
Abstract
Objective
The aim is to consider Long COVID not as a new clinical entity but as another example of a disabling, historical phenomenon.
Conclusions
A triad of polymorphic symptomatology, an elusive pathophysiological explanation and a hostile defensiveness has appeared throughout history. The reluctance to consider these contextually may delay early intervention and appropriate patient care.
‘… two societies confronting each other with conflicting universes will both develop conceptual machinery to maintain their respective universes’.
1
The 2019, SARS-CoV-2 pandemic was associated with significant mortality. Long COVID appeared as a term to describe a range of polymorphic symptoms persisting 3 months or more following the initial infection and has been associated with significant clinical, social and economic consequences. 2 Common experiences include fatigue, headache, anxiety, inattention (‘brain fog’), myalgia, breathlessness, dizziness, postural orthostatic tachycardia syndrome (POTS) and gastrointestinal disturbance. It is more common in females and is associated with significant morbidity. The exact mechanism behind this ongoing persistence remains unclear and no test is pathognomonic. Putative causes include chronic inflammation, an aberrant immune response and viral particle persistence. 2 Management is supportive and includes symptom-based pharmacology, psychotherapy, physiotherapy and occupational therapy. Prognosis is guarded. However, a number of unsettling observations have appeared.
In Long COVID, there is both a persistence and a variability to the reported 203 possible symptoms. Symptoms may occur without a preceding positive test or in the presence of a negative test, and there is only a weak association between the severity of acute COVID-19 and the onset of Long COVID. 2 Possible explanations include differing testing policies between countries, testing too early or too late in the disease course and an inconsistent or aberrant immune response. 2 However, an older narrative may exist, with Long COVID having similarities to a number of named, historical disorders.
In 1983, a seemingly new illness appeared in the small New Zealand town of Tapanui. 3 Subsequently named chronic fatigue syndrome (CFS), symptoms of Tapanui Flu included fatigue, headache, anxiety, inattention, myalgia, breathlessness, dizziness and other subjective complaints that were difficult to substantiate objectively. No test was pathognomonic. The pathophysiology of CFS remained elusive despite continued inquiry including by investigators whose lives had been significantly touched by the condition. CFS is more common amongst females, prognosis is guarded and treatment remains primarily supportive but now includes a more articulate inter-disciplinary support network, perhaps developed in response to a sceptical audience.
Even earlier, a similar unexplained epidemic occurred amongst the staff at London’s Royal Free Hospital. 4 Symptoms included fatigue, headache, anxiety, inattention, myalgia and breathlessness. No pathological basis was found and no test pathognomonic. There was again a female preponderance and whilst proving relatively benign, some patients were affected for up to a year. A Lancet article entitled ‘A New Clinical Entity’ followed and suggested ‘benign myalgic encephalomyelitis (ME)’ as the diagnosis. However, there was an unexpected comment at the end of the article – ‘… we believe that its characteristics are now sufficiently clear to differentiate it from poliomyelitis, epidemic myalgia, glandular fever… and need it be said, hysteria’. McEvedy and Beard were perplexed, as the case for hysteria had not been examined and they had noted the overlapping symptoms between those reported and those they had encountered in a previous epidemic of hyperventilation in 154 school children. 5
The curious disregard for hysteria
‘At first glance it is extremely difficult for [anyone] to grasp how such physical symptoms… may in fact be an extension of ideas or fantasies. If the mysterious leap from the mind to the body is ever to be understood, then what is needed is an attentive and understanding approach to the entire patient’.
6
It is a curious phenomenon that, every now and then, a clinical entity appears seemingly for the first time. It is given a new name, yet its signature remains identifiable – a triad of polymorphic symptomatology, an elusive pathophysiological explanation and often a disproportionate defensiveness to suggestions that there may be psychological contributions.7,8 Hysteria has become pejorative, rather than an extraordinary attribute of an attuned human response. Acknowledging a female preponderance may be seen as sexist despite the observation that unexplained illnesses may be associated with trauma and a unique set of societal pressures that women more often endure. Associated features of new unexplained entities include the presence of a triggering threat, re-naming of old symptoms and a personal investment on the part of the investigators attempting to establish scientific legitimacy.
That a psychological process may have a somatic effect has been long documented in both the clinical and non-clinical fields. In a review of epidemic hysteria that dated back to 1374, threats have included environmental factors (contaminated water, chemical exposure and gas leaks) as well as conflict that was both high and inescapable. 8 In 1859, Briquet speculated on untoward development and life experiences including parental mistreatment and spousal abuse and described his first series in men. 9 In the workplace, stress related to boredom, production pressures, labour-management relations, job dissatisfaction or conflict between one’s job and other obligations, particularly those at home, were noted. 8 When there was a fear of toxic gas being released in Tokyo’s subway, more than 85% of the 5500 people seeking hospital treatment were found to have a psychogenic aetiology. 10 Fear was heightened by the unique challenges associated with COVID-19, including communicated global mortality, protracted lockdowns, vaccine hesitancy and misinformation. In the non-clinical realm, similar symptoms were reported following the extraordinarily realistic, 1938 War of the Worlds radio broadcast where listeners panicked, believing they were being invaded from Mars. 11 In 1954, fear of a local radiation leak causing car windscreen pitting took hold. 11 In 2016, fear of a Russian-initiated, invisible ray attack on United States 12 personnel in Cuba, known as the Havana Syndrome, appeared. 13 Spreading easily, contagion appears enhanced by the general excitement of emergency personnel and equipment, the media, rumours and interestingly, labelling the illness with a specific diagnostic term. 8
In order to evaluate epidemiological observations, Bradford Hill suggested that for A to cause B, specific criteria might be met. 14 These include a strong association that intuitively is plausible, coherent, specific and consistent in other populations. Further, the stimulus must precede the outcome and that the relevant outcome could be reproduced experimentally. With respect to Long COVID, a follow-up study of 54,960 patients showed that pre-infection psychological distress predicted an increased risk of Long COVID. 15 The mortality of acute COVID-19 and persistence of Long COVID stand in contrast to the Havana Syndrome where no deaths occurred. 13 The experimental induction of a similar psychogenic illness has recently been reported and, interestingly, demonstrated no gender differences. 16 Despite these observations, psychogenic factors often polarise rather than contribute to the understanding and management of these disabling conditions.
Getting the name right by understanding the problem
‘Refusing to acknowledge its existence or changing its name will not make it go away. The way we formulate the diagnosis and the way society responds to patients with the disorder do have consequences for course and outcome’. 17
Described as the social construction of reality, knowledge is not just made up of objective inquiry but also of the result of communicable social perceptions, values and beliefs. In an attempt to comprehend complexity and uncertainty, differing narratives may reflect the prevailing discourse in the only available currency at the time. For example, given the predominance of gynaecological- and obstetric-related symptoms, Hippocrates suggested the uterus (‘hyster’) was a central factor in ‘female complaints’. When spirit possession was at the fore, exorcism dominated. Influenced by the notion of planetary and magnetic forces on the human body, Mesmer suggested magnetism as a treatment. In 1697, Sydenham conceived hysteria as an emotional condition, moving the source of the disorder from the uterus to the brain with Freud emphasising unbearable conflicts presenting as physical manifestations. 18 Comparing the similar symptoms of neurasthenia in the East and CFS in the West, social influences were described, including the respect accorded to neurasthenia which confirmed those affected were often hard working and high achieving. 19
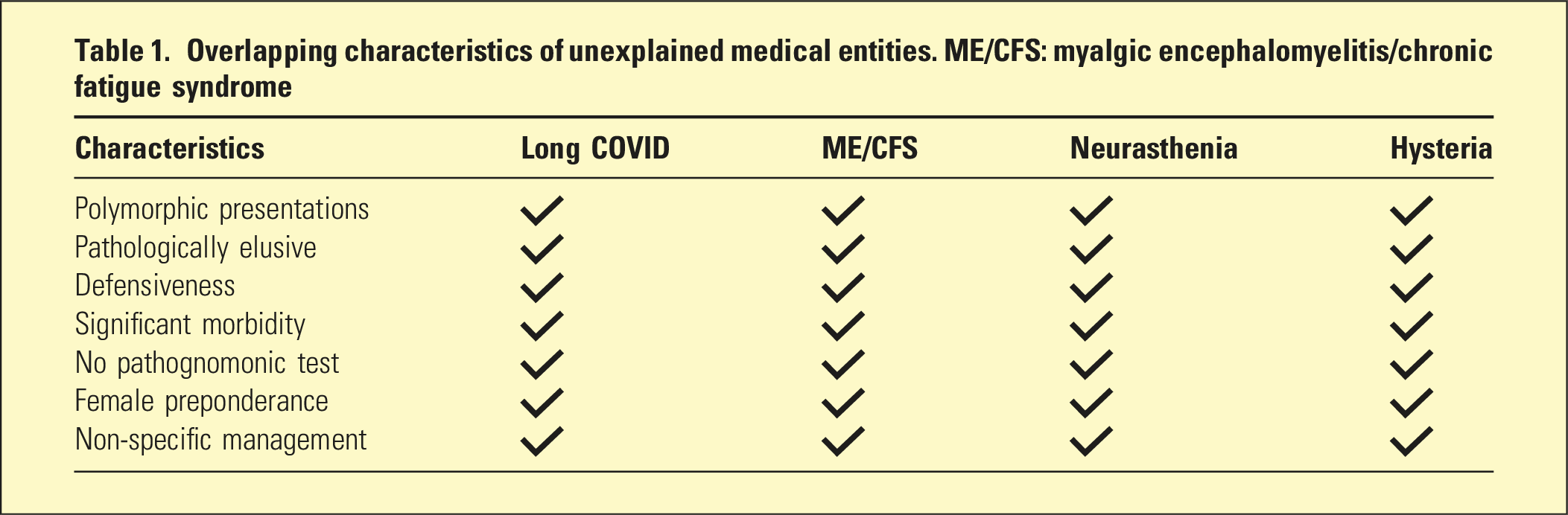
Overlapping characteristics of unexplained medical entities. ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome
Conclusion
There has been an uneasiness in writing this article. An uneasiness for fear of its misinterpretation and in so doing of being distracted from its overall aim, namely, to contextualise social and psychological factors in unexplained illnesses, both current and historical. The narrative offered here necessarily reflects the values and beliefs of the authors, all of whom are psychiatrists. Long COVID has similarities to other historical, clinical and non-clinical events that have appeared across time and cultures. The clinician can be alerted to this possibility by recognising familiar polymorphic presentations that remain pathologically elusive but are associated with a disproportionate defensiveness. Reacquaintance with historical lessons may offer an appreciation of the agility of the mind and body and an opportunity to intervene early with a focus less on the molecular and more on the context from which the person presents.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.