
Abstract
Objective
Contemporary medical education lacks a strong focus on health economics which guides major decisions in private and public health services. We briefly outline the rationale, guiding principles, main analytic methods, and a suggested framework for health economics education in psychiatry.
Conclusions
Health economics aims to improve the efficiency of healthcare. Some analytic methods can be harnessed by psychiatrists to better plan clinical care. Health economic methods will also assist psychiatrists in translating their expertise and clinical priorities more effectively to policy-makers, governments, and private insurers motivated by economic reasoning.
There is a relative neglect of health economics in undergraduate and postgraduate medical education. 1 This hampers doctors’ ability to contribute more effectively to healthcare policy and planning. 1 Few psychiatrists have received education in health economics. The Royal Australian and New Zealand College of Psychiatrists (RANZCP) training curriculum has limited reference to health economics. There is a managerial competency to 'prioritise and allocate resources efficiently and appropriately', 2 and an ethical competency to assess 'the influence of industry and resource availability in local services, financing, agencies and others and the impact on professional practice and patient care'. 3 While these principles address aspects of health economics, a more detailed practical understanding is needed.
How is health economics useful in healthcare?
Modern psychiatric care presents many more opportunities for prevention, intervention, and treatment than previously possible. 4 Due to scientific and technological advances as well as empowerment of patient advocacy, there are now many more care options than the necessarily limited resources of taxpayers, governments, and private providers can service. 4 The allocation of resources should therefore be as transparent and fair as possible. 4 Health economics is a branch of economics applied to healthcare regarding the allocation of finite healthcare resources. 4 Health economic assessments usually include the development of economic models and analysis. What is regarded as valued depends on the assumptions, inputs, and outputs of these health economic models. 4 Equity, that is, a fair distribution of resources, is a consideration in such modelling. 4 Patients with equal needs should receive the same care (horizontal equity), and patients with higher needs should receive greater care (vertical equity). Also, the benefits gained from healthcare should exceed those forgone, that is, the opportunity costs. 4 Accordingly, health economics provides a decision-analytic framework in which to consider the efficient and equitable provision of healthcare. 4
Health economic modelling and analysis involves measurement, comparison, and valuation of positive outcomes (benefits), as well as negative outcomes (costs).
4
This allows assessment of whether benefits of a healthcare intervention outweigh the foregone benefits, or opportunity costs.
4
There are three major guiding principles in health economic analysis:
4
1. Opportunity costs arise because all budgets are finite, and spending in one domain will result in less spending in another domain – this constitutes the lost opportunity.
4
2. Perspective is everything – the viewpoint of the investigator determines the definition of benefits and costs.
4
The viewpoints of patients, carers, families, clinicians, health services, governments, Non-Governmental Organisations, and other healthcare payors are often different. 3. Marginal analysis is applied as healthcare decisions generally relate to whether to expand or decrease existing health services, so benefits are not necessarily linear.
4
This evaluation involves understanding how incremental benefits accrue with incremental resource allocation, in contrast to estimating the aggregate average benefits incurring average costs.
4
Based on these principles, there are five major methods of economic evaluation that could be used by psychiatrists to advocate in healthcare policy, planning, and implementation:
4
1. Cost minimisation: A priori, the outcomes of two or more interventions are considered equivalent.
4
This analysis is delimited to costs, to choose the cheapest option, for example, cheapest of two atypical antipsychotic medications considered of equal efficacy.
4
In reality, outcomes are rarely equivalent, and so this is not often used.
4
2. Cost-effectiveness analysis: This is the method most commonly used, and may be the most familiar to psychiatrists. It compares interventions that have a common health outcome,
4
for example, reduction in positive symptoms of psychosis. This may also involve surrogate outcomes,
4
such as the cases detected or reduction in medication side-effects, which need to be clinically relevant to be useful for evaluation. These analyses are reported as a ratio,
4
for example, psychiatric treatment order enforcement costs per year of life saved. 3. Cost-utility analysis: This assesses the benefits and costs of interventions on the quality and quantity (years) of life as measured through techniques such as standardised questionnaires, standard gamble, or time trade-off.
4
Standard gamble is the willingness to risk death to avoid a certain state of ill-health. Trade-off involves the choice between a shortened life expectancy in perfect health and a longer one in chronic ill-health. The Disability Adjusted Life-Year (DALY) is a specific version of the quality adjusted life-year and is a measure of impact on length and quality of life, wherein health is valued on a continuum between 0 (worst) and 1 (best) adjusted by the length of time in that state. The DALY represents the loss of one year of full health, calculated by the years of life lost due to living in less than full health and years lived with a disability due to the prevalence of a health condition, and is commonly used for psychiatric disorders.
5
This analysis is challenging due to methodological issues in quantifying the base measures such as years of life lost, which is difficult to effectively estimate for psychiatric illness.
4
4. Cost-benefit analysis: This attempts to monetarily value all the outcomes and costs of an intervention, with the aim that an acceptable intervention has benefits that are less than the costs.
4
However, there are substantial challenges in this type of analysis due to the requirements for large datasets and valuation of non-monetary benefits such as numbers of lives saved, or disability averted, etc.
4
Accordingly, this method is rarely used.
4
5. Cost-consequences analysis: Since disparate outcomes cannot be summarised in a single benefit measurement, policy-makers and governments often use this method.
4
Outcomes and costs are disaggregated
4
(see Table 1). Cost consequence analysis example – transferring depot antipsychotic treatment to primary care (see reference for more detail)
4
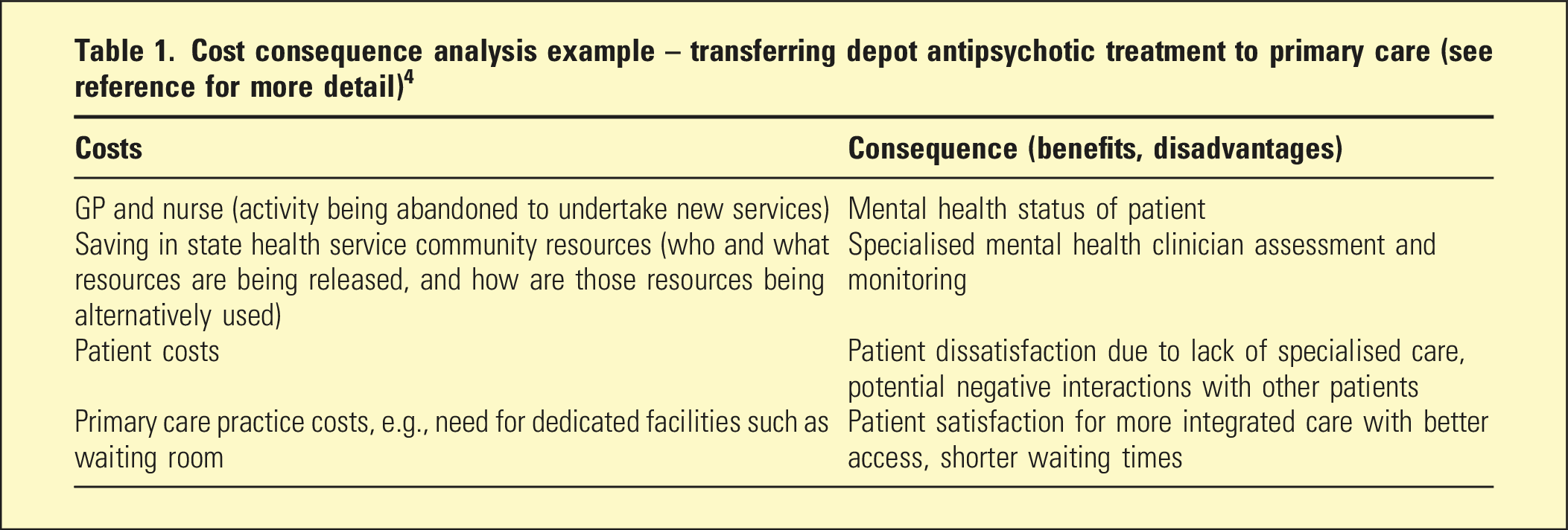
There are limitations. Cost and consequences need to be credibly evaluated and discounted. The latter refers to the fact that the value of a dollar spent in the present is worth more than if spent in the future, both because of economic inflation and because of a preference to derive benefits now rather than in some time to come. In addition, all measures of utility have some degree of subjectivity. These limitations therefore require the use of sensitivity analyses of the effect of varying the underlying assumptions.
Governments and policy-makers routinely incorporate such health economic analysis into their governance of society, and increasingly, the economic impact of the burden of mental disorders in society has been recognised. 6 This can be quantified in terms of direct and indirect costs to society, which the Australian Productivity Commission has estimated at between AUD 40-70 billion per year. 7 Health economics can therefore assist in the allocation of funds for improving mental health and monitoring outcomes, as well as the practical governance of healthcare, known as health stewardship. 7 Health stewardship focuses on governmental responsibility for the wellbeing of their population and provision of healthcare, 8 and where health economics can make a significant contribution is in providing a foundation for credible decision-making processes, as well as guiding effective financing and resource mobilisation.
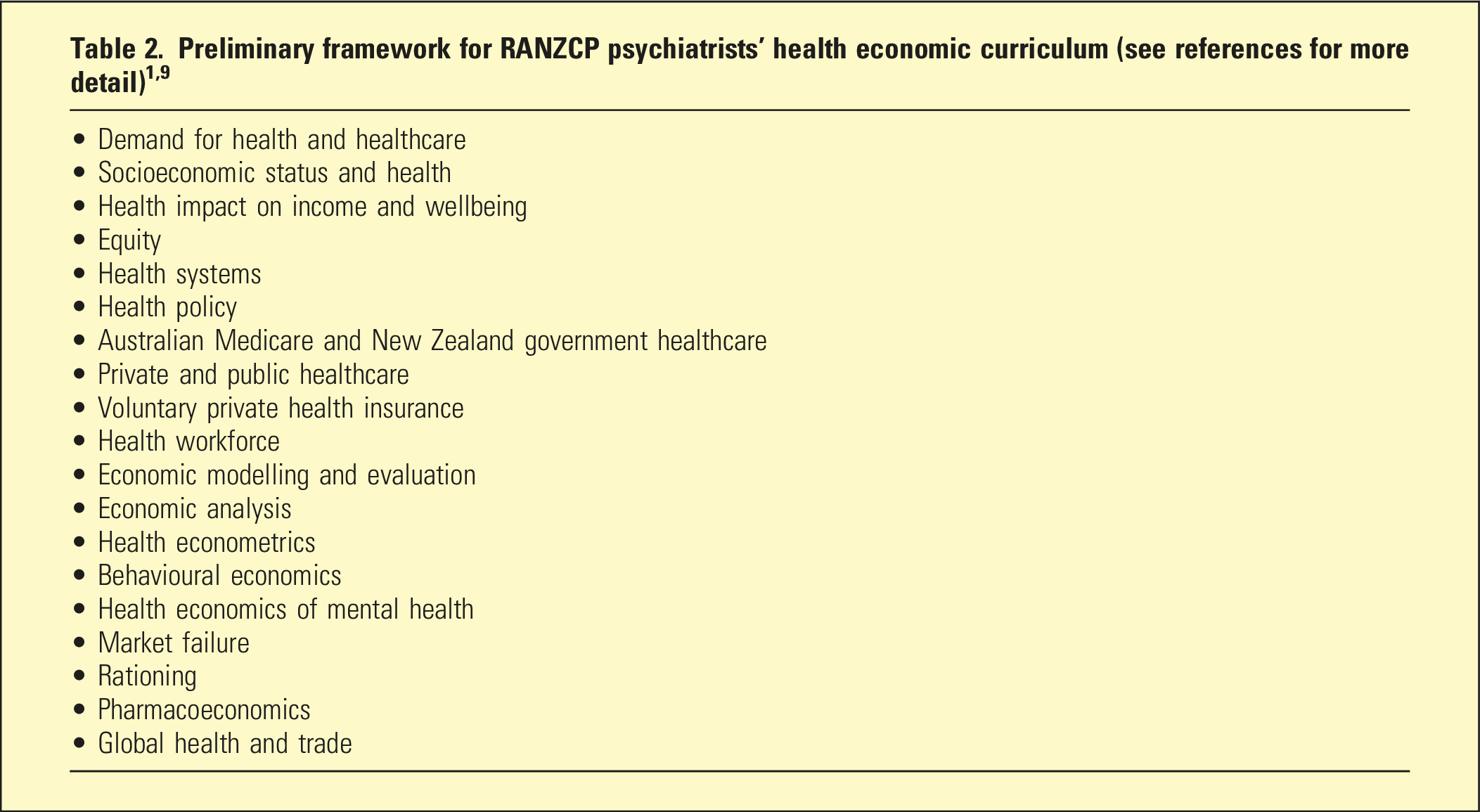
A health economics curriculum framework for psychiatrist specialist training
Public sector psychiatry applications
Table 1 is a simplified form of presentation of a real-world cost-consequences analysis that a psychiatrist might present to their clinical director in a public sector setting.
Activity-Based Funding (ABF) of Australian public hospitals is predicated on a classification of service types, the weighting of prices for services, and a reference Nationally Efficient Price determined by the Independent Health and Aged Care Pricing Authority.10,11
Psychiatrists with health economic skills will be better prepared to understand the underlying assumptions, develop informed arguments addressing funding shortfalls, and address system-wide inefficiencies or misconceptions. These skills can also assist in industrial advocacy on working conditions and pay, for example, unsafe and unsupportive workplace culture increases clinician turnover and therefore increases costs from onboarding new staff, as well as sourcing locums.
Private psychiatry applications
As small business operators, private practice psychiatrists may be familiar with basic economic principles, such as capital outlay to purchase rooms. However, private practitioners also engage with third-party payors for patient care, such as private health insurance for hospital care, Veterans’ Affairs, and workers’ compensation insurance. The formation of the Honeysuckle Health – nib buying group by private health insurers – was predicated on one large buyer purchasing clinical services from healthcare providers and hospitals. However, the subsequent deed of settlement at the Australian Competition Tribunal demonstrated the danger of financial control being consolidated in the private healthcare sector. 12 This could lead to managed care involving selective contracting, financial incentives and penalties for doctors, and limitations on patient use of healthcare. 13 Health economics could therefore assist private psychiatrists in understanding the benefits, and especially costs of such a wide-ranging development. 13 These skills can also help private psychiatrists better plan for patient care. One example is indicating to a workers’ compensation provider that a planned inpatient admission for intensive care may benefit recovery and rehabilitation, and reduce overall costs that might otherwise be incurred by repeated failures of graduated-return-to-work from less intensive care.
Conclusion
Psychiatrists in public and private practice should be advocates for evidence-based care. Through further education and upskilling in health economics, psychiatrists can access the analytic skills and lexicon that translates the benefits of psychiatric care, balanced against costs, in policy and planning with policy-makers and governments. Health economics advice is shaped by what is valued, as well as the inputs and outputs that are measured. 4 Informed by psychiatrists’ clinical acumen, credible and transparent health economic analysis can assist in empowering planning of equitable and efficient psychiatric care.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.