
Abstract
Keywords
In Australia there are limited descriptive data regarding the patterns of referral for psychiatric consultation in the general hospital. Furthermore, there is no information about referrals of people from particular cultural groups to consultation–liaison (C-L) psychiatry services. Mental disorders are the second leading cause of disease burden in Aboriginal and Torres Strait Islander peoples [1]. Furthermore, Indigenous Australians are overrepresented in hospital for mental and behavioural disorders, particularly including psychoactive substance use [2]. Physical and mental health comorbidity is common [3]. Determining the nature of specific mental disorders and their prevalence in Indigenous Australians is problematic due to considerable methodological difficulties including identification, categorization, attribution and interpretation [4].
The widespread experience of adversity and social disadvantage in many Indigenous peoples, including Australians, is well recognized [5, 6]. This is particularly important to understand in clinical psychiatry given the close association between social circumstances, interpersonal difficulties, and adverse life events, with mental and general health problems [5, 7, 8]
Concepts of mental health
Indigenous people have expressed concern that their worldview or cultural beliefs about mental health are not taken into account in Western models of mental health service delivery [9]. Aboriginal peoples endorse the broader concept of social and emotional well-being rather than mental illness [10]. Indigenous perceptions of mental health incorporate the mind, body, spirituality, environment (including relationships with family, land and culture) and sociopolitical factors. When one or more of these elements is compromised the person may be predisposed to physical or mental problems [11]. Ypinazar et al. highlighted the importance of considering the differing and evolving worldviews of cultural groups because they impact upon their concepts of mental health, illness and well-being [12]. Not surprisingly, there is ongoing debate about whether mainstream psychiatric diagnostic criteria are relevant to Indigenous peoples [13].
As in many cultures, family is integral to the mental health of Indigenous Australians [14]. Pratt highlighted the importance of understanding the significance of an Indigenous person's social, emotional, physical, cultural and spiritual life with reference to their sense of belonging to a family, community and culture [15]. Family and friends, with their unique knowledge of individual patients longitudinally and of potentially relevant cultural beliefs and events, may also provide valuable corroborative history that helps clarify diagnostic dilemmas [16]. Phillips found that families wanted to be involved and were concerned about the lack of communication between them and community mental health and emergency departments (EDs) [17].
Communication
Aspects of best practice in the mental health care of Indigenous Australians have been described [9, 16, 18, 19]. Arguably the most fundamental component of quality to be assessed in any health service is communication. Westerman noted that engaging Indigenous people in mental health assessments is a function of both the cultural appropriateness of the clinician's approach to engaging the patient and qualities specific to the clinician [16]. She outlined some useful approaches to engage Indigenous people and recommended obtaining a corroborative history about how the person is viewed by and functions within their usual cultural context and the mainstream environment. Hunter refers to the concept of informed listening, that is, the clinician demonstrating an understanding about salient background matters that facilitate placing the patient's story in a context [18].
Communication problems are often identified as the main barrier to delivering effective, quality psychiatric care for Indigenous Australians. The liaison component of C-L psychiatry encompasses the referring team, family, community mental health teams, general practitioners and other health-care providers. This function is essential given holistic Indigenous beliefs regarding social and emotional well-being, and the importance of family in particular. This was reflected in a file audit of Indigenous psychiatric inpatients, in which carers were consulted 69% of the time [20].
Aboriginal mental health workers
Communication may be enhanced by Aboriginal mental health workers (AMHWs), who make valuable contributions to the delivery of culturally appropriate mental health care for Indigenous Australians [21]. The Royal Australian and New Zealand College of Psychiatrists Position Statement, Aboriginal and Torres Strait Islander Mental Health Workers, emphasized the recognition of and support for AMHWs [22]. Formalized education and clinical programmes have been developed for AMHWs to promote stronger links with Indigenous communities and mental health services, deliver culturally appropriate services in partnership, and in an effort to standardize the profession and ensure its proper recognition [23, 24]. Patients have also indicated that they want mental health services to have AMHWs [25].
McAndrew and Frost presented their experience of working with AMHWs in a C-L setting in the Northern Territory [McAndrew V, Frost M: unpublished data, 2003]. They highlighted the complementary role that AMHWs performed, including assisting with interpreting phenomenology, establishing rapport, delivering a more holistic service particularly through practical assistance, providing cultural advice and education to non-Indigenous clinicians, mobilizing appropriate family and community services, and facilitating follow up with local Aboriginal health services. They advocated that C-L psychiatry continue to work with AMHWs in order to provide better quality treatment for Indigenous patients.
Evaluations of psychiatric services
A needs analysis was undertaken by Eley et al. to determine the quality and effectiveness of mental health services to Indigenous patients within an area of Southern Queensland [26]. Most patients did not feel well informed about their treatment, understand the information given to them, or feel involved in clinical decision-making. The responses of family members and friends similarly highlighted poor communication. The same group identified further problems with communication, including a lack of understanding of Western concepts of mental illness [25]. Reasons given by respondents for avoiding psychiatric admission or contact with mental health services were ‘fear of being locked up’, shame, and perceptions that services were not Murri friendly, had few Indigenous staff, and that communication difficulties were likely to arise [25].
Present study
The mental health issues of Indigenous Australians, including comorbidity, must therefore be considered in the context of Indigenous concepts of health, with proper recognition of the role of the family and social circumstances. Problems with communication that impede access to mental health care are known, as are approaches to address them (such as partnerships with Aboriginal health workers, AHWs). In light of these aspects of best practice this report describes the referral patterns, liaison process, management and follow up of Aboriginal and Torres Strait Islander peoples referred to the C-L psychiatry service of an inner-city teaching hospital and seeks to evaluate aspects of quality.
It was hypothesized that some general hospital and ED referrals of Aboriginal and Torres Strait Islander peoples to the C-L psychiatry service reflect cultural misunderstanding or stereotypes rather than actual mental illness. The authors also sought to evaluate whether the management strategies suggested by the C-L psychiatry service take culture into account, which is fundamental to providing a culturally appropriate service.
The term ‘Indigenous Australians’ will be used to refer collectively to Aboriginal and Torres Strait Islander peoples.
Method
This study was a retrospective hospital medical record audit of all Indigenous Australians referred to a C-L psychiatry service in Sydney, Australia, during the period 1 July 2004–30 June 2007. The C-L psychiatry service consisted of several psychiatrists, between 3.5 and 4 full-time equivalent psychiatry registrars (one of whom was a rotating ED registrar), a psychologist and nurses. The C-L service provided consultation to general hospital teams including the ED. In addition, some teams have a specific psychiatry liaison attachment, for example, obstetrics and oncology. Patients may also be seen in outpatient clinics, but they were not included in the present study due to incomplete records.
Referrals were taken during working hours on weekdays. They were received by direct verbal communication from the referring team to either the C-L psychiatry consultant or trainee and were usually recorded on a consultation sheet. Assessments by the non-medical members of the C-L team were not examined.
The Medical Records Department provided the total number of Indigenous and non-Indigenous Australians admitted to the general hospital and the ED in the study period. These two figures were compared with the numbers of Indigenous and non-Indigenous Australians referred to the C-L psychiatry service in order to estimate referral rates.
Referral patterns, diagnosis, components of liaison, suggested management, legal interventions, disposition and follow up were evaluated. The C-L psychiatry notes were examined for references to the patient's Aboriginality, including consideration of cultural beliefs and health concepts. Data were analysed using the SPSS version 15 (SPSS, Chicago, IL, USA). Frequencies and percentages were reported for simple descriptive variables. Significance was tested at p < 0.05. Cramer's V was used to examine associations between categorical variables. A thematic analysis of a subset of these files was undertaken to examine more closely whether and how culture was taken into account in the assessment and management plan [27].
The results were discussed with AHWs to validate the interpretation of the data. Ethics Committee approval was obtained from the Aboriginal Health and Medical Research Council of New South Wales (NSW), the NSW Institute of Psychiatry and the Area Health Service.
Results
Overview of referral rates and demographic data
There were 3154 referrals to the C-L psychiatry service during the study period; of these, 162 referrals involved Indigenous Australians. This represented 99 individuals: 88 Aboriginal, three Torres Strait Islander and eight Aboriginal and Torres Strait Islander people. Referral rates were 3% for Indigenous Australians and 1.7% for non-Indigenous people. The local Aboriginal population was 2% at the 2006 census [28]. The majority of referrals of Indigenous Australians were male (54.9%), living in an urban setting (82.1%), and single (61.7%). The mean age was 37.5 years, with a range from 18 to 74 years (SD = 10.28).
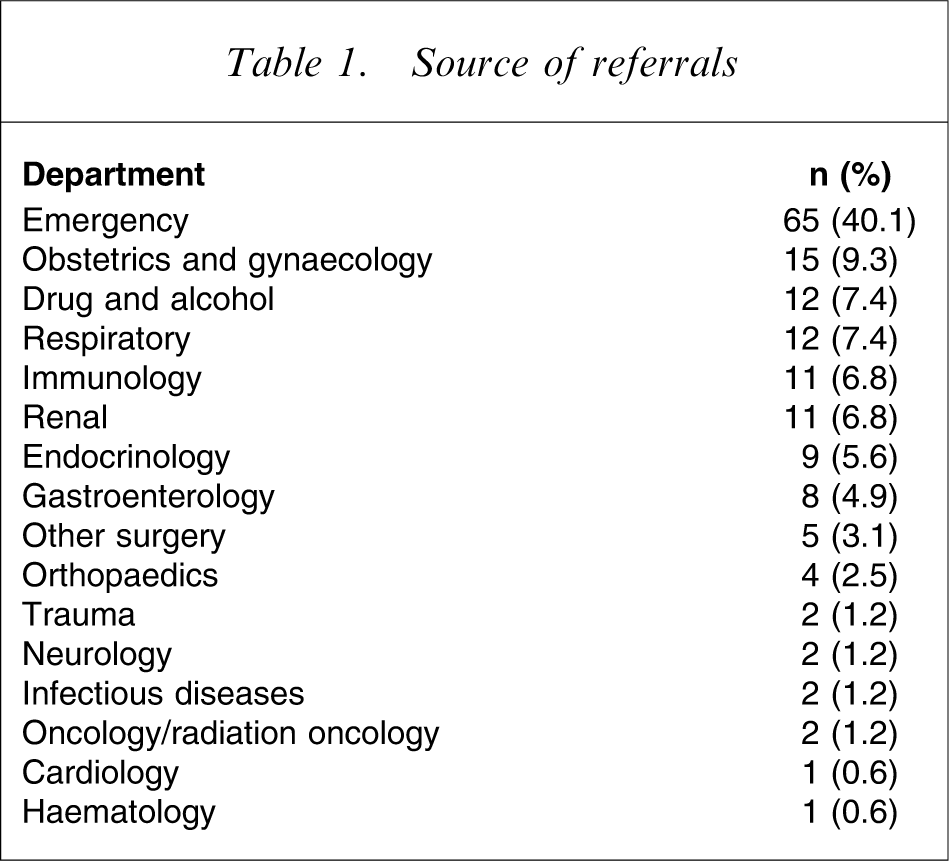
The ED contributed the highest rate of referrals (40.1%), followed by Obstetrics and Gynaecology (9.3%), and individual medical teams (Table 1).
Source of referrals
Reasons for referral
The reasons for referral to the C-L psychiatry service are listed in Table 2. Risk assessment, depression and behavioural problems were the most frequent. Behavioural problems included agitation and aggression (42%), deliberate self-harm (25%), wanting to leave and non-adherence to medical treatment (approx. 16% each) and unusual behaviour or confusion (12.5%).
Reason for referral
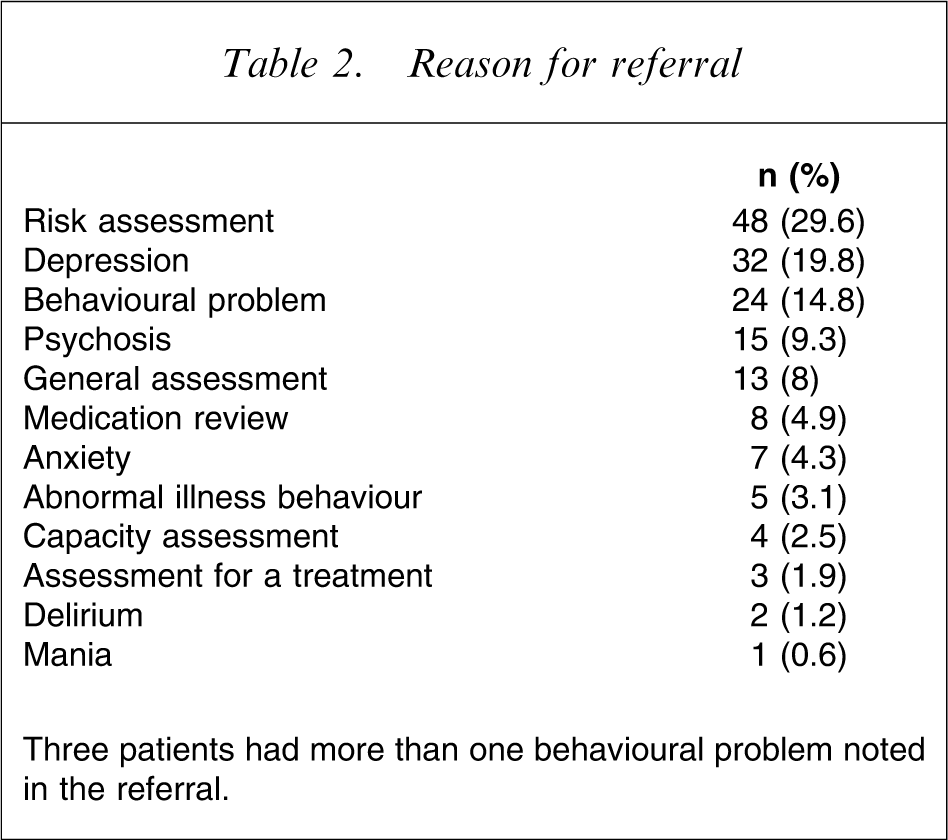
Three patients had more than one behavioural problem noted in the referral.
The C-L psychiatry service identified the primary mental health issue underlying the referral (Table 3). Twenty-four per cent had more than one psychiatric diagnosis. There was a significant relationship between the reason for referral and the subsequent interpretation of the underlying problem by the C-L psychiatry clinician (Cramer's V = 0.48, p < 0.01). The diagnostic category “no mental illness” encompassed patients thought to be malingering; with a past history of mental illness but no current diagnosis; capacity assessments; and assessments of suitability for procedures (such as transplants). No patients were identified as having a culturally based presentation.
Underlying mental health problem identified by C-L
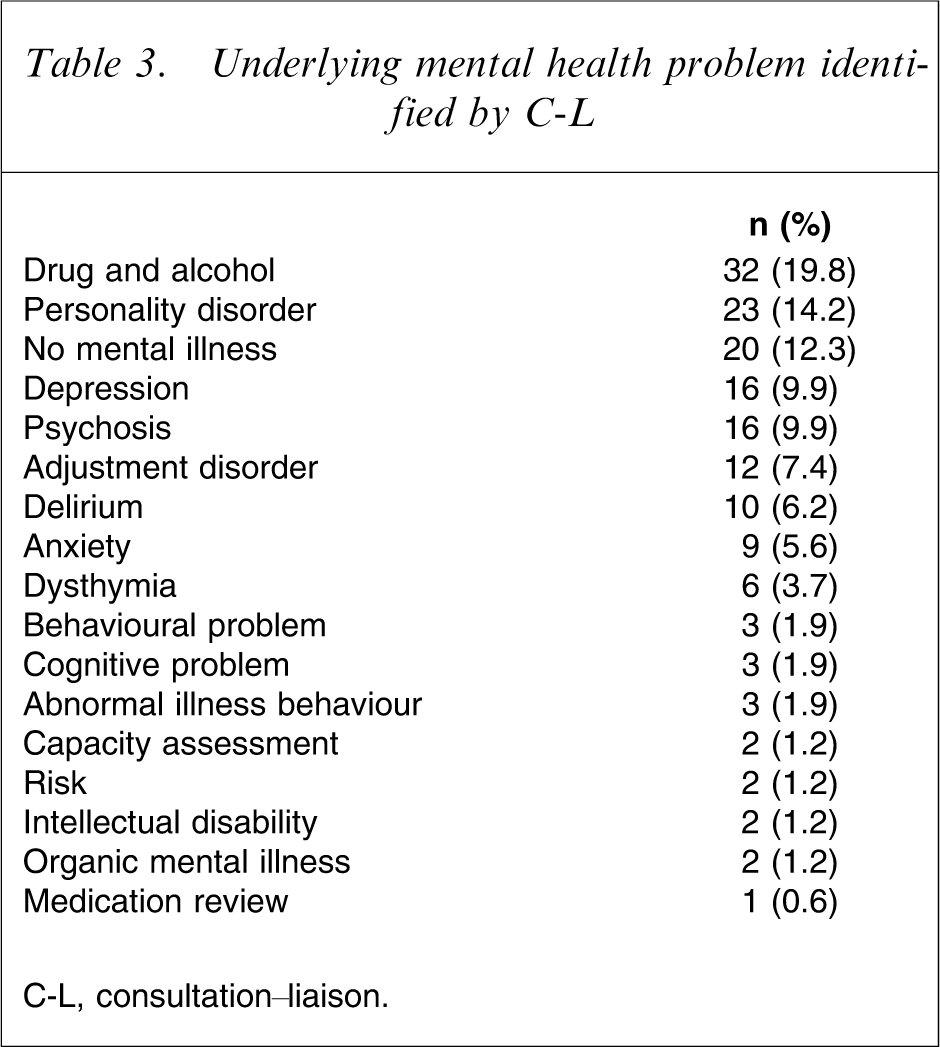
C-L, consultation–liaison.
Evidence of a liaison process
Recorded contact with general practitioners (15.4%), mental health services (66.4% of people with previous contact with mental health clinicians), other external services (17.9%), and family/friends (34.6%) during admission were noted. Table 4 lists the contact with AHWs during the C-L assessment process. Patients referred from the wards were more likely to see an AHW than those referred from the ED. Patients for whom there was no documented C-L liaison with one or more AHWs or general mental health clinician were more likely to be discharged against medical advice (Cramer's V = 0.169, p = 0.031). There was no association, however, between involvement of an AHW alone and discharge against medical advice.
Liaison with Aboriginal health workers
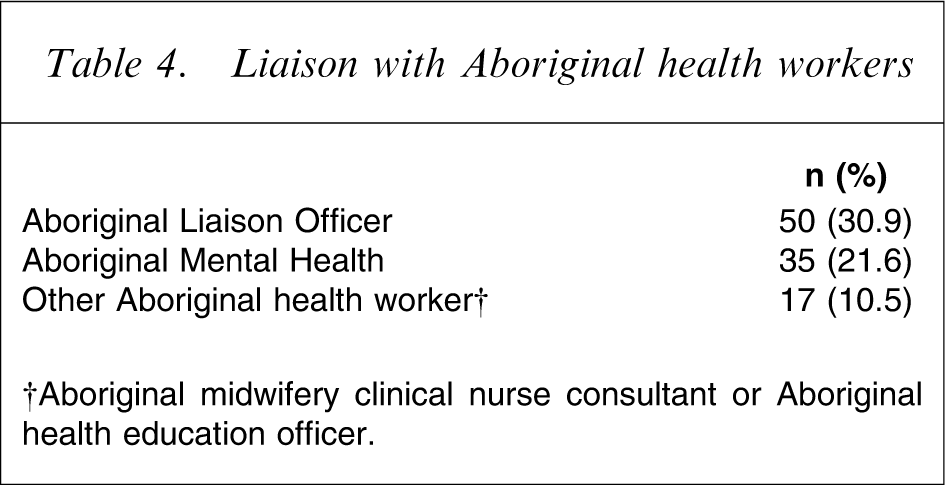
†Aboriginal midwifery clinical nurse consultant or Aboriginal health education officer.
Suggested C-L psychiatry service management
The interventions recommended by the C-L psychiatry team are listed in Table 5. Suggestions about psychotropic medications were most common. Staff intervention included providing information about the patient's assessment, advising staff how best to interact with the patient, and behaviour management plans. Environmental manipulation included advice to change the patient's location on ward or their bedside environment and recommendations for the patient to have periods of leave. Psychotherapy was found to be an uncommon intervention, despite being broadly defined to include psychoeducation and referral for or the provision of psychotherapy.
Analysis of C-L psychiatry interventions
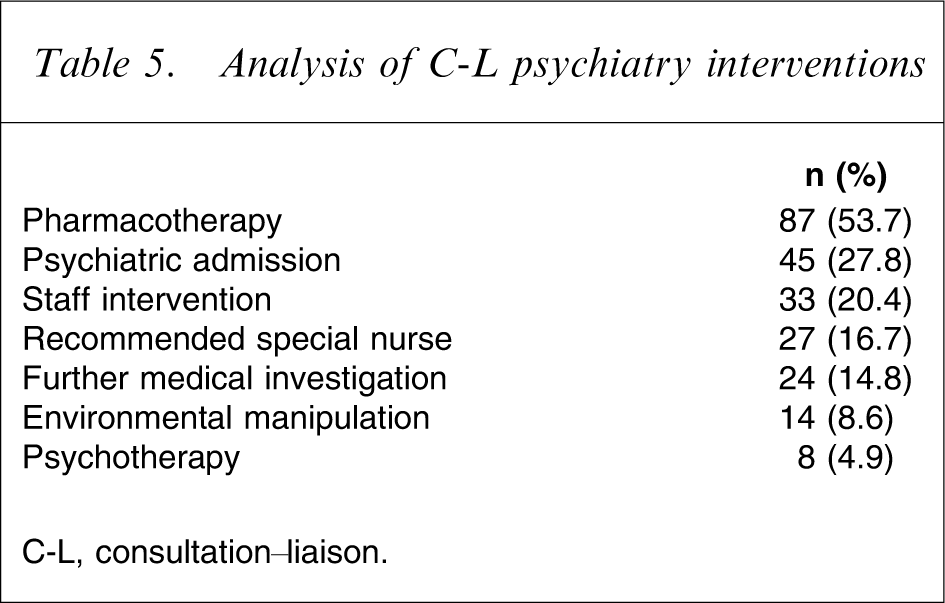
C-L, consultation–liaison.
Recommendations by C-L psychiatry pertaining to the patient's legal status were examined. There were no legal interventions in the majority of consultations (75.3%). In the remainder, rates were as follows: patient certified under the Mental Health Act 1990 (11.1%), guardianship application recommended (4.9%), explicit mention of using duty of care (3.7%), cancellation of certification under the Mental Health Act 1990 (3.1%), and notification to child protection services (3.1%). A small number of patients had more than one legal intervention.
Outcomes and follow up
Following their general hospital admission or ED presentation 56.2% of referred patients were discharged home. The remainder were admitted to a psychiatric unit (27.8%), discharged against medical advice (7.4%) or transferred to another hospital (4.9%). Two patients were discharged to a drug and alcohol facility and one was admitted to a nursing home. Three patients died from medical causes during their admission.
All patients were referred for follow up (some patients were referred to more than one service). Of the patients discharged home, 31.5% were referred to Aboriginal or general mental health services, medical outpatient clinics (37.3%), other services (including charities, community groups, and nurses, 31.4%), general practitioners (27.5%) and drug and alcohol services (9.8%).
Discussion
To the best of our knowledge this is the first study to look specifically at referral patterns, C-L psychiatry assessments and management plans provided to Indigenous Australians. Because there is no culture-specific C-L literature with which to compare our findings we have referred to papers describing the best practice of mental health service delivery for Indigenous Australians.
Patterns of psychiatric consultation
The rate of referrals was higher in Indigenous Australians than non-Indigenous people. This is not unexpected given the higher burden of physical and mental illness in Indigenous peoples [1]. Indigenous status, however, is generally underrecognized and underreported. The present study also found inconsistency in the recording of Indigenous status even within the same patient's file. It may therefore be assumed that the true rate of mental health problems in Indigenous Australians admitted to general hospitals is even higher.
The ED was responsible for the greatest number of referrals to the C-L psychiatry team. This is not surprising in a health service where C-L services are embedded within the ED, with an on-site mental health nurse practitioner and daily C-L ward rounds commencing in the ED. The ED is often the first point of call for families in crisis, particularly after hours. Indigenous families may delay Western treatment until crisis point due to fear of hospitalization, as a result of previous familial or community experiences of contact with mental health services [9].
Reasons for psychiatric referral
Risk assessment was the most common reason for referral, accounting for just under one-third of referrals, followed by depression. This is consistent with statistics showing that suicide and self-harm rates are comparatively higher in Indigenous Australians than the general population [23]. Referrals under the heading of behavioural problems (e.g. wanting to leave) may have related to miscommunication and the lack of culturally appropriate hospital management rather than an underlying mental illness.
The most common mental health problems underlying referrals in the present study were identified by C-L as drug and alcohol related, personality disorder, and no mental illness. The present findings may reflect the inner-city location of the study, where rates of drug and alcohol problems are relatively higher than other metropolitan areas. An even higher prevalence of drug and alcohol problems (79%) was reported in a review of hospital separation data in South Australia [3]. That review similarly found significant comorbidity, with most people having multiple and complex mental and physical problems [3]. Studies of all people referred to a comparable C-L setting in Melbourne found depression to be more common than emerged in this study [29]. Depression is also known to be prevalent in Indigenous Australians in the community [8, 30], so it was surprising to find that depression was diagnosed less often than personality disorder. Depression may have been misdiagnosed as personality disorder, an uncertain diagnosis in this population given the high rates of psychosocial adversity, multiple comorbidity, and communication issues (particularly pertaining to cultural expressions of illness). There was rarely sufficient detail recorded to verify this diagnosis.
Contrary to our predictions, there were no cases in which symptoms commensurate with cultural experiences were identified. Although they may have been missed, such presentations may be uncommon in Indigenous Australians living in urban areas, who may be influenced by Western concepts and may consequently harbour hybrid theories of cultural beliefs and understandings about mental illness [12]. Perhaps the referral label of ‘behavioural problem’ when patients wanted to leave hospital or did not adhere to treatment reflected the staff's lack of appreciation of the impact of culture on the patient's experience of illness.
C-L psychiatry intervention
In two-thirds of the C-L assessments there was documented contact with external mental health services who had previously seen the patient. This is in contrast to low rates of contact with the patient's general practitioner or family. The rate of consultation with carers was also low in comparison to that found in the inpatient study by Nagel and Thompson [20]. But better communication with carers would be expected in an inpatient psychiatric setting, where the staff have training in mental health compared to the general hospital or ED, where the psychiatric input is by definition delivered via consultation. Nonetheless, the results are disappointing given the importance of these sources of corroborative history, cultural information, and ongoing support for the patient.
Because C-L operates at the interface between medicine and traditional psychiatry, facilitating psychiatric admissions is a key role. The high rate of disposition to inpatient psychiatry units in the present study, however, is notable. The present high rate may be due to the significant proportion of patients receiving a diagnosis of drug or alcohol problem, or presenting ongoing risk concerns (active suicidal or self-harm ideation). Pharmacotherapy was the most commonly used therapeutic tool. Although psychosocial issues were reasonably well identified by C-L [27], they were infrequently addressed in management plans.
The Western focus upon medication and hospitalization is at odds with Aboriginal traditional treatments, which include methods to build resilience against spirits to increase wellness [12]. Perhaps, issues relating to communication may partly explain the utilization of more biomedical rather than psychosocial interventions. Greater participation of AHWs and family in making collaborative C-L management decisions may have resulted in treatment approaches that were more acceptable to patients and which better met their health-care needs in a holistic way. C-L services, however, generally operate within a biomedical paradigm, and the time-pressured ED environment, for example, may not be conducive to holistic care.
Rates of involuntary hospitalization reported for the general population are low, <1–3.6% [29, 31], compared to the present study (11.1%). This in part confirms the fear of ‘incarceration’ expressed by Indigenous patients in the Queensland study [25]. It would be important to compare these data with the use of the Mental Health Act in non-Indigenous people referred, before drawing any conclusions. The recognition, however, of disproportionately high rates of suicide and self-harm in Indigenous Australians may have contributed to the use of more cautious management strategies by the C-L psychiatry service.
Outcomes
The rate of discharge against medical advice found in the present study, was 7.4%. It would be useful to know whether a similar proportion of non-Indigenous referred patients had this outcome. It is likely that the reasons for this mode of discharge are complex and relate to staff–patient communication, diagnosis, the nature of the underlying medical problem and treatment, availability of support and the personal circumstances of the patient. Having consulted an AHW alone did not protect against discharge against medical advice, but patients for whom there was no liaison with either an AHW or general mental health clinician were more likely to be discharged against medical advice. Due to small numbers this must be interpreted cautiously. It may reinforce the importance, however, of the psychiatry liaison role in this setting.
References to culture
Aboriginality was acknowledged in some form in the C-L assessment in just over half of the consultations. AHWs (mostly not AMHWs) were involved with 48.1% of referred patients identifying as Indigenous Australians. This occurred more often for ward patients, which is not surprising because they are generally admitted longer than ED patients. Additionally, some wards such as obstetrics have their own AHWs. Referral is at the discretion of the clinician because there is no policy outlining who should be referred under which circumstances. An audit of the inpatient psychiatric unit of Royal Darwin Hospital in 2001 found that AMHWs were involved in the care of 64% of Indigenous patients during their hospital stay [20]. Similar rates of consulting a Maori mental health nurse and/or cultural advisor were reported in a file audit of inpatient psychiatric units in New Zealand [33]. This discrepancy is not surprising because AMHWs would be expected to have a closer relationship with inpatient psychiatric services than the general hospital, and psychiatric inpatient staff should also be more familiar with working with AMHWs. In Australia there is a paucity of AMHWs, which would place practical limits on the settings (and the frequency) in which they could attend.
Interestingly, an AHW may have been involved but did not personally document their interaction. The AHW's involvement was noted in a number of files by another clinician and has implications for improving communication. Upon presentation with these data, AHWs explained that they primarily communicate verbally with hospital staff; do not record interventions they may have with patients’ family members; often see their input as not relevant to the medical record (e.g. social interventions); and are reluctant to document culturally sensitive or private issues that may be misinterpreted. There is no policy guiding documentation. Similar findings were reported by Harris and Robinson, who found few references to the involvement of AMHWs in patient files despite high levels of informal engagement between AMHWs and clinicians in patient care [24]. They concluded that there was a need for more formalized support for AMHWs, for clearer definitions and development of their clinical role, and recognition of their independent contributions to mental health care.
Limitations
There are a number of inherent difficulties in studies of medical records. The identification of Indigenous people in hospital records is variable and incomplete, ranging from 55% to 100% accuracy [32]. Attempts were made to improve this by cross-referencing the medical record's classification of Aboriginality with textual references to culture. Because the present study relied solely upon recorded data it is possible that we have underestimated the number of cases in which an AHW was involved. It is also possible that the C-L clinician recognized the patient's cultural background but did not record it. This may be particularly true for patients who presented on multiple occasions, receiving multiple C-L assessments, during the study period.
Time constraints prevented the important comparison with referrals of non-Indigenous people. Such data would illuminate whether there were differences in the assessment and management of the two groups in this particular C-L service, with obvious implications for quality improvement.
Recommendations
The present study demonstrated high rates of referrals of Indigenous Australians to C-L psychiatry, which reinforces the need for C-L services to become more culturally safe. Referrals for risk assessment, depression and drug and alcohol problems were most prevalent. This knowledge should alert the C-L team to routinely consider these issues in assessments of Indigenous Australians. The focus on biomedical interventions identified may be at odds with holistic Indigenous concepts of health and therefore be less acceptable to patients, acting as a barrier to engaging with psychiatric services. These data also highlight the importance of maintaining close relationships with other health services, such as drug health. The recent appointment of an AHW in drug health at the study hospital should facilitate this liaison and result in this common comorbidity being addressed simultaneously with medical and psychiatric illness.
Fundamental to best practice in psychiatry is clear two-way communication with patients, family, external health-care providers and other mental health services. The present study has highlighted that communication problems are still an issue in the delivery of culturally appropriate mental health services to Indigenous Australians in the general hospital. Given that Aboriginal concepts of health and well-being are holistic, communicating with all services, family and carers involved with the patient is the only way to address comorbidity, coordinate care, and to ensure that complex needs are met. Although there is increasing recognition of the valuable role performed by AHWs, particularly as cultural brokers, they are not regularly involved in C-L psychiatry assessments. AHWs should be more routinely engaged for cultural expertise, involvement with assessment, and addressing psychosocial issues. Hospital guidelines for referrals to AHWs that clearly define roles, responsibilities and support structures should be developed.
Asking patients about their culture and how it relates to their experience of illness and treatment is a straightforward way to strengthen the therapeutic alliance, and enhance understanding of the patient and their predicament [33]. Developing more culturally appropriate and accessible C-L psychiatry services will require direct examination of patients’ experiences of their general hospital psychiatric assessments: that is, canvassing their needs and levels of satisfaction with the service. Nonetheless, lessons learned here for improving communication with Indigenous Australians are applicable to psychiatric services in general.
Footnotes
Acknowledgements
Anne Wand was supported by a NSW Institute of Psychiatry Research Fellowship. The authors would like to thank Mr Gavin Lackey, Quality Improvement Unit, Royal Prince Alfred Hospital, for his assistance with statistical analysis.