
Abstract

A 54-year-old man with ankylosing spondylitis (AS) presented to the emergency department 1 day after a staircase slip and fall injury. He complained of localized neck pain after the injury. He had no limb numbness, weakness, urinary retention or incontinence.
On examination, he was fully conscious with a blood pressure of 137/84 mmHg and a heart rate of 85 beats per minute. He had no dyspnoea and the respiratory movement was normal. Neck examination found midline lower cervical spine tenderness with a restricted range of movement, which is similar to baseline according to the patient. He had full limb power. Sensation was intact.
X-rays of his cervical spine were taken and shown below (Images 1 and 2).
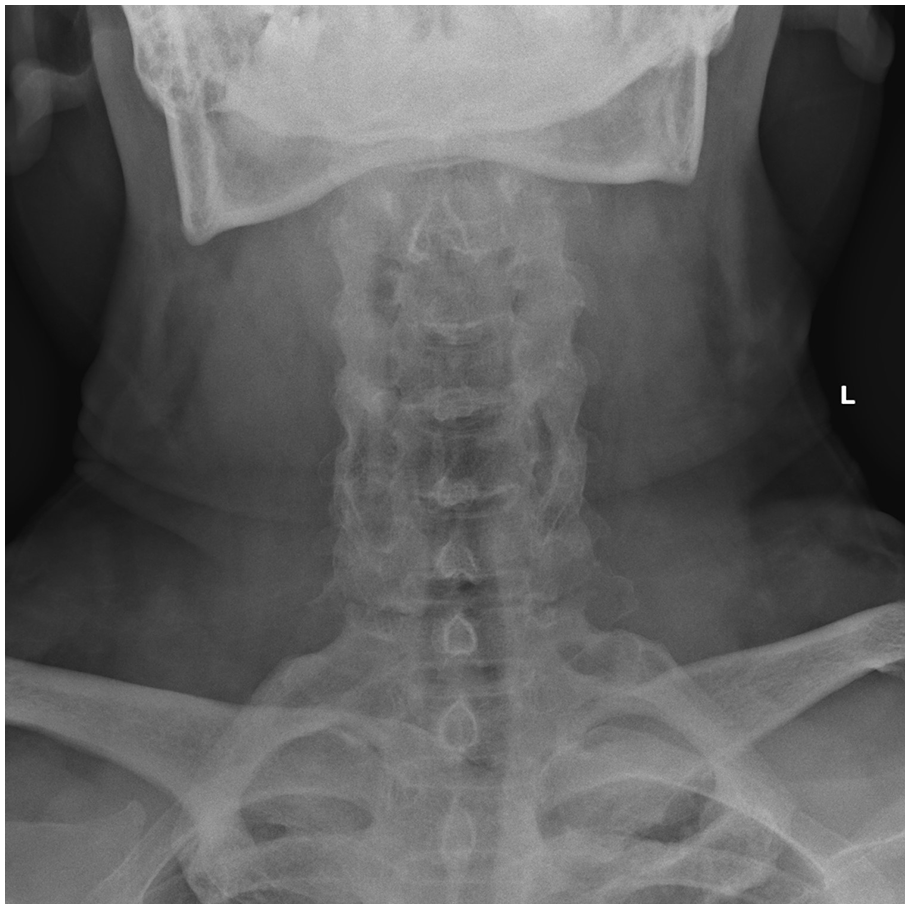
Anteroposterior view of X-ray of the patient’s cervical spine.
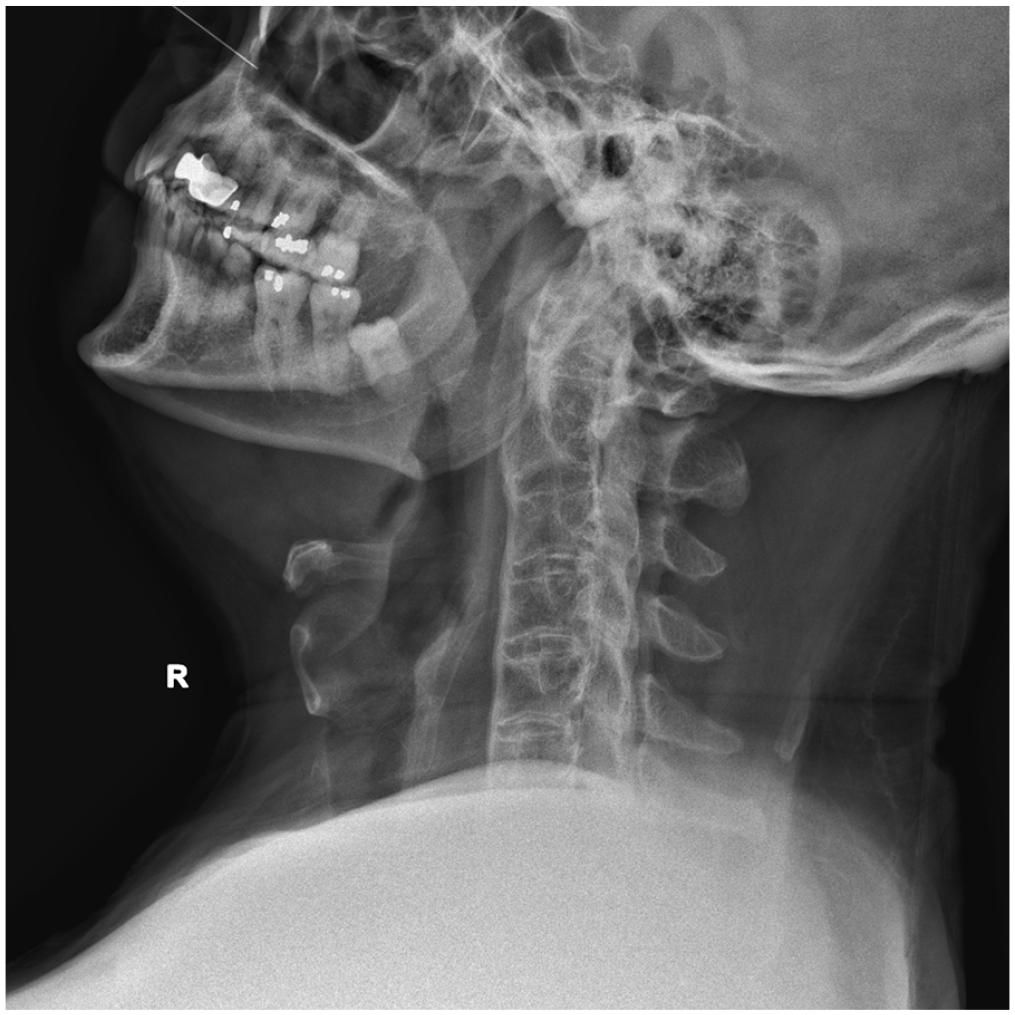
Lateral view of X-ray of the patient’s cervical spine.
Questions
What are your interpretations of his X-rays?
Why should emergency physicians be cautious when encountering cases of minor spine injury in AS?
Trauma guidelines recommend cervical spine precaution, protection and clearance in blunt neck injury. How are these measures different in AS patients from the general population?
Answer
The cervical spine X-rays showed a bamboo spine which is in line with AS. The anteroposterior view showed a radiolucent line at C7. The lateral view failed to include C7 and hence it did not show the suspected fracture line.
Computed tomography of cervical spine confirmed an unstable, undisplaced three column chalk stick fracture at C7 (Image 3).
AS patients have a rigid, osteopenic spine which is prone to fracture at any level. Patients living with AS are up to 4 times more likely to sustain spinal fractures and 7 times more likely to sustain blunt cerebrovascular injury than the general population.1,2
Delayed and missed diagnoses of spinal fracture in AS are common, due to absence of major trauma in the patient’s history (up to 55%), absence of neurological deficit on presentation (up to 42%) and difficulty to interpret X-ray film of spine with preexisting pathologic osseous change.3,4 When the condition is missed in an inherently unstable fracture, abrupt neurological deterioration could occur in a delayed manner–a phenomenon known as ‘the fatal pause’. 4 Therefore, careful radiological assessment should be undertaken for all patients with AS and spinal injury.
In AS and other ankylosing conditions, the cervical spine may develop a fixed flexion deformity. The hard collar, which is often used to maintain the cervical spine in a neutral position, will not fit the rigid, kyphotic cervical spine. Inattentive application of hard collar in these patients can cause injury exacerbation, neurological complication and death. An injured neck could instead be supported manually or with sandbags at either side of the neck and under the occiput. Consult the orthopaedics surgeon for halo brace application. 5
Avoid applying the cervical spine clearance rules in AS patients. The original study of Canadian C-spine rule excluded AS patients and the rule had not been validated among AS patients with blunt neck injury. 6
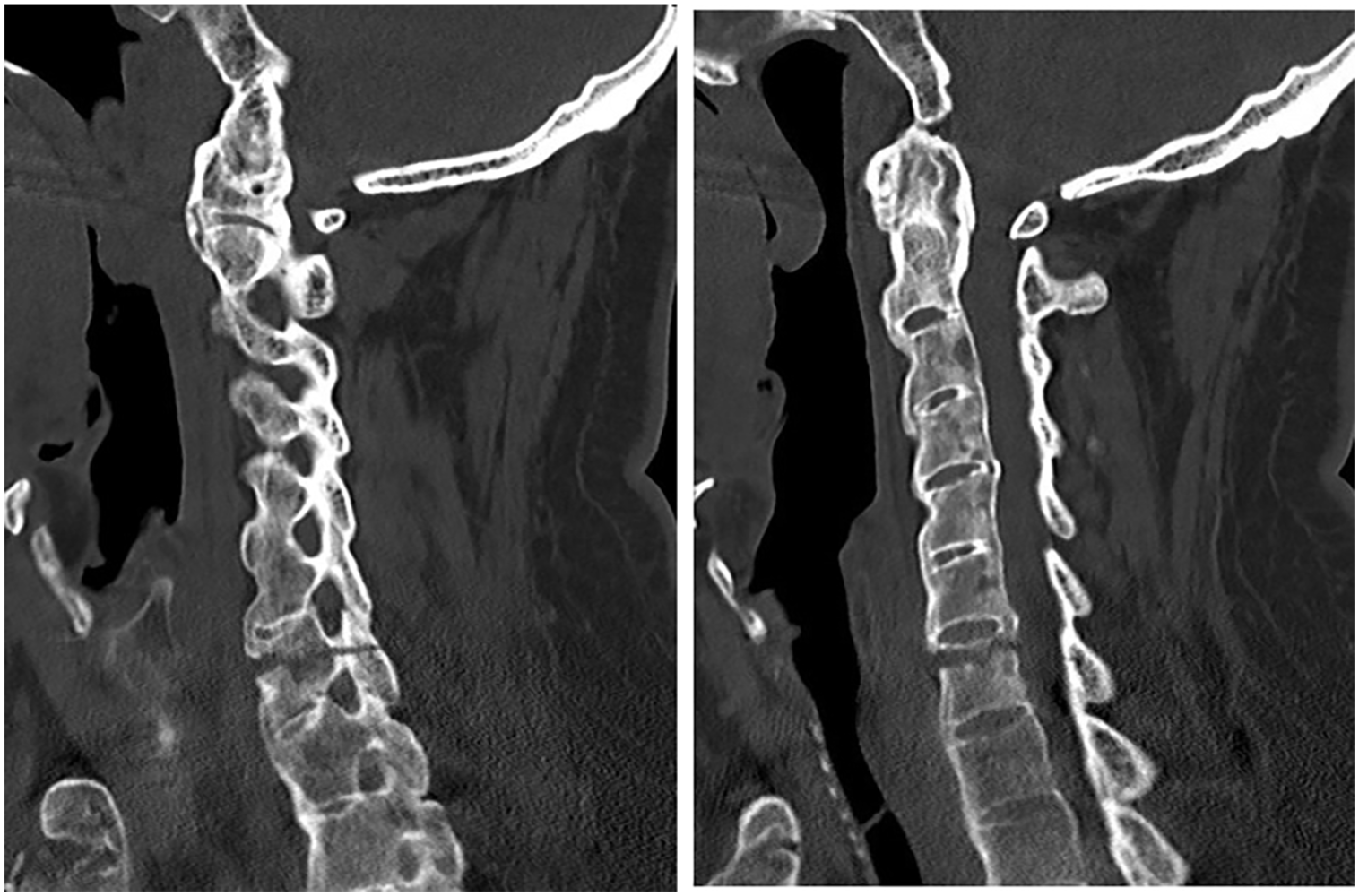
Selected image of patient’s cervical spine computed tomography scan.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.