-symptom groups specific to mothers or fathers. Across the total sample, the high borderline symptom group experienced greater rates of emotional χ2 (1, n = 106) = 5.31, p = .02, phi = .24; and physical abuse χ2 (1, n = 106) = 3.76, p = .05, phi = .21, than low borderline symptom group. Across the total sample, the high borderline symptom group was significantly more likely to have more than one type of abuse identified within the assessment χ2 (1, n = 106) = 4.90, p = .03, phi = .23.
Discussion
This audit demonstrated that among 107 parents who participated in a PCA, BPD symptoms were documented. Of this group, 48.59% were considered to reflect a group high in borderline symptoms. Similar to prior research,4–6 our findings identified greater parental risk factors for maltreatment among this group. Specifically, mothers in the high borderline symptom group were more likely to have a childhood history of physical and emotional abuse and parent–child attachment difficulties with their children. This finding aligns with local data which estimated that 84% of children with substantiated child abuse also had mothers who had childhood contact with statutory bodies. 13 An unanticipated finding was that fathers in the high borderline symptom group were significantly more likely to have a history of abuse towards other children.
As with prior research in CP settings, parents high in borderline symptoms were more likely to engage in multiple types of abuse, 5 with our audit identifying emotional and physical abuse as particularly problematic. Our findings highlight the importance of screening for personality symptoms in CP settings, and the need for workers to be provided training to develop their knowledge, assessment and intervention recommendations given that borderline symptoms and parenting behaviour are amenable to psychological intervention. 14 Poor parental emotional regulation may be a significant component of intergenerational transmission of maltreatment which may be reduced with early intervention. 15
This audit had a number of limitations. First, a large number of records were excluded due to missing MSI-BPD data and the reasons for the screening tool not being administered were not available. Second, the use of the self-report screener or psychiatric clinical judgement alone is not sufficient to warrant a clinical diagnosis which incorporates a comprehensive assessment process and ruling out differential diagnosis. In view of these limitations, this audit highlights the need for further research exploring the rates of BPD utilising structured methods in CP settings.
This study adds to the literature as it highlights a concerning number of parents in this sample rated high in borderline symptoms. This subgroup demonstrated a greater number of parental risk factors and was more likely to engage in multiple forms of supported abuse, indicating a potentially high-risk group of maltreating parents. Further, this audit adds to the literature as it included fathers, a demographic largely missing in the extant literature despite research suggesting a higher risk of child maltreatment potential among men with borderline symptoms.16,17 Given the availability of effective interventions for BPD, it is recommended that CP services routinely screen for borderline symptoms to inform parenting capacity assessment recommendations. Early identification of parental borderline symptoms and intervention embedded in CP services for these at-risk parents may reduce the likelihood of children being placed in OOHC.
Footnotes
Acknowledgements
The authors would like to acknowledge Abbey Mugford, Alice Wakefield, Georgia Kirkwood, Georgia Baker, Isabella Belperio, James Wilsdon and Maya Mikati for assisting with data extraction.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors completed this project as part of their employment with their respective departments within SA Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data that supports the findings of this study are available on request from the corresponding author. Data are not publicly available due to privacy or ethical restrictions.