
Abstract
Introduction:
Activated charcoal is administered through a nasogastric tube to some poisoned patients, but occasionally the insertion of unweighted nasogastric tube fails in the emergency department. Weighted nasogastric tube with a stylet, for example, the Corflo® nasogastric tube, facilitates insertion, but it is not clear whether it would impede activated charcoal delivery. We aimed to compare the utility of the Corflo® and usual (Comforsoft®) nasogastric tubes in administering activated charcoal in manikins.
Method:
This was a single-centre, randomised, single-blinded, crossover manikin non-inferiority trial involving 28 participants. Each participant administered 50 g of activated charcoal using the Corflo® and Comforsoft® nasogastric tubes in a random sequence interspersed with a 2-hour washout period. We compared the difference in the time required for activated charcoal administration with a pre-defined non-inferiority margin of 300 seconds and the perceived level of effort between the two nasogastric tubes.
Results:
The mean time for administering 50 g of activated charcoal through the Comforsoft® and the Corflo® nasogastric tube were 87.1 s and 301.6 s, respectively. The mean difference of 203.2 s (95% confidence interval: 147.5–258.9, p < 0.001) was within the non-inferiority margin. The perceived level of effort was significantly higher with the Corflo® nasogastric tube (mean effort score 7.0 vs 1.4, p < 0.001).
Conclusion:
Our study provides experimental data to support the use of the Corflo® nasogastric tube as a non-inferior alternative to the usual nasogastric tube in administering activated charcoal to poisoned emergency department patients. More studies are warranted to verify the findings and optimise the settings for AC administration.
Introduction
Activated charcoal (AC) is the commonest method of gastrointestinal decontamination in acute poisoning.1–6 In 2019, 15% of the poisoned cases recorded in the Hong Kong Poison Information Centre required single-dose AC. 7 The efficacy of AC is time-dependent, and it should be given within 1 hour of poison exposure.1 –4 Poisoned patients who are unconscious and for whom AC is indicated require AC delivery through a nasogastric tube after airway protection. In Hong Kong, the unweighted Comforsoft® nasogastric tube without a stylet, generally known as Ryle’s tube locally, is most frequently used in emergency departments (EDs). However, insertion of Ryle’s tube may occasionally fail in the ED, leading to a significant delay in administering AC.
Weighted nasogastric tube with a stylet, for example, the Corflo® nasogastric feeding tube (Avanos, Georgia, USA), facilitates insertion with the stylet, making insertion faster and easier in emergency situations. 8 Unlike the polyvinyl chloride (PVC) Ryle’s tubes, the Corflo® nasogastric tube is made of polyurethane, making it more resistant to abrasion, chemical, oil and pressure.9,10 It also offers a larger lumen than PVC tubes and Silicone tubes of the same size. 11 These qualities make the Corflo® nasogastric tube a potential alternative when insertion of Ryle’s tube fails in emergencies, especially in intubated patients for whom insertion of the unweighted Ryle’s tube may be more difficult. Such an approach has already been adopted in many local intensive care units (ICUs), but it is not yet widely used in local EDs. Currently, the weighted 8 Fr. Corflo®nasogastric tubes are the only available weighted feeding tube with a stylet in the Hospital Authority (HA), and it is narrower than most Ryle’s tubes available in the ED. It is unclear whether AC can be administered through the Corflo® nasogastric tube without significant delay or clogging.
In this study, we aimed to demonstrate the non-inferiority of the Fr. 8 Corflo®nasogastric tube to the commonly used Ryle’s tube in terms of time for administering 50 g of AC to a manikin. If non-inferiority of the Corflo® nasogastric tube to Ryle’s tube is demonstrated, it may be considered as an alternative when Ryle’s tube insertion fails in poisoned patients in the ED for whom AC is indicated.
Methods
Study design
It was a single-centre, randomised, single-blinded, cross-over manikin non-inferiority trial conducted in the Accident & Emergency Department of Queen Mary Hospital (QMH). The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (CRER No.: HKWC-2022-292; IRB Reference No.: UW 23-007). We followed the Reporting of non-inferiority and equivalence randomised trials: extension of the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement in reporting this study. 12
We compared the time required to administer a single dose of 50 g AC through the 8 Fr. Corflo® nasogastric feeding tube and that for the standard 16 Fr. Ryle’s tube (Comforsoft® nasogastric tube, Symphon Medical Technology Co. Ltd., New Taipei City, Taiwan). The 16 Fr. Ryle’s tube is the one with the largest internal diameter in the ED in QMH and most ED nurses would pick for administering AC, based on a staff poll. Therefore, it was chosen as the standard method for administering AC for comparison in this study.
Two identical manikins (3B Scientific® Patient Care Manikin PRO, Efficiency Medical Products Co., Ltd/3B Scientific GmbH, Germany) were used to simulate a drug overdose situation when the patient was unconscious and for whom AC through a nasogastric tube was indicated. The manikins have simulated oesophagus and stomach, and they are routinely used in training nursing students to perform nasogastric tube insertion. The manikins were positioned in a semi-recumbent position. A Corflo®nasogastric tube, 8 Fr., 43 inches in length, connected to a 50-mL Luer lock syringe was inserted to one manikin and a Comforsoft® nasogastric tube, 16 Fr., 125 cm in length, connected to a 50-mL Luer lock syringe via an adaptor was insert to another. A bottle was put under the distal end of each feeding tube to receive the administered AC. The feeding tubes and AC collected in the bottles were reused.
A bottle of 50 g of AC (Toxicarb®, SERB/Société d’Étude et de Recherche Biologique, Paris, France) has a volume of 250 mL. Despite shaking before use according to the drug insert, it is not uncommon to see precipitates deposited at the bottom of the bottle. In daily practice, it is a common local practice to dissolve all precipitated AC in water before use in many medical wards and ICUs to ensure all 50 g of AC is given. Some overseas centres have protocols of dilution of AC with sodium chloride before use to prevent emesis of stomach content following bolus administration. 13 In this study, we poured the whole bottle of AC into another bottle and mixed it with 50 mL of water to dissolve all the precipitates before use, constituting to a total volume of 300 mL. After each administration, we measured the volume of the collected AC and replenished with spare AC and water mixture at the same ratio to keep the total volume at 300 mL before re-use.
Participants
ED doctors and nurses in QMH were eligible and invited through open invitation to participate in the study. We included both doctors and nurses since AC is administered by either doctors or nurses in the resuscitation room of our department. Participation was voluntary, and all participants gave a written informed consent at enrolment which included that their anonymised information to be published in this article. Each participant was asked to administer the prepared AC mixture through the feeding tube by strictly following the procedure below:
Remove the plunger from the syringe;
Pour AC into the syringe while holding it upright;
Reapply the plunger to the syringe;
Push the plunger to administer AC from the syringe through the feeding tube.
The above 4 steps were repeated until the entire 300 mL of AC was administered. Each participant needed to administer AC twice: one attempt with the Corflo® nasogastric tube and the other through the standard Ryle’s tube. As a token of appreciation, each participant was given a $50 supermarket coupon after completion of the study.
Randomisation, allocation concealment and blinding
Block randomisation was performed with a block size of 4 generated by an online block randomisation generator (sealedenvelope.com). Participants were randomised into two groups: Group A, in which the participants were instructed to administer AC through the Ryle’s tube first, followed by the Corflo® nasogastric tube; Group B, in which the sequence of feeding tube use was reversed (Figure 1). The two attempts were spaced at least 2 hours apart to allow a wash-out period, which aimed to minimise the carry-over effect and exhaustion of participants after the first attempt. Allocation concealment was achieved by using sequentially numbered opaque envelopes prepared by a research assistant who was not involved in the study design and data analysis. Once the envelopes were opened, the participants could not change their group assignment. To blind the participants, the exposed portions of the feeding tubes were wrapped with foil. It was, however, not possible to blind the timer.

CONSORT flow diagram.
Outcome measures
The primary outcome was the time for administering 50 g of AC in seconds, counted from the moment when the participant started to pour AC into the syringe until all AC in the bottle was administered. A research assistant, who was not involved in the study design and data analysis, timed the whole procedure using two timers of an identical brand. An average value was taken if the time recorded by the two timers differed. Secondary outcomes included the perceived level of effort of administration rated by each participant immediately after each attempt using a numerical scale from 0 (with no effort) to 10 (with maximal effort), incidence of tube clogging and broken feeding tube.
Statistical analysis
Prior to the full-scale study, a pilot cross-over study that involved 5 participants was conducted by the first author, in which 3 participants administered AC through Ryle’s tube first and the other 2 used the Corflo® nasogastric tube first. Randomisation and wash-out period were not applied in the pilot study. The intraclass correlation coefficient was 0.4 in the pilot study. We then calculated the sample size based on the method published by Lui. 14 Based on the calculation for two-factor analysis of variance (ANOVA) without replication, the required sample size was 27 at alpha of 0.05 and power of 80%.
The non-inferiority margin was set at 5 minutes (300 s). Healthy volunteer studies showed that the maximum reduction in adsorption of toxic substances was observed when AC was administered within the first hour of ingestion.6,15 Some studies have shown that AC can be effective up to 4 hours after ingestion, but efficacy decreases over time.15,16 One review suggests AC be given for timed-release preparations up to 6 hours after the ingestion. 17 We therefore considered 5 minutes as an acceptable non-inferiority margin because such a delay would be negligible in affecting poison adsorption and patient outcome.
We analysed the difference in time required to administer 50 g of AC with the Corflo® nasogastric tube and Ryle’s tube as per protocol. We tested for non-inferiority by comparing the upper boundary of the 95% confidence interval (CI) of the difference between the times used with both feeding tubes with the pre-defined non-inferiority margin of 300 s. We used Welch Two Sample t-test for data analysis and utilised a generalised linear additive model to identify any potential carry-over effect or interactions between the sequences and the tubes used. We also compared the perceived level of effort of administration using the Mann–Whitney U Test. Microsoft Excel version 2017, Statistical Package for the Social Sciences for Windows version 29.0 and RStudio were used for data analysis.
Results
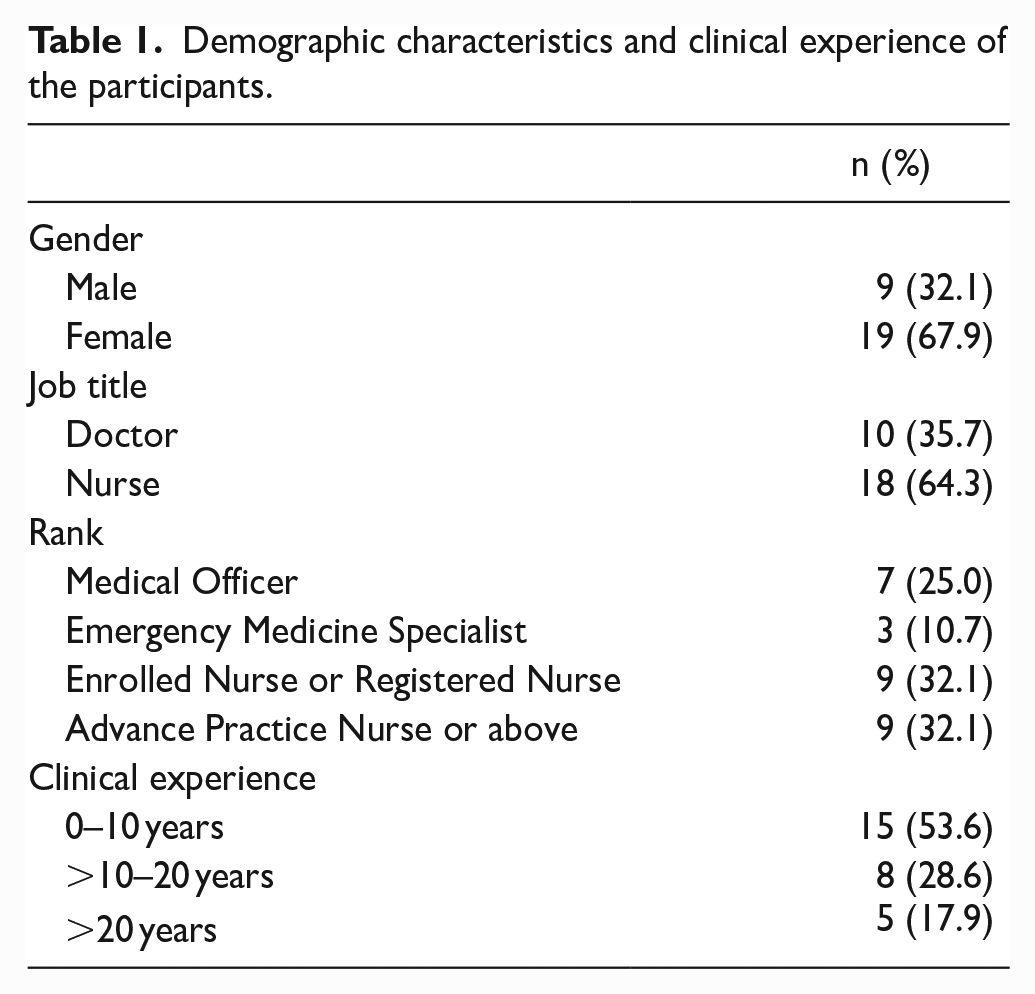
In total, 28 participants, including 10 doctors and 18 nurses, performed 56 administration of AC. More than half of the participants (67.9%) were female and nurses (64.3%). The demographic characteristics and clinical experience of the participants are summarised in Table 1.
Demographic characteristics and clinical experience of the participants.
The mean time for administering 50 g of AC through Ryle’s tube and the Corflo® nasogastric tube were 87.1 s (95% CI: 79.1–95.1) and 301.6 s (95% CI: 262.6–340.5), respectively (Table 2) (p < 0.001). The use of Corflo® nasogastric tube led to a longer time for AC administration with a mean difference of 203.2 s (95% CI: 147.5–258.9, p < 0.001). Based on the generalised linear additive model, there was no statistically significant carry-over effect or interaction between the sequences of the tubes used (p = 0.58) (Table 3). According to the pre-defined non-inferiority margin of 300 s, the non-inferiority of Corflo® nasogastric tube was established (Figure 2).
Comparison of the primary and secondary outcomes between two feeding tubes.

CI: confidence interval.
Welch Two sample t-test was carried out for time for application of activated charcoal. Mann–Whitney U Test was carried out for perceived levels of effort from participants.
General linear addictive model with interaction.

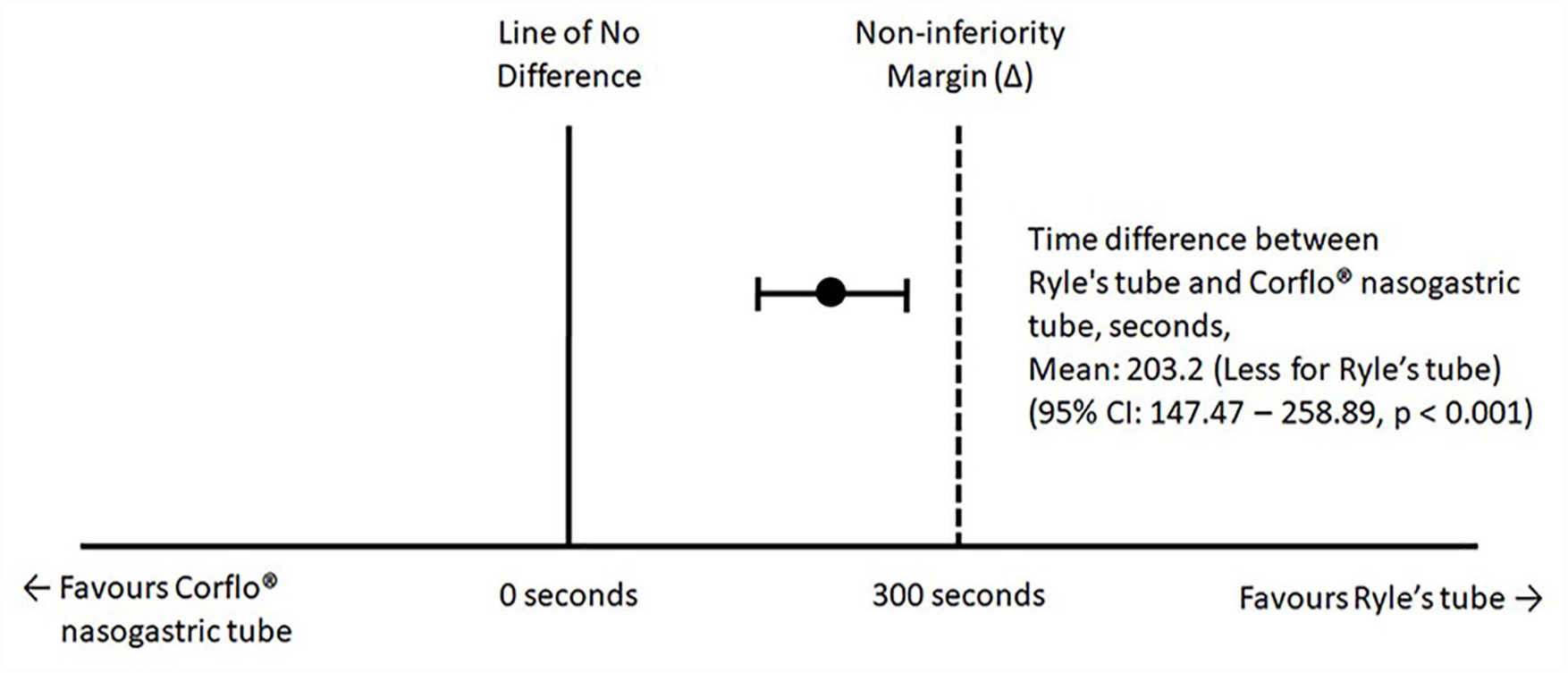
Non-inferiority trial forest plot.
The perceived level of effort was higher with the Corflo® nasogastric tube (mean effort score 7.0, 95% CI: 6.3–7.6) compared with Ryle’s tube (mean effort score 1.4, 95% CI: 0.9–91., p < 0.001) as depicted in Figure 3. We observed no clogging or breaking of any tubes during the study.

Bar chart for perceived level of effort.
Discussion
Drug overdose is a common ED presentation and AC is a widely adopted method of gastrointestinal decontamination.1 –6,17 AC adsorbs and retains substances in the gastrointestinal tract, minimising the systemic absorption of poisons to reduce systemic toxicity.4 –6 It is imperative to administer AC as soon as possible, best within 1 hour of oral exposure to the poison, as its effectiveness decreases over time. 4 Multi-dose activated charcoal, MDAC, is indicated for intoxications with agents that persist for a longer time in the stomach and with timed-release drugs or drugs with a marked entero-hepatic or entero-enteric circulation 17 by enhancing gastrointestinal elimination known as ‘gastrointestinal dialysis’.10,18 The American Academy of Clinical Toxicology and the European Association of Poisons Centres and Clinical Toxicologists recommended MDAC for life-threatening intoxication of carbamazepine, dapsone, phenobarbital, quinine, or theophylline, and believe this could avoid invasive extracorporeal treatment. 2
In the ED, intoxicated patients occasionally require nasogastric tubes for administration of AC, for example, patients with an altered mental state. When gastric lavage is indicated, AC can be given after gastric lavage using the lavage tube. However, when gastric lavage is not indicated, insertion of a nasogastric tube will be needed for the administration of AC or MDAC. Moreover, one of the major side effects of MDAC is nausea or emesis, which could be improved by administration through a nasogastric tube.2,19 However, it is well reported in the literature that insertion of nasogastric tubes in unconscious and intubated patients may be difficult, with the first-attempt success ranging from 34% to 56%.20,21 There is a lack of relevant studies on poisoned patients regarding the failure rate of nasogastric tube insertion. When Ryle’s tube insertion fails in the ED, it is important to identify an alternative way to administer AC promptly without causing a significant delay. Previous randomised controlled trials on anaesthetised and intubated patients showed that the success rate of nasogastric tube insertion was higher with oesophageal guidewire compared with usual method of insertion and the incidence of kinking, coiling and injuries to the aerodigestive tract was lower.20,21 It is, therefore, reasonable to believe that the insertion of a nasogastric tube with an internal guidewire or stylet (e.g. Corflo® nasogastric tube) can be considered as an alternative for AC administration when insertion of Ryle’s tube fails.
Our study showed that the Corflo® nasogastric tube was non-inferior to the Ryle’s tube in terms of the time required to administer 50 g of AC with a pre-defined clinically insignificant difference of 300 s. The upper bound of the 95% CI surrounding this difference was 259 s. The longer time recorded with the Corflo® nasogastric tube could be partly explained by its smaller internal diameter compared with the Ryle’s tube we chose for comparison. Earlier study on flow rate of nutrient preparations through nasogastric tubes has shown that the flow rate is inversely proportional to the fluid viscosity but proportional to the internal diameter of the nasogastric tube. However, the relationship between the internal diameter of the nasogastric tube and flow rate was not linear. The presence of side holes at the end of the nasogastric tube makes no difference to the flow rate. 22 Corflo® nasogastric tube with a larger internal diameter might have resulted in a shorter time for administration. To have a fair comparison, nasogastric tubes of a comparable internal diameter should have been used. However, the 8 Fr. Corflo® nasogastric tube is the only model that is currently available in the HA. Yet, even a smaller internal diameter compared with the Ryle’s tube, we were able to demonstrate its non-inferiority in terms of time for administering AC, thus it can serve as a non-inferior alternative to Ryle’s tube when Ryle’s tube insertion fails.
Although we did not observe any breaking or clogging of the feeding tubes throughout the study, the participants generally made a significantly greater effort when administering AC through the Corflo® nasogastric tube. It is likely due to the larger inner diameter of the 16 Fr. Ryle’s tube we chose as the standard treatment that required a lower pushing force on the plunger in administering AC through the tube. Our study also confirmed that mixing 50 g of AC with 50 mL of water is an effective way to avoid tube clogging during administration through a narrow nasogastric tube as we did not observe any tube clogging or breaking throughout the study.
To our knowledge, this is the first randomised cross-over manikin study to compare the time required for administration of AC through different feeding tubes and to evaluate the perceived level of effort from healthcare workers. There is no previous data available for comparison. It warrants further clinical study to confirm the findings, to optimise the settings of different nasogastric tubes (including the best internal diameter) and to identify problems that may arise for emergency administration of AC in the ED. In particular, a longer time of administration and a higher staff perceived effort might affect staff compliance in real clinical practice. There is a need to optimise the settings of weighted nasogastric tube, such as choosing tubes with a larger lumen, to further shorten time for AC administration and reduce staff effort.
This study has several limitations. First, it was a manikin study. A manikin cannot totally reproduce the clinical condition of real patients. Confounding variables, such as patient’s different oropharyngeal and oesophageal anatomies and pathologies, presence of different amount and types of stomach contents, and individual tolerance to nasogastric tube insertion and feeding are all present in real patients but not in manikins. We tried to mitigate this problem by using manikins that are specifically used for nasogastric tube training.
Second, we are not certain whether repeated use of the feeding tubes would have affected the measured time for AC administration. Factors such as wear and tear of the feeding tubes after repeated use and residual charcoal deposited in the tubing might slow down the flow rate of AC. The research team did not have enough budgets to purchase a new Corflo® nasogastric tube for each participant. We did not wash the tubes in-between use because that would otherwise require repeated removal and reinsertion of the nasogastric tubes from the manikins, causing potential mechanical damage to the tubes and delay in the trial execution. We believe the impact of the repeated use should be small because we did not observe any lengthening of the time of administration towards the end of study.
Finally, we did not take into account of the time needed for the insertion of different nasogastric tubes in our study. Previous studies comparing nasogastric tube insertion with or without guidewire suggested the former is associated with higher success rate in first-attempt insertion, faster insertion time and less complication rate.20,21 It is reasonable to believe that insertion of a nasogastric tube with an internal guidewire or stylet is an alternative to traditional nasogastric tubes without stylet. However, given the fact that most local ED nurses and doctors have not been trained to insert nasogastric tubes with stylets, the insertion of the Corflo® nasogastric tube may take a longer time than the Ryle’s tube, which might cause further delay in AC administration.
To include the Corflo® nasogastric tube as a viable alternative to the Ryle’s tube, more training of the frontline ED staff is needed. Further studies that include the time for insertion of the nasogastric tube are warranted such that the ease with the Corflo® nasogastric tube insertion can be properly factored in during data analysis. Further studies that simulate intubated patients are also necessary to factor in the effect of the indwelling endotracheal tubes on AC delivery through the nasogastric tubes.
Conclusion
Our study provides experimental data and empirical evidence to support the use of the Corflo® nasogastric tube as a non-inferior alternative to the Ryle’s tube in administering AC to poisoned patients in the ED when Ryle’s tube insertion fails. Prior to adoption in daily practice, more experimental and clinical studies after adequate staff training on real patients are warranted to confirm the findings of this study and to optimise the settings for AC administration. Future studies should also factor in the time for insertion of different nasogastric tubes for a more complete assessment of the whole process.
Footnotes
Acknowledgements
The authors sincerely thank the Hong Kong College of Emergency Medicine for sponsorships for all the expenses from this study; School of Nursing, the University of Hong Kong, for lending the manikins for use; Dr Yiu Cheung CHAN, Chief of Service, Accident and Emergency Hospital, United Christian Hospital, for inspiration for the study; Dr Anthony WONG, Dr William WONG, Dr Tommy LAM, Dr Sam YANG and Dr Thomas AU, EBM (Evidence Based Medicine) Subcommittees of Hong Kong College of Emergency Medicine, for guidance through the whole course of study; Dr William WONG, Associate Consultant, Accident and Emergency Department, Princess Margaret Hospital, for instruction and contribution on data analysis; Dr Timothy WONG, Resident, Accident and Emergency Department, Queen Mary Hospital and Ms Jamie AU YEUNG, Pharmacist, Hong Kong Poison Information Centre, for logistic and information support. We would also like to thank Mr Michael LAU and Ms Crystal TANG, research assistants of the Department of Emergency Medicine, School of Clinical Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong for helping to run the trial. We would also like to express our gratitude to all doctors and nurses from Accident and Emergency Department, Queen Mary Hospital for participation in this study.
Author contributions
(1) HYY conceived and designed the study, (2) HYY acquired the data, (3) HYY analysed and interpreted the data, (4) HYY and RPKL drafted the manuscript, and (5) HYY, RPKL, MSHT critically revised the manuscript for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Availability of data and materials
The datasets generated and analysed during the current study are available from HYY.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Grant from Hong Kong College of Emergency Medicine.
Informed consent
Written informed consent was obtained from all participants before the study.
Ethical approval
This study is approved by the Institutional Review Board of the University of Hong Kong / Hospital Authority Hong Kong West Cluster (CRER No.: HKWC-2022-292; IRB Reference No.: UW 23-007).
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the IRB committee.
Trial registration
Not applicable because it is a manikin study.