
Abstract
Objective:
The prevalence of sexually transmitted infections in Hong Kong is not high. The objective of this study was to determine the risk factors that associated with occurrence of sexually transmitted infections in local sexual assault victims, so as to facilitate the counseling and management of victims upon their initial attendance at an Accident and Emergency Department.
Methods:
This was a retrospective cohort of sexual assault victims presented to Accident and Emergency Department of Kwong Wah Hospital between 1 January 2016 and 31 December 2021. The outcome was the occurrence of sexually transmitted infections. Variables were analyzed using univariate and multivariable analyses.
Results:
A total of 190 victims were included in the study. Univariate analysis indicated that sexual assault involving multiple perpetrator, oral penetration, and anal penetration were associated with increased occurrence of sexually transmitted infections in the victims (all with p < 0.05). Among these, multiple perpetrator was the only statistically significant risk factor on multivariable analysis (p < 0.05).
Conclusion:
Multiple-perpetrator sexual assault was identified as a significant risk factor of sexually transmitted infections. Emergency physicians should consider explaining to victims of multiple-perpetrator sexual assault that they have a higher risk of contracting sexually transmitted infections and emphasizing on the importance of complying with medical treatments, attending follow-up and observing symptoms of sexually transmitted infections. Proper clinical assessment, adequate follow-up, and reassurance for the victims with lower likelihood of contracting sexually transmitted infections are suggested for managing sexual assault victims.
Introduction
Sexually transmitted infections (STIs) and blood-borne viruses can be transmitted during sexual assault. Consequently, victims of sexual assault often attend the Accident and Emergency Department (AED) for fear of acquiring infections.
For some STIs, namely chlamydia, gonorrhea and trichomoniasis, there are prophylactic antimicrobials, whereas in other STIs, such as genital wart and herpes, there is no effective prophylaxis.
The United States Centers for Disease Control and Prevention (CDC) 1 recommended empirical antimicrobials at the initial attendance regardless of sexually transmitted diseases (STD) testing. This recommendation was based on the high prevalence of STIs in the whole community 2 and the low rate of return for follow-up visits among sexual assault survivors. 3 However, the estimated prevalence varies widely depending on the population studied and the known risk factors of STIs. 2
Antimicrobials are not without side effects and they may cause serious allergic reactions. Metronidazole often induces nausea, vomiting, and diarrhea, which may prevent absorption of other orally taken STIs prophylaxis and emergency contraception. Moreover, unnecessary use can contribute to development of resistant strains of infectious organisms.
To facilitate the management and counseling of the victims, risk factors of contracting STIs should be considered. In general, risk factors that may increase the risk of STIs transmission include unprotected intercourse, multiple sexual partners, past history of STIs, being forced to engage in sexual activity, use of alcohol or recreational drugs, and young age. 4
The objectives of this study were to identify risk factors associated with increased occurrence of STIs in sexual assault victims and to investigate whether antimicrobial prophylaxis is associated with reduction of STIs in the victims.
Service protocol for management of victims of sexual assault
AED of Kwong Wah Hospital (KWH) runs a clinic for female victims of sexual assault and has been collaborating with two crisis intervention centers, CEASE Crisis Centre and RainLily, in Hong Kong for many years. RainLily is a non-government charitable organization that aims at providing crisis support, and coordinating different services and procedures to take place in one center for victim of sexual violence. The CEASE Crisis Centre provides crisis intervention and support service, which aims to provide comprehensive support to victims of sexual violence and individuals/families facing domestic violence or in crisis, and to link them with appropriate healthcare and social services units for necessary protection and services.
The clinic provides one-stop service to sexual assault victims including pregnancy prevention, screening and prevention of STIs, medical examination, psychological support, and reporting to the police if desired by the victims. At initial presentation, the victims’ past health, details of the sexual assault, symptoms, and signs are identified by history taking and physical examination. They are screened for HIV, syphilis, hepatitis B, and hepatitis C infections by blood tests. Emergency contraception is prescribed, if indicated. Prophylactic antimicrobials are not universally offered and instead are prescribed according to the clinical judgment of the attending emergency physicians, therefore only some of the victims are prescribed antimicrobials prophylaxis.
In general, the attending emergency physicians will take into account factors such as the use of condoms, the presence of symptoms of STIs, the likelihood of follow-up, the victims’ preference, and so on when considering the prescription of prophylactic antimicrobials. Consistent with the 2015 CDC Guideline, single dose of intramuscular injection of ceftriaxone 250 mg, single dose of oral azithromycin 1 g, and single dose of oral metronidazole 2 g are used, if STI prophylaxis is prescribed.
First follow-up is usually arranged on day 10 to day 14 after the sexual assault. During the follow-up arranged on day 10 to day 14 after the sexual assault, gynecological examination is done and various swabs are taken, namely urethral swab for bacterial culture, high vaginal swab for bacterial culture, and endocervical swabs for bacterial culture and chlamydial polymerase chain reaction (PCR) test. Throat and rectal swabs are also taken, if clinically indicated. For victims who had a late presentation or defaulted the first follow-up on day 10 to day 14, the gynecological examination and tests for STIs would be arranged on the earliest day that the victims can attend our clinic. Subsequent follow-up appointments are arranged at 6 weeks, 3 months, and 6 months after the sexual assault. Victims are monitored and blood tests for screening of syphilis, HIV, hepatitis B, and hepatitis C are done during subsequent follow-up appointments. For victims who defaulted follow-up, our staff will contact either the victim or the social worker in-charge and offer an appointment for follow-up at another time.
Methods
Study design and population
This retrospective cohort study was carried out by collecting data from the records of the sexual assault victims attending the AED of KWH between 1 January 2016 and 31 December 2021. The sexual assault cases were identified from the special case list of the clinic for female victims of sexual assault of AED of KWH. All victims attending the AED within the study period were included unless they met any of the following exclusion criteria: (1) vaginal/endocervical culture swabs were not taken, (2) service was refused by the victim, (3) delayed presentation to AED beyond 28 days after sexual assault, and (4) exact date of sexual assault was unrecalled.
Data collection
Data collection was done by reviewing written medical records in the medical records office and electronic records in Clinical Management System (CMS). CMS is a system used in Hospital Authority for clinical staff to access and make patient clinical records, patient appointments, doctor consultations, and prescriptions. Medical records were reviewed by the principal author. Victims’ demographics, characteristics of the sexual assault, laboratory test results, and outcomes were reviewed.
The STIs of interest in this study were Chlamydia trachomatis, Neisseria gonorrhea, and trichomoniasis as effective prophylaxis was available. Victims were considered to have suffered from STIs if their swabs for culture or PCR test were tested positive for C. trachomatis, N. gonorrhea, or trichomoniasis.
Statistical analysis
Data were analyzed by MedCalc software Version 20.100. The chi-square test or Fisher’s exact test was used to compare the statistical significance between categorical variables. Fisher’s exact test was used when one or more cells in the table was less than or equal to five, otherwise chi-square test will be used. Multivariable logistic regression was performed on the significant factors with p-value < 0.005 identified in the univariate analysis. Sample size calculation was not done as this was a pilot study.
Results
Characteristics of victims
There was a total of 259 cases presented to AED of KWH from January 2016 to December 2021. Sixty-nine cases were excluded based on the exclusion criteria. A total of 190 cases were included in the final analysis (see Figure 1). The age of victims ranged from 14 to 54 years. The median age was 27 years. Forty victims (21.1%) had history of psychiatric illnesses (mental and behavioral disorder diagnosed by ICD-10 codes). Eighteen out of 190 victims (9.5%) were subsequently found to have contracted STIs after sexual assault.
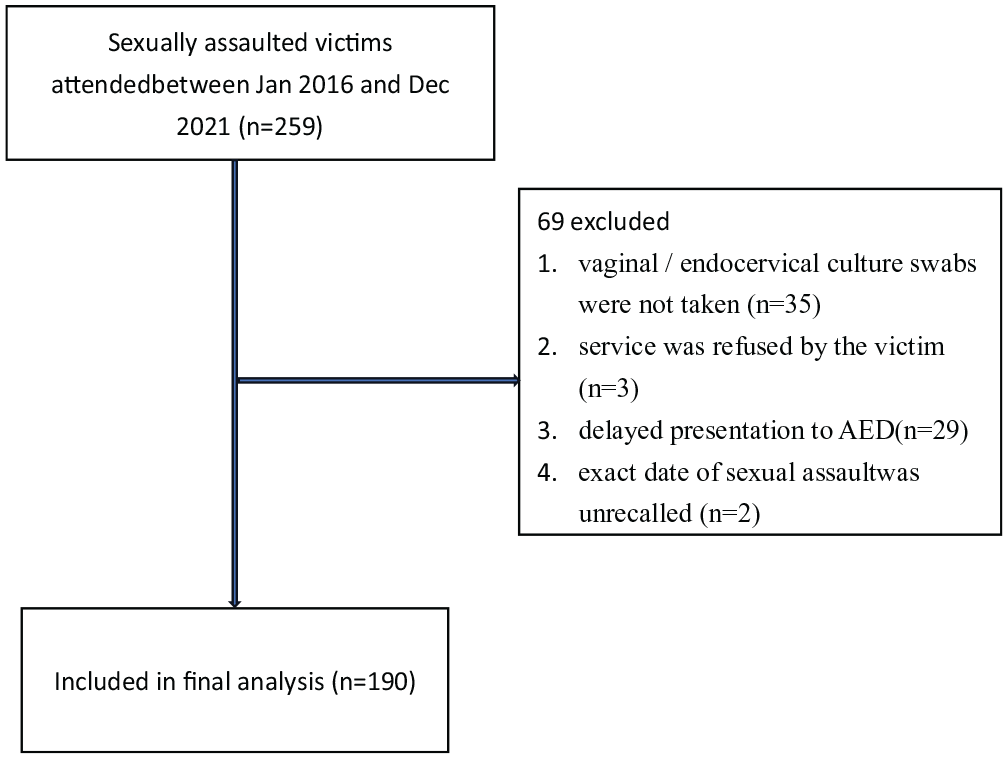
Enrollment flow diagram.
Table 1 summarized the characteristics of the sexual assault victims included in this study. The median time lapse between the day of the sexual assault and the day of presentation was 3 days. Among the 190 victims, 112 (58.9%) assailants were their friends or acquaintances, 36 (18.9%) were strangers, and the remaining 42 (22.1%) were not documented. There were 177 victims (93.2%) being sexually assaulted by one man, whereas 13 victims (6.8%) were sexually assaulted by more than one man.
Characteristics of victims and the results of statistical analysis related to STIs.
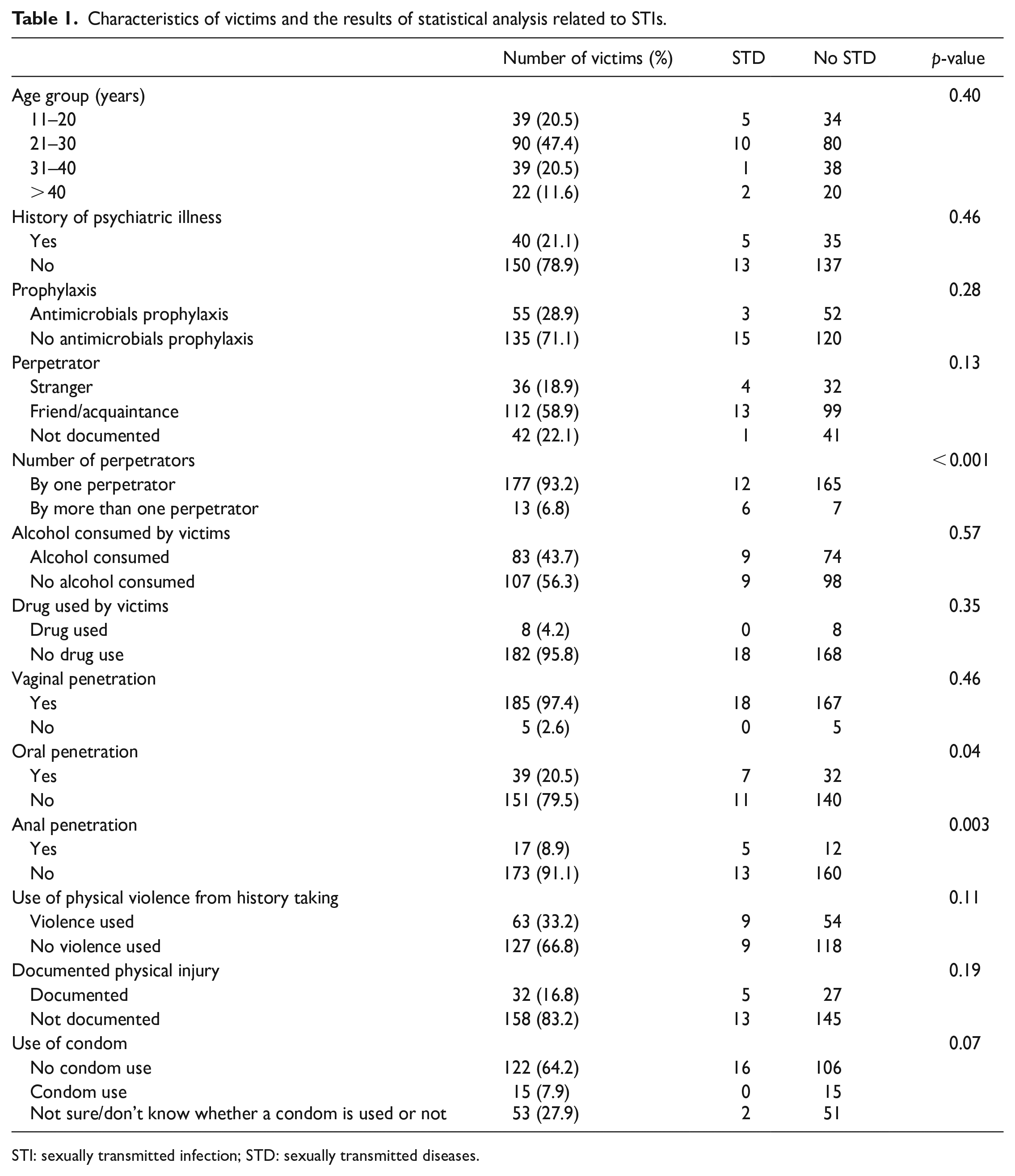
STI: sexually transmitted infection; STD: sexually transmitted diseases.
Eighty-three victims (43.7%) consumed alcohol and 8 (4.2%) used drugs. Our service protocol did not include a toxicological testing, and therefore victims were not routinely tested. For victims with toxicological tests performed, the drugs identified included gamma-hydroxybutyrate, clonazepam, and mirtazapine.
Some victims were sexually assaulted by more than one way of penetration. A total of 185 victims (97.4%) reported vaginal penetration, 39 victims (20.5%) reported oral penetration, and 17 (8.9%) victims reported anal penetration. There were 32 documented cases of victims (16.8%) who suffered physical injuries during the sexual assault. The physical injuries included abrasions, bruises, cut wounds, erythema, and tenderness. Of the 32 documented cases, 4 victims had injuries around the genital area, namely abrasions, anal fissure, vulval erythema and swelling. None of the victims needed in-patient management as a consequence of their physical injuries. More than half of the cases (122 cases, 64.2%) were sexually assaulted without a condom and the remaining 15 cases (7.9%) reported condom use. Fifty-three (27.9%) victims were unsure about whether a condom was used or not.
Among the 190 victims, 108 of them informed the police of their cases while 82 of them did not do so. Most victims turned up for follow-up at 2 weeks (95.3%) and at 6 weeks (83.7%).
Antimicrobial prophylaxis versus no antimicrobials prophylaxis
We investigated the STIs, namely C. trachomatis, N. gonorrhea, and trichomoniasism, which can be treated by prophylactic antimicrobials. They were diagnosed by positive culture or PCR results of the swabs (urethral swab, high vaginal swab, endocervical swab, throat swab, and rectal swab) during the gynecological examination, which was usually arranged approximately 2 weeks after the sexual assault. We identified 18 victims with positive culture results, of which 16 victims were infected with C. trachomatis, 1 victim had N. gonorrhea infection, and 1 victim had trichomoniasis.
Upon the initial presentation after their sexual assault, 55 victims were prescribed prophylactic antimicrobials and the remaining 135 victims were not. Of the 55 victims who were given prophylactic antimicrobials, 3 victims had positive cultures during their follow-up. Of the 135 victims who were not given prophylactic antimicrobials, 15 victims had positive cultures during their follow-up. The p-value of the association between prescription of antimicrobials prophylaxis and presence of STIs was 0.28, which was statistically insignificant. For victims who were given prophylactic antimicrobials, none of them reported significant side-effects or adverse effects during follow-up.
Risk factors associated with STIs
In the univariate analysis, sexual assault involving more than one perpetrator, with oral penetration, and anal penetration were significantly associated with the occurrence of STIs. The p-value, odds ratio, and 95% confidence interval (95% CI) were as shown in Table 2.
Univariate analysis and multivariate regression model—odds ratio with 95% CI.
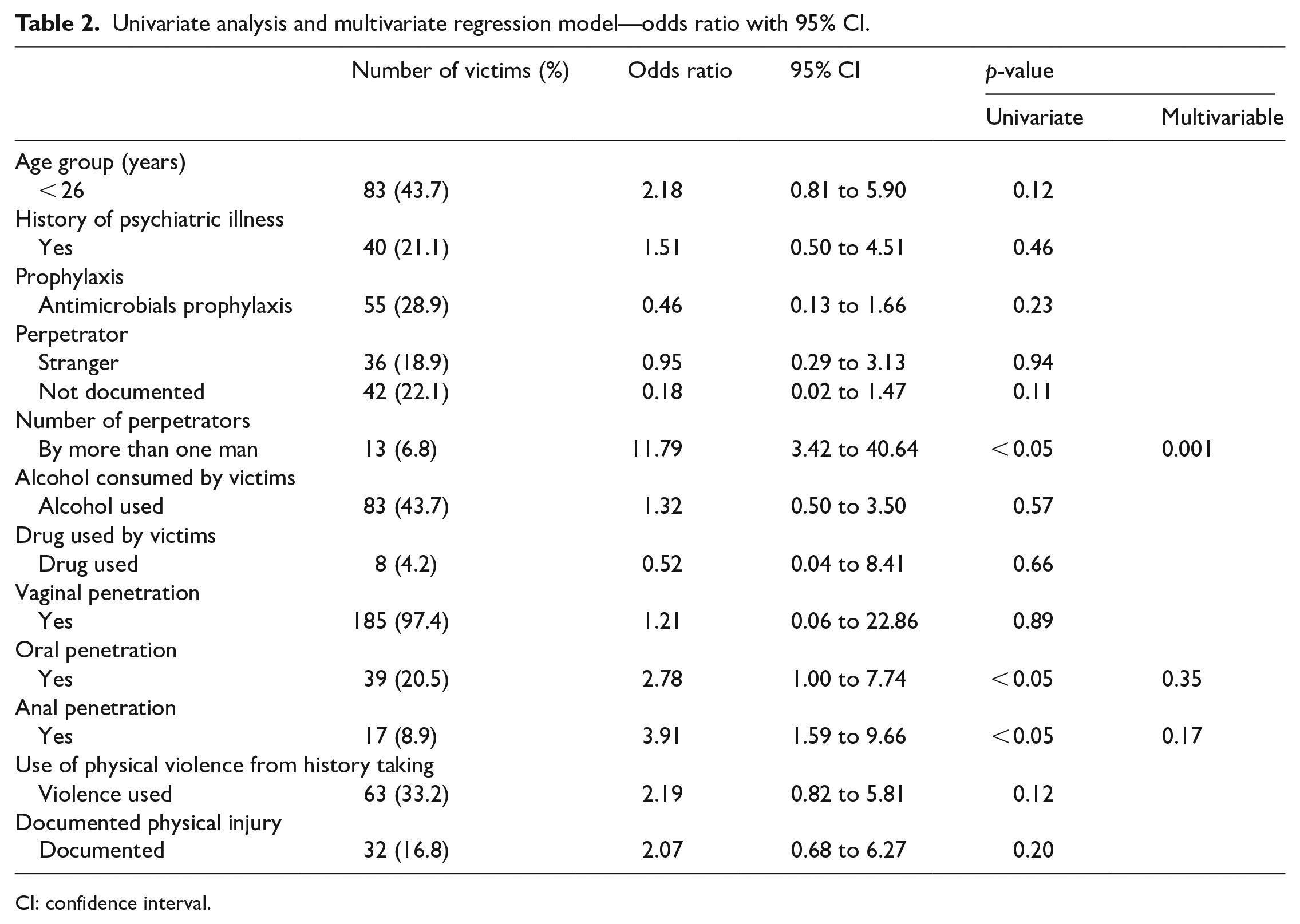
CI: confidence interval.
The multivariable logistic regression showed that only sexual assault involving more than one perpetrator remained statistically significant. The odds ratio was 13 with 95% CI 3.42 to 40.64.
Emergency contraception for sexual assault victims
Emergency contraception was given to 138 victims (72.6%), of which 135 victims (71.1%) were prescribed levonorgestrel or other hormonal drugs. Intra-uterine contraceptive device (IUCD) was used in three of the victims (1.6%). Fifty-two victims (27.4%) were not prescribed emergency contraception as they presented outside the therapeutic window.
Four victims became pregnant as a result of their sexual assault whereas two of which were given oral contraceptives and the remaining two were outside the therapeutic window for any form of contraception. Of these four cases, two victims underwent termination of pregnancy.
Discussion
Risk factors
In our study, multiple perpetrator was associated with the occurrence of STIs based on both univariate analysis (p < 0.05) and multivariable analysis (p < 0.05). Thirteen victims reported multiple-perpetrator sexual assault, of which 6 out of 13 victims (46.2%) contracted STIs. This result was statistically significant (p < 0.001), showing that the risk of a victim acquiring STIs appeared to be greater in a multiple-perpetrator sexual assault case. It could be explained that when a victim was being sexually assaulted by more than one perpetrator, the victim could be viewed as suffering from multiple assaults in one incident, and as such the cumulative risk of contracting STIs would be increased. It could also be presumed that the likelihood of these perpetrators being engaged in risky sexual behavior would expose them to higher risk of contracting STIs, and thus victims in multiple-perpetrator sexual assault suffered a higher risk of contracting STIs. Nonetheless, research that attempted to identify the risk of acquiring STIs in relation to multiple-perpetrator sexual assault is limited.
Prophylactic antimicrobials
Our study did not show statistically significant beneficial effects of prophylactic antimicrobials on preventing STIs. A possible explanation could be the small sample size. According to a study published in 2021, the overall prevalence of the composite sexually transmitted diseases in Hong Kong was 1.9% only, with 1.2% for men and 2.5% for women. 5 The global prevalence of STIs was 4.5% among men and 10.5% among women, 6 which was much higher compared to the figures in Hong Kong. Therefore, the chance of contracting STIs in Hong Kong after sexual assault might be lower. Having considered the low STIs prevalence locally in Hong Kong, a much larger sample size would be required in order to reach statistical significance in this regard.
Prophylactic antimicrobials were recommended during the initial evaluation by different guidelines due to the low rate of return for follow-up. A retrospective study by Gavril et al. 3 found that less than half (48.8%) of sexually assaulted victims returned for a follow-up evaluation. On the contrary, we achieved a higher follow-up rate in our clinic. In our study, 95.3% of victims returned for follow-up about 2 weeks after the sexual assault. This high follow-up rate is likely due to the efforts of the two intervention centers, namely CEASE Crisis and RainLily, who assisted in victims’ follow-up arrangement and reminding the victims the importance of attending the follow-up appointments. Based on this finding, as the antimicrobials treatment for bacterial STIs are extremely effective for both symptomatic and asymptomatic patients, 7 a conservative approach to treat victims who develop symptoms and signs of STIs or with positive culture results of STIs during subsequent follow-up is a reasonable alternative. Prophylactic antimicrobials should be offered to victims who are not likely to attend follow-up and for those who are in distress because of fear of STIs. From Table 1, among the 18 patients who were found to have STIs, 16 were sexually assaulted without the use of condoms. Emergency physicians should consider prescribing prophylactic antimicrobials to victims who are assaulted without the use of condoms, especially those who may likely default follow-up.
It is noteworthy that of the 52 victims being prescribed with prophylactic antimicrobials upon their initial attendance at AED of KWH, three were found to have contracted STIs in their subsequent follow-up. Thus, emergency physicians should emphasize the importance of follow-up given that there is still the possibility of contracting STIs after the prescription of antimicrobials.
Condom
Condom is known to reduce the transmission of STIs. 8 Of the 190 cases, condoms were used in 15 sexual assault cases of our study (7.9%). None of these victims were found to have STIs. Our result showed that the use of condoms in a sexual assault is less likely to result in STIs in victims. Unfortunately, due to small sample size and the fact that 53 (27.9%) victims were unsure of the use of condoms during the sexual assault, the expected difference were not statistically significant on multivariable analysis (p = 0.06).
O’Neal et al. 9 found the prevalence of condom used in sexual assault ranged from 11.7% to 15.6%. From our result, condoms were used in 7.9% of our cases. Sexual contact without condom increased the risk of contracting STIs and unwanted pregnancy for victims. These two complications would certainly cause additional stress to the victims. Doctors should be aware that condom use is not common at all in sexual assault cases. More efforts should be done to encourage the sexual assault victims to seek help from healthcare professionals in a timely manner for emergency contraception and management of STIs.
Other management aspects
Most sexual assault victims were reluctant to disclose the sexual assault to their friends and relatives, or to the authorities. In our study, 56.8% victims reported to the police, which was similar to the rate reported in a large epidemiological study in the United States. 10 The under-reporting of sexual assault to police resulted in failure of the police to apprehend, convict, and sentence the perpetrators. Ruch et al. 11 and Maria Hansen et al. 12 summarized the barriers for the victims to report the sexual assault to the police. Reporting rates had decreased because (1) some victims attributed a high level of blame to herself for the assault, (2) the sexual assault was non-violent, and (3) they were assaulted by someone they knew. Non-reporting victims showed higher levels of disrupted personal lifestyle, denial and rationalization of the sexual assault, searching for meanings of the assault, self-blame, and social isolation. We should encourage the victims to inform the police because underreporting of sexual assault will have negative impact on the potential apprehension, arrest, and conviction of violent sexual offenders. Nevertheless, if they decide not to inform the police, we should still respect their decisions and be supportive.
Sexual assault can result in severe physical and psychological to the victims. Although our study focused on the physical management and risk factors of STIs in sexually assaulted victims, emergency physicians should attend to the psychological and emotional needs of the victims of sexual assault.
Limitations
There were several limitations in our study.
First, the sample size was small, in particular the number of victims contracting STIs. Even though AED of KWH has been collaborating with two crisis intervention centers, that is, CEASE Crisis and RainLily, for management of sexually assaulted victims, only 259 cases were presented to our hospital from 2016 to 2021. Consequently, our study was conducted based on a small sample size, thereby affecting the reliability of the outcome statistically.
Second, this was a retrospective study, the completeness of information depended on the documentation. For example, in our study, the ethnicity of the victim and the victim’s sexual behavior could not be identified from the record while they might have an effect on the types of sexual assault and hence the chance of contracting STIs. Moreover, the use of condom was not known in 53 cases (27.9%). This may be due to the retrospective design of our study, and maybe explained by some of the victims being under the influence of alcohol or drugs during the assault. A total of 83 victims (43.7%) reported consumption of alcohol whereas 8 victims (4.2%) reported use of drugs. Their consciousness level might be impaired, and therefore they could not ascertain whether a condom was used or not.
Third, we could not exclude the possibilities that some of the STIs detected was unrelated to the sexual assault. Some of the victims might suffer from preexisting STIs before the sexual assault. This might affect the result of our study. We could not confirm that the STIs detected in our study were the direct result of the sexual assault.
Finally, this study did not include all the possible STIs resulting from sexual assault. The results of this study can only be applied to C. trachomatis, N. gonorrhea, and trichomonas infection.
Conclusion
Our study showed that multiple-perpetrator sexual assault was associated with a higher risk of contracting STIs. When managing victims of multiple-perpetrator sexual assault, it is suggested that emergency physicians should explain to these victims that they are exposed to a higher risk of contracting STIs, and thus it is important for them to comply with medical treatments, attend follow-up, and observe for symptoms of STIs.
Footnotes
Acknowledgements
The authors would like to thank the Clinical Research Centre, KWH for their biostatistics support to the study.
Authorship
The listed authors had participated sufficiently in the work of designing and conceptualizing the study, analyzing the data, and drafting the article and/or revising it critically for important intellectual content. All authors approved the article to be published. All authors participated sufficiently in the work to take public responsibility for appropriate portions of the content. The authors had full access to all the data in this study and would take complete responsibility for the integrity of the data and accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data for this study are available for from the corresponding author.
Informed consent
Written informed consent was not necessary because no patient data have been included in the article. Waive of informed consent was approved by the Research Ethics Committee (Kowloon Central/Kowloon East) of Hospital Authority.
Ethical approval
This study was approved by Research Ethics Committee (Kowloon Central/Kowloon East) of Hospital Authority on 12 January 2023 (Reference no. KC/KE-21-0161/ER-3).
Human rights
There were no human rights conflicts to declare.