
Abstract
Objectives
The National Disability Insurance Scheme (NDIS) was introduced in 2013 and offered a new way of providing support to people with permanent and significant disabilities. Despite pilot testing, implementation of the scheme has been challenging, particularly for people with a disability arising from a mental health condition. In 2019, to address the challenge of accessing the NDIS, researchers from Flinders University worked with the National Disability Insurance Agency (NDIA) to develop a streamlined access process for psychosocial disability. The aim of this paper is to provide guidance on the evidence required to demonstrate that a person has a significant and persistent psychosocial disability to access the NDIS.
Conclusion
Providing evidence for a psychosocial disability requires knowledge of how to address the disability requirements. The Evidence of Psychosocial Disability (EPD) form has been designed to address these requirements and offers guidance on the evidence that should be provided. A range of resources to accompany the EPD form are freely available online. These resources address a significant knowledge gap that currently exists with the implementation of the NDIS.
The introduction of the NDIS in 2013 resulted in a significant change in the way people living with permanent and substantial disabilities were supported, moving from a block funded ‘one size fits all’ system to individualised person-directed supports. 1 The implementation of the NDIS has been one of the biggest public policy shifts in Australia. 2 While there is considerable information available about the policy impacts of the scheme, there has been a lack of information on how people with a disability access the NDIS. This is particularly the case for people living with psychosocial disability, who need to gather evidence demonstrating that their mental health (MH)-related disability meets the NDIS access criteria. A substantial number of people (27%) who received psychosocial supports through the previously funded MH programs did not meet the NDIS access criteria despite receiving support to apply. 3 Further, people living with a MH condition and their carers reported that they found the access process confusing and stressful, and that it was challenging to identify what information was required. 3
Consistent with the core principals of the NDIS, the access process takes a person-centred approach, requiring the person with the disability and/or their carer to initiate the process, liaise with services to collate and submit the required evidence within the given time frames. 4 This can be extremely difficult for people with a MH condition, given that psychosocial functional impairments commonly include difficulties with communication, cognition, planning, goal setting and task management, and an inability to recognise their own impaired functioning. 5
While assistance to apply is available for people within funded MH programs, people who are not connected to any services do not have support available. A 2019 review examined the rollout of the NDIS for individuals with psychosocial disability and found that there had been a general lack of information to help people engage with the scheme and to understand its language and terminology. 6
Although the terms ‘psychosocial disability’ and ‘mental health condition’ are sometimes used interchangeably, it is important to recognise that not all individuals with a MH condition will experience psychosocial disability.
“Psychosocial disability is the term used to describe disabilities that may arise from mental health conditions. Whilst not everyone who has a mental health issue will experience psychosocial disability, those that do can experience severe effects and social disadvantage. People with a significant disability that is likely to be permanent may qualify for NDIS support.”
7
The Transition Support Project (TSP), based at Flinders University, was funded by the Australian Government Department of Health and Aged Care (DoHAC) to provide resources and training to support Primary Health Networks and community MH providers to assist previous Commonwealth-funded MH clients to apply to the NDIS. Project staff worked closely with the DoHAC, Department of Social Services and the MH team at the NDIA to develop a series of access resources, as well as the Evidence of Psychosocial Disability (EPD) form.
The aim of this paper is to provide guidance on accessing the NDIS for people with psychosocial disability. Given the nature of this work, ethical approval was not required.
The evidence of psychosocial disability form
The national roll-out of the NDIS began in 2016 and by 2018 the challenges of providing evidence to meet the psychosocial disability requirements to access the scheme were evident. 8 To address this, the TSP collaborated with the NDIA to improve the access process for people with a MH condition. The resulting ‘streamlined access process’ was launched in September 2018 and included fact sheets, a consent form allowing someone to act on behalf of the applicant during the access process, and the EPD form.
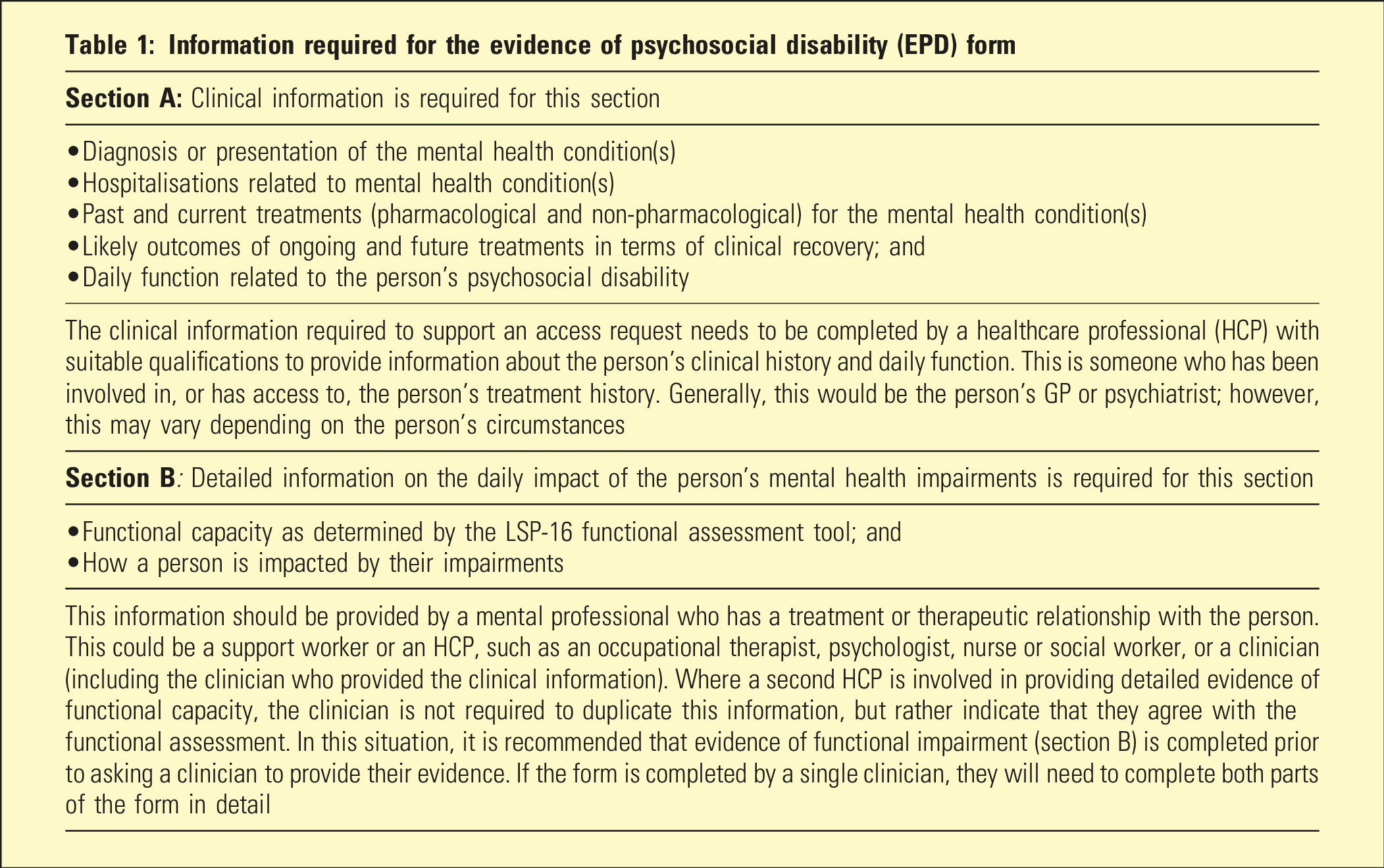
The EPD form replaced the NDIS supporting evidence form and provided guidance for the applicant and their treating team on the type of evidence required. The Life Skills Profile−16 (LSP-16) 9 was embedded within the EPD form to provide an objective measure of a person’s level of functional capacity related to their MH condition. The EPD form was piloted with general practitioners (GPs) and MH service providers and was approved for use by the NDIA.
Information required for the evidence of psychosocial disability (EPD) form
The disability requirements
Section 24 of the NDIS Act 10 defines five criteria a person must satisfy to demonstrate that they meet the disability requirements for access. A person must satisfy all 5 criteria through providing medical and allied health evidence. Of note, in 2022, the Australian Parliament passed legislation amendments to the NDIS Act 2013. 11 While a number of amendments were passed, the only change in regards to Section 24 of the Act included the recognition that some conditions may be episodic or fluctuating, which should be taken into consideration when determining if an impairment is permanent.
Demonstrating the presence of a permanent disability 24(1)(a) and (b)
Potential NDIS participants must provide evidence that they have or are likely to have a permanent disability resulting in impairments. If a person has a formal diagnosis, it is important to include when it was made and by whom. If there is no diagnosis or conflicting diagnoses, it is recommended to state that the person has a ‘mental health condition’ and provide information on when it first appeared and its presentation.
To demonstrate that the diagnosis and associated impairments are permanent, there must be information provided to show that all appropriate and available evidence-based treatments (pharmacological and/or non-pharmacological) have been tried along with a statement regarding their effectiveness in relation to the underlying MH condition and/or its associated impairments.
In addition, the treating clinician must include a statement as to whether the underlying MH condition and associated impairments are likely to persist for the person’s lifetime. Without this statement of permanency, the person is unable to demonstrate they satisfy this criterion.
Tips to consider: • If a person has recently (≤2 years) been diagnosed or begun to experience symptoms of a MH condition, it will be difficult to demonstrate that all available and appropriate evidence-based treatment has been tried. Hence, it might be more appropriate to focus on clinical management of the underlying condition. • All treatments recommended must have been tried with outcomes documented in order to show that the disability is likely to be permanent, as demonstrated in a recent ruling from the Administrative Appeals Tribunal (AAT).
12
Functional Capacity 24 (1)(c)
To meet this criterion, the applicant must show substantially reduced functioning in one or more life domains. Social interaction, self-care and self-management are the most common domains that people with psychosocial disability experience difficulties in. The evidence provided needs to demonstrate that the person is unable to complete most activities within the selected domain(s) without supports on a daily basis. This evidence should only focus on the MH impairments (and not any other co-occurring health conditions) and on day-to-day functioning between acute episodes. Current assessments that address daily functioning (e.g. occupational therapy, neuropsychological) are particularly helpful and can be used to complete the EPD form or provided as an attachment.
Questions to ask to help determine the impact of the mental health condition on a person’s functioning
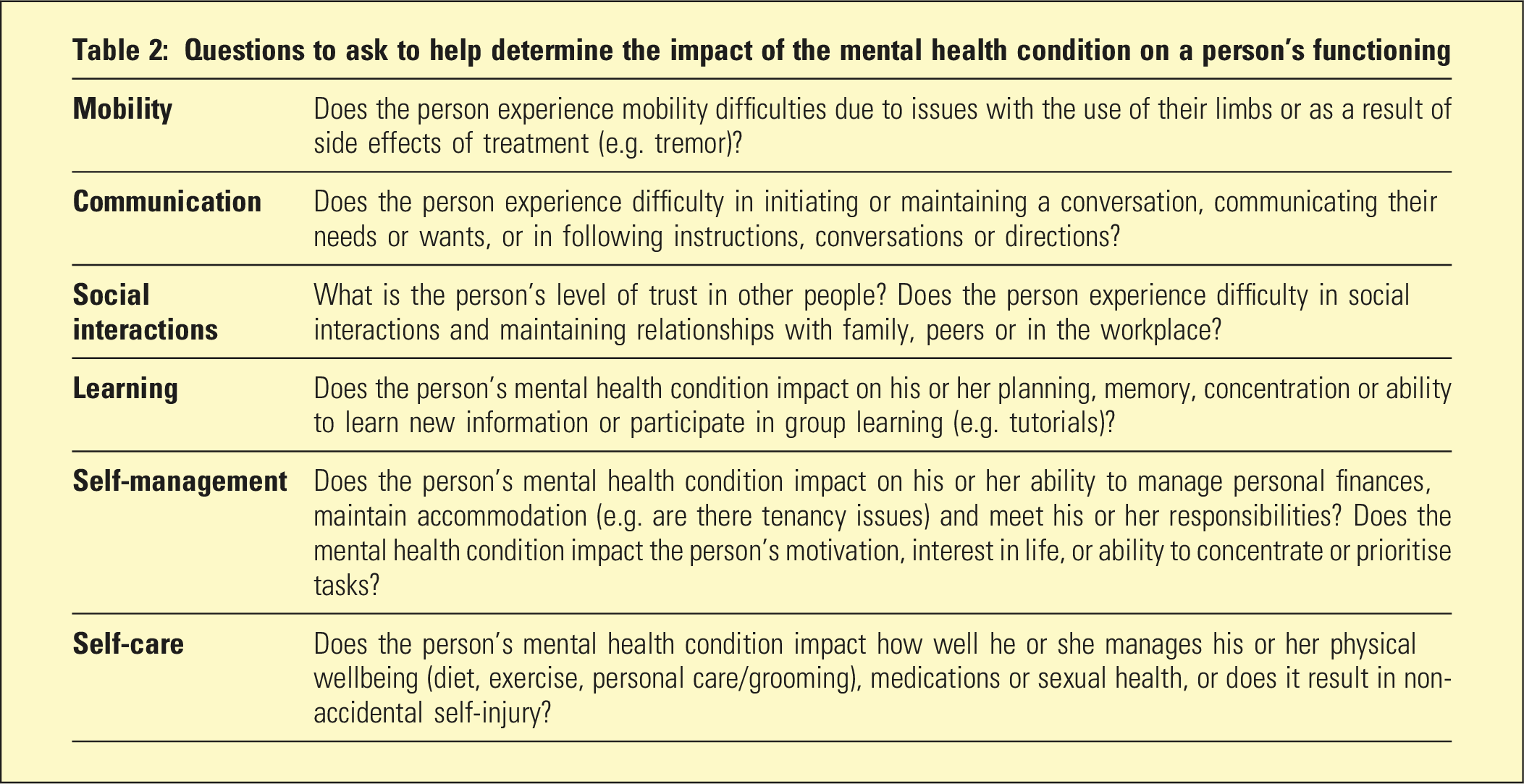
Tips to consider: • Provide examples to support the statements around functional capacity and use language that infers it is substantial and is beyond what people without a disability would experience and occurs every day. • Include an objective functional assessment rather than relying on the applicant’s self-reporting. • Only describe the domain(s) that a person is experiencing difficulties in. Minor impairments are not cumulative across multiple domains and do not add up to an overall substantial impairment. • Do not include details of acute, or current crises that are affecting the person. The NDIA will want to know what the person’s functional capacity looks like once the crisis has been resolved.
Ability to participate economically and socially 24(1)(d)
Unlike functional capacity, there is no threshold that a person must meet to satisfy this criterion. Rather, the evidence needs to demonstrate that the disability does affect a person’s ability to participate in the community. Generally, evidence provided to address criterion 24(1)(c) will suffice.
Likely to need support from the NDIS for their lifetime 24(1)(e)
The final criterion relates to the types of supports needed and who is responsible for providing these supports. To demonstrate that a person meets this criterion, it is important the evidence provided throughout the application only focuses on the impacts of the psychosocial disability and its associated impairments. If the evidence includes impairments related to underlying physical health condition(s), education, justice or other mainstream services, the NDIA may consider that the person needs support from those mainstream services rather than the NDIS.
Tips to consider: • Focus only on the MH condition. Do not bring in other related health conditions, for example, chronic health conditions, which are out of scope for the NDIS. • Where evidence around alcohol or other drug dependency is provided to support the application, the applicant will need to include additional evidence to show that their described functional difficulties are related only to the MH condition and not underlying substance misuse. This evidence will need to come from a suitably qualified medical professional and may include historical records demonstrating functional difficulties were present prior to alcohol/drug dependency or at a time where the person was undergoing a period of sobriety. • Decisions made around permanency and treatment are about what is reasonable for the person in the context that they live. As such, it is important that the context in which an individual exists is addressed in the cover letter to ensure the NDIA are aware of, and take into account any issues which may impede access (e.g. cultural/ethnicity factors).
Conclusion
The rapid roll-out of the NDIS has resulted in several implementation issues as HCPs, carers and people with disabilities begin to navigate the scheme. The EPD form is the only disability-specific access form currently available to assist individuals in applying to the NDIS. To support the use of the EPD form, and to provide information on the evidence required to meet the disability criterion for NDIS access, the TSP has developed online training modules and resources (www.tspforall.com.au) that are freely available to MH professionals.
Footnotes
Acknowledgements
The authors acknowledge the NDIA Mental Health team who helped develop the evidence of psychosocial disability form, in particular, Ms Elspeth Jordan who led the work from the NDIA. The authors also acknowledge staff from the Department of Social Services and the Department of Health and Aged Care who were involved in the development of the streamlined access process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Psychosocial Support Section of the Australian Government Department of Health and Aged Care.