
Abstract
This study investigates the confluence between accounting and natural disasters by examining the case of the cholera epidemic that occurred in Bologna in 1855, a city of the Papal States, where there was a strong (medical) intellectual class critical of the central government exercised by the Pope and clergy. We analysed primary and secondary sources available in Bologna in the Municipal Library of the Archiginnasio, State Archive, and Municipal Historical Archive to demonstrate how the accounting for and of the epidemic overturned the traditional power structures of the Papal States. Specifically, the medical establishment, leveraging the medical-administrative accounting technologies, replaced the clergy and local aristocracy as the governing body of the city, paving the way for the future secularisation of the administration. The study contributes to the literature by providing political implications of accounting technologies for natural disasters.
Keywords
Introduction
The existence of natural disasters has been a constant phenomenon throughout the history of humanity, with considerable consequences at the national and international levels. Some of these consequences have an eminent political nature as they can subvert the pre-existing balance of powers. Ayalon (2017) asserts that managing such disasters was crucial to both the rise and fall of the Ottoman Empire. Similarly, Walker (2014: 2) argues that responses that are considered inadequate ‘may diminish the authority of those holding office at national, state and/or local levels’ and can reveal ‘latent socio-economic fissures which animate demands for fundamental political change’.
Sargiacomo et al. (2021) state that investigations on natural disasters in the field of accounting history are still underdeveloped and the existing studies use recurrent investigational loci, mainly focus on twentieth-century cases, and mostly address post-earthquake outcomes; drought and pandemics are the exceptions to slow-moving disasters that unfold over long periods of time. Prior studies focus on calculative practices to understand the governance of the exceptional event that guides the emergency responses (Manetti et al., 2017; Sargiacomo, 2015; Shimizu and Fujimura, 2011) and post-disaster recovery (Carungu and Paolicelli, 2018; Cho, 2009; Miley and Read, 2013; Sargiacomo et al., 2014; Vosslamber, 2015; Walker, 2014). Research on the relationship between the use of calculative practices and political consequences is limited in the accounting history literature. This study aims to fill this gap by highlighting the possible political consequences of the intersection between accounting and epidemics.
During an epidemic, the government needs to mitigate the risks of infection by implementing several coping strategies that may cause social, political and economic consequences over time. As these strategies are informed by expert medical knowledge, it raises the issue of the medicalisation of power raised in Foucault's studies (1975, 1990, 2004). Thus, capitalising on the ‘political’ benefits of medical knowledge, this study explores the case of the cholera epidemic that occurred in 1855 in Bologna, a city of the Papal States. We investigated this case study because the political scenario of the city was characterised by the critical position of the local (medical) intellectual class towards the central governance exercised by the Pope and clergy. Specifically, we reviewed how the accounting for and of the epidemic adopted by the local medical establishment allowed them to take the city government over from the clergy and local aristocracy allied with the Pope. This replacement of roles during the emergency represented an important testing ground for what would later be the secularisation of city government.
The study contributes to the literature on accounting and natural disasters in several ways. First, it demonstrates how accounting can not only be a tool to confront an emergency but also a leverage to use an emergency to propose an alternative government model to the pre-existing one. Second, it adds to the strand of research about accounting and the interplay between local and central government (Gomes and Sargiacomo, 2013). Sargiacomo et al. (2021) highlight that this existing gap is important considering that different governmental bodies at central and local levels must work concurrently during natural disasters. Third, the study contributes to the emerging research field of accounting for and of death (Moerman and Van Der Laan, 2022), as well as to our knowledge of accounting for the medical profession, because epidemic accounting derives meaning from the broader political context in which it occurs in addition to the scientific aspect of the disease and death.
The remainder of the study is organised as follows. In the following sections, we describe our theoretical framework and the research method adopted; then, we provide an overview of the conflicting political rationales inspiring the political authorities and medical establishment of the city during the epidemic. Subsequently, we present the outbreak of the epidemic and the consequent emergency plan both in its managerial and accounting aspects. Finally, we describe how the medical establishment took control of the city. The last section analyses how the accounting technologies adopted by the medical establishment brought the secular class to the government of the city and draws the conclusions of the study.
Theoretical framework
The Foucauldian theoretical framework addresses ‘how-type’ research questions about the way power is exercised (Foucault, 1982: 786; Foucault, 1991; Miller and Rose, 1990). Moreover, it examines the role of modern medicine in technologies of power. Consequently, the study adopts the Foucauldian perspective, according to which medicine ‘is not a pure science, but part of an economic system and of a system of power’ (Foucault, 2004: 19). The scientific aspect of medical knowledge enables the realisation of power dynamics, facilitating the expansion of medical practices to other domains, known as medicalisation because ‘today medicine is endowed with an authoritarian power with normalising functions that go beyond the existence of diseases and the wishes of the patient’ (Foucault, 2004: 13). Referring to the problematisation in political terms regarding the health of a population, Foucault describes the general ‘police’ of health where the health and physical well-being of the population, in general, is one of the essential objectives of political power: Different power apparatuses are called upon to take charge of bodies, not simply so as to exact blood service from them or levy dues, but to help and, if necessary, constrain them to ensure their own good health. The imperative of health: at once the duty of each and the objective of all (Foucault, 1984: 275). …the administration acts as a point of support and sometimes a point of departure for the great medical inquiries into the health of populations, and conversely, doctors devote an increasing amount of their activity to tasks, both general and administrative, assigned to them by power. A medico-administrative knowledge begins to develop concerning society, its health and sickness, its conditions of life, housing, and habits, which serves as the basic core for the social economy and sociology of the nineteenth century. And there is likewise constituted a politico-medical hold on a population (Foucault, 1984: 283).
Four processes lead to the politico-medical control over people (Foucault, 2004: 13): (1) the appearance of medical authorities; (2) the appearance of medical fields of intervention distinct from disease, such as hygiene and environment; (3) the introduction of the hospital as the site of collective medicalisation; and (4) the introduction of mechanisms of medical administration, such as recordkeeping. These processes allow medical mechanisms to execute a disciplinary technology according to the model of the Panopticon, an adaptation of Bentham's concept for the ideal prison, which Foucault considers the model for the efficient operation of disciplinary technology in everyday life.
In its various forms, the panoptic schema serves ‘to treat patients, to instruct schoolchildren, to confine the insane, to supervise workers’ (Foucault, 1995: 205). The medical mechanisms and their processes represent a form of ‘medical gaze’ that is an exercise of continuous surveillance and coercion.
Epidemics allow us to better observe the medical gaze because they are ‘limit cases’ that always justify an exceptional treatment and give rise to forms of ‘authoritarian medicalisation’ (Foucault, 1984: 277) incorporated into ‘emergency plans’ (Elden, 2003: 242). These emergency plans affect ‘disciplinary diagrams’ 1 (Foucault, 1975: 231), requiring ‘a strict spatial partitioning, careful surveillance, detailed inspection, and order’ (Elden, 2003: 243). They represent a ‘military model of organised discipline’ (Evenson et al., 1996: 218) and ‘the birth of administrative and political strategy’ (Foucault et al., 1999: 44), whose four modes are selection, normalisation, hierarchisation and centralisation (Foucault, 2012: 161).
The ‘disciplinary diagram’ of the emergency plan for epidemics first requires a selection criterion to identify those who can optimally perform a function. Then, the bodies are classified according to normative segments, that is, subjecting an individual to behave in a quasi-automatic (and not autonomous) manner. Each docile body occupies a place on a scale of values allowing power to circulate according to its capillary reality, at different, polymorphic levels and of varying intensities, but making everyone traversed by this mesh of power into participants of a relay that renews this power. Finally, the various places are not arbitrarily distributed but arranged around a central operating pole from which hierarchy develops.
Epidemics enhance the ability of medical expertise to constitute power relations because the doctors, as disease experts, problematise the emergency, posing new problems to the political authorities (Radcliffe, 1999) and develop specific programmes of action. This is consistent with Rose and Miller (1992), who identify the programmatic aspect in terms of the suggestions of various experts and specialists having knowledge of the field that requires programme intervention. ‘Disciplinary diagrams’ always need an intellectual machinery that renders elements of the emergency thinkable.
Concerning epidemics, programmes are informed by medical statistics that are mainly in the form of accounting for and of death (Moerman and Van Der Laan, 2022). The calculative practices related to death, in addition to giving measurability and visibility to the emergency, serve as a technology for power because they provide a basis for what constitutes acceptable behaviour, that is, normalisation. According to Foucault (1990: 145–146), statistics gave rise to: infinitesimal surveillances, permanent controls, extremely meticulous orderings of space, indeterminate medical or psychological examinations, to an entire micro-power concerned with the body. But it gave rise as well to comprehensive measures … and interventions aimed at the entire social body or at groups taken as a whole.
Research method
The study examines the relationship between the accounting for and of the epidemic effected by the local medical establishment, and the political fact-building of Bologna. Thus, the first step is to clarify what kind of documents should be included under the ‘accounting’ label. The study adopts the definition of accounting provided by Sargiacomo et al. (2012: 396) as ‘documents of any kind which typically use text and numbers in structured or unstructured ways to provide records of commitments and transactions between named and unnamed parties’. Considering this perspective, the (medical) experts are ‘account fabricators’ (Chua, 1995), that is, producers of records, and our primary sources are the medical statistics reports, bulletins, forms, and registers of health care and assistance adopted to manage epidemics, available in Bologna in the Municipal Library of the Archiginnasio (BCAB), State Archive (ASB), and Municipal Historical Archive (ACB).
Subsequently, as science and accounting are instrumental activities (Chua, 1995), these documents must be related to the rationale of the management of the epidemic and the government of the city. As ‘context is everything’ (Hopwood, 1983; Moerman and van der Laan, 2022), we followed the suggestion ‘to look beyond the boundaries of the laboratory or the laboratory's influence to the larger society to consider the forces that encourage laboratories or provide counterweights to sink them’ (Scott, 1991: 30). This methodological approach involved various primary and secondary sources with potentially different views and perceptions (Tinker et al., 1982) of the epidemic in Bologna in 1855.
Consistent with the historical method depicted by Droysen (1893) and Bernheim (1889), where historical research is embedded in a logic of questions and answers (Assis, 2015), our ‘how-type’ research question (i.e., how the accounting allowed the local medical establishment to take control of the city government), was articulated into sub-research questions. These clarify the main question and break down the research objective into elementary parts for better understanding. Above all, these sub-questions provided specific directions for guiding the exploration of both primary and secondary sources and allowed each source to provide an answer to a specific sub-research question (see Appendix 1) and to combine the best available information about the same phenomena (Sy and Tinker, 2005).
Bologna in the Papal states in 1855
After Rome, Bologna was considered the second most important city of the Papal States, officially the State of the Catholic Church (De Benedictis, 1990; Santoncini, 2002), owing to its size, university and scientific institutes. After the Treaty of Vienna, the Papal States covered most modern Italian regions and were considered a manifestation of the Pope's temporal power, in contrast to his ecclesiastical primacy.
The political authorities and their political rationale
Since the beginning of the nineteenth century, the political rationale of the Papal States included both the ideals of the absolute monarchy and the principles of Christianity. According to the former, the Pope had total power and controlled the territories through a centralised political-administrative system. According to the latter, the Pope, the Head of the Church, promoted the process of clericalisation of the State (Gatti and Poli, 2014; Prodi, 1987).
The Pope governed his lands, including the province of Bologna, through a Legate, a member of the clergy, who held temporal power over the territory and personally responded to the Pope and ruled the provinces in his name (Fantini, 2011). Bologna held a special status that guaranteed its privileges and autonomy to the Papal State's legal systems (Santoncini, 2002; Volpi, 1983), whereby the city was supervised by a local collegial body, the Senate, whose members were secular noblemen who elected a Senator to preside it. The Senate and Legate ruled nominally together: It was said: ‘the Legate can do nothing without the Senate, the Senate cannot without the Legate’. However, the Legate was solely responsible for the administration of justice and maintaining public order. He supervised all the main resolutions of the municipal bodies: the appointment of municipal officials, organisation of local taxation, interventions on welfare institutions, city corporations, universities, and initiatives concerning public works (Santoncini, 2002).
In 1852, to restore order after the 1848 uprisings, the Pope sought to promote a strict conservative policy with substantial authoritarian aspects (Hearder, 1975), and appointed Monsignor Grassellini as the Legate of Bologna. The Bolognese population disapproved of the appointment; however, the support of the Austrian occupation troops and connection with the repressive forces of other Papal territories enabled him to suppress – initially with rigorous police measures – the residual insurrection outbreaks (Bottrigari, 1960). Then, he secured loyal allies for the city government by garnering support from the local aristocracy (Monsagrati, 2002). Therefore, in early 1855, the Marquis Luigi Davia was directly invited by the Pope to hold the office of Senator because of the ‘many tests of respect and devotion’ the Marquis had reserved for the Papal government and Pope (Gibelli, 1869: 27). Despite the involvement of the local representatives in the municipal bodies, citizens lacked substantial power on the city's government. It was exclusively clerical because ‘the only way to take part in the political life was that of an ecclesiastical career’ (Cavazza, 2005: 313). Furthermore, clericalisation of the State included public instruction that, with the Pope's decree of 1824, known as Quod Divina Sapientia, must be under ecclesiastical supervision.
The experts and their political rationale: the medical-surgical society
Bologna and its University boasted a centuries-old tradition in medical studies. Its Medical-Surgical Society, one of the oldest in the world, founded in 1802 and then formally recognised in 1805 by the Napoleonic government, enjoyed great scientific respect within the international scientific community (D’Antuono and Bernabeo, 1988).
Since 1848, the Italian scientific community supported the unification of the country because political fragmentation was considered the greatest obstacle to the growth of Italian science and, simultaneously, advanced the claim of reorganising society through a secular vision of life (Pancaldi, 1983). The Medical-Surgical Society of Bologna was established to promote the ‘unity of science’, the ‘political unity of the fatherland’ (Sighinolfi, 1924: 43), and the primacy of reason and science ‘against superstition and dogma’ as a lever to secularise the administration of the city (Sighinolfi, 1924: 5). The medical-surgincal society: wanted to represent an independent and free institution that intended to protect the people, for a high sense of patriotism, humanity, and civilisation, while the restored governments did not recognise the importance of this duty and neglected it in the name of their dominion. The sciences, and mainly medicine, have been always architects of the freedom and greatness of civilised peoples (Sighinolfi, 1924: 32).
In the perspective of ‘political medicine’ (Predieri, 1855: 3), in addition to promoting the advancement of medical-scientific knowledge, the exponents of the Society used to discuss social, economic and political issues in public (Sighinolfi, 1924). In 1848, Dr Rossi published an economic and social analysis, charging the origins of widespread pauperism to the Pope's bad governance and suggesting countermeasures. Dr Paolo Predieri, who was the treasurer of the Society, suggested measures of agricultural policy (Predieri, 1855).
The central government tried to block the activity of the Society owing to its propaganda against the Pope's bad governance and most of its exponents’ (as well as students who attended the University of Bologna) affiliation to the many sectarian clubs of the city that campaigned for national unity (Sighinolfi, 1924).
Over the years, some of its chairmen were arrested or forced to leave the university professorship on conspiracy charges (Majocchi, 1924: 9). The first chairman was accused of heresy for providing rational explanations for a miracle performed by the Church. In 1824, all university professors took an oath on their knees before the Cardinal, and on Sundays professors and students had to attend the religious service to recite the prayers and hear the sermon (Sighinolfi, 1924). In 1831, the Pope suspended the activity of the Society and that of the University for four years for participating in some anti-government riots. The former chair, Dr Alessandrini, who in 1848 had presided over the provisional government formed by the rioters, was persecuted during the Restauration (Il Conservatore, I, I, 1865).
In the Society's political rationale, these acts of repression were used as arguments to portray the doctor as a ‘peaceful conspirator’ for the welfare of the people against the Pope's bad government: While the most arduous problems of civil life are urgent from all sides and threaten society, the Government is very little and feebly interested not only in solving them, but only in warning them, busy as it is to protect the vaunted rights of sovereignty and of empire against the subjects. It disguises the recognition of his duties and his own interest and, instead of assisting and helping the subjects to alleviate the multiple evils, from which there are multiple damages they are oppressed and disheartened and against which they fight for legitimate and natural defense, it contributes to alienate souls from trust and obedience, which it claims to impose with violence (Sighinolfi, 1924: 88).
Cholera in Bologna in 1855
In 1855, the entire Italian peninsula was hit by a cholera epidemic leading to 120,000 casualties (Bianchini, 2010; Nitto, 1962). It broke out mostly in Bologna, causing 4,000 deaths in a few months (Corradi, 1973). The first cases in the city appeared in the register of a hospital, the Lazzaretto of S. Lodovico, on 29 May 1855 (Figure 1).
The first cases of cholera in Bologna. Source: ACB, Carteggio amministrativo (CA), Register of individuals affected by Cholera Morbus in Bologna who entered and left the Lazzaretto in the former convent of San Lodovico from 29 May 1855 to 19 July 1855.
An emergency plan with two ‘disciplinary diagrams’
Cholera was a mysterious disease with no available information, and all treatments seemed ineffective (Tognotti, 2000). To control the epidemic, the Papal States executed two parallel ‘disciplinary diagrams’ as depicted in Figure 2. The first one comprised the traditional institutions inherited from the epidemics that occurred in the previous decade. The second one relied on the new elite of doctors who professed the freedom of science (Figure 2).
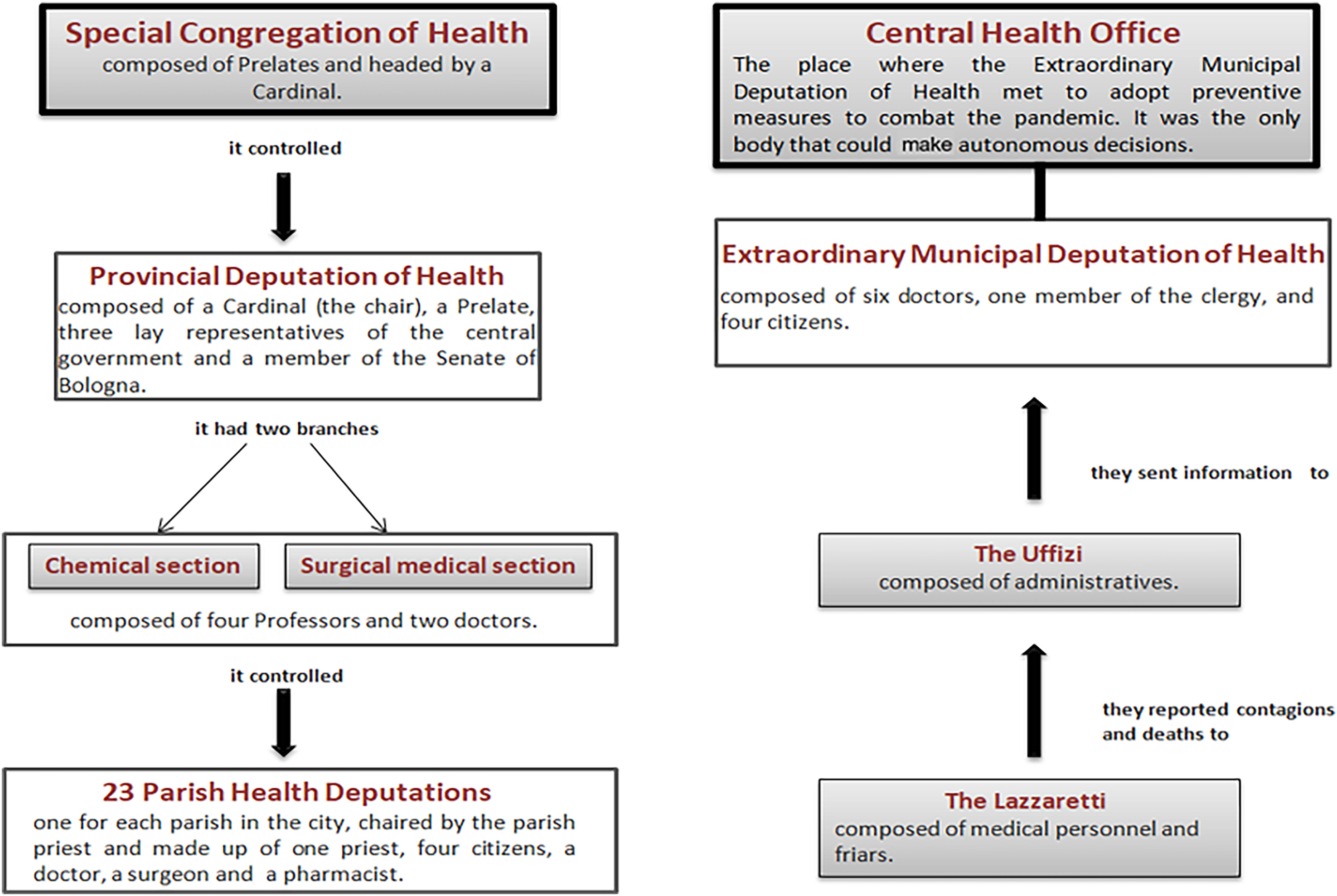
The ‘disciplinary diagrams’ of the emergency plan for cholera in Bologna in 1855.
The first diagram depicts the view of the central government. According to the selection mode of this ‘disciplinary diagram’, 23 parishes of the city were entrusted with aiding the sick and cleaning houses and streets based on their own normalising judgement. Each of them constituted a Parish Health Deputation, chaired by the parish priest, and constituted one priest, four citizens, a doctor, a surgeon and a pharmacist (Deputazione Comunale di sanità, 1857: 242). The hierarchy in the ‘disciplinary diagram’ indicated that the Pope, utilising a Special Congregation of Health, comprising prelates and chaired by a cardinal, directly supervised the Provincial Deputation of Health of Bologna. The Provincial Deputation of Health of Bologna was chaired by the Legate, Monsignor Grassellini, and included three representatives of the central government and a member of the Senate of Bologna (Deputazione Comunale di sanità, 1857: 217). The experts of the medical sciences were relegated to a consultative role in the Provincial Deputation of Health and were divided into two branches: a chemical section and a surgical-medical section including four university professors and two doctors (Deputazione Comunale di sanità, 1857: 217). The central operating pole relied on Monsignor Grassellini, who, as chair of the Provincial Deputation, appointed all the members of the Parish Health Deputation.
The second ‘disciplinary diagram’ represented the local government's view of the city and was based on a municipal body. The Sanitary Reform n. 887 of 22 July 1836 had established a Municipal Deputation of Health in the city to manage epidemics involving the care of the sick and the burial of corpses (Fondo Commissione Provinciale di sanità della Legazione di Bologna FCPS, 1836: 2). It was chaired by a parish priest and composed of six people from medical staff, one member of the clergy, and four citizens. However, after 1836, the political and social climate of the city must have changed because, on 18 June 1855, it was replaced by an Extraordinary Municipal Deputation of Health (EMDH), chaired by Dr Paolo Predieri (conservatore municipale) from the Medical-Surgical Society and comprised two doctors (secretary and vice-secretary), six medical deputies (three professors, one doctor, one pharmacist) and five non-medical deputies (four lay members and one Monsignor). This second ‘disciplinary diagram’ was the expression of the medical expertise of the Medical-Surgical Society, and the presence of a Monsignor was justified by the necessity to coordinate with the parishes (Deputazione Comunale di sanità, 1857: 224).
This EMDH, expression of the medical expertise, planned the four modes of the ‘disciplinary diagram’. First, the main actors were selected: the Lazzaretti, places of confinement, isolation, and care (Sabbatani et al., 1997), and the Uffizi di Soccorso, neighbourhood offices set up to verify the cases of cholera. According to the normalisation mode, the infection case must be, first of all, reported to an Uffizio, and only after the doctor had visited the patient (Deputazione Comunale di sanità, 1857: 257). In the case of overt cholera, the patient was referred to a Lazzaretto or, depending on the severity of the symptoms, cared for at home with drugs provided free of charge by the neighbourhood pharmacy. The EMDH supervised (hierarchisation) the intellectual machinery and established a Central Health Office (CHO) as its central repository to meet and allocate resources among all the actors (Verardini, 1856). It employed eight doorkeepers and two messengers at its entrance to transmit orders and instructions to the Uffizi di Soccorso, hospitals, parishes, and wherever it was necessary to send a message (Deputazione Comunale di sanità, 1857: 260).
The accounting technology for the emergency
The ‘disciplinary diagram’ executed by the medical experts, who were accustomed to carrying on scientific reporting, was the only one to adopt an accounting technology supporting the emergency plan. The importance of the ‘pathological, therapeutic and clinical statistics’ was one of the main scientific themes discussed within the Medical-Surgical Society (Sighinolfi, 1924: 147). This kind of reporting was executed during the cholera epidemic to combat the disease. It consisted of detailed tables, accompanied by a letter from the doctor who drew them, where each row showed the clinical health status of each patient (Figure 3). These tables represented the base to enhance the scientific knowledge about cholera (Brugnoli, 1887: 11–13).
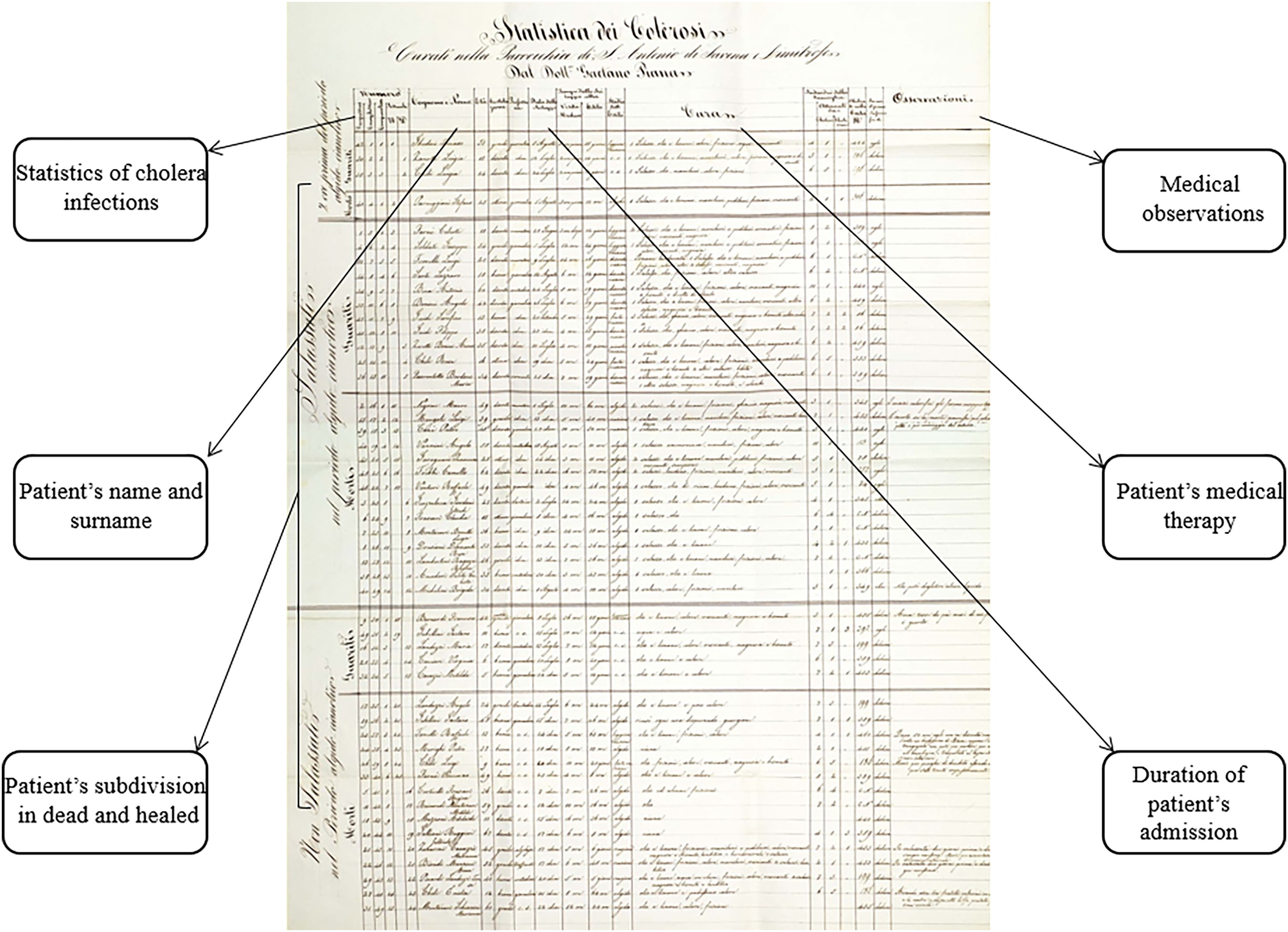
An example of scientific reporting of a doctor on 17 December 1855. Source: BCAB, Brugnoli 43.
However, the intellectual machinery developed by the EMHD also needed a medico-administrative information system to work. The CHO operationalised it in two forms: accounting for and accounting of the epidemic (Moerman and van der Laan, 2022).
The medico-administrative accounting for cholera
This form of accounting technology considered visits, hospitalisations and deaths as quantitative measures of the ‘disciplinary diagram’ and therefore accounted for to allow the EMHD to supervise and manage the emergency. The CHO standardised the recording and documentation of visits, hospitalisations and deaths through pre-printed forms to be filled by the Uffizi di Soccorso and Lazzaretti periodically. When an overt case of cholera was detected in the Uffizio di Soccorso, the doctor of the Uffizio notified the CHO and sent a form to the Lazzaretto for the hospitalisation of the patient (Figure 4).
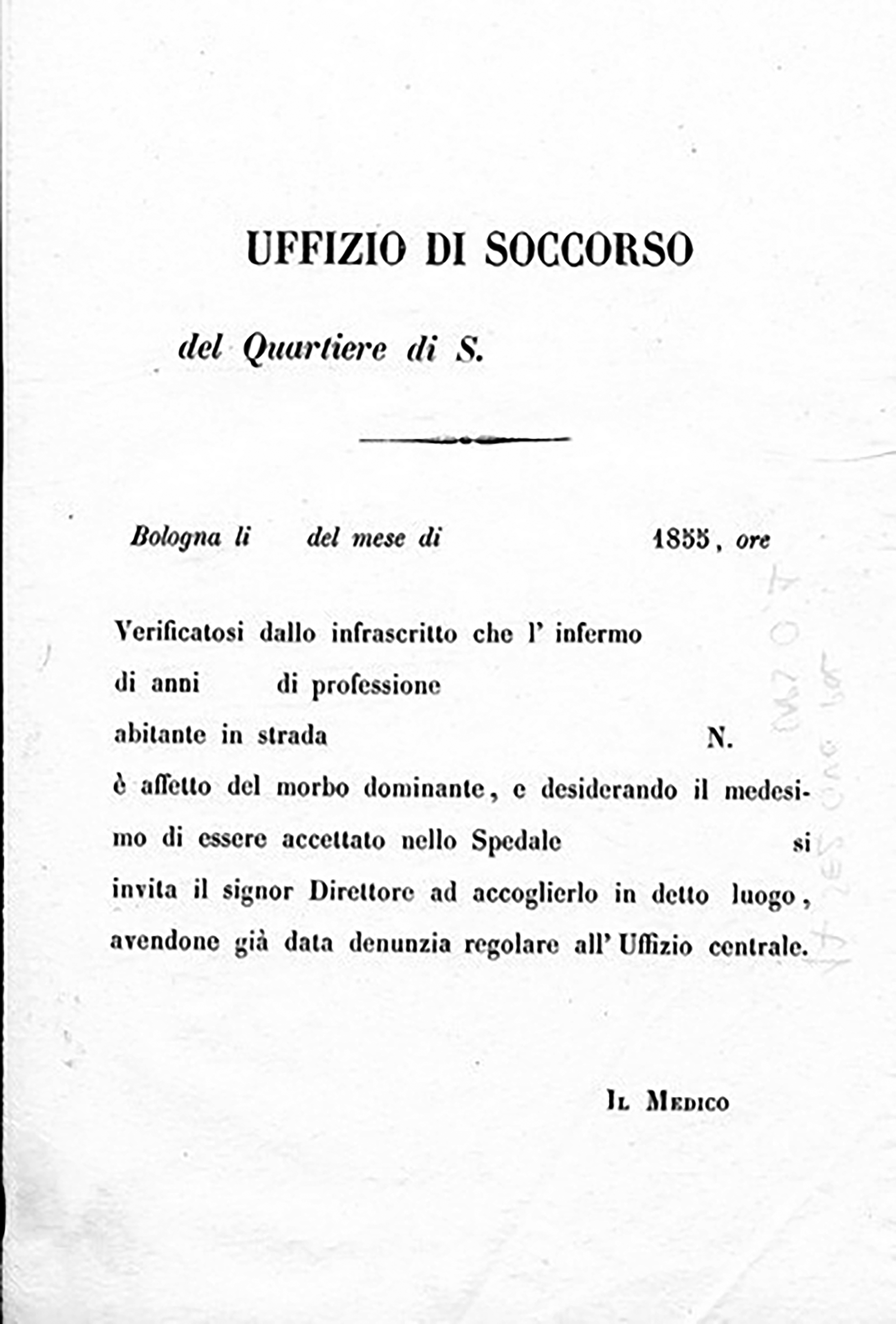
Form for hospitalisation of the patient in the Lazzaretto. Source: ACB, CA, 1855.
The Uffizi di Soccorso had to send their reports to the CHO regularly. Each Uffizio di Soccorso was equipped with register clerks in charge of collecting the notification of suspected cases and the doctors’ reports. Additionally, the Uffizi produced a daily report of the number of medical examinations by the doctor, the names of the patients and the diagnosis for each case (Figure 5).
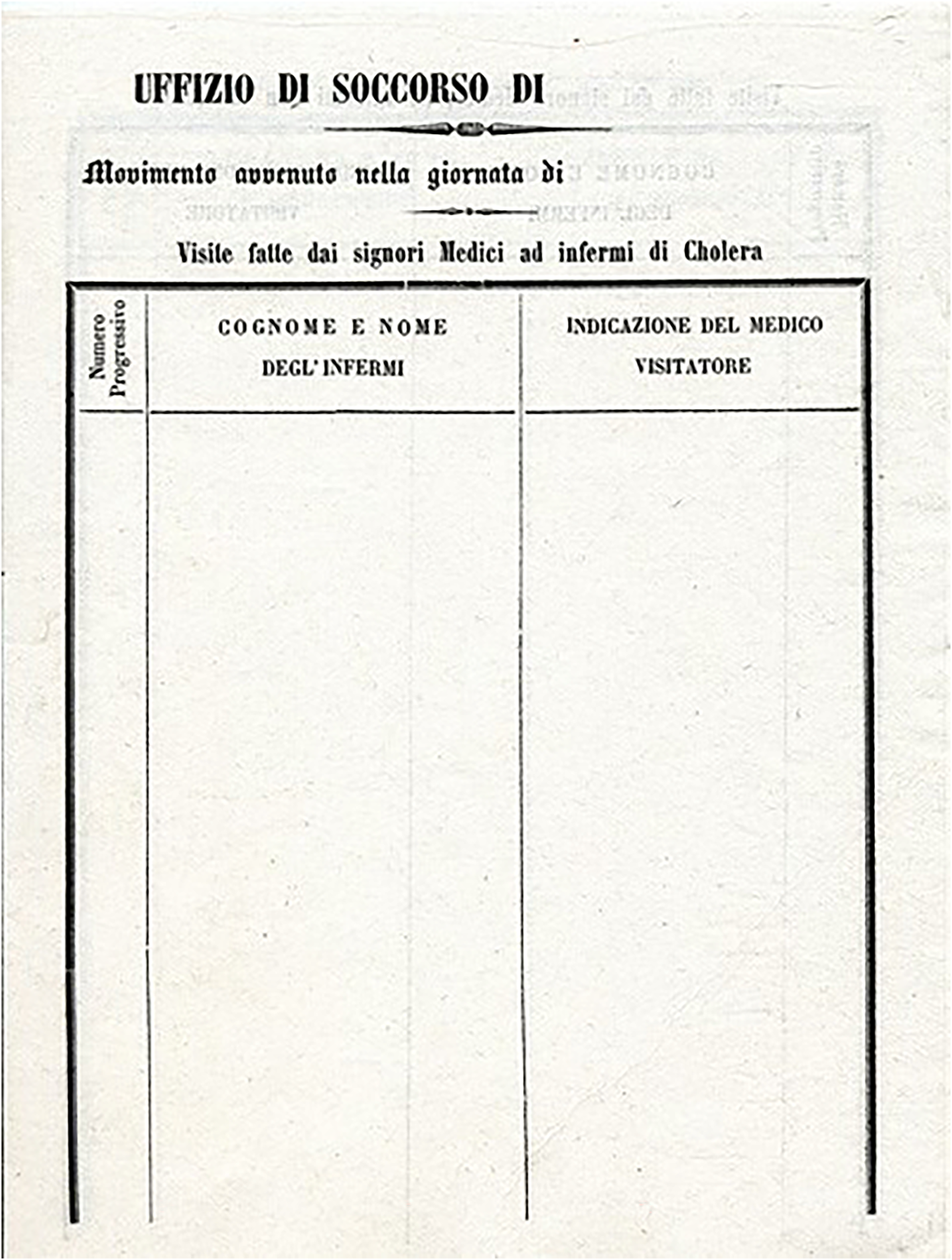
Daily register form of Uffizi di Soccorso. Source: ACB, CA, 1855.
The medico-administrative accounting of cholera
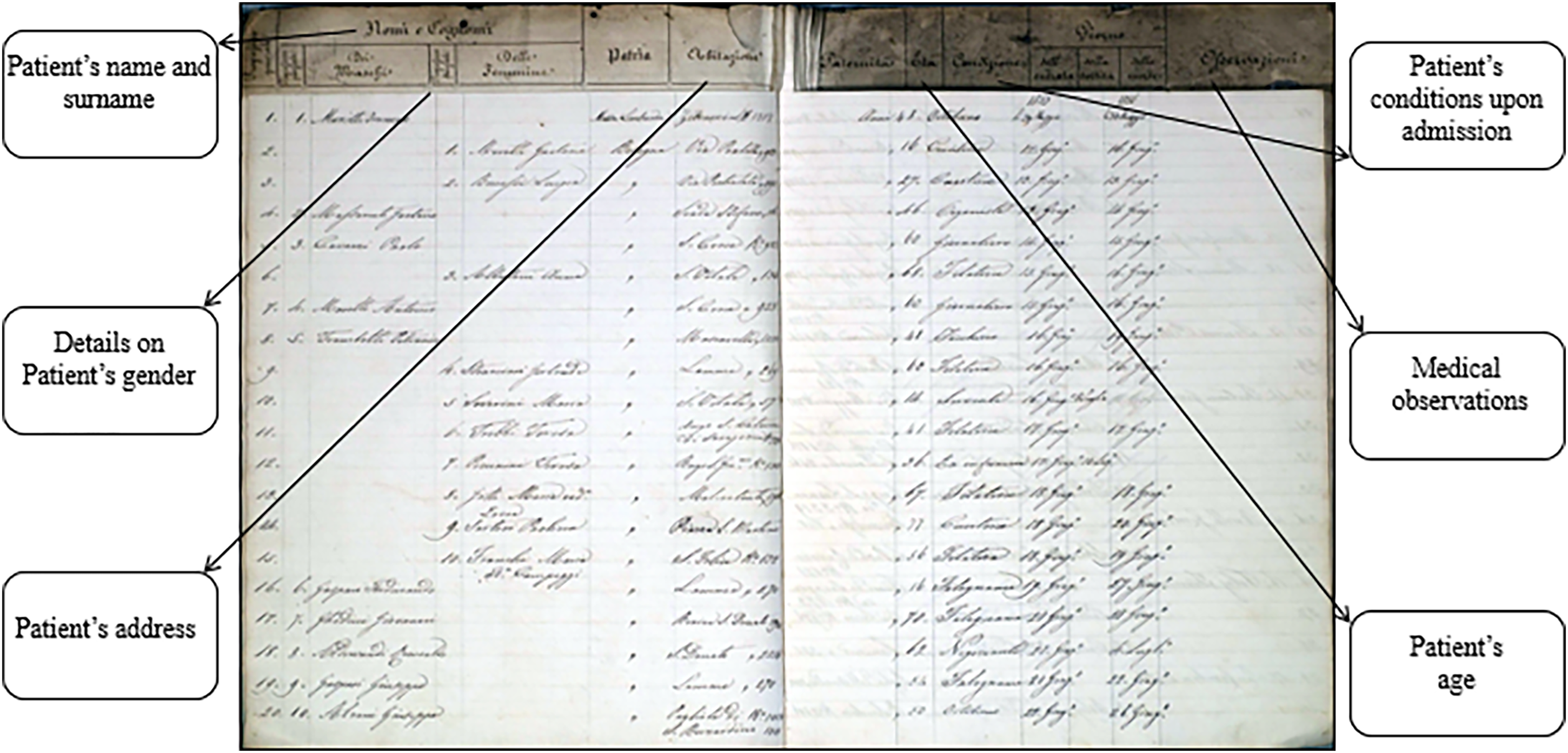
This second form of accounting technology considered cases of contagion, visits, hospitalisations, and deaths as consequences of the epidemic, as well as performance indicators of the ‘disciplinary diagram’. The CHO maintained a general register collecting all the reports of contagion both in the city and its surroundings. It reported, with the progressive number and annotation of the day, time and Uffizio di Soccorso where the case was detected, names of the patients and their fathers, age, marital status, profession and address. Moreover, it specified the house where they lived, the place where they were cured, the names of their doctors, and who signalled the infection. The last record reported the positive or negative outcome of the disease as well as the day and time of the outcome.
Furthermore, secondary registers were maintained: a register for the city cholerosis and another for the healed, with separate sections for the city and its surroundings, and a register of people admitted to hospitals. ‘In this way, it was easy to know in each moment the Health Bulletin of the reports of cholera cases, of the healed, of the dead, of those received in hospitals’ (Deputazione Comunale di sanità, 1857: 260).
The Uffizi sent their data thrice a day (before 8 a.m., 12 p.m., and 8 p.m.) to the CHO, which compiled a bulletin of the cases and sent it to the Government, Military and Municipal Authorities. The 12 p.m. bulletin was also distributed to anyone interested. The number of those requiring it ‘grew so much that the Deputation was forced to publish it’ (Deputazione Comunale di sanità, 1857: 260). A doctor suggested selling the bulletin every day and using the proceeds for cholera orphans’ assistance. The EMDH also published health bulletins covering a longer period, starting from the official beginning of the epidemic, 29 May 1855, and reporting the numbers of dead, recovered and in-care patients, sometimes classifying them by gender (Figures 6–8). These reports were also published in the official source of the city government, the Gazzetta di Bologna (GB) (BCAB, GB n. 220).
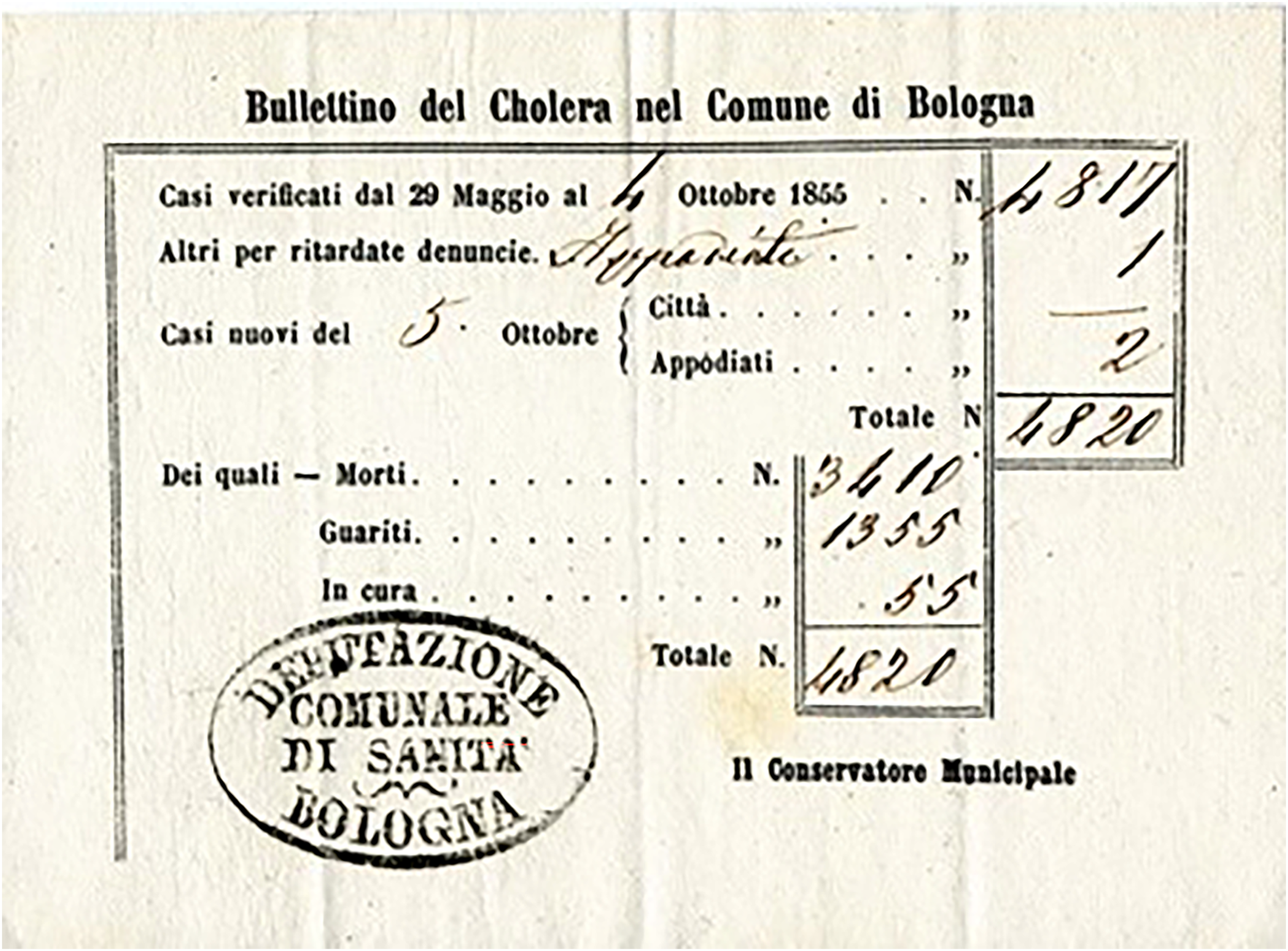
Health bulletin of cholera cases in Bologna from 29 May until midnight on 4 October 1855. Source: ACB, CA, 1855.
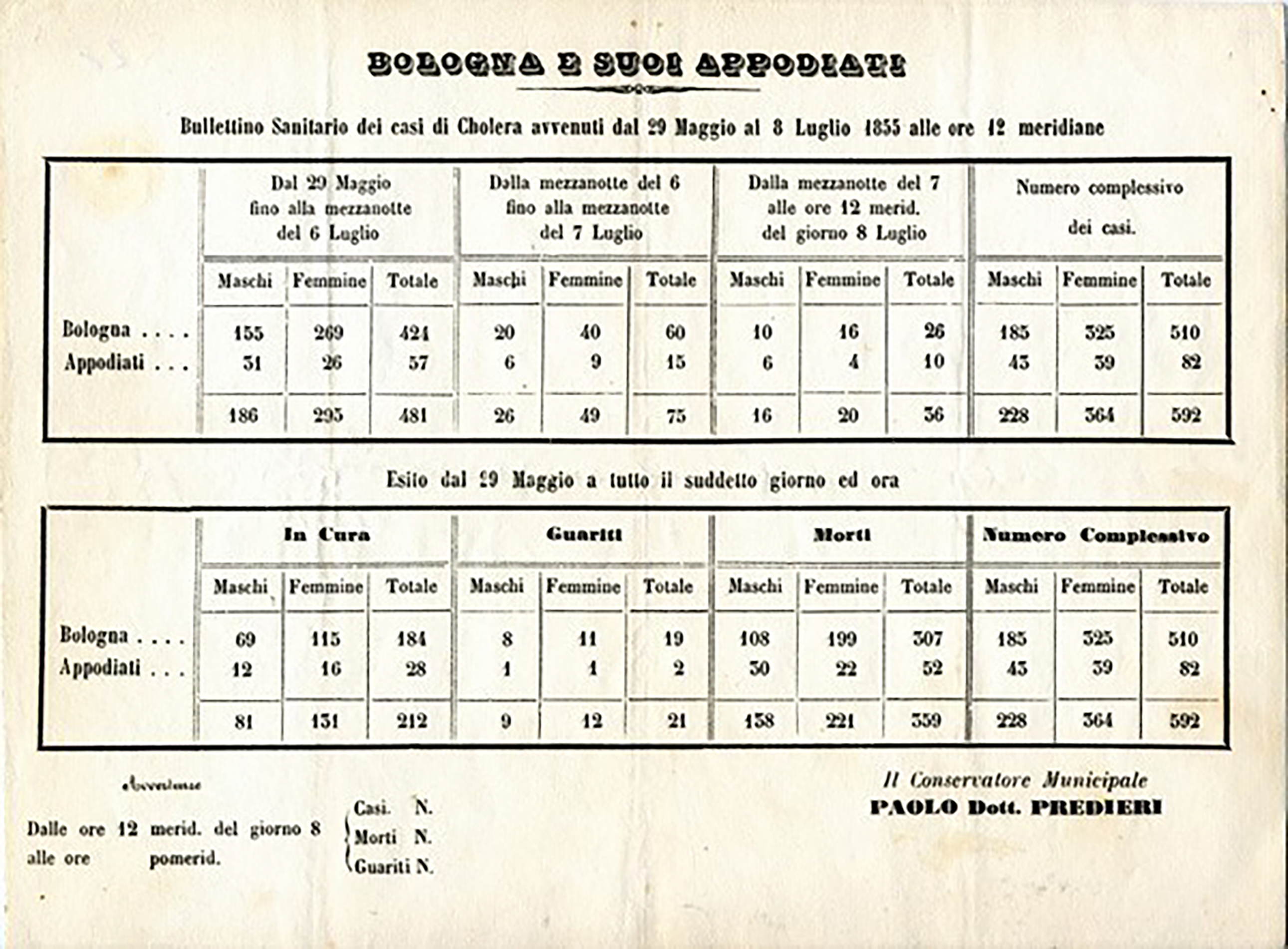
Health bulletin of cholera cases in Bologna from 29 May until 8 July 1855 at 12 noon. Source: ACB, CA, 1855.
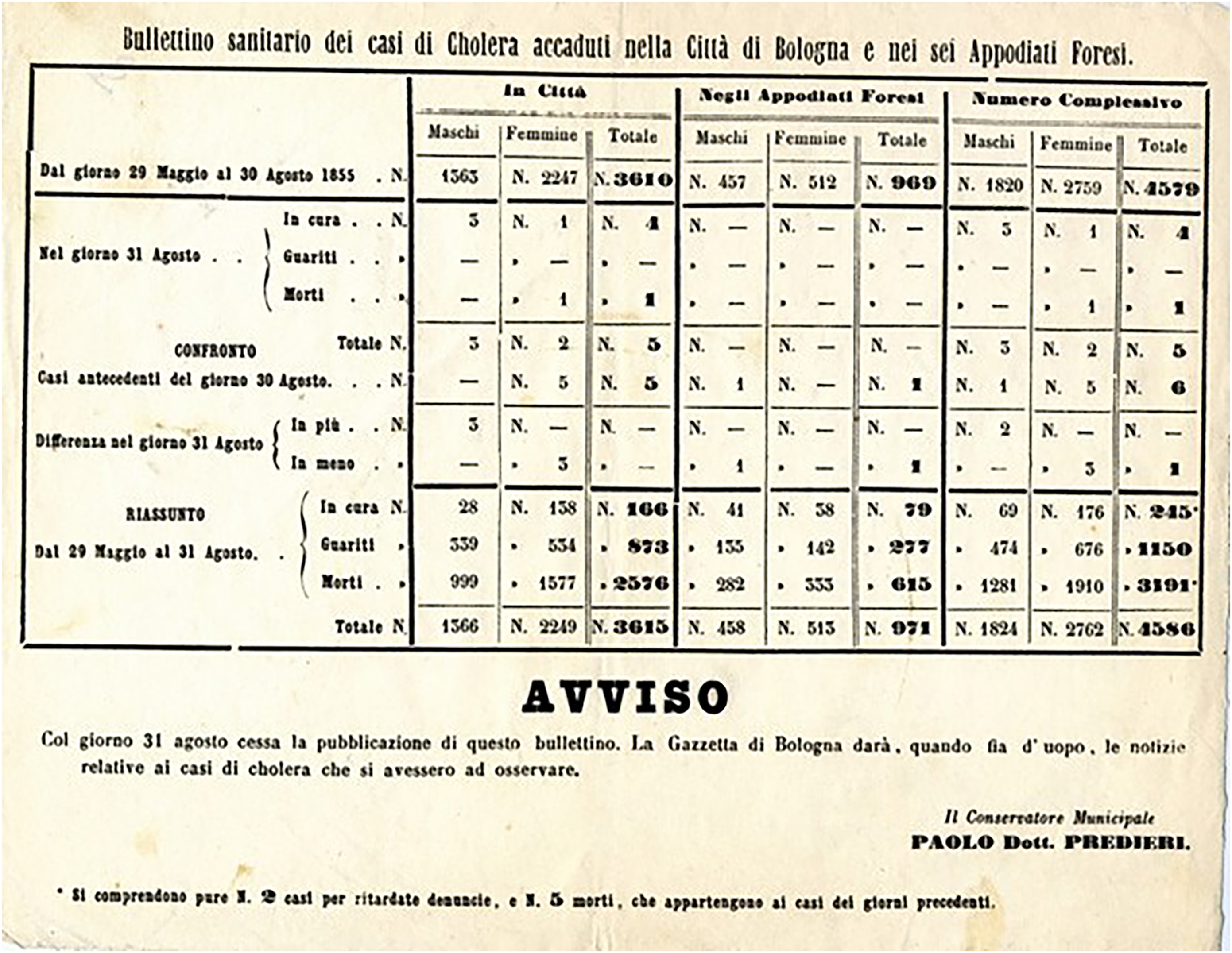
Health bulletin of cholera cases in Bologna from 29 May until 30 August 1855. Source: ACB, CA, 1855.
To maintain these records and draft the bulletins, the CHO was equipped with a ‘First Clerk’ and five other clerks under the direction of the secretary (doctor), vice-secretary (doctor) and the Inspector of the Uffizi di Soccorso (Deputazione Comunale di sanità, 1857: 260).
The experts pose problems for the political authorities
The two ‘disciplinary diagrams’ conflict
Experts would enter into a kind of double alliance. On the one hand, they would ally themselves with political authorities, focusing upon their problems … translating political concerns … into the vocabulary of … medicine. On the other hand, they would seek to form alliances with individuals themselves translating their daily worries and decisions … into a language claiming the power of truth and offering to teach them the techniques by which they might manage better … (Rose and Miller, 1992: 188).
The fact that the experts, that is, the Medical-Surgical Society of Bologna, which has always been inspired by a secular vision of the life and government of the city, implemented a ‘disciplinary diagram’ independent of that of the central Papal power testifies its choice that it should not enter alliances with the political authorities but should propose an alternative way of managing the emergency. This circumstance caused the conflict between clerical and anti-clerical political rationalities, pre-existing in the city, to translate into a conflict between ‘disciplinary diagrams’.
The anti-clericals openly criticised both Senator Davia and Legate. The Senator was viewed as a weak personality, incapable of providing for the city government (Bottrigari, 1960: 320), and Monsignor Grassellini was described as a fearful inept and a deserter: Monsignor (Grassellini) perseveres in the fear and is an impassive spectator of the misfortunes that afflict the poor city. Therefore, no initiative on the part of the (pontifical) government to improve the very painful condition in which we find ourselves; no measure that applies to public health, none that heartens the hearts of citizens! Some philanthropists wanted to set up a Society to collect offerings to relieve the poor Orphans whose parents had been taken away by the disease; but Monsignor objected. Who would believe it! The Municipality provides for everything, which is increasingly burdened by the huge expenses that the (pontifical) government bears on it …. Since a case of cholera had occurred in the apostolic palace, the Monsignor, in fear, …, expelled the Central Health Commission, appointed by the Town Hall. This poor Commission, homeless, took refuge in the deserted hall known as the Podestà, building canvas huts for their own shelter. Incredible things, if they did not happen under the eyes of everyone. After giving this order, Monsignor hastily hitched up the horses to go to Modena to breathe uninfected air (Bottrigari, 1960: 336–337).
Moreover, the Provincial Deputation of Health, chaired by Grassellini, questioned the charitable spirit of the medical establishment of the city by sending them formal complaints as some doctors, called to assist the sick, had referred them to the Uffizi di Soccorso (Figure 9). The Uffizi di Soccorso were the first line bodies of the ‘disciplinary diagram’ of the medical establishment of the city. However, the complaints indicated that the Uffizi were to be considered as a secondary option in the absence of anything else.
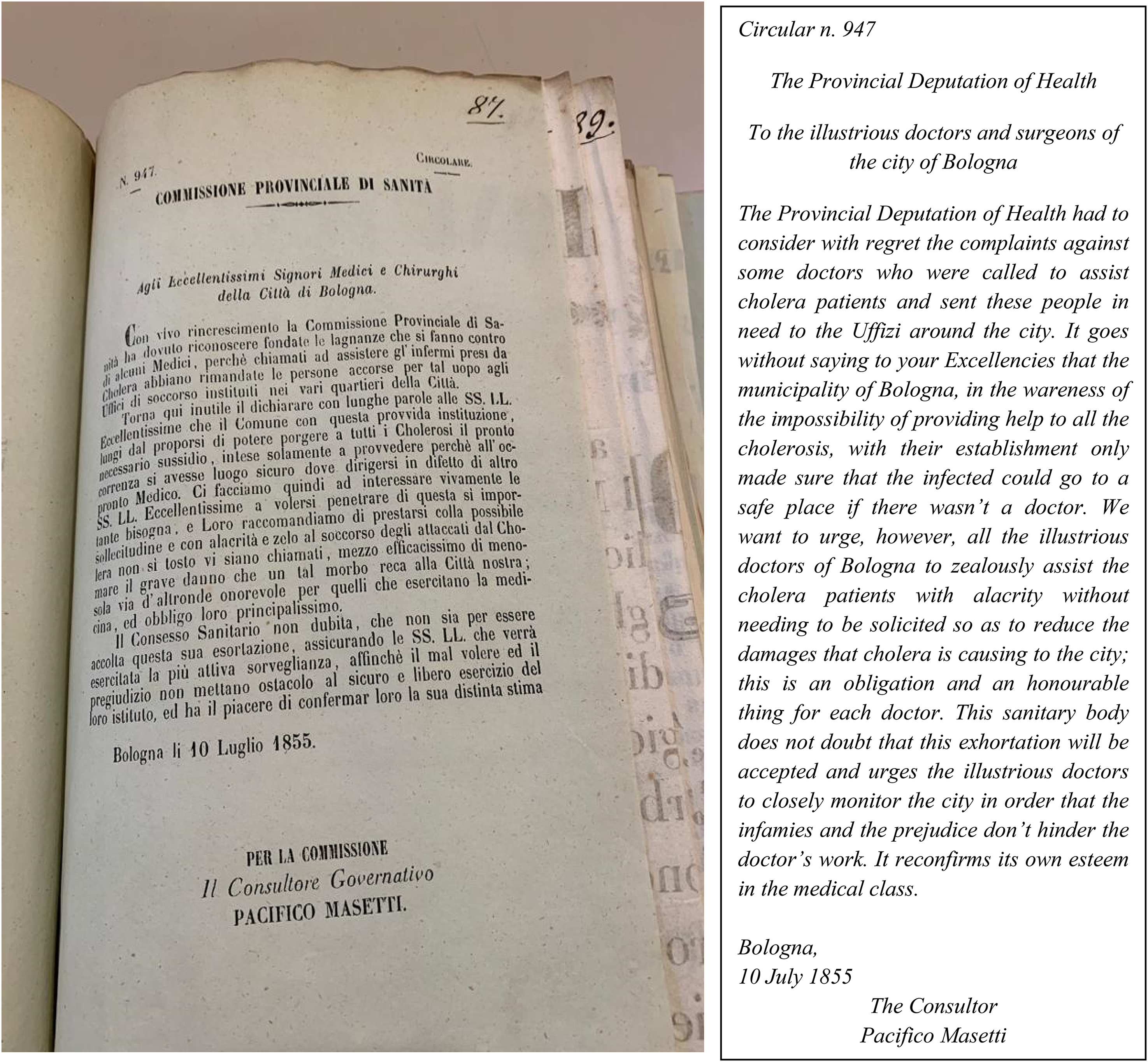
The provincial deputation of health questions the role of the Uffizi di Soccorso. Source: ASB, Commissione di sanità del Dipartimento del Reno (CSDR), Serie Stampe (S), 1855.
From the medico-administrative accounting to the politico-medical hold of the city
The effectiveness of the ‘disciplinary diagram’ implemented by the Medical-Surgical society to manage the emergency was predictable, given the assumptions. What was less predictable was that the experts literally replaced the political authorities in governing the city.
‘Government is defined as a right manner of disposing things’ (Foucault, 1991: 95), and the administrative documents of Bologna show Predieri disposing things for the city not only in the medical field but also by signing provisions that were in charge of the political authority, Senator Davia, and only subsequently communicating them to the latter.
We find evidence in a long letter Predieri sent to Senator Davia on 20 July 1855, reporting the formal provisions signed by Predieri with which he had adopted the solutions considered more appropriate by him. Specifically, he had changed the intended use of buildings according to Monsignor Grassellini's decision (Figure 10); he established new Uffizi (Figure 11) and managed to find and rent new locations for them (Figure 12); he coordinated the countermeasures to be adopted by the mayors of the surrounding villages, hired employees, assigned them to Uffizi and Lazzaretti, and defined their remunerations (ACB, CA, 1152, 1855).
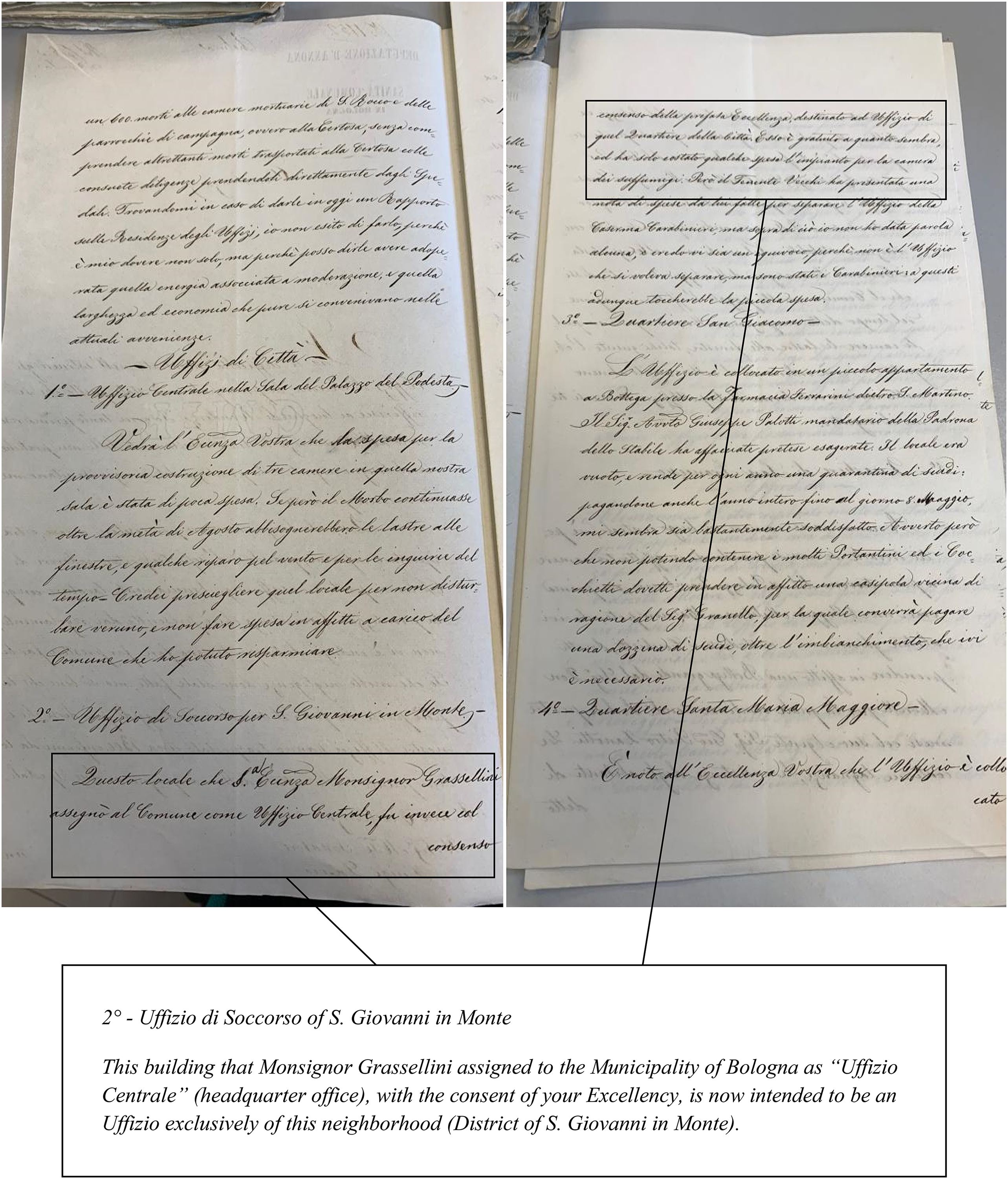
Dr Paolo Predieri changes the use of buildings in contrast to Monsignor Grassellini's previous decisions. Source: ACB, CA, 1152, 1855.
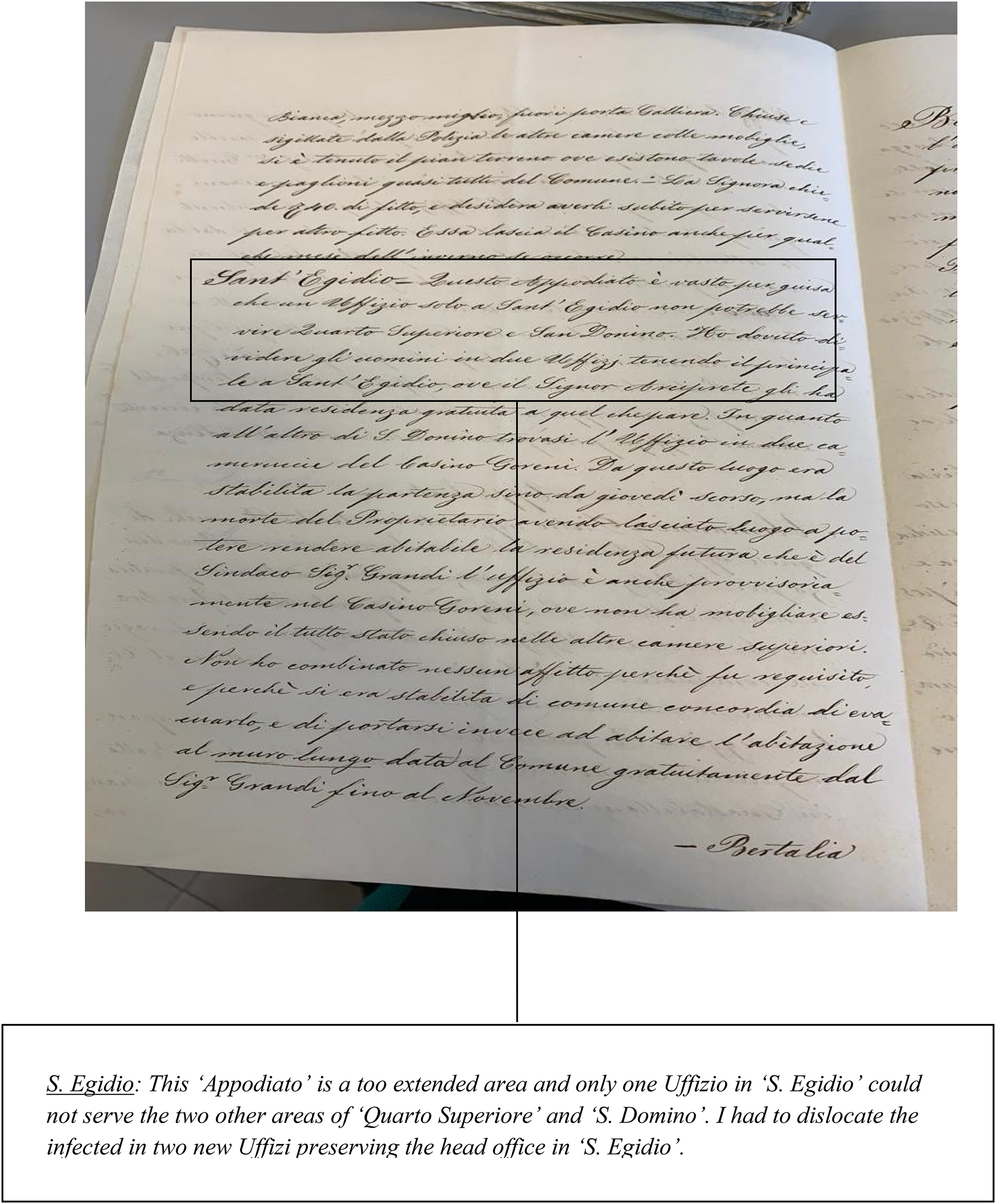
Dr Paolo Predieri establishes other Uffizi in the surroundings of the city. Source: ACB, CA, 1152, 1855.
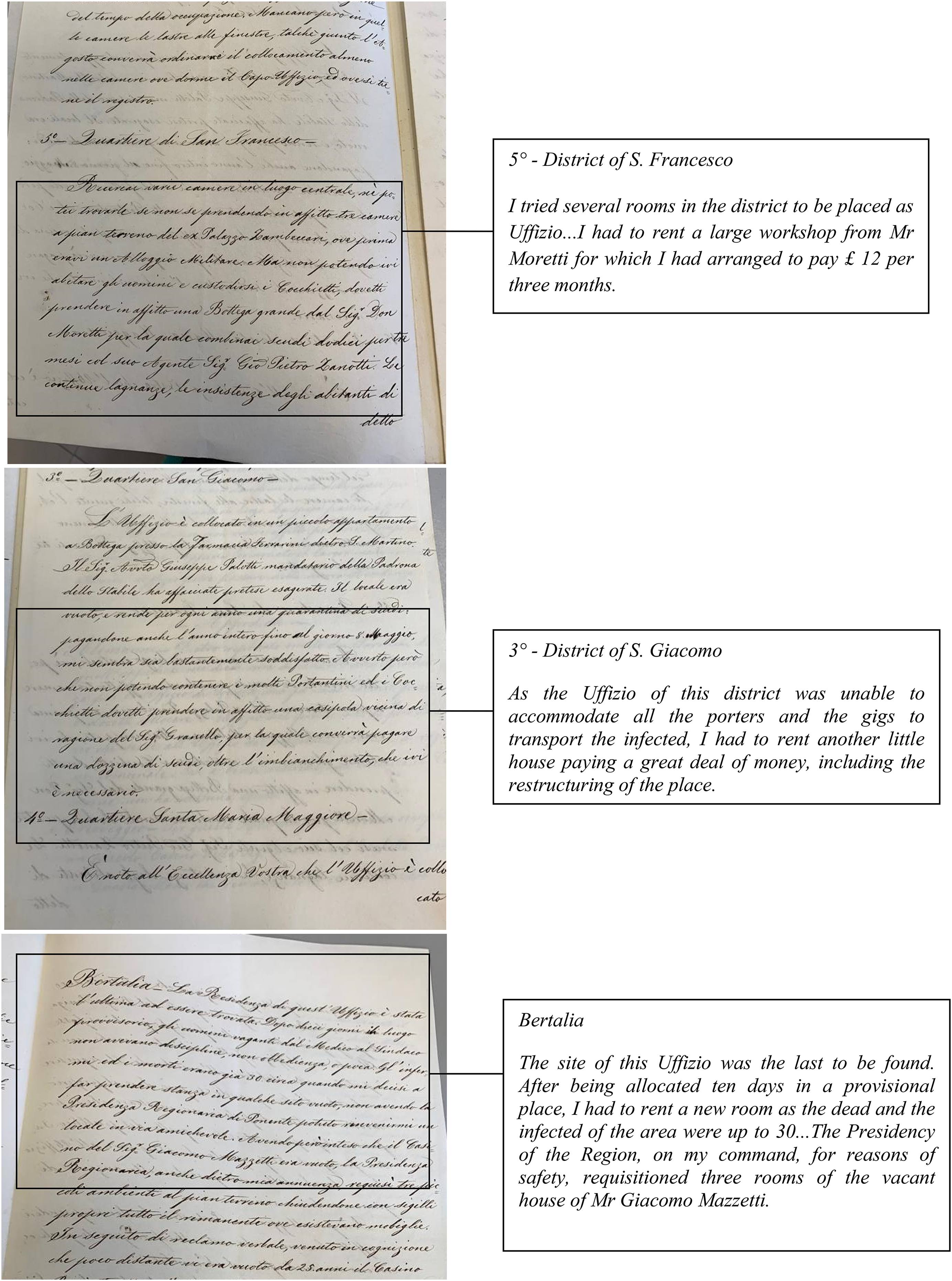
Dr Paolo Predieri manages to find new locations for the Uffizi. Source: ACB, CA, 1152, 1855.
This letter, where Predieri also complained about the lack of zeal of the priests (‘How religious and civil it would be if the priests, in addition to the doctors, accompanied the transport of the sick to the Lazzaretti!’), testifies that the ‘disciplinary diagram’ of the experts had de facto taken control of the city, removing it from the bodies expressing the central Papal power. The parish health deputations, the emergency centres in the ‘disciplinary diagram’ of the central Papal government, ended up losing any role relating to the care of the sick and were limited to charitable activities for orphans and the destitute (BCAB, Brugnoli 28; Deputazione Comunale di sanità, 1857: 331). ‘The parish priests reported to the CHO what the needs of each person and place were and obtained the most appropriate measures’ (Deputazione Comunale di sanità, 1857: 224).
The justification provided in the letter was the urgency to act under the emergency push and the information deriving from the medico-administrative accounting that only Predieri could have at his disposal. The accounting technologies he could rely on were included to provide evidence of the goodness of his choices: In order for your Excellency to know what has already been studied by the Municipal Deputation of Health and what are the effects obtained so far; I believed I was gathering together various documents relating to the management that it believed it had to give after June 20 in obedience to the higher prescriptions on the dominant disease and gathered here the reports compiled by the sections that this your Municipal Deputation appointed to know and direct the various related tasks the health rules that must be followed in these unfortunate emergencies (ACB; CA, 1518, 1855).
summary of the statistics of the infirm who entered, left and died in hospitals, a report from the chief physician of the main hospital of the city, S. Lodovico, which describes the therapeutic treatment used in the treatment of the sick and the outcome obtained so far, and the latest health bulletin and a summary of all cases reported in the municipality from 29 May to 20 July and of those who are being treated and deceased, both males and females, in the city and its surroundings (ACB; CA, 1518, 1855).
The inclusion of the accounting technologies had the purpose to ‘persuade’ Senator Davia:
With these reports and documents, your excellence will be able to know the state of things attributable to the sanitary conditions of this municipality and at the same time will be able to persuade You of the many difficulties that have been presented up to now and of the best ways used to solve them and improve them (ACB; CA, 1518, 1855).
The letter praised the effectiveness of the accounting technologies in supporting decisions:
Your Excellency, in general, the rule prescribed by the Deputation for keeping records and reporting the sick, deaths and the cured, as well as the accompanying letters of the sick to the hospital and deaths to the mortuary, was recognised as good and uniform. Equally commendable are the provisions made regarding the equipment of the personnel assigned to the Uffizi, … And although the visit is carried out suddenly and in the afternoon hours, which are the most critical, since they are those in which everyone is absent to take food, the offices are also found to be sufficiently equipped for the personal help, especially the low attendants (ACB, CA, 1152, 1855).
The persuasive power of accounting technologies was effective, as Senator Davia responded with meekness to the new situation and warmly supported Predieri in illustrating the importance of the reporting system to the population by reminding doctors, parishioners and pharmacists of the importance of complaints of cholera cases, which would have affected the government choices (BCAB, Brugnoli 28).
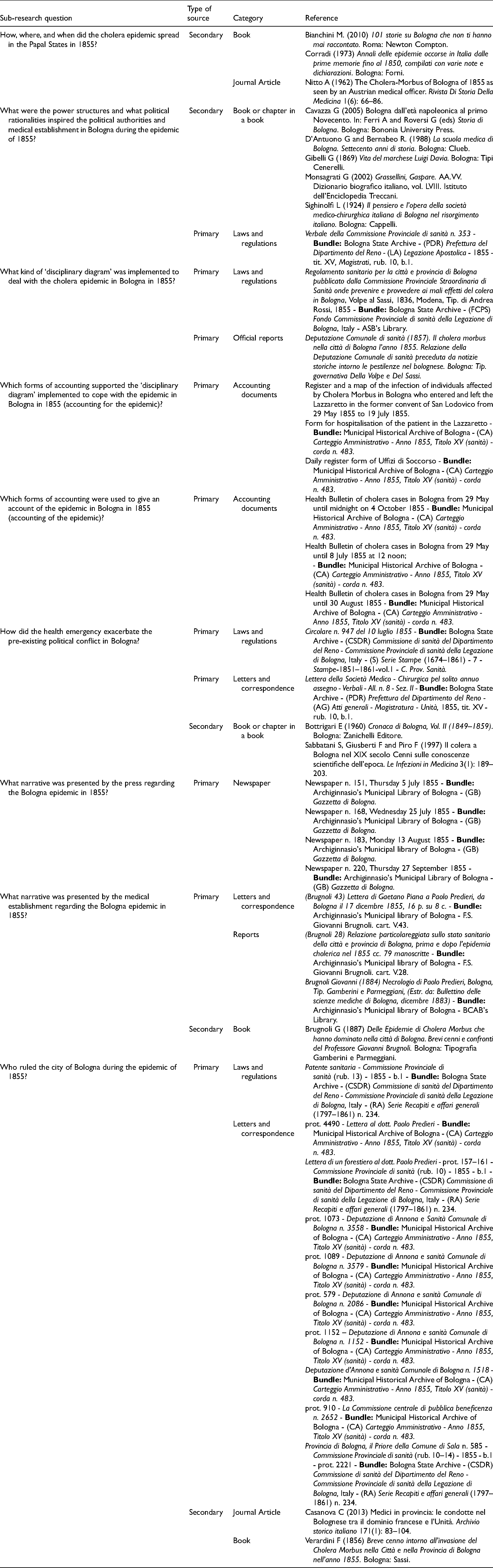
Predieri, strong in his leadership, also took the chance to defend the interest of the medical establishment: ‘Experts have the capacity to generate what we term enclosures: relatively bounded locales or types of judgement within which their power and authority is concentrated, intensified and defended’ (Rose and Miller, 1992: 188). The medical officers of the province for years had complained of being underpaid and forced to live in penury (Casanova, 2013; Sighinolfi, 1924: 220). Predieri addressed many requests to Senator Davia to appropriately remunerate the medical officers again, leveraging accounting technologies. Each request was justified through reports certifying their professional services (Figure 13).
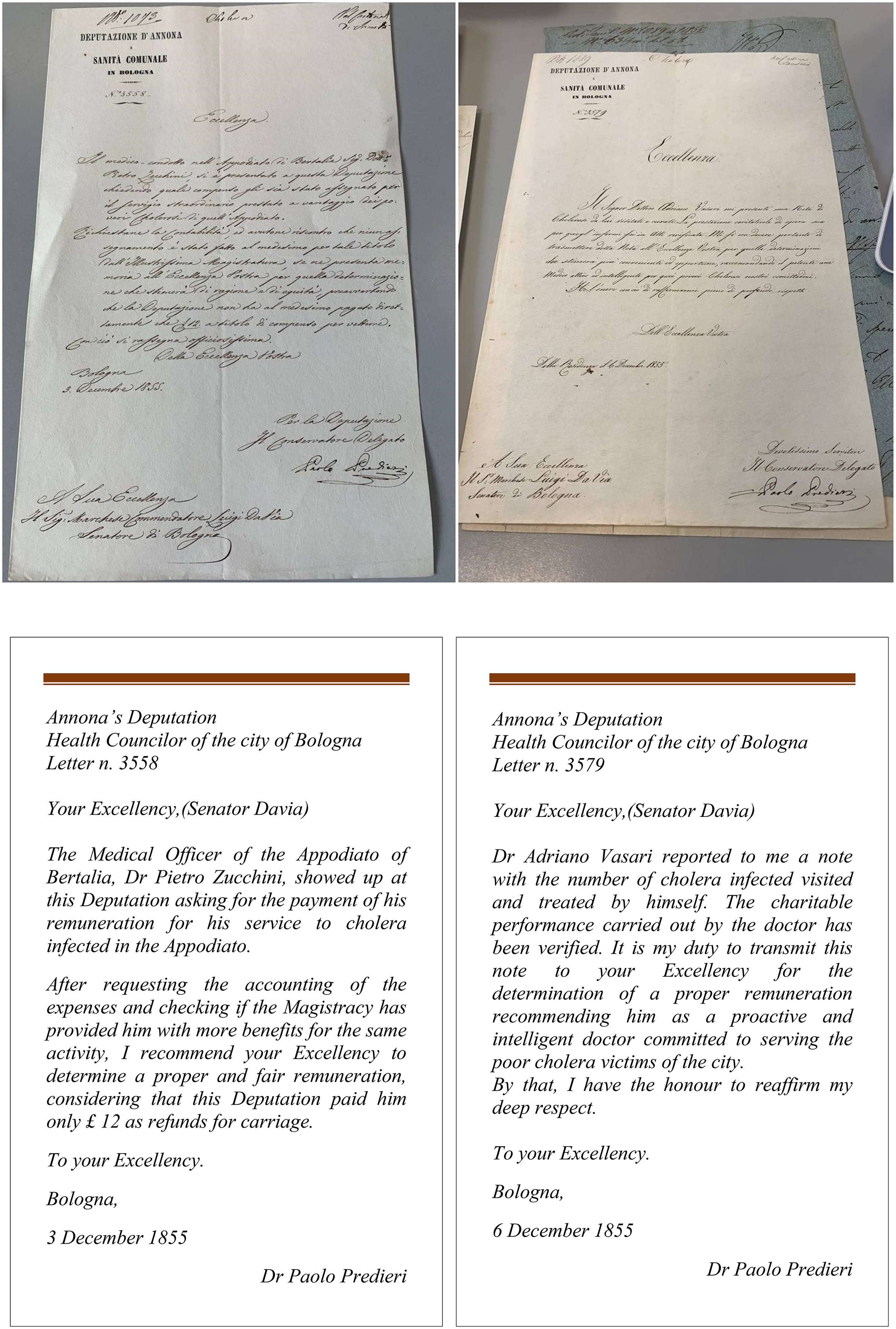
Examples of Predieri's requests addressed to Senator Davia to obtain remuneration for medical officers. Source: ACB, CA, prot. 1073; ACB, CA, prot.1089.
Predieri managed to achieve what the anti-clericals aspired for years, namely, the city government by means of a secular class. Anti-clerical sources took this occasion to praise the heroism of the secular government of the city and its medical establishment (Bottrigari, 1960). The Medical-Surgical Society always considered Dr Predieri a hero because he, ‘de facto, governed Bologna’ by chairing the EMDH that, during the epidemic, ‘night and day, provided for all sanitary measures and all needs of the population of the whole city’ (Brugnoli, 1887: 3).
After the epidemic, the EMDH, in its official final report, stated that, in accordance with Senator Davia, Predieri ‘made all the administrative decisions and emanated all the orders and the necessary measures to be taken to limit the effects of the epidemic and preserve the city of Bologna and its population’ (Deputazione Comunale di sanità, 1857: 258). Moreover, the Pope gave him the prestigious title of Cavaliere del Pontificio Ordine di San Gregorio Magno ‘for his outstanding achievements during the 1855 health emergency in the city’ (Deputazione Comunale di sanità, 1857: 336).
Analysis and conclusions
Following the call of Sargiacomo et al. (2021) to consider natural disasters as social phenomena and to explore, in accounting history research, perspectives offered by politics, we have examined the relationship between scientific expertise, accounting and power. The existing accounting literature has highlighted some of the possible roles accounting can play during the occurrence of a natural disaster (Baker, 2014; Lai et al., 2014; Rahaman et al., 2010). However, the potential of the experts’ inscriptions has been overlooked despite the natural disaster management involving some kind of scientific expertise. This case study explores this potential in a scenario where the experts and political authorities are inspired by different political rationalities.
Walker (2014: 2) has highlighted that ‘in contexts where there already exists discontent in civil society a natural calamity … provides opportunities for the advocates of alternative modes of socio-political action to gain currency (Pelling and Dill, 2006)’ and that ‘heroic bureaucracies’ may emerge. In addition to the esprit de corps, the main characteristic of this heroic bureaucracy is the conduct of ‘demonstration endeavours’ or large-scale efforts to devote public resources to a significant social problem in a new manner (Marcus, 1981: 129). During the cholera epidemic of Bologna, the ‘heroic doctor’ emerged with scientific knowledge and accounting numbers rendering the emergency a knowable, calculable and administrative object.
This case study highlights the role of medico-administrative accounting as a technology for the politico-medical hold of the population. The EMDH, in addition to defining the reports of the epidemic as a ‘means of evidence’ of the advancement of medical science and a tool to ‘find aetiological and therapeutic truth’, also officially stated that ‘deductions arise from them that are certainly useful for the Medical Police to which they were intended and also beneficial to the administrators of public affairs’ (Deputazione Comunale di sanità, 1857: 363–366). Furthermore, the EMDH stated that the reports were explicitly aimed to inspire reflections for the ‘philosopher doctor and the politician’ (Deputazione Comunale di sanità, 1857: 367).
In addition, it shows the role of medico-administrative accounting as a persuasive tool to replace, within an epidemic scenario, a clerical ruling class with a secular one constituting doctors. This result evokes the ancient figure of the medicus-politicus, formalised in the seventeenth century by Dr Rodrigo de Castro (1614). His practice is addressed not only to the individual but also to society because scientific-technical knowledge and human–social understanding form an inseparable whole and medicine is authentic only if it is also an ‘ethics of the polis’ (Cosmacini, 2021). Similarly, Foucault (1975: 33) states that the doctor's first task is political: ‘the fight against disease must begin with a war against bad governments’.
The persuasive power of medico-administrative accounting is derived from both science and accounting. As Latour (1983: 144) stated: science is ‘one of the most convincing tools to persuade others of who they are and what they should want’. The persuasive power of science is due to being linked to reason and rationality. In contrast, ‘accounting numbers command consent’ because ‘inscriptions make black boxes visible’ and ‘visualisation is especially persuasive’ (Chua, 1995: 116).
Predieri made the black box of the emergency visible to Senator Davia so that it could be imaged, counted and, above all, managed. In this way, his medico-administrative accounting allowed to transform into ‘docile bodies’ (Foucault, 1995) not only those affected by the disease but also political opponents such as Davia to whom there was nothing left but to (ex-post) legitimise Predieri's disciplinary power over the city.
The accounting literature about expertise's role has mainly focused on accounting, financial and auditing expertise (Gendron et al., 2007; Neu et al., 2006; Power, 1995, 1996, 1997, 2003; Rahaman et al., 2007) or the role of experts on accounting practices’ change (Chua, 1995). Sargiacomo and Walker (2022) have recently argued the role of experts in solving problems at the meso-political and micro-organisational levels during disaster governance. This case study has focused on the less explored scientific–medical expertise and on a scenario of conflict between the experts and official political authorities owing to a lack of alignment in terms of political rationales.
The study confirms that ‘the complex of actors, powers, institutions and bodies of knowledge that comprise expertise have come to play a crucial role in establishing the possibility and legitimacy of government’ and that ‘expertise … poses problems for political authority’ (Rose and Miller, 1992: 188). Specifically, it reveals the experts’ ability to replace the political authorities by leveraging their accounting technologies and the emergency push of natural disasters. As these accounting technologies are mainly calculative practices related to death, the study also provides new perspectives of investigation into the intersections between accounting and death, as advocated by Moerman and van der Laan (2022). Finally, it adds to the confluence between natural disasters and the local–central government interplay (Sargiacomo et al., 2021) by demonstrating that the experts’ accounting technologies mobilised in health emergencies are not politically neutral in the case of a problematic relationship between local and central government. Further, it can exacerbate its conflictual nature in favour of one or the other party.
Van Bavel et al. (2020) argue that analysing past disasters not only helps to understand the political functioning of past societies but also allows a better understanding of how societies should deal with current disasters. Compared to any previous health catastrophe, we witnessed a global medicalisation of the fight against the COVID-19 pandemic. Science has never assumed such a preponderant role; the decisions relied on the data of the epidemiologists and knowledge of the virologists. Medicine appeared to be the guardian of the health of humanity and guarantor of political choices. Further research is required on the potential of medico-administrative accounting technologies in these scenarios.
Footnotes
Acknowledgements
The authors gratefully acknowledge the anonymous reviewers for their insightful comments and suggestions, which have significantly strengthened the article.
Author contributions
The article is the result of a joint effort of the authors, the individual contributions are as follows: Tiziana Di Cimbrini wrote the ‘Introduction’; ‘Theoretical framework’; ‘Research Method’ and ‘Analysis and conclusions’; Alessio Maria Musella wrote ‘Cholera in Bologna in 1855’; ‘An emergency plan with two disciplinary diagrams’; ‘The accounting technology for the emergency’; ‘The medico-administrative accounting for cholera’; ‘The medico-administrative accounting of cholera’; ‘The experts pose problems for the political authorities’; ‘The two disciplinary diagrams conflict’; ‘From the medico-administrative accounting to the politico-medical hold of the city’; Christian Corsi wrote ‘Bologna in the Papal States in 1855’; ‘The political authorities and their political rationale’; ‘The experts and their political rationale: The Medical-Surgical Society’.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix 1 – Primary and secondary sources of the cholera epidemic in Bologna in 1855.
| Sub-research question | Type of source | Category | Reference |
|---|---|---|---|
| How, where, and when did the cholera epidemic spread in the Papal States in 1855? | Secondary | Book |
Bianchini M. (2010) 101 storie su Bologna che non ti hanno mai raccontato. Roma: Newton Compton. |
| Corradi (1973) Annali delle epidemie occorse in Italia dalle prime memorie fino al 1850, compilati con varie note e dichiarazioni. Bologna: Forni. | |||
| Journal Article | Nitto A (1962) The Cholera-Morbus of Bologna of 1855 as seen by an Austrian medical officer. Rivista Di Storia Della Medicina 1(6): 66–86. | ||
| What were the power structures and what political rationalities inspired the political authorities and medical establishment in Bologna during the epidemic of 1855? |
Secondary | Book or chapter in a book | Cavazza G (2005) Bologna dall'età napoleonica al primo Novecento. In: Ferri A and Roversi G (eds) Storia di Bologna. Bologna: Bononia University Press. |
| D’Antuono G and Bernabeo R. (1988) La scuola medica di Bologna. Settecento anni di storia. Bologna: Clueb. | |||
| Gibelli G (1869) Vita del marchese Luigi Davia. Bologna: Tipi Cenerelli. | |||
| Monsagrati G (2002) Grassellini, Gaspare. AA.VV. Dizionario biografico italiano, vol. LVIII. Istituto dell’Enciclopedia Treccani. | |||
| Sighinolfi L (1924) Il pensiero e l’opera della società medico-chirurghica italiana di Bologna nel risorgimento italiano. Bologna: Cappelli. | |||
| Primary | Laws and regulations | Verbale della Commissione Provinciale di sanità n. 353 - |
|
| What kind of ‘disciplinary diagram’ was implemented to deal with the cholera epidemic in Bologna in 1855? | Primary | Laws and regulations | Regolamento sanitario per la città e provincia di Bologna pubblicato dalla Commissione Provinciale Straordinaria di Sanità onde prevenire e provvedere ai mali effetti del colera in Bologna, Volpe al Sassi, 1836, Modena, Tip. di Andrea Rossi, 1855 - |
| Primary | Official reports | Deputazione Comunale di sanità (1857). Il cholera morbus nella città di Bologna l’anno 1855. Relazione della Deputazione Comunale di sanità preceduta da notizie storiche intorno le pestilenze nel bolognese. Bologna: Tip. governativa Della Volpe e Del Sassi. | |
| Which forms of accounting supported the ‘disciplinary diagram’ implemented to cope with the epidemic in Bologna in 1855 (accounting for the epidemic)? | Primary | Accounting documents | Register and a map of the infection of individuals affected by Cholera Morbus in Bologna who entered and left the Lazzaretto in the former convent of San Lodovico from 29 May 1855 to 19 July 1855. |
| Form for hospitalisation of the patient in the Lazzaretto - |
|||
| Daily register form of Uffizi di Soccorso - |
|||
| Which forms of accounting were used to give an account of the epidemic in Bologna in 1855 (accounting of the epidemic)? | Primary | Accounting documents | Health Bulletin of cholera cases in Bologna from 29 May until midnight on 4 October 1855 - |
| Health Bulletin of cholera cases in Bologna from 29 May until 8 July 1855 at 12 noon; - |
|||
| Health Bulletin of cholera cases in Bologna from 29 May until 30 August 1855 - |
|||
| How did the health emergency exacerbate the pre-existing political conflict in Bologna? | Primary | Laws and regulations | Circolare n. 947 del 10 luglio 1855 - |
| Primary | Letters and correspondence | Lettera della Società Medico - Chirurgica pel solito annuo assegno - Verbali - All. n. 8 - Sez. II - |
|
| Secondary | Book or chapter in a book | Bottrigari E (1960) Cronaca di Bologna, Vol. II (1849–1859). Bologna: Zanichelli Editore. | |
| Sabbatani S, Giusberti F and Piro F (1997) Il colera a Bologna nel XIX secolo Cenni sulle conoscenze scientifiche dell’epoca. Le Infezioni in Medicina 3(1): 189–203. | |||
| What narrative was presented by the press regarding the Bologna epidemic in 1855? | Primary | Newspaper | Newspaper n. 151, Thursday 5 July 1855 - |
| Newspaper n. 168, Wednesday 25 July 1855 - |
|||
| Newspaper n. 183, Monday 13 August 1855 - |
|||
| Newspaper n. 220, Thursday 27 September 1855 - |
|||
| What narrative was presented by the medical establishment regarding the Bologna epidemic in 1855? | Primary | Letters and correspondence |
(Brugnoli 43) Lettera di Gaetano Piana a Paolo Predieri, da Bologna il 17 dicembre 1855, 16 p. su 8 c. - |
| Reports | (Brugnoli 28) Relazione particolareggiata sullo stato sanitario della città e provincia di Bologna, prima e dopo l’epidemia cholerica nel 1855 cc. 79 manoscritte - |
||
| Brugnoli Giovanni (1884) Necrologio di Paolo Predieri, Bologna, Tip. Gamberini e Parmeggiani, (Estr. da: Bullettino delle scienze mediche di Bologna, dicembre 1883) - |
|||
| Secondary | Book | Brugnoli G (1887) Delle Epidemie di Cholera Morbus che hanno dominato nella città di Bologna. Brevi cenni e confronti del Professore Giovanni Brugnoli. Bologna: Tipografia Gamberini e Parmeggiani. | |
| Who ruled the city of Bologna during the epidemic of 1855? | Primary | Laws and regulations | Patente sanitaria - Commissione Provinciale di sanità (rub. 13) - 1855 - b.1 - |
| Letters and correspondence | prot. 4490 - Lettera al dott. Paolo Predieri - |
||
| Lettera di un forestiero al dott. Paolo Predieri - prot. 157–161 - Commissione Provinciale di sanità (rub. 10) - 1855 - b.1 - |
|||
| prot. 1073 - Deputazione di Annona e Sanità Comunale di Bologna n. 3558 - |
|||
| prot. 1089 - Deputazione di Annona e sanità Comunale di Bologna n. 3579 - |
|||
| prot. 579 - Deputazione di Annona e sanità Comunale di Bologna n. 2086 - |
|||
| prot. 1152 – Deputazione di Annona e sanità Comunale di Bologna n. 1152 - |
|||
| Deputazione d’Annona e sanità Comunale di Bologna n. 1518 - |
|||
| prot. 910 - La Commissione centrale di pubblica beneficenza n. 2652 - |
|||
| Provincia di Bologna, il Priore della Comune di Sala n. 585 - Commissione Provinciale di sanità (rub. 10–14) - 1855 - b.1 - prot. 2221 - |
|||
| Secondary | Journal Article | Casanova C (2013) Medici in provincia: le condotte nel Bolognese tra il dominio francese e l’Unità. Archivio storico italiano 171(1): 83–104. | |
| Book | Verardini F (1856) Breve cenno intorno all’invasione del Cholera Morbus nella Città e nella Provincia di Bologna nell’anno 1855. Bologna: Sassi. |