
Abstract
Objective:
To explore the rates and characteristics of self-harm across the Kimberley region of Western Australia.
Method:
Retrospective, cross-sectional audit. We obtained and descriptively analysed routinely collected self-harm data from the Kimberley District of the Western Australia Police Force (2014–2018) and the Emergency Department Data Collection (June 2017–December 2018). Variables included age, sex, Indigenous status, time of incident, and alcohol and drug use.
Results:
The rate of emergency department attendance for self-harm was three times higher in the Kimberley than the rest of Western Australia. Both emergency department and police data showed a disproportionately high percentage of incidents involving Aboriginal people, with highest rates in the 15–19 and 20–24 year age groups. Almost 80% of self-harm events recorded by police involving individuals aged 25–50 years involved alcohol. Many self-harm incidents occurred in the evening and at night.
Conclusions:
The rates of self-harm across the Kimberley region from 2014–2018 are unacceptably high. Increased funding and alignment of services to meet regional need are required as part of a holistic effort to reduce regional rates of self-harm.
Aboriginal Australians have demonstrated a significant capacity for strength and resilience in the face of substantial adversities. However, colonisation and the enduring experience of marginalisation, racism and intergenerational trauma coalesce with other social determinants of health to create much higher levels of psychological distress among Aboriginal Australians than non-Indigenous Australians.1,2 An indicator of distress is the disproportionately high rates of suicide in Aboriginal Australians.3,4 In the remote and expansive Kimberley region, 42% of the population identify as Aboriginal and/or Torres Strait Islander (with Aboriginal people comprising the vast majority). The age-adjusted suicide rate for Kimberley Aboriginal people (2013–2017), was 5.18 per 10,000 people, compared to a national rate of 1.22.5,6 The suicide rate among Aboriginal people in the Kimberley is twice as high as the suicide rate among all Indigenous Australians. 5 Another indicator of psychological distress is deliberate or intentional self-harm. 7 During a 2014 study, Aboriginal people in the Kimberley region had a hospital self-harm presentation rate at ten times that of the international self-harm presentation rate.3,8
Self-harm data across the Kimberley region are collected by multiple agencies in the region; the fragmentation of data and non-standardised definitions of self-harm hamper effective analysis. Notwithstanding these limitations, analysis of existing data is important to monitor trends in the region. This paper presents self-harm data from 2014–2018 from two major collectors of this information (Western Australian (WA) Police and WA Health Emergency Department Hospital Data). We aimed to identify rates of self-harm across the region including demographic and time of day trends. Results from the data help inform the innovation required in the resourcing and delivery of services to align to community need and positively impact on regional self-harm rates.
Methods
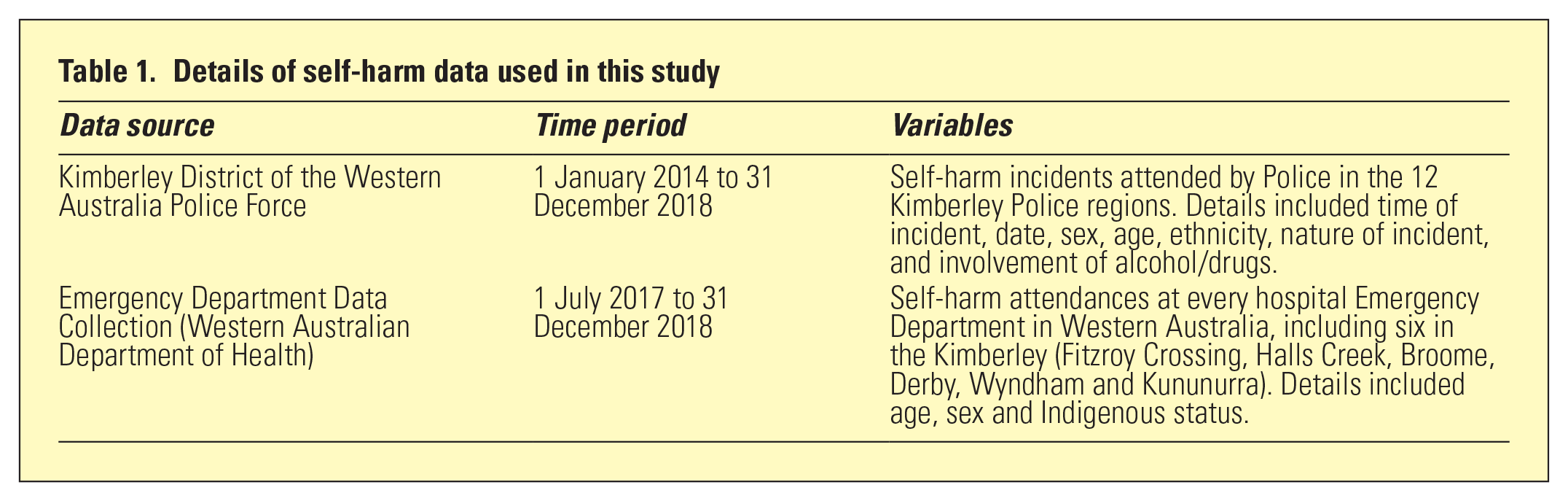
This study was a retrospective, cross-sectional audit of routinely collected self-harm data obtained from the Kimberley District of the WA Police Force (WAPF) and the WA Department of Health Emergency Department Data Collection (Table 1). Data analysis was descriptive, with no linkage between the two datasets. This study was supported by the Kimberley Aboriginal Health Planning Forum Research Subcommittee. Ethics approval was conferred by the WAPF, the Department of Health Human Research Ethics Committee (RGS0000001110) and the WA Aboriginal Health Ethics Committee (Project 855).
Details of self-harm data used in this study
Results
The recorded rate of attendance to Kimberley Emergency Departments for self-harm was three times the rate for the rest of WA (Table 2). In the Kimberley, 81% of those who presented for self-harm were Aboriginal and/or Torres Strait Islander people and 59% were females. Both emergency department and police data showed highest rates of self-harm incidents in the 15–19 year age group, followed by age 20–24 years (Table 2).
Incident rates of self-harm by age group attended by the Kimberley District of the WAPF and emergency departments in Kimberley and elsewhere in WA
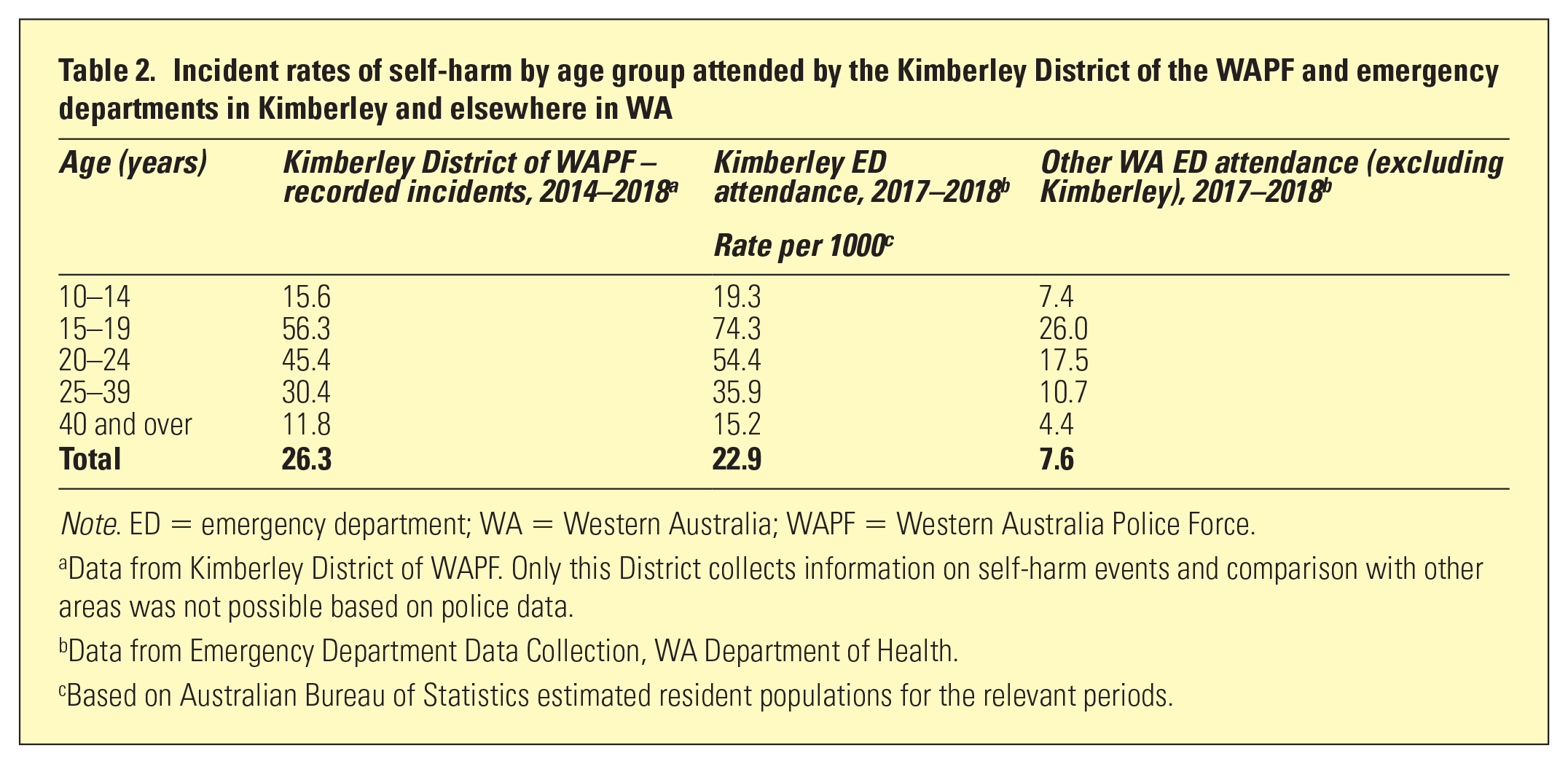
Note. ED = emergency department; WA = Western Australia; WAPF = Western Australia Police Force.
Data from Kimberley District of WAPF. Only this District collects information on self-harm events and comparison with other areas was not possible based on police data.
Data from Emergency Department Data Collection, WA Department of Health.
Based on Australian Bureau of Statistics estimated resident populations for the relevant periods.
Of self-harm incidents recorded by police, 92% involved Aboriginal and/or Torres Strait Islander people and 57% involved females (Figure 1). The rates in local government areas within the Kimberley ranged from 20 to 33 per 1000 population (Table 3). Self-harm events were most common between 9 pm and midnight, although this pattern varied by age (Figure 2). In those aged under 25 years, self-harm events were much more evenly spread across the day, while in those aged 25–39 years, there was a substantial peak period of risk between 9 pm and midnight. For those 40 years and over, there was a more modest peak risk period earlier in the evening between 6 pm and 9 pm. There was a modest trend by day of week, with highest rates on Fridays and Saturdays.
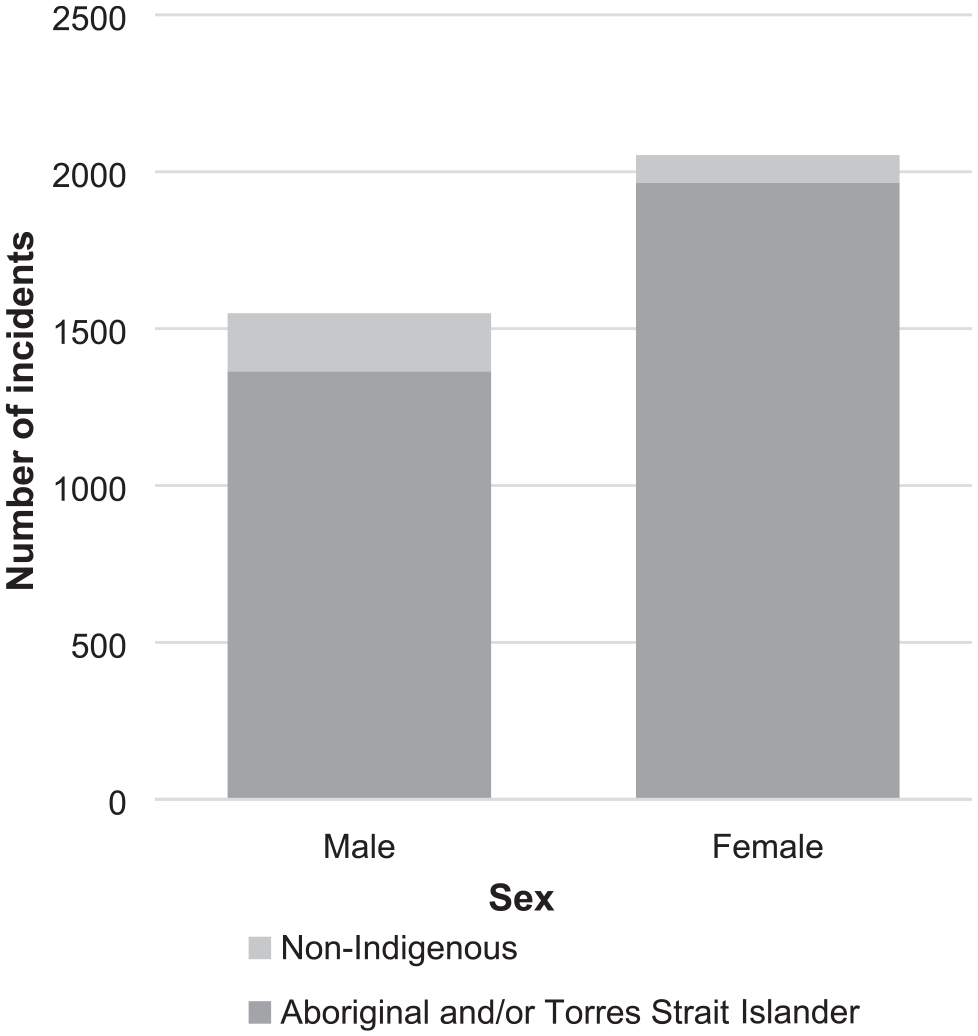
Number of self-harm incidents by Indigenous status and sex recorded by the Kimberley District of the Western Australia Police Force, 2014–2018.
Average annual self-harm incidents attended by the Kimberley District of the Western Australia Police Force in each local government area, a 2017–2018
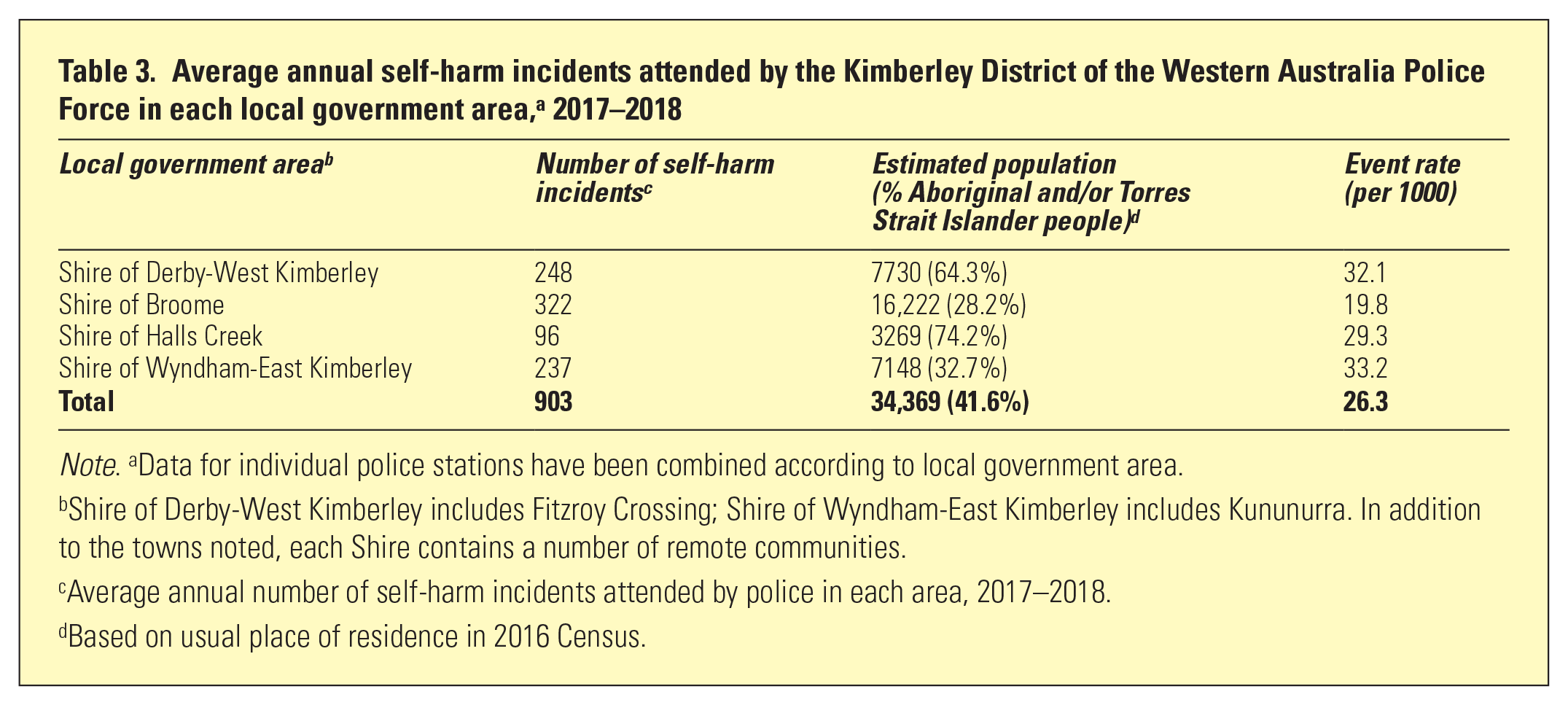
Note. aData for individual police stations have been combined according to local government area.
Shire of Derby-West Kimberley includes Fitzroy Crossing; Shire of Wyndham-East Kimberley includes Kununurra. In addition to the towns noted, each Shire contains a number of remote communities.
Average annual number of self-harm incidents attended by police in each area, 2017–2018.
Based on usual place of residence in 2016 Census.
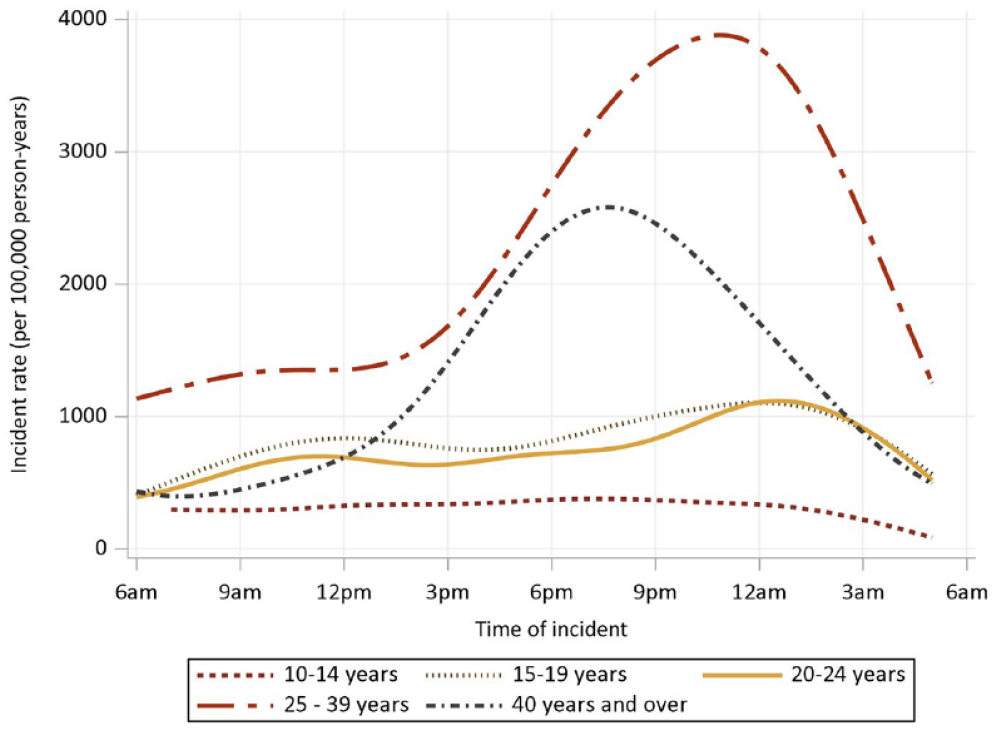
Rates of self-harm incidents attended by Kimberley District of the Western Australia Police Force by age group and time of incident, 2014–2018.
Alcohol and/or drugs were recorded as being involved in 65% of self-harm events attended by police (90% of these recorded alcohol only). Alcohol-related self-harm events were slightly more common on Friday and Saturday evenings, and most common in individuals aged between 25 and 50 years where almost 80% of self-harm events were recorded as involving alcohol.
Discussion
Our findings contribute to an understanding of self-harm characteristics and rates across the Kimberley. The results build from the 12-month Kimberley self-harm data audit of 20143,8 and demonstrate that over a 4-year period rates of self-harm across the region remain unacceptably high. Aboriginal people, particularly Aboriginal young people and Aboriginal people affected by alcohol, are over-represented in the self-harm data. Further, our findings show a large amount of self-harming occurring in the evening and at night.
The deeply complex drivers of Aboriginal distress and self-harming require urgent resourcing in a manner that supports self-determination. Mental health funding is currently weighted to acute service provision, 3 and it is difficult to quantify what is spent on prevention at the regional level. 9 Social and emotional well-being services across the region, as delivered by Aboriginal Community Controlled Health Services (ACCHS), are lacking the required financial investment to operate the culturally and therapeutically skilled multidisciplinary teams they critically require. Our findings also support the need for regional stakeholders, their funders and Aboriginal community members to consider the redesign, or addition, of services to respond to the high rates of self-harm occurring in the evening and night time. Across the Kimberley, very few, if any, therapeutically based prevention and early intervention services are available outside business hours. 9
In addition to improved service responses, this paper highlights the need for regionally agreed upon definitions of self-harm 10 and a subsequent means to disseminate these definitions to the regional services involved in data collection. This is particularly important given high workforce turnover across the region and the role of non-clinicians (WA Police) in recording self-harm data. Additionally, we recommend that a regional protocol be developed to guide the management and aftercare of self-harm presentations.11,12 The development of this framework would need to be cognisant of the limitations of data sharing across services and balance the cultural and theraputic needs of individuals with the resource and service contraints of the Kimberley.
It is important to note several limitations of the data in the current study. First, many people self-harming across the region may never come to the attention of police and/or the hospital. For Aboriginal people, a fear of mental health stigma, 13 historical difficulties with police 14 and challenges in accessing appropriate health care 15 are barriers to seeking service-based help. It is not possible to determine multiple incidents involving the same individuals in these data, or to what extent emergency department presentations were also incidents recorded by Police. Finally, other data sources such as the ACCHS, Kimberley School Psychology Service (Department of Education); Kimberley Mental Health and Drug Service (WA Health) and Ambulance data were not included. This is partly due to the complicated ethical processes required for accessing various datasets, and that the Kimberley ACCHS only commenced clinical coding of self-harm presentations in 2020. Even with these limitations, the findings are compelling.
Chronic levels of distress are being expressed via self-harm across the Kimberley region. The amelioration of self-harm and suicide rates across the region requires sustained investment and innovation. This includes the resourcing of Aboriginal community controlled responses to the inequities in the social determinants of health and reform of current services to align to regional need.
Footnotes
Acknowledgements
We thank Kristen Orazi for her thoughtful review of this work.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.