
Abstract
Objective
To provide a brief clinical research update and commentary advice on the practical psychiatric care of patients suffering workplace bullying.
Conclusions
While there is empirical research on the prevalence and impacts of workplace bullying, there is a relative dearth of clinical research into psychiatric patient care. Accordingly, we provide commentary on practical considerations that assist in psychiatric care planning and delivery.
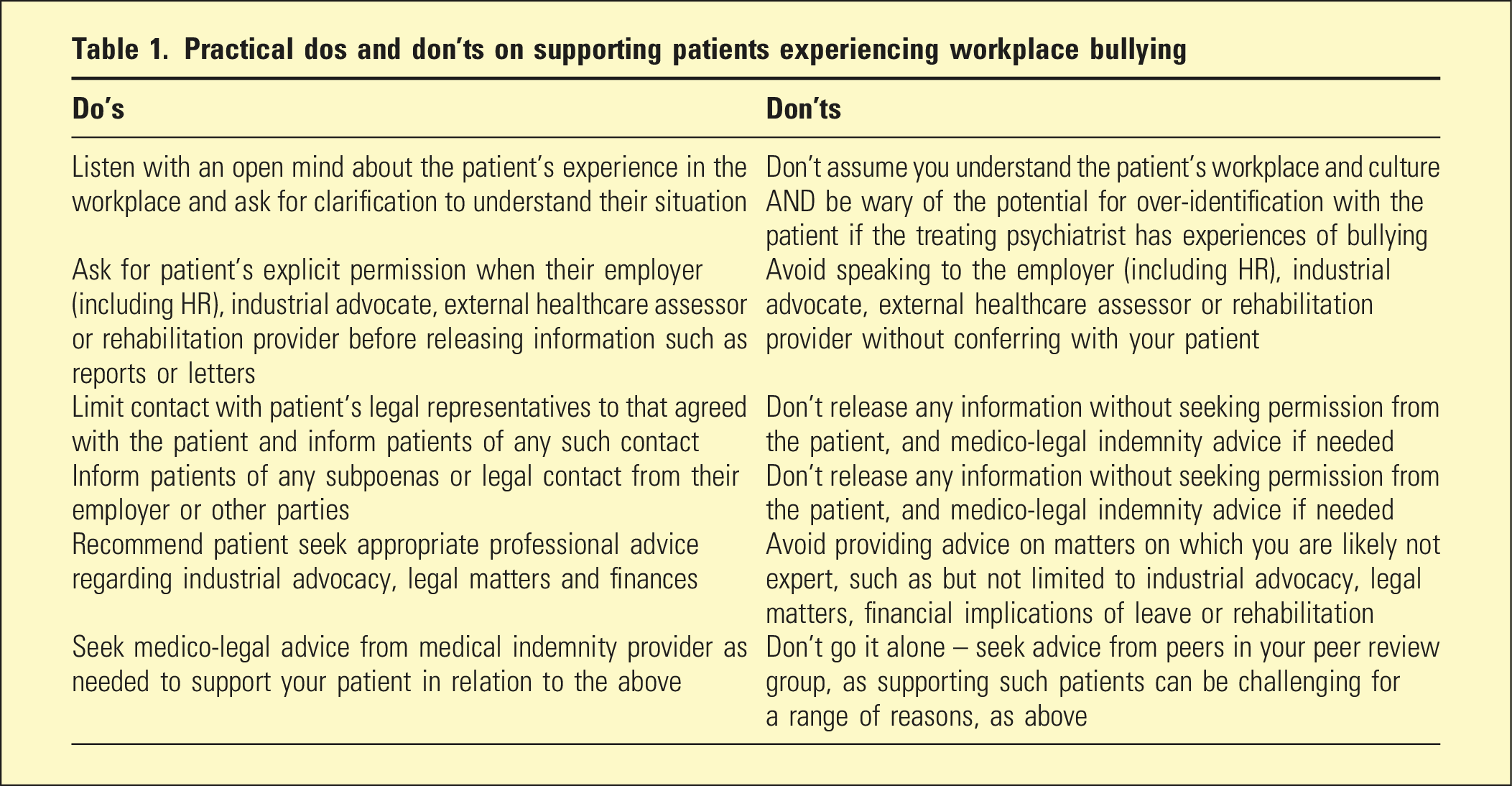
Practical dos and don’ts on supporting patients experiencing workplace bullying
These phenomena often occur in large hierarchical organisations where bullying is perceived within the person’s line-management structure. The reasons for self-labelling include the difficulty of researching all other viewpoints, such as a full 360-degree assessment of all involved including the alleged perpetrator and their supporters, the target and bystanders. 2 Following pioneering Scandinavian research into the phenomenology of workplace bullying,3,5 interdisciplinary research has enriched the understanding of the antecedents, impacts and organisational and individual workplace-based interventions.6,7
The worldwide prevalence of bullying varies by definition, but the most recent meta-analysis in 2010 indicated the rate was 15%. 8 In terms of the psychological impacts of workplace, the most recent (2015) meta-analysis (n = 115,783) indicated there were positive cross-sectional associations of bullying with depression (r = 0.28, CI = 0.23–0.34), anxiety (r = 0.28, CI = 0.29–0.40) and psychological stress-related conditions (r = 0.37, CI = 0.30–0.44). 9 Pooled longitudinal studies (n = 54,450) showed that workplace bullying was related to mental health complaints over time. 9 Recent Australian data found that the prevalence of workplace bullying decreased from 9.7% in 2014–15 to 8.6% in 2020–21. 10
Despite burgeoning research, there remain knowledge shortfalls regarding causality, processes, mediators and moderators. 1 This has hampered effective research into interventions, rehabilitation of both victims and perpetrators, as well as the remediation of work environments to prevent and treat workplace bullying. 1 We focus on an overview of clinical interventions for victims that can be provided by psychiatrists, primarily in outpatient settings. For broader generalisability, we do not focus on patients from any particular workplace. Medico-legal psychiatric assessments and direct industrial advocacy are outside the scope of this paper. Workplace harassment, although often associated with bullying, warrants separate discussion, as there is a separate but related evidence-base and potentially, different approaches in clinical care.
Intervention and rehabilitation for patients experiencing workplace bullying
Primary prevention aims to forestall occupational risks before they occur. 7 Secondary prevention implies early intervention, which is practically difficult due to the insidious nature of bullying. Secondary prevention involves both investigation of complaints, as well as counselling and psychotherapy of bullying victims. 7 Tertiary prevention refers to interventions that ensure the sustainability of treatment. 7
There is a relative dearth of clinical psychiatric research into specialist medical care and secondary interventions for patients presenting with symptoms arising from workplace bullying. However, there is some research evidence on counselling 11 and inpatient treatment of bullying victims. 12 As there are specific assessment and treatment guidelines for a range of the resultant mental disorders, such as anxiety and depression, we will focus on the framing of collaborative care and practical advice on specific interventions relating to the impacts of bullying.
Secondary prevention and treatment: General approaches
Direct workplace interventions are complex due to differing organisational and individual patient agendas. Unless employed by the work organisation, psychiatrists will not necessarily have right of entry or authority within that organisation. If psychiatrists are employed by the organisation with which the patient has a workplace bullying complaint, there is a potential material conflict of interest with the patient’s welfare. For these reasons, our focus in on the psychiatrist as a medical specialist providing a consultation service to a patient who self-labels as having been bullied in the workplace. Some additional practical tips (Do’s and Don’ts) are summarised in Table 1.
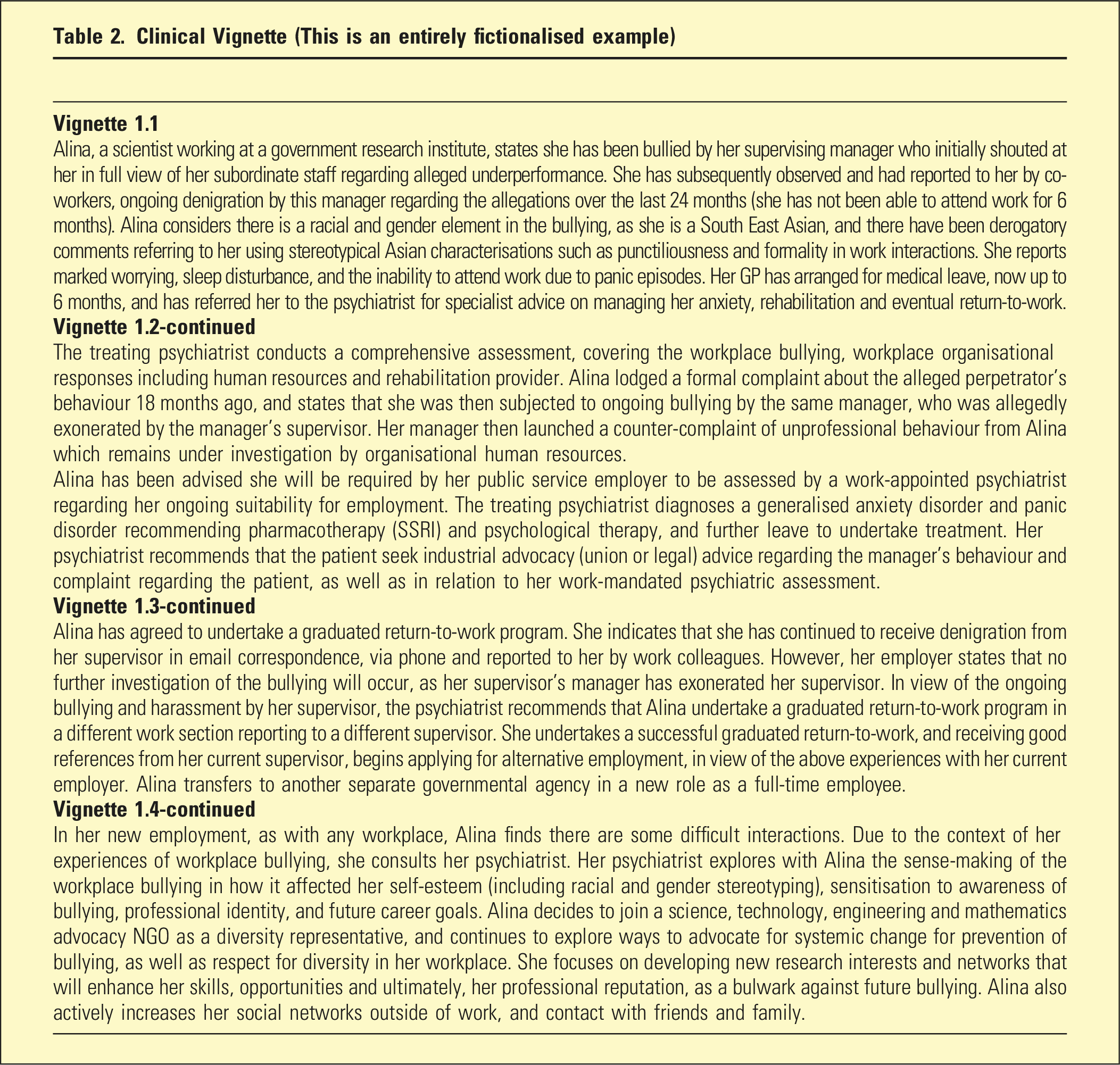
Clinical Vignette (This is an entirely fictionalised example)
The psychiatrist’s role is as a medical specialist advocate for the patient and includes the following: clarification of the workplace context, social relations and bullying; diagnosis; the need for ongoing leave; workplace and worker duty modification; psychological and pharmacotherapy; graduated return-to-work, and; if absolutely necessary medical retirement as a last resort.
Patients should be advised to seek professional industrial advocacy through the relevant union, professional organisation or legal advisor, within the legal framework that exists – in Australia this is governed by the Fair Work Act as well as Workplace Health and Safety legislation. 14 (See Table 2, Vignette 1.2 for an example)
Sometimes, patients will make a worker’s compensation claim in relation to the psychological injury, and if the claim is accepted, introduces the compensation provider into management of rehabilitation. This adds a further level of complexity to management, as the provider may then pay the psychiatrist and other health providers for treatment of the patient. However, the psychiatrist necessarily must act in the patient’s best interests, and not as an agent for either the employer or compensation provider. For example, the worker’s compensation provider may request a report on the patient’s condition, treatment and suitability for work. The psychiatrist advises the patient of the request for information and discusses a collaborative care approach to response, based on the patient’s best interests.
When a patient suffers severe anxiety, depression and/or psychological stress, an inpatient admission may be required for severe debilitation, risk of self-harm or to facilitate a rapid change of pharmacotherapy, among other reasons. In such circumstances, patients will need private health insurance, approval from the worker’s compensation provider or an admission to hospital.
When patients are able to make a graduated return-to-work, there may be a number of workplace conditions that are recommended by the psychiatrist in the context of the bullying such as the following: changes in work duties to allow for recovery; change of supervisor away from the alleged bully and team (which may include transfer to another part of the organisation if practicable); and in some circumstances, a departure to alternative employment (See Table 2, Vignette 1.3 for an example). However, some workplaces are so toxic from a bullying and organisational cultural perspective that employees may need to leave to prevent burnout, and for their own health. 15
Lastly, some patients have ongoing psychiatric symptoms that present an insurmountable challenge for recovery. These patients may need to consider a medical retirement, and the psychiatrist should recommend the patient seek further industrial, legal and financial advice.
Even when returning to work, and more for those unable to do so, patients face substantial existential issues from being subjected to bullying (See Table 2, Vignette 1.4 for an example). These issues can include the loss of professional identity, and the group processes of scapegoating and ostracization, as well as their impact on the patient and their family. Psychotherapy might include focus on the making sense of the bullying episode in terms of the effect on identity, how to recognise and prevent further bullying, and goals for sustainable recovery including improving professional and social supports and networks.
Conclusions
Workplace bullying is an important clinical patient care issue for psychiatrists. We have provided a brief clinical update and commentary on clinical approaches to management.
There are a range of societal, organisational, workplace, group and individual factors related to bullying that warrant separate research, analysis of the evidence and discussion, including related workplace behaviours such as harassment, and the broader bio-psycho-socio-cultural context.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
No ethics approval or consent was required as this paper does not involve research with humans or animals.