
Abstract
Objective
Borderline personality disorder (BPD) is common and poses many clinical challenges. Despite limited evidence of effectiveness, psychotropic medications are often prescribed. We aimed to characterise overdose presentations in patients with BPD.
Method
This is a retrospective observational series of patients with BPD presenting to a tertiary hospital following an overdose from January 2019 to December 2020. Medical records were reviewed to determine baseline characteristics, overdose details, clinical features, treatment, and disposition.
Results
There were 608 presentations in 370 people (76% female), median age 28 years (range 16–75 years). The majority (331[89%]) of patients were prescribed at least one psychotropic medication, with 129 (35%) being prescribed three or more different psychotropic agents. Of the total prescribed psychotropics, 520/1459 (36%) were for off-label indications. The majority of agents (860/1487[58%]) taken in overdose were prescribed. The commonest drug classes taken in overdose were benzodiazepines (241[16%]) and antipsychotics (229[15%]). Severe toxicity occurred in 99 (16%) cases with either coma (GCS<9) or hypotension (systolic BP <90 mmHg). The commonest agent associated with severe toxicity was quetiapine 39/99 (39%).
Conclusions
Psychotropic polypharmacy is common in BPD, often with off-label indications. Prescribed medications are commonly taken in overdose. Quetiapine is over-represented both in off-label prescribing and associated harm.
Borderline personality disorder (BPD) is characterised by marked impulsivity and a pervasive instability of interpersonal relationships, self-image and affects. 1 In Australia, the prevalence of BPD in adults is estimated to be 1–3.5%.2,3 It is one of the most common personality disorders encountered in the clinical setting, contributing up to 43% of all psychiatric inpatients and 23% of outpatients. 4
In addition to an association with severe functional impairment and an array of comorbid psychiatric and substance use disorders,5,6 patients with BPD are subjected to a rate of mortality by suicide 50 times that of the general population. 7 On average, BPD patients make three lifetime suicide attempts, with the majority encompassing a drug overdose 8
Psychosocial therapy is well proven and recommended as the mainstay intervention for BPD. 9 Although there is insufficient high-quality evidence substantiating the efficacy of pharmacological treatment, 10 patients have historically been prescribed a multitude of psychotropic agents including antidepressants, mood stabilisers and neuroleptics. 11 Polypharmacy is common and serves as a significant safety concern in this population.
There is limited literature on the clinical presentation of deliberate self-poisonings in patents with BPD. Case reports often describe an overdose of multiple agents resulting in severe toxicity.12–15 Our study aims to characterise deliberate self-poisoning in patients with BPD who present to a clinical toxicology unit.
Methods
Study design and setting
This was a retrospective observational series of patients with a documented history of BPD presenting to the Princess Alexandra Hospital, an adult (≥16 years old) tertiary hospital located in Brisbane, Queensland, Australia. The Princess Alexandra Hospital has a dedicated Clinical Toxicology Unit which manages all poisoning presentations, with approximately 2000 annual admissions. These presentations are prospectively entered into a relational database by the unit’s medical staff which undergoes weekly auditing and data review. Information captured in this database includes patient demographics, clinical features, investigations, treatments and complications. Ethics approval has been acquired to utilise this database and relevant patient medical records in observational research.
Selection of patients
A database search was conducted for all presentations of deliberate self-poisoning over a 2-year period, from January 2019 to December 2020. These entries were then cross-referenced with a state-wide mental health clinical record application, the Consumer Integrated Mental Health and Addiction (CIMHA). Patients with a documented formal diagnosis of BPD or emotionally unstable personality disorder (EUPD) in CIMHA were included in the study.
Data collection
Elements of each presentation were extracted from the unit’s database onto a data collection sheet. These included baseline characteristics (age, sex), ingestion details (agent, co-ingestion), clinical features of severe toxicity (coma [Glasgow Coma Scale (GCS) < 9], hypotension [systolic blood pressure (SBP) < 90mmHg], death), treatments (inotropes, intubation), disposition (intensive care unit (ICU) or mental health admission) and length of stay.
Concomitant formal mental health diagnoses were also extracted from CIMHA. A review of the patient’s clinical records was performed to assemble a list of prescribed medications that the patient was taking at the time of their presentation. Prescribed psychotropic medications were appraised in the context of the Therapeutic Goods Administration (TGA) designated clinical indications to determine if it was consistent with prescription guidelines or prescribed for an off-label indication. Psychotropics included antipsychotics, antidepressants, mood stabilisers and benzodiazepines (including Z-drugs). Double extraction of the data was carried out for the first 10% of records of which there was excellent agreement with the remaining 90% performed by a single extractor.
Analysis
Descriptive statistics were employed with continuous variables reported as medians, interquartile ranges (IQRs) and ranges. All figures were created in GraphPad Prism 8 for Mac OS (GraphPad Software, San Diego, CA, USA).
Results
Baseline characteristics
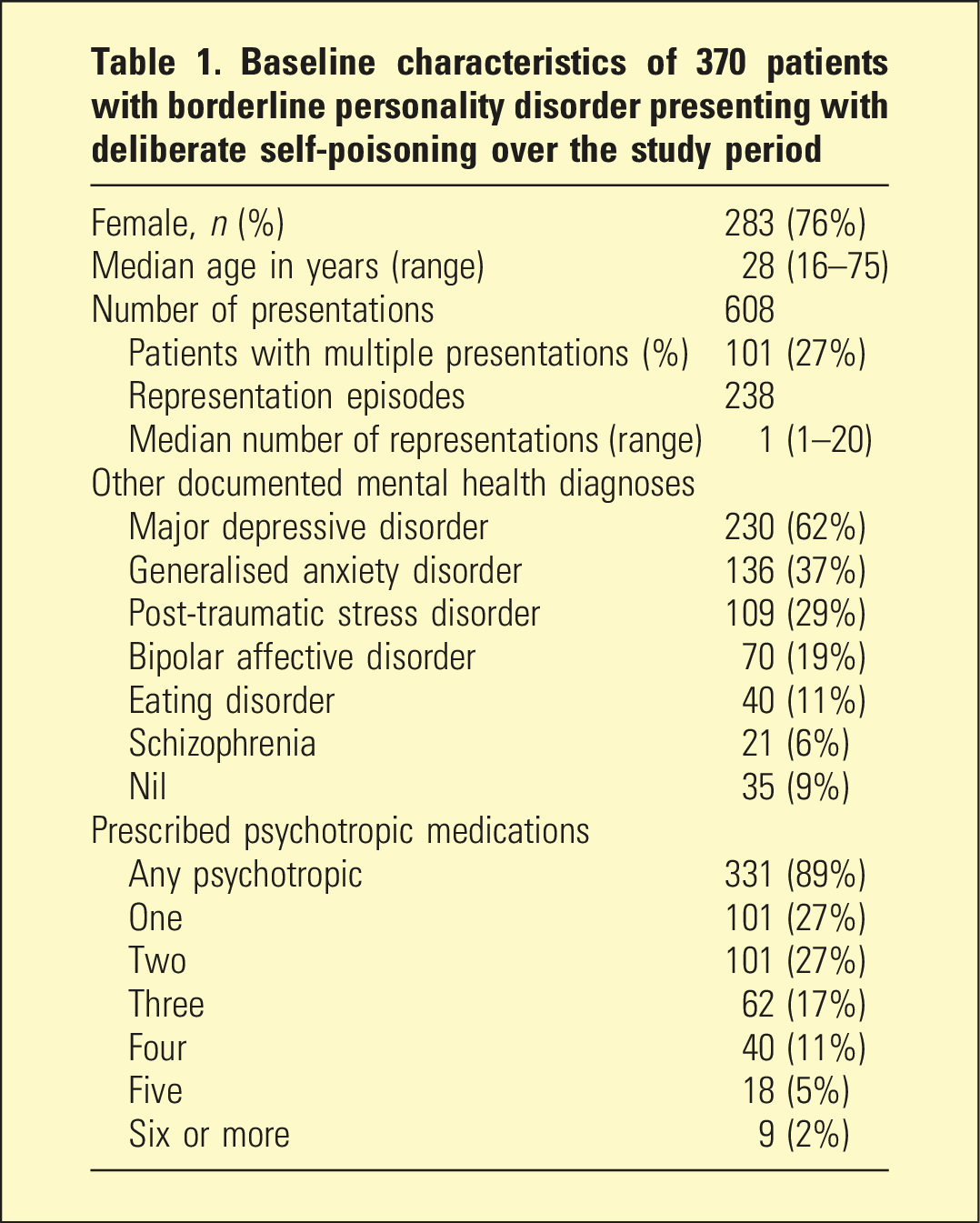
Baseline characteristics of 370 patients with borderline personality disorder presenting with deliberate self-poisoning over the study period
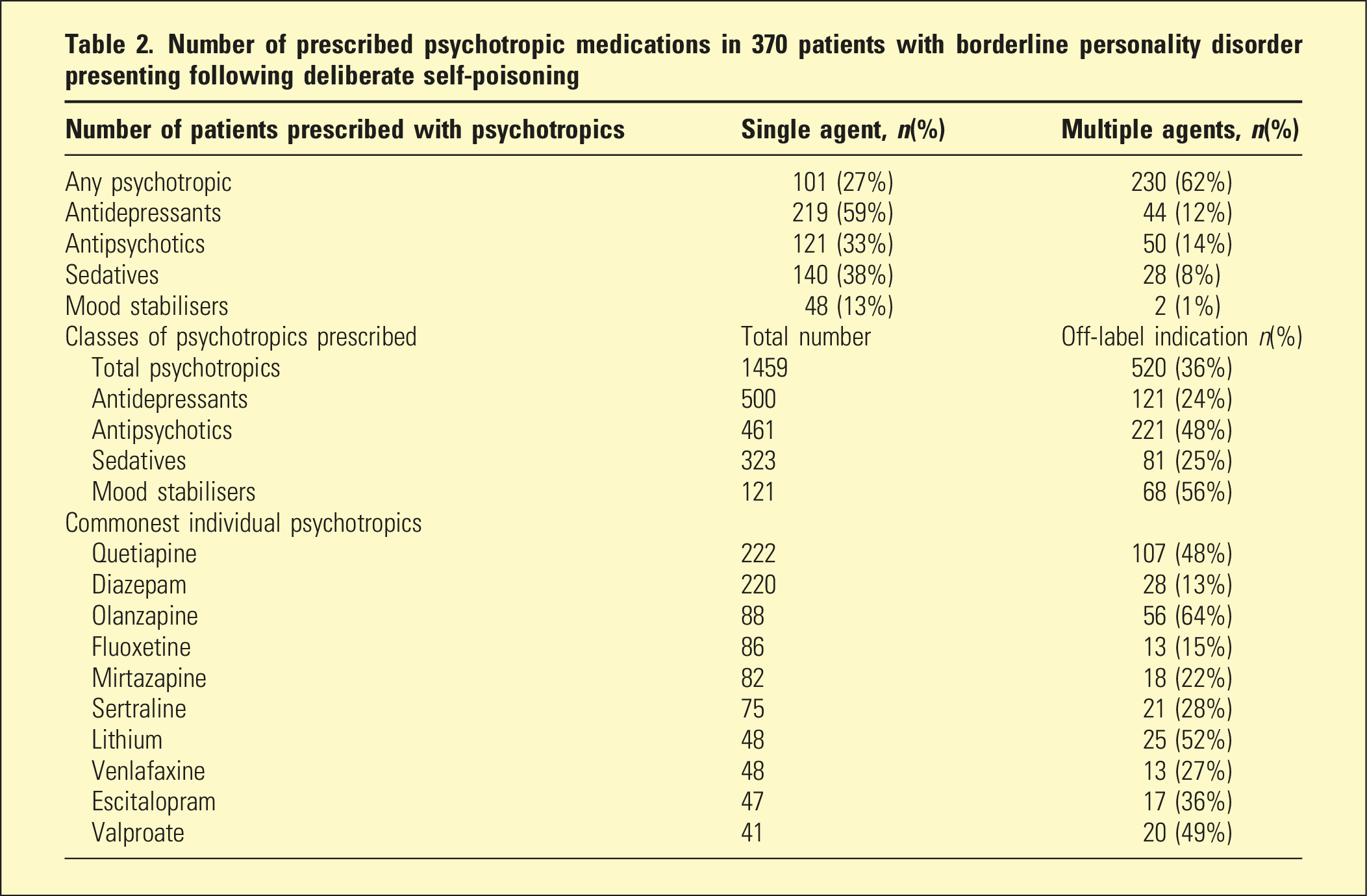
Number of prescribed psychotropic medications in 370 patients with borderline personality disorder presenting following deliberate self-poisoning
Agents taken in overdose
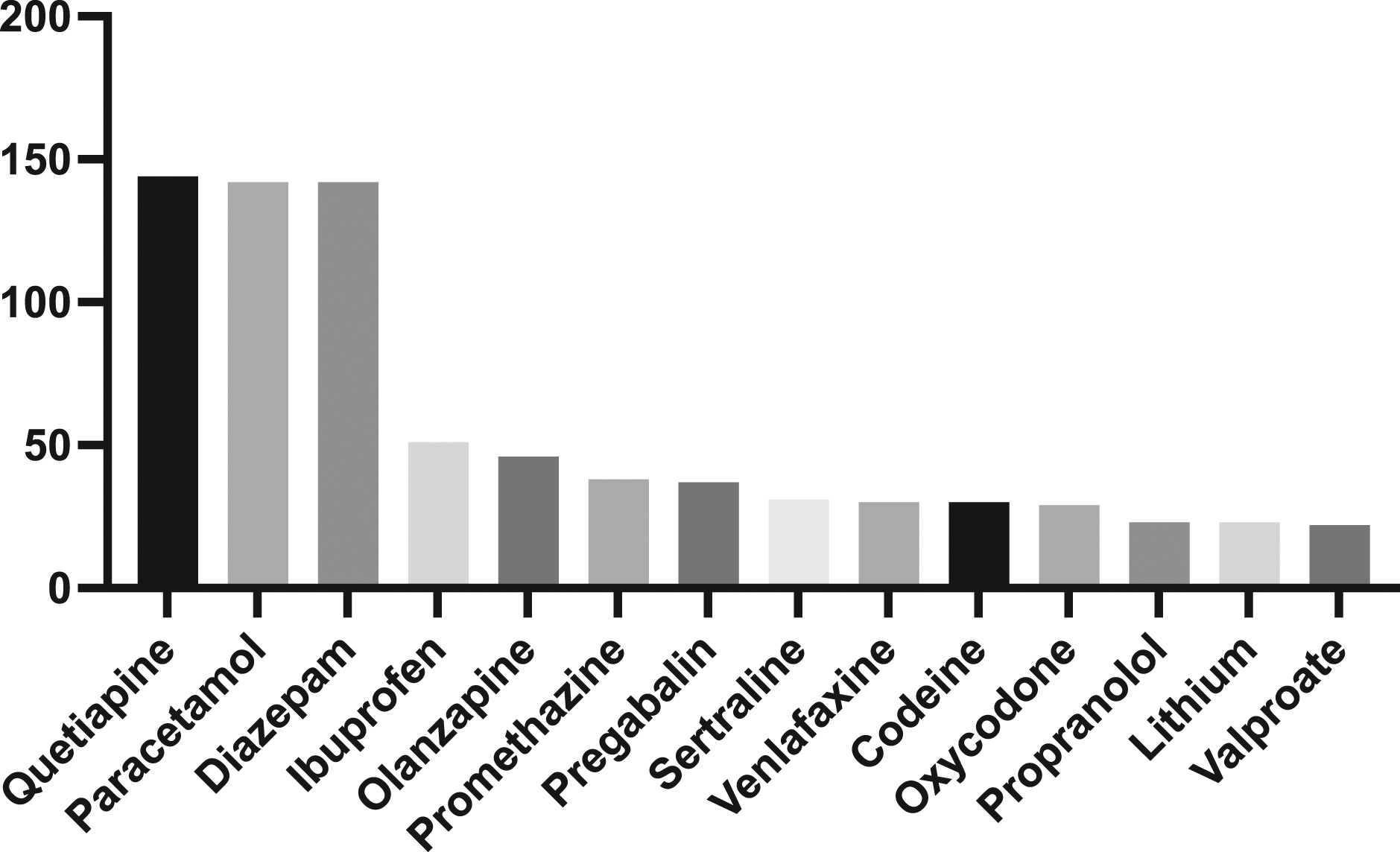
Of the total 1487 agents taken in overdose in this series, 860 (58%) were prescribed. A single agent was ingested in 207 (31%) presentations while the remainder were polypharmacy overdoses. The most common class of pharmaceuticals taken in overdose was benzodiazepines, followed by antipsychotics and over-the-counter analgesics [Figure 1]. The most common single agent taken in overdose was quetiapine, followed by paracetamol and diazepam [Figure 2]. There were a total of 695 (47%) psychotropics taken in overdose, 583 (84%) of which were prescribed with 210 (36%) of these prescriptions for off-label indications. Pharmaceutical drug class taken in deliberate self-poisonings. Individual agents taken in deliberate self-poisonings.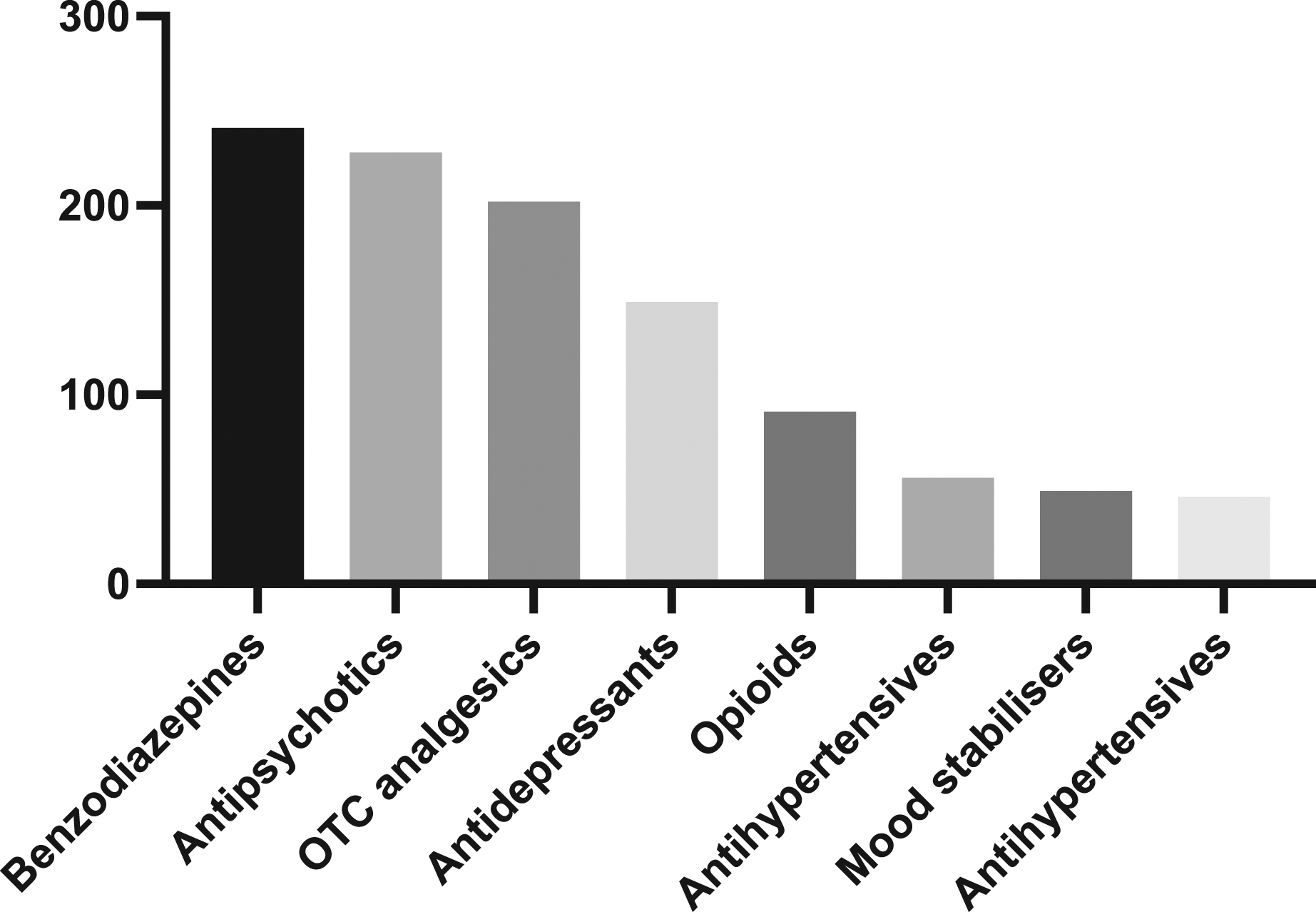
Severe Toxicity
Severe toxicity occurred in 99 (16%) presentations, with overdose resulting in hypotension and coma in 67 (11%) and 54 (9%) cases respectively. Inotropes were administered in 13 (2%) cases and intubation was performed in 23 (4%). Psychotropics were taken in 84/99 (85%) cases of severe toxicity. The commonest agent ingested in patients with severe toxicity was quetiapine (39 [39%]), followed by diazepam (30 [30%]) and pregabalin (14 [14%]) [Figure 3]. Individual agents taken in overdose in patients who developed severe toxicity.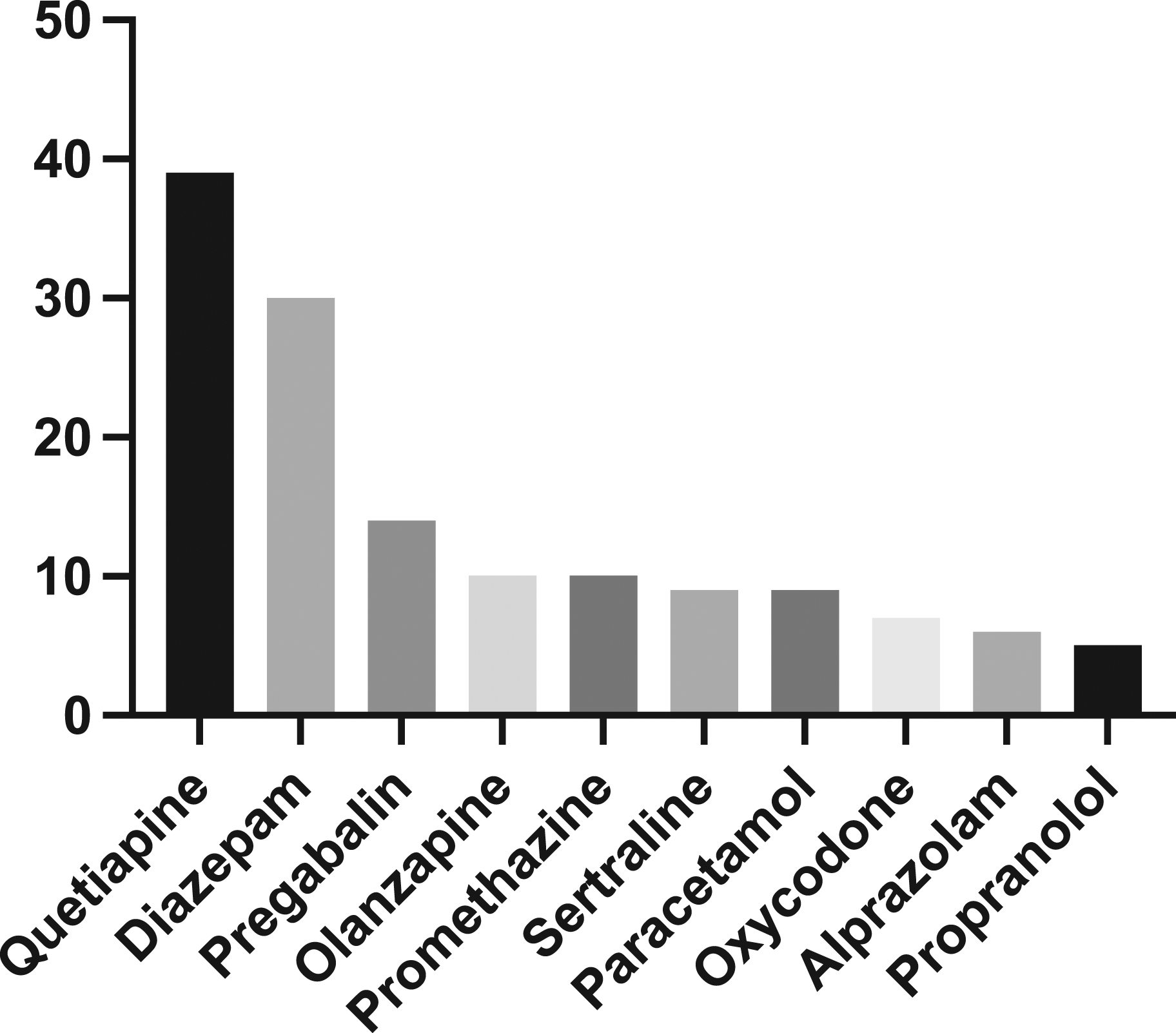
Disposition
The majority of patients (559 [92%]) were managed solely in the ED, which included an admission to the short-stay unit under the clinical toxicology team. There were 23 (4%) presentations that were admitted to the ICU and 26 (4%) that were admitted to a hospital ward. The median length of stay was 15.1 h (IQR 8.1–23.1 h). Following the resolution of toxicity there were 87 (14%) mental health admissions with all remaining patients discharged to their place of residence. There were no deaths in this series.
Discussion
Psychotropic polypharmacy is common amongst patients with BPD, with many prescribed for off-label indications. In our series, most patients with BPD took medications they were prescribed with in overdose.
Despite limited evidence for pharmacotherapy in the treatment for BPD, 9 prescription rates are high. It is estimated that 78–84% of patients with BPD are prescribed psychotropics for a sustained period of time.16–18 Polypharmacy is exceedingly common in this group, occurring in 67–84% of patients.19–22 This is comparable to our study, whereby 84% are prescribed any psychotropic and 35% are receiving three or more agents. The prescription of multiple psychotropics appears to contradict the consensus that they should be reserved as an adjunct to psychosocial interventions for specific symptoms or psychiatric comorbidities.4,7,23 Chanen and Thompson 9 advocates for caution in prescribing psychotropic pharmacotherapy, recommending the use of single drugs for a limited amount of time, and the judicious cessation of ineffective drugs upon reassessment.
While gold standard treatment – in the form of psychotherapy – exists for BPD, this is a process that requires a substantial time commitment to make functional and symptomatologic gains. 24 Meanwhile, many consumers present in significant distress prompting clinicians to prescribe medications such as quetiapine and benzodiazepines in order to address specific symptoms such as emotional dysregulation, insomnia, impulsivity, self-harm or suicidal ideation and intense anger.25–27 However, while certain psychotropics can improve specific BPD symptoms, none have been demonstrated to significantly reduce the overall severity of BPD.28,29 If used to treat acute crises, efforts should be undertaken to actively mitigate downstream risks associated with their use, such as limiting the quantity dispensed and ensuring adequate and timely follow-up. Targeting specific BPD symptoms with psychotropics may counterintuitively augment polypharmacy. This is perpetuated by multiple factors, including a limited number of trained clinicians who are available to provide opportune psychotherapeutic interventions, 30 and punitive responses of some healthcare providers to self-harm behaviour. It is hoped in the future that this will improve with evolving awareness and positive attitudinal shifts in the landscape of the mental health system. 31
There is limited medical literature regarding off-label prescriptions in patients with BPD. In a survey conducted at a large UK psychiatric hospital, 80% of BPD patients were receiving one or more psychotropics exclusively for BPD, all of which were prescribed off-label. 32 Another study of prescription practices among Italian psychiatrists found that more than 50% frequently prescribed second-generation antipsychotics for off-label indications, which include BPD amongst other psychiatric disorders. 33 In our study, 36% of all psychotropics prescribed and 36% of the prescribed psychotropics taken in overdose were deemed to be off-label as per TGA guidelines.
In our study, quetiapine is over-represented as the single most commonly prescribed psychotropic as well as the agent most frequently ingested in overdose. More concerningly, it is the single agent most associated with severe toxicity. The high incidence of quetiapine prescriptions among the BPD population is corroborated in literature.19,34,35 Bridler and Häberle 19 described a significant recent increase in prescription rates from an average of 7.5% in 2001–2003 to 32.9% in 2009–2011. While trials of quetiapine in BPD patients have demonstrated some improvements in mood, impulsivity and aggression,25,26 this is accompanied by significant dose-related adverse effects. 36 Rising prescription rates have been strongly correlated with an increase in the rates of quetiapine-associated poisoning and mortality.37–39 Given that no specific therapy reverses quetiapine toxicity, 40 this accentuates a need for caution in prescribing, especially off-label, with an overall objective of harm minimisation.
There are several limitations in our study. The most important are related to its retrospective design. Documentation in medical records may have been inaccurate or incomplete, particularly in relation to medication history. This effect should have been limited as prescription dispensing data from the patient electronic health records was cross-checked where available. Other factors beyond the scope of this retrospective series included markers of an increased severity in illness such the number and lethality of prior suicide attempts, prior electroconvulsive therapy and unsuccessful trials of intensive psychotherapy. Furthermore, agents taken in overdose relied on patient history without objective toxicological analysis. Finally, our study used only public health system medical records. Any additional mental health diagnoses (such as bipolar affective disorder) in the private health system were not recorded which may mean rates of off-label prescribing were overestimated.
Conclusion
Deliberate self-poisoning in BPD patients is a common and prescribed medications are taken in the majority of cases. Psychotropic polypharmacy, including off-label prescribing, is common and may contribute to both the number and severity of overdose presentations. Quetiapine is over-represented in off-label prescriptions and ensuing harm following overdose. This research highlights the importance to optimise current prescribing practices in order to emphasise treatment efficacy while minimising potential harm from pharmacological misuse.
Footnotes
Author’s note
This study has been presented via posters at the TAPNA conference and the PAH Health Symposium, in addition to an oral presentation at the QLD Autumn Symposium in 2021.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.