
Abstract
Background:
Despite the increasing demand for procedural sedation and analgesia training, the number of available instructors remains limited.
Objective:
The aim of this study is to compare distance education with in-person learning for knowledge acquisition and participant satisfaction in procedural sedation and analgesia education.
Methods:
We conducted a randomized controlled trial comparing distance education with in-person learning in Japan on three occasions. Twenty participants per course were randomly divided into five groups with stratification by year of graduation. The groups were randomized to either a distance education group or an in-person group. We conducted pre- and post-testing of procedural sedation and analgesia knowledge and surveyed participants’ perceptions by using a scale ranging from 0 (not enough) to 100 (enough). Our primary outcomes were knowledge acquisition and the quality of discussion.
Results:
We included 48 healthcare professionals in the analysis. Forty-one participants (83.6%) were men and the median years of experience was 5 (interquartile range: 3–9). Both groups had similar knowledge acquisition with the pre-test and post-test score difference and reported similar scores on the quality of discussion with the exception of the clarity of audio quality (93 vs 100, p = 0.017).
Conclusion:
In a randomized trial of distance versus in-person learning for the sedation course, we did not observe statistically significant differences in knowledge acquisition and participant satisfaction between the two groups except for audio quality for the case discussion. Further efforts to improve quality for distance learning in procedural sedation and analgesia education are needed.
Introduction
In areas where there are few resources such as specialists and training course instructors, distance education is necessary to improve the quality of healthcare.1,2 In previous reports, distance learning was used in geriatric medicine and pathology education.3,4 Chipps et al. 5 reported that the effectiveness of video-camera-based distance education and in-person teaching was equivalent in increasing knowledge and knowledge retention. They also reported that distance education saved time, reduced travel costs, and increased the number of participants. 6
Procedural sedation and analgesia (PSA) is a common emergency department (ED) clinical practice using sedatives and/or analgesics in order to control pain and body movement during painful or unpleasant procedures. 7 In Japan, PSA in EDs is often performed by physicians who are not specialized in anesthesiology, including emergency physicians and residents.8–10 Due to limited training during medical school and post-graduate training, 11 the Japan Society of Procedural Sedation and Analgesia created a training module in 2014 called the “Sedation Course” with instruction focusing on safe sedation and analgesia. 12 This course consists of 4 h of didactics and 3 h of small group sessions. Table 1 shows the overall schedule of the training module. A skill session, simulation cases, and group discussions involving adult and pediatric cases are held during small group sessions. The effect of knowledge and skills retention and student interest in small group case discussion have also been shown in previous studies.13,14 However, the small group discussions require multiple instructors, which limits the number of courses available in remote areas.
Overall schedule of the PSA training module developed for Japanese health care professionals.
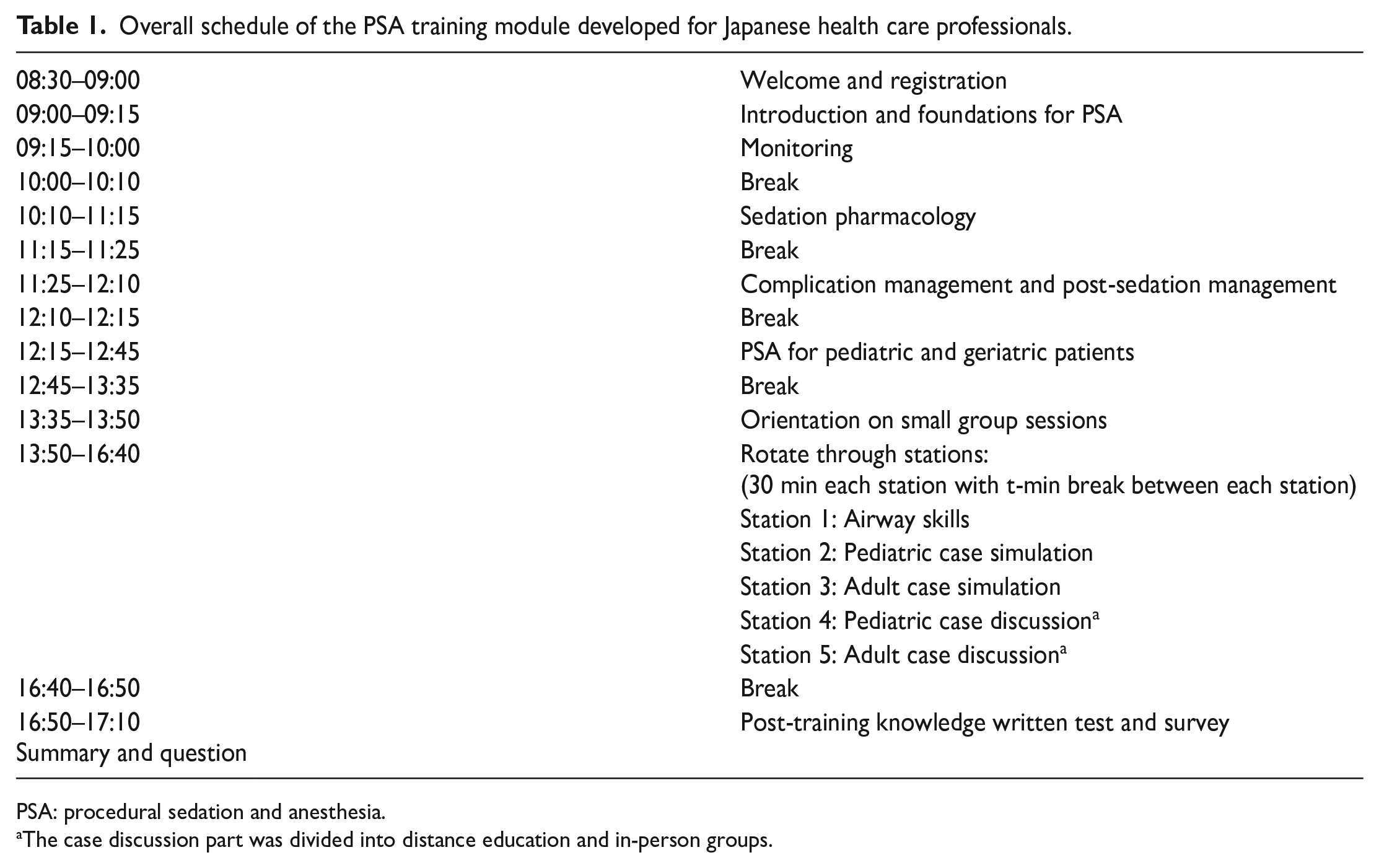
PSA: procedural sedation and anesthesia.
The case discussion part was divided into distance education and in-person groups.
Due to the increasing demand of the course, particularly in remote areas, as well as the limited number of instructors, we developed a distance education system to conduct teaching with case-based discussion. However, to date, there are limited studies focusing on knowledge acquisition and satisfaction of distance education in PSA education. The aim of this study is to compare distance education with in-person learning for the knowledge acquisition and participant satisfaction in PSA education in Japan.
Methods
Study design
We conducted a randomized controlled trial comparing distance education with in-person learning. The course was held on three occasions at two different institutions, Tokyo Bay Urayasu/Ichikawa Medical Center (June 2016 and February 2017) and Sapporo Tokushukai Hospital (March 2017). This study was conducted in accordance with the CONSORT statement (Supplemental Appendix 1).
Data collection and measurements
We included all participants who took the course and excluded participants who declined to consent, those who were not physicians (e.g. nurse), and those with incomplete responses to the questionnaire. We asked participants to complete a questionnaire on the quality of the small group discussions after the completion of the course (Table 2). We used a semantic differential scale method. On our scale, 100 was “enough” and 0 was “not enough.” The questionnaire was developed by a team of physicians specialized in anesthesiology, emergency medicine, and critical care medicine with significant experience in teaching PSA. We were also advised by a survey development expert on content, structure, and language. We also carried out a pre-test of PSA knowledge questions and a post-test immediately after the training intervention. Both pre- and post-assessments consisted of 10 written knowledge questions with multiple-choice questions. The case discussion section as well as the pre- and post-assessment tests covered all content of the sedation course. The pre- and post-assessment tests were scored by computer. Instructors with at least 10 years of PSA practice and teaching experience created the written knowledge questions. The details of the course and knowledge questions are discussed elsewhere. 12 Each question was categorized into one of five topics: PSA complications, pharmacology, sedation depth, NPO (nil per os) guidelines, and special populations including pediatrics and geriatrics. Pre- and post-intervention knowledge questions were identical.
The questionnaire after the procedural sedation and analgesia training module.
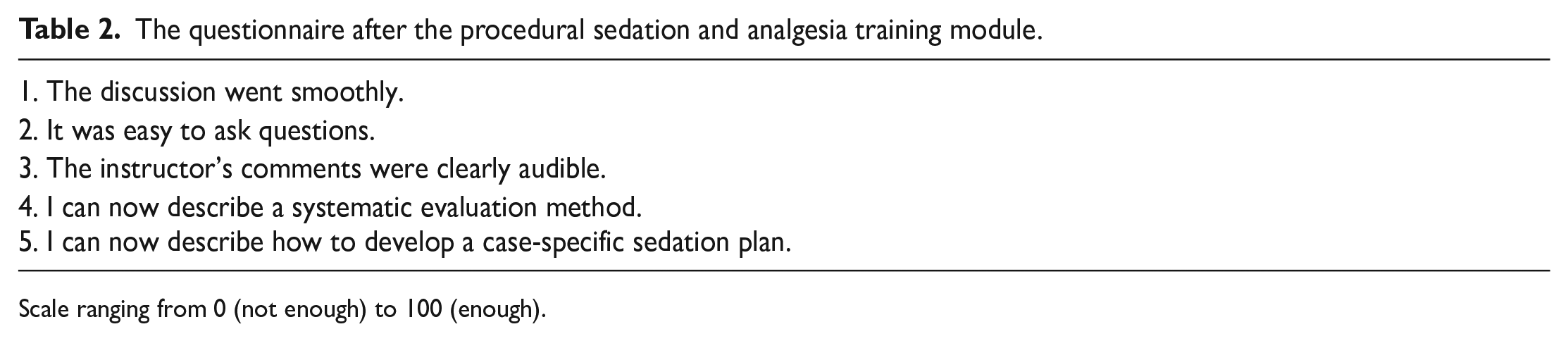
Scale ranging from 0 (not enough) to 100 (enough).
For the distance education group, we used Skype (Microsoft, Redmond, WA, USA), a free communication service with text, voice, and video messaging. 15 In 2012, there were 31 million registered Skype users and around 560 million people who had ever used the service. 15 The utility of distance education using Skype was reported in various specialties such as urology, obstetrics and gynecology, and surgery in several countries.16,17
We divided 20 participants per course into five groups randomly with stratification by graduation year. The randomization was performed by the staff of the course who were not involved in the study, using sealed envelopes. The five groups were randomized to the distance education group or the in-person group with a 1:1 allocation. Of the total 350 min training course, the case discussion (60 min) was randomized to distance education and in-person education. Due to the nature of the study, we could not blind participants nor instructors to their assignment. In order to reduce the facilitator’s influence, the same instructor led sessions with both the in-person group and distance education group. In the distance education group, the facilitator was in a separate room to avoid direct contact with participants. We used an assistant to manage issues with equipment and they were not allowed to participate in the session. In the distance education group, the case discussion was conducted remotely, and the other sections, including the content of education, were the same as those used in the in-person group. In both groups, all sessions, tests, and questions were conducted in Japanese.
Data analysis
Our primary objective was to compare the knowledge acquisition and participant satisfaction between distance education and in-person learning. The median and interquartile range (IQR) were calculated for continuous variables, with the number of cases and percentages calculated for nominal variables. Mann–Whitney U tests were used to compare the group difference because the data were not normally distributed. The p values presented were from a two-tailed test, and values <0.05 were considered statistically significant. All data analyses were performed with EZR software V.1.28 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a modified version of R commander designed to add statistical functions. 18
Results
There were 59 healthcare professionals who participated in the courses. Among them, 49 (83.1%) physicians were included in the analysis. Figure 1 shows the selection and exclusion of the study participants. Forty-one participants (83.6%) were men. The median years of experience was 5 (IQR: 3–9), and nine (18.4%) were residents. Figure 2 shows the physicians’ primary specialties. The most common specialty was emergency medicine (n = 24, 49.0%), followed by general internal medicine (n = 9, 18.4%).
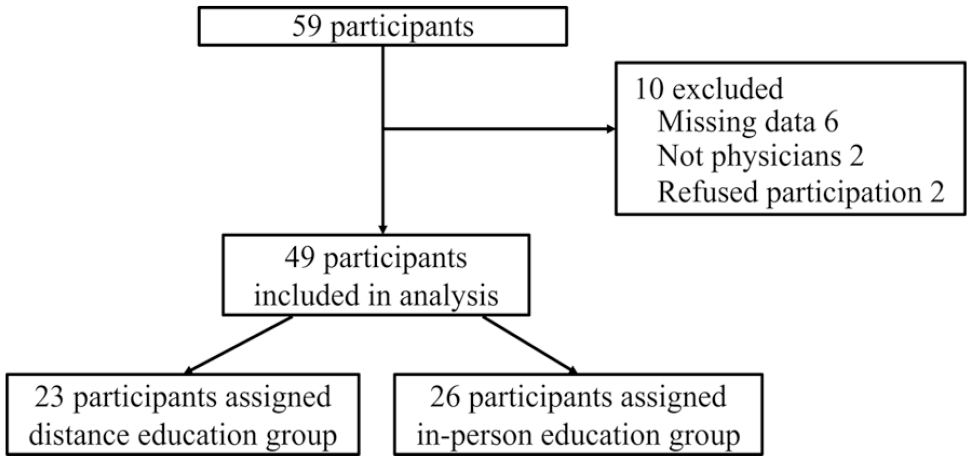
The flowchart of participants.
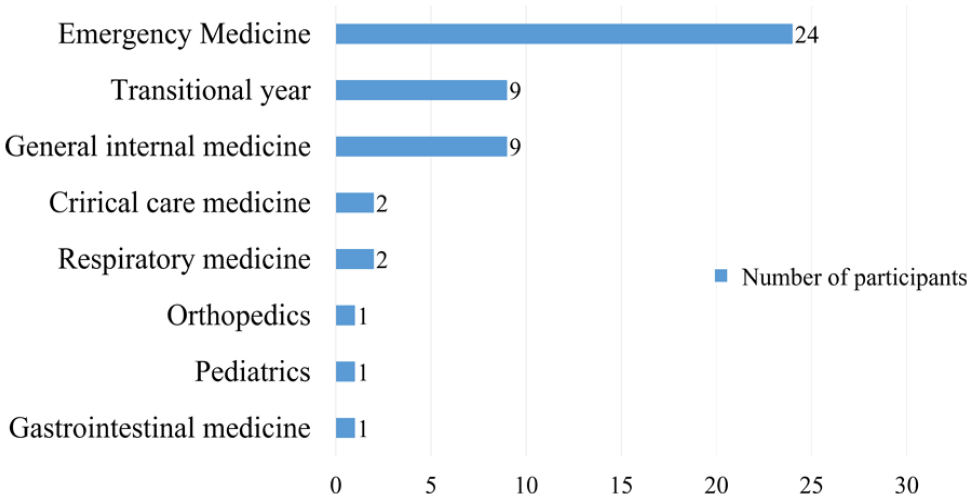
Primary specialties of physicians who participated in the study.
Both groups had significant improvement on knowledge acquisition as indicated by the score difference of the pre- and post-tests (distance education group vs in-person group; median: 2 (IQR: 1–4) vs 2 (1–2.75), p = 0.226) and there was no statistically significant difference between the two groups (Table 3). In the questionnaire, the in-person group reported higher scores for the statement, “The instructor’s comments were clearly audible” compared to the distance education group (median: 93 (IQR: 67–100) vs 100 (94–100), p = 0.017). There were no other statistical differences in the remainder of the questionnaire (Table 3).
Comparison of results of questionnaire and test scores, according the educational device.
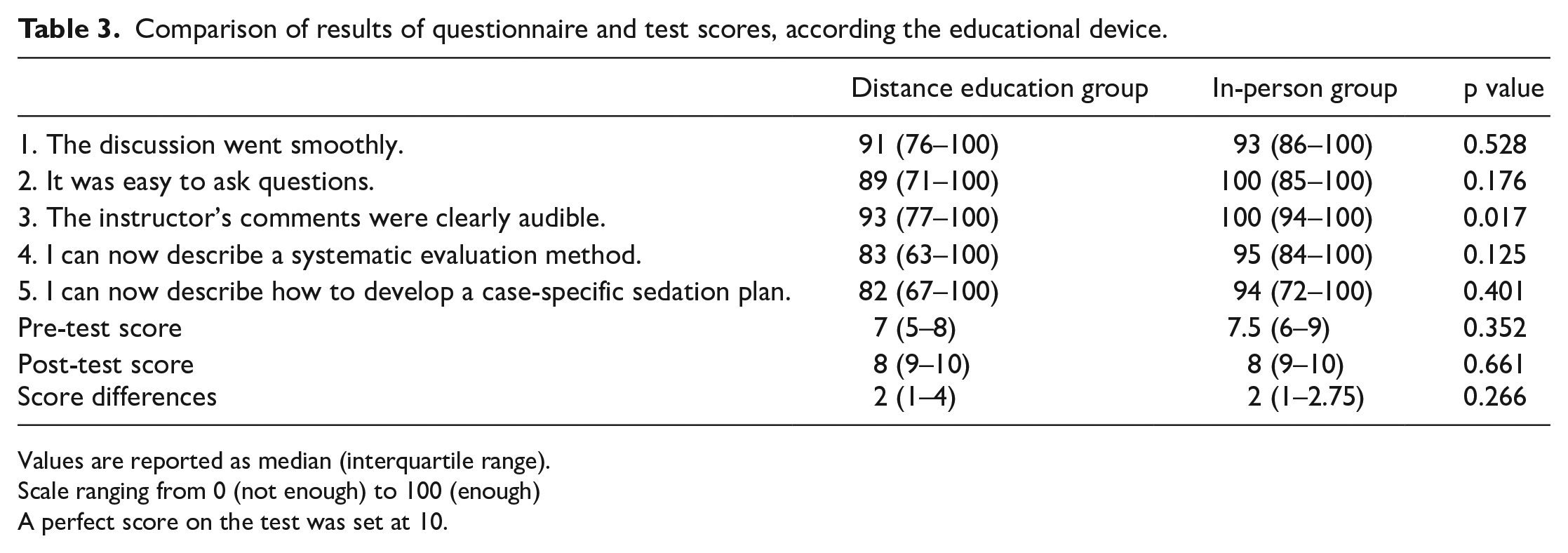
Values are reported as median (interquartile range).
Scale ranging from 0 (not enough) to 100 (enough)A perfect score on the test was set at 10.
Discussions
In this study, we compared knowledge acquisition and participant satisfaction between distance education and in-person education using a PSA training course. The in-person group reported better audio clarity compared to the distance education group; however, there was no statistically significant difference in the other outcomes, including knowledge acquisition.
Our results of the study were consistent with a previous study conducted by Chipps et al. 6 In the study, the audio quality in the distance education group was not as clear during the discussion; however, participants responded that the quality was satisfactory. As there were no significant differences between the other items in our study, the audio quality did not appear to have a significant effect on the knowledge acquisition and participant satisfaction.
There is an increasing amount of literature suggesting that the effectiveness of distance education might be equivalent to in-person education in certain settings.3–5 The reported barriers of distance education included time constraints, poor technical skills, and inadequate infrastructure. 19 In addition, the use of distance education during case-based discussion to teach complex clinical concepts is limited and has not been well studied. This study showed new evidence of distance education during case-based discussion.
The advantages of distance education would include reduced cost and travel time. Because instructors do not need to travel, there is no need to reimburse travel expenses. The cost of travel for instructors accounted for the second largest portion of overall costs, after the instructors’ honorarium. 20 Computers are often available at the facility or at home, which is another financial advantage for the module. Therefore, reduced participation fees may be considered in the future. This is especially beneficial for training non-anesthesiology-trained healthcare providers in remote locations. The PSA course typically costs around US$800 to cover the travel cost of the required instructors. The travel cost could be reduced by 100% by fully implementing distance education to our course. If the hands-on portion remained as in-person training with the discussion section conducted as distance education, the cost could be reduced by up to 40% per course. We also would have to consider travel time for instructors, which would allow for more flexibility with scheduling the date of the course.
Another advantage of distance learning is that it requires less contact. Case-based group discussion is one of the most common methods of teaching complex clinical concepts such as difficult airway management and is frequently performed during training courses such as Advanced Trauma Life Support. 21 Due to the COVID-19 pandemic, distance learning has received more attention as an alternative method for education.22,23 COVID-19 is transmitted by aerosol. 24 Since aerosol emissions are released during speech and emission rate increases with voice loudness, 25 in-person small group discussions may be a risk for infection. Appropriate implementation of measures against contact and droplet transmission is important to prevent COVID-19 transmission. Unfortunately, healthcare workers are at a higher rate of infection risk than non-health care workers. 26 Instructors could participate even if they were in high-risk areas. Not only are in-person discussions associated with risk of infection due to close contact, but these courses often require travel in order to attend courses that put them at risk of infection. In the future, offering this PSA course completely online could mitigate these risks. This is particularly useful to continue providing necessary training to practitioners while complying with safe social distancing practices.
There are several limitations in this study. First, the validity and reliability of this questionnaire have not been examined. To our knowledge, there is no questionnaire that has been validated for reliability and validity of the teleconference discussion format. Therefore, it is necessary to develop questionnaires that have been verified for reliability and validity in the future. Second, this trial was designed as a superiority trial and not a non-inferiority trial due to the large sample size required. Thus, we could not conclude that distance education and in-person education on PSA training are equivalent. Third, this study might present a ceiling effect. In many cases, the participants received full marks on the post-test. However, if we increase sample size, the ceiling effect may still occur in a highly satisfactory course. Fourth, since each training course has its unique objectives and curriculums, the results of the study may not be applicable to other training courses. Finally, we only assessed the knowledge acquisition and participant satisfaction. Further studies are warranted to assess improvement of skills and attitudes as the next step.
Conclusion
In a randomized trial of distance versus in-person learning for the sedation course, we did not observe statistically significant differences in knowledge acquisition and participant satisfaction between the two groups except for audio quality for the case discussion. Because distance learning may also require low cost and less contact, this is beneficial for emergency physicians and other healthcare providers particularly in remote areas. Further efforts to improve quality for distance learning in PSA education are needed.
Supplemental Material
sj-docx-1-hkj-10.1177_10249079231166331 – Supplemental material for Comparison of distance education and in-person education in procedural sedation and analgesia: A randomized controlled trial
Supplemental material, sj-docx-1-hkj-10.1177_10249079231166331 for Comparison of distance education and in-person education in procedural sedation and analgesia: A randomized controlled trial by Shinya Takeuchi, Tatsuya Norii, Marisa Rivera and Yosuke Homma in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors also would like to acknowledge Nakagawa Urara, MD, and Simosato Akihikari, MD, for their valuable comments and suggestions in improving the quality of the training courses and the study. We also would like to thank all the instructors who teach the “sedation course” in the Japan Society of Procedural Sedation and Analgesia.
Authorship
S.T., T.N., and Y.H. conceived the project and designed the study. S.T. and Y.H. analyzed and interpreted the data. S.T. drafted the primary draft of the manuscript. T.N., Y.H., and R.M. revised the manuscript critically for important intellectual content. All authors have revised and approved the final version of the manuscript.
Availability of data and materials
The data sets generated and/or analyzed during the current study are available from corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All subjects provided verbal and written consent.
Ethical approval and ethical number provided by the review board
A detailed plan for this study was prepared prior to implementation and was approved by the Ethics Committee of Tokyo Bay Urayasu/Ichikawa Medical Center (No. 186, 15 July 2015).
Human rights statement
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.