
Abstract
The beneficial potential for music in hospital contexts is well established, with research showing that music can promote patient well-being and support recovery. However, less attention has been paid to the ways in which musicians’ practices and professional identities are informed by working in hospital settings. As arts-and-health approaches continue to proliferate, it is essential to recognize the values, emotional labor, and skills associated with these approaches through understanding the experiences of practitioners. As part of an international collaboration led by Hanze University in the Netherlands, the ProMiMiC project explores the professional development of musicians and nurses through person-centered music-making in hospital settings. The current study focused on five conservatoire-trained musicians’ delivery of personalized music-making via Zoom in a hospital maternity setting in London during the COVID-19 pandemic. Their experiences of adapting to the new context, and the impacts on their personal and professional development, were explored using reflective journals, group discussions, and semi-structured interviews. The data were interpreted using the theoretical lens of vocational habitus to examine the skills and dispositions required to be the right musician for this job. Qualitative synthesis revealed the musicians’ developing musical values as they adapted to the online maternity setting, highlighting the centrality of communicative and musical versatility as well as the ability to connect and empathize through music. The findings offer insights into possible ways of supporting emerging music practitioners in healthcare settings and emphasize the imperative for higher music education to prepare and train musicians for this type of work.
Keywords
The utility of music in hospital settings is well established, from reducing pain (Dobek et al., 2014; Nilsson, 2008), and lowering anxiety and stress (Bradt et al., 2013; van der Heijden et al., 2015), to promoting well-being during recovery (Evans, 2002; van der Wal-Huisman et al., 2018). Live music, in particular, has been shown to be beneficial for patients’ recovery (Hole et al., 2015; Walworth et al., 2008), supporting social interactions that can further enhance patients’ satisfaction and staff–patient relationships (Petrucci, 2018; van der Wal-Huisman et al., 2018). Also, when performing live music in hospitals, musicians have the advantage of being able to adapt to patients’ situations and preferences in real time (Smilde et al., 2019).
In the Netherlands, a specialist practice named Meaningful Music in Healthcare (MiMiC) has been developed as a form of highly individualized musical engagement between musicians and hospital patients (Smilde et al., 2019). 1 MiMiC takes a person-centered approach that emerged through workshops and creative practice with people living with dementia, aiming to retain the personhood and identity of participants (Dons et al., 2021; Smilde et al., 2014, 2019). Its goal is to co-create a musical experience that is meaningful for both patient and musicians (Smilde et al., 2019; Zeilig et al., 2018). Research into the MiMiC approach has shown that it can be used across numerous healthcare settings including hospital wards and care homes (Smilde et al., 2019), and be effective for both patients and musicians. To date, however, the MiMiC practice has not been applied to the specific context of hospital maternity wards (used in this article to refer to hospital wards that care for people during pregnancy and birth).
Patients hospitalized during pregnancy can experience high levels of stress and uncertainty (Cetin et al., 2017; Gourounti et al., 2015; Kent et al., 2015; Zadeh et al., 2012), which has been further linked to negative impacts on postnatal mental health (Beck, 2001; Milgrom et al., 2008; Robertson et al., 2004). For expectant parents, music has been identified as a promising method for promoting well-being, due to both the observed prevalence of personal use of music during pregnancy (Arabin & Jahn, 2013) and its use as a way of alleviating anxiety and stress (Sanfilippo et al., 2021; Shin & Kim, 2011; Ventura et al., 2012). Systematic reviews suggest that, although there is inconsistent evidence for the long-term effects of music interventions during pregnancy, they may decrease anxiety for expectant mothers immediately post-intervention (Corbijn van Willenswaard et al., 2017). However, as Corbijn van Willenswaard et al. (2017) noted, the use of live music in clinical maternity settings appears to be far less common than the use of recorded music. In light of the importance of the social support provided by family, midwifery, and medical staff (Gupton et al., 1997; Leichtentritt et al., 2005) for people hospitalized during pregnancy, the role of live, personalized music to enhance these relationships may be particularly valuable.
There is currently little understanding of how musicians train for, adapt to, and experience live music-making in maternity settings. The experience of working with women with postnatal depression, for example, can have a significant emotional impact on musicians. If they are to respond to people’s specific needs, musicians need to have formed strong team relationships, to be flexible, and to plan ahead (Perkins et al., 2018). However, additional factors associated with the hospital setting, and participants who are pregnant, may also have an impact on the ways in which musicians prepare for and experience this type of work. Indeed, the majority of existing arts-and-health literature, particularly in relation to maternity settings, focuses on outcomes for patients, which limits our understanding of how practitioners’ development and well-being can be supported most effectively. As highlighted by Hume and Parikh (2022), it is crucial for building sustainable practices in creative, health-related, practice to acknowledge the impact of this type of work for practitioners, and to understand the skills and processes required to deliver it.
This is particularly important given the growing prominence of health-related work in musicians’ professional portfolios. Arts-and-health and community approaches are valued by practitioners for building identity and musicianship (Ascenso, 2016), changing pedagogical approaches (Perkins et al., 2015), and promoting professional development and satisfaction (Hallam et al., 2016). The increasing focus in higher education music institutions on training musicians in these socially responsible practices reflects the importance of these activities and their growing role in musicians’ careers. Artistic citizenship and community engagement have begun to be incorporated in the curricula and graduate outcomes of these institutions, and their importance for building successful and socially responsible portfolio careers is frequently highlighted (Elliott et al., 2016; Gaunt et al., 2021). Gaunt et al. (2021) argue that the musician now performs a rapidly changing role as a “maker in society” (p. 1), in which their own social, moral, and political values are woven into their professional music practices, and where they must balance artistic creativity with societal engagement. There are growing calls not only for support for these activities in higher music education but also recognition of their implications for the practitioner’s well-being and how this can be protected (Belfiore, 2022; Hume & Parikh, 2022; Musgrave, 2022).
Insights into the ways in which musicians adapt and develop their practice in the specific context of MiMiC can be used to prepare other musicians to carry out this type of work, illuminating the values, emotional labor, and skills associated with it. Such preparation includes supporting musicians to respond to the specific needs of different groups of people, and to protect their own well-being. In the context of restricted access to hospitals during the COVID-19 pandemic, it also includes training them, where needed, to negotiate digital work and connect with patients through online technology. This research, therefore, focused on MiMiC in maternity hospital wards in the United Kingdom, exploring the ways in which professional musicians adapted to and developed the online delivery of personalized music-making.
Theoretical context and research question
To provide a conceptual grounding for the research, the lens of vocational habitus (Colley et al., 2003) was used to interpret the musicians’ experiences. Vocational habitus originates from the Bourdieuian concept (Bourdieu, 1989) of habitus, which explores how people’s identities and roles are negotiated and constructed in a field. The field in this case refers to the online maternity hospital setting. Bourdieuian habitus conceptualizes the shaping of our actions, choices, and practices by structural conditions including class, profession, and gender (Bourdieu, 1989), and suggests how we orientate ourselves around those conditions. This has particular applications in the workplace. Colley et al. (2003) have discussed the way vocational habitus can be seen as the combination of values and dispositions used by the individual to orientate themselves in professional settings. Vocational habitus is the process of developing an identity that is “the right person for the job” (Colley et al., 2003, p. 488). Vocational habitus can be thought of as “developing not only a ‘sense’ of how to be, but also ‘sensibility’: requisite feelings and morals, and the capacity for emotional labour” (Colley et al., 2003, p. 471).
In the workplace, the development of this sensibility is more complex than simply adapting to specific workplace values or cultures (Colley et al., 2003). It further involves the identities, backgrounds, and experiences of each individual. In the current project, for example, the processes of becoming the right person for the job are shaped by the musicians’ personal beliefs and previous experiences. This includes related forms of musical work, alongside the structural characteristics of the field (here the maternity wing of the hospital), the online context, and the wider arts-and-health setting. Our research, therefore, asked how professional musicians develop a sense of becoming the right musician for the job when entering the field of personalized, online music-making in a maternity hospital context.
Methods
Procedure
The study took place as part of the ProMiMiC research project, which explores the interprofessional learning processes that take place between musicians, nurses, and music therapists while delivering the live music practice MiMiC, as detailed above. ProMiMiC is led by the Lifelong Learning in Music research group at Hanze University, Groningen (the Netherlands). Partners in the project are the University Medical Center Groningen; the Nursing Diagnostics research group of Hanze University; Royal Conservatoire; The Hague; Haaglanden Medical Centre; The Hague; University of Music and Performing Arts, Vienna; Allgemeines Krankenhaus, Vienna; Royal College of Music/Centre for Performance Science, London; Chelsea and Westminster Hospital NHS Foundation Trust and its partner charity CW+; and Foundation Mimic Muziek. The project is co-financed through the RAAK-Pro program of Regieorgaan SIA, part of the Dutch Research Council (NWO). CW+ provided additional funding for the London study, particularly supporting patient evaluation.
For this study, the MiMiC practice was delivered over four periods of between 4 and 5 days each during 2021, as detailed in Table 1. During each period of delivery, three musicians worked together in a small team to connect virtually with patients on the maternity (predominantly antenatal) wards at Chelsea and Westminster Hospital in London. Due to COVID-19 restrictions, all the sessions were delivered online via Zoom. Musicians accessed the call together from the Royal College of Music and patients accessed the call via mobile/tablet while on site at the hospital. A research associate was also on the call (muted and camera off) to provide support. Each session lasted between 1 and 2 hr, interactions with individual patients lasting roughly 10–15 min each. During the interaction, the musicians would make music following the personalized MiMiC approach with each patient. This would involve asking them what sort of mood they would like the music to evoke, for example, or if they would like to offer a stimulus such as an emotion or a place for a personalized improvisation.
Details of delivery.
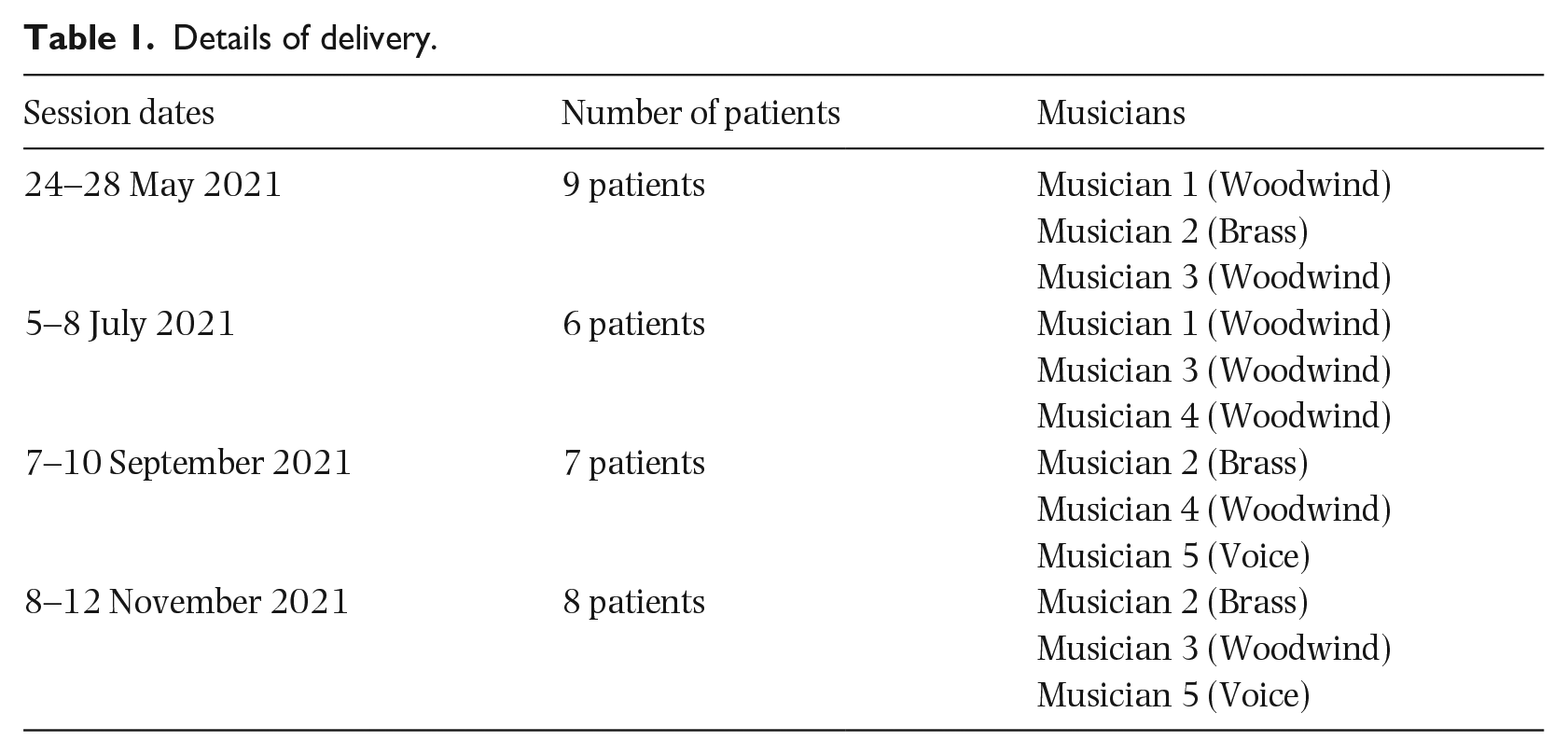
Patients were invited to take part on the day of each session by a project mediator (the second author). The mediator liaised between musicians and researchers on the Zoom call and the patients and staff on the ward. The mediator would visit each bed in the ward to invite patients to participate and help each interested patient set up their access to the call. In many cases, patients used their own devices and headphones to access the music session, but there was also a project tablet to use in cases where this was preferred. Patients only took part with their express consent; others in the ward were not exposed to the music because of the use of headphones. Patients were free to leave the Zoom call at any point without giving a reason and musicians debriefed at the end of each session to ensure a reflective approach to their practice.
Participants
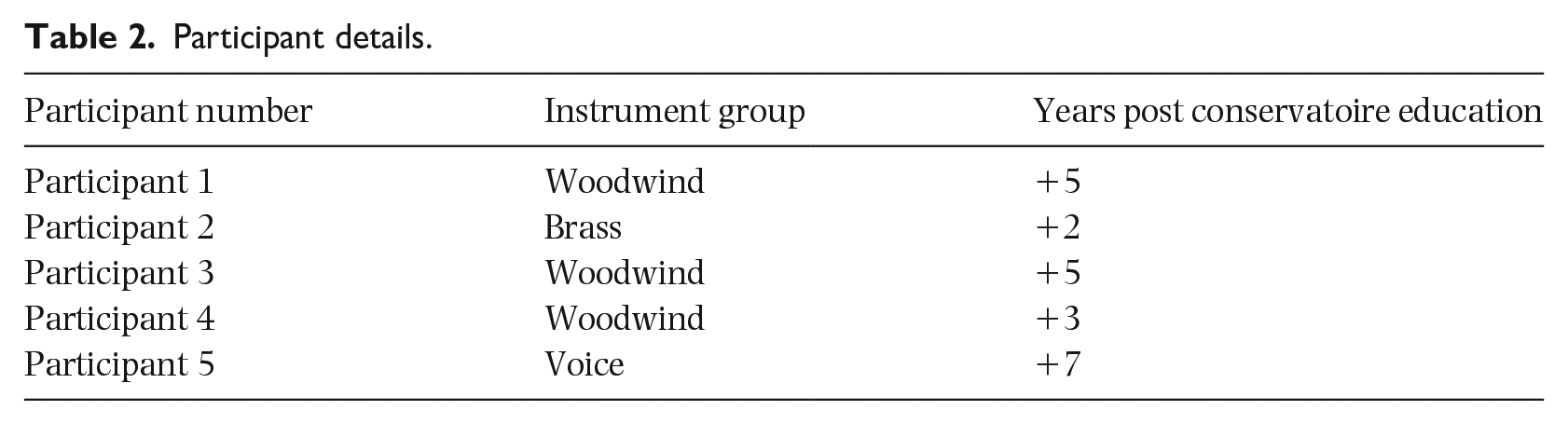
Five musicians were recruited to work on the project through an internal hiring process at the Royal College of Music. Once recruited, they were invited to take part in the research. 2 All participants were conservatoire graduates and had received training as instrumental or vocal specialists in the Western classical tradition. For the current project, training took place over 2 days and included an introduction to the MiMiC practice and the research, group discussions, three practical sessions based on improvisation and repertoire development, a site visit (pre-pandemic) to the maternity ward, and debrief sessions. The initial training, pre-pandemic, assumed face-to-face delivery, so the participants undertook further training once the decision was taken to move the project online. Ethical approval was granted by the Conservatoires UK Research Ethics Committee (21 December 2020, CUL/2020-21/1) and all participants gave informed written consent (see Table 2).
Participant details.
Methods
Data were collected using three qualitative methods: reflective journals, group discussions, and one-to-one semi-structured interviews. Each method was chosen to explore different elements of the participants’ experiences.
Data gathered in the reflective journals were used to understand participants’ experiences on a session-by-session basis. These journals were completed after each session in response to two open-ended questions: “What was today’s session like for you? What have you learnt from today’s session?” Participants completed the journals in writing or using voice messages that were later transcribed. The group discussions explored the participants’ collective experiences. At the end of each week’s cluster of sessions, a group discussion was conducted, guided by a starter invitation: “Let’s talk about how the sessions this week have gone and how we’ve experienced them.” The conversation was freely structured, allowing it to develop organically, with minimal intervention from the researcher. The aim of the one-to-one interviews was to understand each participant’s experience in retrospect. Each interview addressed the highlights and challenges of the project, according to the participant, and used their journals as a tool for generating their reflections on their experience of delivering the sessions.
The data were analyzed using qualitative synthesis (Hodkinson et al., 2005; Williamon et al., 2021). This method emphasizes the importance of producing an account that can be used for constructing a story. The method was deemed appropriate as it enabled the multiple sources of data to be integrated into a holistic account of the development of the participants’ vocational habitus. Analysis took place in three main stages, following Williamon et al. (2021). First, an in-depth reading of the dataset, synthesizing key elements relevant to the research question, was conducted by the first author and critically discussed with the third author. Second, the synthesis was developed by the first and third authors. This involved re-reading and organizing the key elements with iterative reference to the theoretical lens of vocational habitus to refine the account. Finally, the data were synthesized into a constructed story (Hodkinson et al., 2005) by all the authors, using the key elements defined in the first and second stages to organize the narrative.
Results and discussion
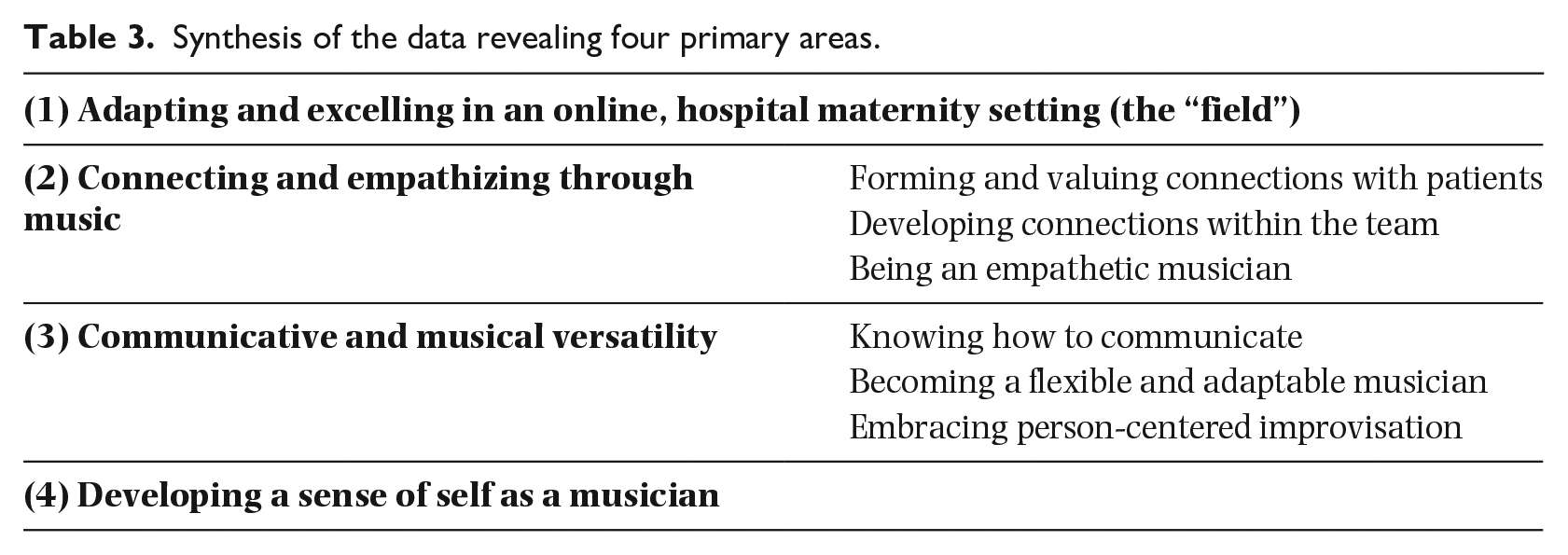
Synthesis of the participants’ data revealed four primary areas of development: (1) adapting and excelling in an online, hospital maternity setting (the field) and, within the field, 2) connecting and empathizing through music, (3) developing communicative and musical versatility, and (4) developing a sense of self as a musician (see Table 3). There were clear overlaps between these four areas, which are captured throughout our account and further discussed with reference to Figure 1 (see Discussion).
Synthesis of the data revealing four primary areas.
Summarizing the vocational habitus.
Adapting and excelling in an online, hospital maternity setting
The hospital maternity setting was a new experience for the participants: “It was an interesting experience because I mean, I’ve never even been around anyone that pregnant, so I’ve never even been in such a situation in real life” (P1). In addition to working in this new context, participants were delivering sessions in a new, online, format. Reflecting on their previous in-person hospital work, they reported that working online enabled their interactions with patients to feel more intimate and less subject to the distractions of a busy hospital setting. Furthermore, they did not have to recruit them; this burden was lifted from them by the involvement of the mediator in inviting patients to take part in the sessions and thus allowing the musicians to focus purely on their musical work. While participants expressed concern about the technical elements of online delivery, including the quality of the sound, Internet connection, and barriers associated with (not) being able to see the patients, these elements were outweighed in participants’ accounts by the opportunities that emerged: I think if we were there in person [it] will be completely different. I think it will be harder to concentrate, I think [it] will be harder to be able to . . . especially for the improvisations, to maybe get them to a very high standard, because of all the distractions, because of lots of people and noise . . . I know from experience of having played in hospitals before . . . sometimes it’s just really hard to get into the sort of good playing zone because there’s so much stuff happening . . . you see people and you’re also human, so you respond emotionally to a lot of things . . . So I think that was, in terms of music-making, maybe it [being online] was not the worst thing. (P1)
Working online also provided a logistical advantage, as the musicians felt that they were not imposing on others in the ward or getting in the way with large instruments: It immediately gets around the problem of . . . us being in situ playing in a ward . . . being in the way of other patients, that maybe actually aren’t that keen on having three musicians turn up and play. So, it sort of immediately took away some of that, and also sort of just playing to one person, actually, especially with something like the [large instrument], which is quite an imposing thing. It sort of took that away as well. Because I feel like if I had three people sort of standing around my bed, actually, I’d be . . . maybe less comfortable than just being able to sort of sit in comfort. (P3)
The fulfillment that the participants described obtaining from the online interactions was reported as being unexpected, and they noted this in clear contrast to their experiences in previous hospital contexts. Online delivery supported the participants to create an intimate musical space with patients, which they experienced through the privacy of headphones. These encounters were perceived as highly impactful: This is the first time that I’ve had really like meaningful musical connections over Zoom . . . I love not interrupting people in their beds, and them being able to have the choice for me that made it really, really enjoyable. (P5)
Connecting and empathizing through music
Forming and valuing connections with patients
The personalized approach taken by the participants was based on building connections with patients through musical interactions. The fulfillment gained from creating these connections became part of the values and habitus of a MiMiC musician. P5 observed that multiple interactions with the same patient strengthened the quality of their connection: The most rewarding in that sense, the lady who returned because she felt comfortable, turned her camera on, which was really amazing. And certainly for longer patients, I think that’s a really lovely idea that you’ve built up this this rapport with someone. (P5)
Participants reported that the ability and willingness of the patients to engage in interaction was another factor that supported them in making connections: [It’s] also, like very different, because of the type of patients that we’re working with, they largely can have really good kind of verbal communication . . . stuff that I’ve done previously has been with, like, very ill patients . . . So in that sense, it’s very different as well. But that was actually really nice, [a] really nice chance to do something where [it was] probably needed just as much as the others. It’s just a really different vibe. And because of that, obviously, as well as what we’re doing, it feels more personal and connected. (P3)
The use of a personalized approach heightened this sense of connection. Discussing baby names and patients’ backgrounds, and creating an anxiety-free environment through conversation, stimulated individualized, intimate experiences. The nature of the improvised music that emerged from these conversations meant that participants saw the interactions as different to everyday performing. In contrast with their previous experiences of behaving as though they were “jukeboxes” (P5), they were able to use a personalized approach to form connections that went beyond the music. Indeed, part of the dispositions that the participants brought to the work was the valuing of such connections with patients. Being the right person for the job required them to be open to the creation of personal connections, respecting and appreciating the significance of the moment for the patients.
Developing connections within the team
It was vital for participants to negotiate connections not only with patients but with the other members of the team. The importance of music for positive impact, for forming relationships, and providing care resonated within the team: To have a group of also all women, to all have the same attitude towards their, their sort of role as an instrumentalist and their role within the industry is really nice. To all have that open-minded “what can I do as an instrumentalist to bring joy to people?” is really positive. (P2)
These values were embedded in the social and musical dynamics of the team. The participants had been trained for individual performance but needed to develop a collective mindset to deliver the musical interactions: It was lovely during the week that we had with the whole team, I think to really feel part of a group and to know that the other sessions are going on in the other weeks, which is great, but that we know everyone has made a difference in terms of the sense of community. Definitely. (P5)
This sense of community in relation to both practice and values was important for the participants and patients alike. The flexibility required for MiMiC improvisation required a high degree of trust and embodied communication among the musicians: “[these settings] come with communication challenges . . . you have to be really honest with the musicians that you’re working with” (P2). In creating team spaces in this way, the participants developed a shared habitus, with the different values of team members coalescing into a shared community of embodied practice.
Being an empathetic musician
Empathy was an important part of the participants’ developing vocational habitus. Building understanding with the patients required the breaking-down of boundaries between the performer and audience, and the scrutiny of mindsets they traditionally associated with performance: I think it’s less to do with perfectionism, and more to do with empathy, and how the audience reacts. I think sometimes, when I’ve been performing in other settings, it’s felt more about how I want to play and less about how the audience takes what I’m playing. It’s more sort of self-serving, sometimes it feels like, I’m playing this beautiful music, and I want to play really well. Whereas definitely in this, there were multiple moments within the different weeks where it felt like, I felt like I played really badly, but actually, the patient was happy. And that’s the main thing. (P2)
As described here, MiMiC required participants to re-consider some of the morals associated (most often in classical music) with the artistic virtue of the piece. To be an effective MiMiC musician, participants were required, rather, to be responsive to the needs and interests of patients, and to let others into their practice and preparation. Excellence was reframed to include being open, empathetic, and adaptable in the musical moment. Representing a perceived shift from some of the traditions of concert performance, participants emphasized the importance of becoming an empathetic player: I think because you’re not, it’s not a concert. In a concert, you just place your audience, and they just listen. But this is more than that. And it’s about in those 10, 20, minutes, however long you have tried to build a bit of a connection, you know, through that music. And if you’re not, if you’re not open to that yourself, then how are you going to build a connection? (P4)
According to the participants, they were required to renegotiate their roles as performers, listeners, facilitators, and improvisers in the context of providing personalized music in a maternity setting. To excel in this space, they needed to continue to develop their understanding of how to engage and connect with other people, empathizing with patients and embodying their empathy in the high-quality music they created.
Communicative and musical versatility
Knowing how to communicate
Central to the success of the musical interactions, all of which took place via Zoom, was clear communication between participants and patients. It was important for participants to learn how to guide conversations about patients’ choices of music. In these conversations they needed to know how to remain flexible and at the same time how not to overwhelm patients with too many options: I think we kind of refined the language where we worked out which ways of explaining it works best or were least confusing . . . Before we’ve been guilty of massively overloading [patients] with too many choices, places, emotions, highs, all of this at once. (P3)
Colley et al. (2003) argue that the development of vocational habitus is not a process of “passive absorption into a community of practice” (p. 488) but involves ongoing adaptations, such as the recognition described by P3. The participants’ reflections on their developing communication styles illustrate the aspects of their habitus that involved social as well as musical labor. The social knowledge they needed to apply in this situation was how to be comfortable with silence, giving space for the patient to respond. This was also linked to their own personal attributes, which they brought to the interactions: I think if you’re comfortable in yourself, then the [patients] are much more comfortable with you. Whereas . . . [if] you’re a bit awkward and nervous, they’re automatically gonna get that, even though it’s over Zoom . . . I think those things do come through. (P4)
Participants’ confidence in these interactions had impacts beyond the ability to mediate social dynamics with patients. A core element of the process of teasing out responses enabling musical connections was creating opportunities for patients to be open. The social skills needed by participants to do this were seen as almost more important than improvisation and technical skill: I think actually, the most important thing is the communication skills. Because especially if you’re working with conservatoire-level musicians, they’re all good enough to do it. It’s about how they communicate, and how they interact and work with the group of people that they’re going to be with . . . I think something that can be learnt, we really saw that, that we all developed that. So actually, in terms of the initial skills that someone needs, I guess they need to be willing to learn and [be] open to exploring a new way of working and sharing music is the most important thing. (P5)
Participants began to recognize the idealized habitus required in MiMiC communication through their experiences: to be sufficiently flexible to coax reflective responses but not so flexible that they offered participants too much choice. In practice, this required participants to develop scripts that guided the start of each interaction with a patient, thus demonstrating realized habitus (Colley et al., 2003).
Becoming a flexible and adaptable musician
Flexibility and adaptability were constantly referred to as requirements in this setting. This included the ability to work with different people, musical genres, and musical roles: I consider myself quite a flexible musician in terms of what I’m happy to play. But things like . . . doing all the different transitions and having to then jump around between things . . . and now instead of just playing the accompaniment part here, you can do the accompaniment and the melody, and you’re also going to that, sort of, filling in what gap needs filling. (P2)
This professional know-how was described as being in tension with some aspects of the musicians’ existing habitus, requiring them to adapt to new musical roles and demands. They valued the opportunity to incorporate flexibility into their skill sets, however, which was appreciated as an element of their developing habitus: I mean, in a selfish way, purely about just being a better musician, I think it makes me a better musician through having to think on my feet and actually be much more flexible, and creative than sometimes I do in a sort of standard recital, concert kind of situation. (P3)
They regarded the integration of these skills into their practice as a way of taking a more expansive approach to music: I mean, yeah, like the [institution] Masters was classical and stuff I did, I used to do quite a lot of jazz. But that was a long time ago. And so that was also quite nice for me to be able to make these two things work . . . it’s just, and it’s so freeing, and I kind of feel like for performing musicians it’s such a great thing to be able to just pick up your instrument and with other people set a few rules, and then just, you know, go . . . So that was super nice. (P4)
Through continuing to develop this form of flexible practice, the participants reported gaining know-how that was relevant not only to MiMiC but also to other professional contexts.
Embracing person-centered improvisation
As highlighted in the sections above, participants needed not only to empathize with patients and their individual circumstances but also to exhibit musical and communicative reflexiveness. The following journal entry encapsulates the weaving of these two factors through person-centered interactions: We couldn’t see [on screen] the second patient today, but she was very chatty, was happy to take part in the music-making and was sharing a lot of personal experiences with us. She did not mind what music we played although she wanted to hear something calm and romantic. We started [some] improvisations based on the patient’s favourite baby names . . . In between the music she was sharing her experiences of loss, insecurity, and worry but also hope and expectation. It was very powerful, and we tried to create music that would reflect the latter. I thought we dealt with the situation well and I hope we left the patient feeling a little calmer and more hopeful. It was an important learning experience for us. (P1)
By positioning themselves as both performers and listeners, the participants were able to create a space in which the patient’s feelings were mirrored in the personalized music. They also noted in their reflections that the presence among them of a singer who incorporated words, including poetry, in the improvisation was particularly useful in helping them respond to the patient’s interests: I think also in terms of feeling like we got what they [patients] wanted, I guess, like if they wanted a seascape, having words that directly correlate to the sea. It’s quite useful . . . it’s almost cheating, but I think also what you were saying about like using little bits of existing music. Yeah. So even if we can be like, there’s little clues in there, but I guess it’s like, not cheating, but something . . . (P2)
The most difficult task for the participants proved to be blending the patients’ experiences and preferences in the music. Throughout the sessions, the participants were navigating between two different dispositions: that of the conservatoire-trained classical musician, whose values may be informed by rehearsing and performing set repertoires, and the flexibility and adaptability required to use repertoire in different and fragmented ways when delivering a personalized, improvisatory music intervention.
Developing a sense of self as a musician
While working on the project, participants reflected on their own values regarding the impact and place of music: “Well for me, hugely, the whole point I share music is to create a sense of community and a bond between not only the singer or the musician and the audience but between the people who are watching” (P5). Part of being the right person for the job was to value and create an environment accessible by everyone. As also discussed above, the relationships formed in this context were, at times, regarded as more important than the performance itself: [It was a] timely reminder of . . . this is the impact music can have. And this is the nice impact, you’re having really positive experiences . . . So that was that was really nice . . . obviously, we liked the music that we were playing, but that was just circumstantial. It was fun to play. But seeing people enjoy it, and like those messages that we received with like, “oh, the baby kicked” and things like that. That’s what brought us the most joy, I think, instead of the performance element. (P2)
As observed by P2 in their reflections, their experiences on the project shaped their own enthusiasm for music. The emotional fulfillment gained from the experience also allowed them to reconnect with the idealized habitus of becoming a musician, and its potential impact (Colley et al., 2003): I just love . . . it sort of, it feels good. It feels good to actually feel like you’re doing something which is connecting with people, and maybe making some kind of positive difference, which you don’t always feel like you’re doing in situations. (P3)
The value of these experiences went further than the skills and professional satisfaction associated with being a musician, as participants focused instead on creating personal, human connections: It just reminds you about actual real life. I think, as I said before getting away from like, musician head . . . It’s about putting the connection first. And the music is then to aid that connection. Rather than music for the sake of music. (P5)
As touched on here by P5, they regarded the project as a way of recognizing and “getting away” from some of the dispositions of having a “musician head.” This meant shifting toward making connections through music rather than prioritizing a musical product per se. For this group, MiMiC involved navigating the interactions between the embodied habitus of (classical) music performance and the embodied vocational habitus of MiMiC, where music is personalized, connective, and impactful for both music maker and listener. Importantly, musical excellence is viewed as essential in both contexts. These values were highly integrated into the work that was required to provide not only an effective MiMiC practice but also the fulfillment experienced by the participants while carrying it out.
Discussion
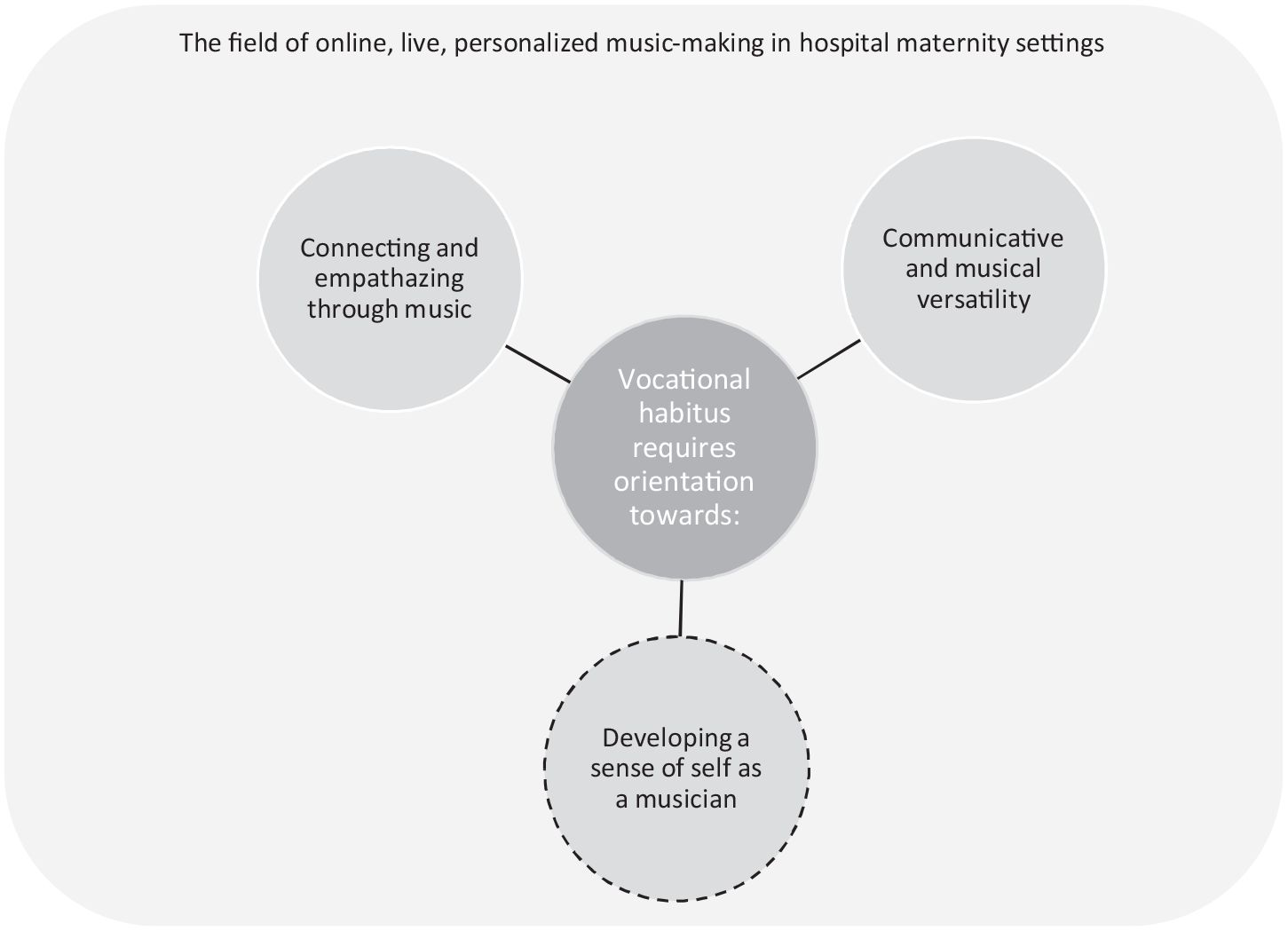
Three aspects of the vocational habitus required to be the right person for the job as a MiMiC musician in the field of live, personalized, online music-making in a maternity hospital setting, as represented by the participants in this study, are drawn together and summarized in Figure 1.
Participants identified the primary skills as the ability to connect and empathize through music and the versatility required to interact meaningfully with patients. Their professional know-how was evident in their accounts of their values associated with prior arts-and-health contexts, and also those they had developed iteratively as they engaged in the MiMiC work. They appeared to have reflected on and developed their sense of self as a musician through their encounters, producing a permeable boundary between their impact on the field and the field’s impact on them, as represented by the dotted line in Figure 1. Vocational habitus for these participants included personal and musical reflections and embodied the values of connection, empathy, and versatility.
The participants’ experiences echoed those of musicians working in wider maternity contexts, including women with postnatal depression (Perkins et al., 2018). The emotional and interpersonal dimensions of the work were again stressed as central to its value, requiring openness to other people’s personal experiences and needs in a way not necessarily demanded by other performing contexts. This can create musical and social vulnerability, which can be both intimidating and freeing. Excellence in this context was seen to require versatility and a responsiveness toward patients and fellow musicians in the moment, where the priority was the musical connection; a point also made by Smilde (2021) who argues that professional performance is about “honest communication through music” (p. 200) with a range of audiences. As shown in this article, the MiMiC musician’s vocational habitus must incorporate a set of embodied skills and values that may also feed into wider creative and health-related work. To develop this habitus, it may be necessary for the musician to nuance their definition of excellence in performance, reframing their understanding of the musical product so as to take into account the needs of individual members of the audience and/or patients. As acknowledged by the participants, developing their practice throughout the project was as much about personal values as it was about adapting their own musical skill sets. Therefore, in order to undertake this kind of work, musicians must be prepared and open to forming new connections, as well as the impacts that this work may have on them (Hume & Parikh, 2022; Musgrave, 2022).
Implications for practice
The findings of this study resonate with those drawn from others’ experiences of personalized practice with people with dementia (Smilde et al., 2014), and in surgical hospital wards (Smilde et al., 2019), among others, suggesting that they may be transferable beyond maternity settings. Participants’ experiences may also offer insights valuable for those supporting the development of professionalism in musicians more widely. While the research reported in this article involved the participation of a small group of conservatoire-trained classical musicians working in one specific context, the findings could be translated to musicians working in other professional contexts such as music educators, facilitators, and community practitioners. The need for them to be versatile, empathetic, and make connections has been shown in research worldwide involving musicians in pediatric hospitals (Tomlinson & Habron, 2021), music practitioners in healthcare settings in Italy (Preti & Welch, 2013), and eldercare hospitals in Finland (Koivisto & Laes, 2022).
The next generation of musicians needs to be supported to fulfill “their societal responsibility and promise as game changers” (Westerlund & Gaunt, 2021, p. xvi). Multiple agents including musicians, training institutions, and healthcare settings share responsibility for this. The educational and professional opportunities afforded to musicians therefore need to respond to this imperative. Responses could be facilitated through revised curricula and assessment processes in music institutions, for example, by creating spaces for music students to explore their versatility and sense of self as a musician, in a culture that prioritizes socially responsible artistry based on musical communication with different groups of people and in diverse settings, including online. In healthcare settings, meaningful and sustainable collaborations between healthcare and arts professionals should continue to be fostered (Smilde et al., 2019), so that musicians can experience professional opportunities enabling them to develop a vocational habitus embodying communicative and musical versatility as well as the ability to connect and empathize through music.
Limitations and future research
This article focuses exclusively on the musicians’ experiences. While this was a deliberate choice, future research exploring how this approach is experienced by those hospitalized during pregnancy will be valuable. Indeed, the wider ProMiMiC research has indicated transformative benefits for both patients and healthcare staff (de Wit, 2021; Smilde et al., 2019) and the relationships between musicians and maternity healthcare professionals could be explored to address the acceptability of the practice in perinatal settings. Another potential limitation of the research was its focus on conservatoire-trained musicians, all of whom identified as women. In future research in this area, it will be important to consider the developing vocational habitus of a wider group of arts practitioners, including those with lived experience. Finally, the ProMiMiC approach detailed in this article could also be expanded to, and investigated with, fathers and partners.
An important consideration during this project and for future work is the potential for music to cause harm. For example, Daykin et al. (2017) remind us of the potential for unintended outcomes and issues of power in music-making, and Belfiore (2022) writes of a duty of care toward artists employed in socially engaged contexts, to avoid harm either to them or those with whom they work. During the research undertaken here, musicians worked in collaboration with the mediator, who was trained and experienced in working safely using arts-based approaches within the hospital setting. Musicians were highly attuned to the needs and preferences of patients, as demanded by the MiMiC training and practices themselves. Indeed, organizations such as CW+ and others provide training for artists embarking on work in health or socially engaged contexts. For the future sustainability of this practice, care should be taken to ensure comparable levels of preparation and support, and research could continue to explore how best to educate musicians (who are not also trained as music therapists) to flourish in these settings.
Conclusion
Overall, our findings illustrate musicians’ adaptations, in multiple ways, to the new online maternity and MiMiC contexts. Participants reflected on their experiences, musical excellence, and performance in health-related settings, highlighting the value of prioritizing the interpersonal dynamics of the interaction alongside a high-quality musical product. As has been reported elsewhere (Perkins et al., 2018), the maternity context was associated with a high degree of emotional significance for the musicians. The online setting was also seen as an unexpected positive factor, removing logistical barriers to musical work in hospital settings and enabling the creation of intimate interactions without distractions. Indeed, it lent meaning to these musical interactions, particularly as they were personalized using the MiMiC approach as part of patient-centered care. While we fully acknowledge the small size of the sample and the context-specific nature of this study, the findings resonate with other recent research highlighting the personal commitment of early career artists to becoming artistic citizens engaged in socially responsible practice (Shaughnessy et al., 2022). The experiences and values detailed in the accounts above also align with Gaunt et al.’s (2021) concept of the musician as a maker in society, presenting personalized music-making in health settings as a forum for musical connection and empathy, communicative and musical versatility, and the development of a sense of a socially oriented musical self.
Footnotes
Acknowledgements
The authors acknowledge and thank the following people who have contributed to and supported the project: Dr Claire Flower, Dr Sunita Sharma, Diana Roberts, Ananya Panwar, Sarah Pugh, René van Munster, the ProMiMiC team and partners led by Prof Rineke Smilde, and the ProMiMiC London musicians, who remain anonymous as research participants but who were fundamental to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was co-funded through the RAAK-Pro programme of Regieorgaan SIA, part of the Dutch Research Council (NWO) and CW+.