
Abstract
Background:
The Hong Kong Poison Information Centre (HKPIC) provides consultation service to health care professionals and collect epidemiological data on poisoning in Hong Kong since 2005.
Objective:
To report and analyse the data of Hong Kong Poison Information Centre on poisoning in 2019.
Methods:
This was a retrospective review of all poisoning cases recorded in the Poison Information and Clinical Management System of Hong Kong Poison Information Centre in 2019.
Results:
A total of 4016 poisoned cases were analysed, which involved 1698 men (42.3%), 2312 women (57.6%) and 6 sex-unspecified patients (0.1%). Majority of cases (77.3%) were between 13 and 69 years of age, and 10.5% were teenagers 13–19 years of age. Self-harm/suicidal attempt (42.1%), unintentional exposure (18.1%) and abusive substance use (11.1%) were common reasons of poisoning. Excluding ethanol, which was the common co-ingestant, the five most common types of poison were benzodiazepines, paracetamol, household products, zopiclone and Chinese herbal medicine. While most patients were managed with supportive treatment, 16.5% and 16.8% of the consultation cases were treated with decontamination and antidotes, respectively. Majority of cases recovered uneventfully, but 1.0% died and 4.7% had a major outcome. A total of six interesting cases and two outbreaks were discussed in this report.
Conclusion:
This 14th annual report provided updated epidemiological information on the pattern of poisoning in Hong Kong and highlighted a number of important changes compared with our previous reports.
Introduction
The Hong Kong Poison Information Centre (HKPIC) was established in 2005. Currently, it provides round-the-clock phone consultation service to healthcare professionals in Hong Kong for poison information and advice on clinical management of poisoning. It also provides onsite clinical toxicology service to poisoned patients in United Christian Hospital where the centre is located, and postgraduate diploma and fellowship training in clinical toxicology. HKPIC routinely collects epidemiological data on poisoning in Hong Kong through voluntary reporting from all accident and emergency departments (AEDs) in the Hospital Authority (HA).
HKPIC has started to publish annual reports on poisoning since 2006. It continues to provide updated information on the epidemiology of poisoning and its changing trend in Hong Kong. This 14th annual report of HKPIC covers the data in 2019 and focuses on the latest pattern of poisoning as in previous reports. We also discuss a few poisoning cases with educational value to healthcare professionals.
Methods
The HKPIC receives notification of poisoning from two primary sources: consultation and reporting. Consultation cases are defined as poisoning cases that healthcare professionals consult HKPIC for poison information or management advice. Reporting cases are defined as poisoning cases reported through HA, mostly from all public AEDs. In this report, we retrieved all cases received by HKPIC in 2019 from its database, Poison Information and Clinical Management System (PICMS), for analysis.
The data of each poisoning case are inputted into PICMS according to the information obtained from the consulting healthcare professionals, medical records, electronic patient record (ePR) of HA and other relevant sources. For consultation cases, data collected include patient demographic data, poison data (poison type and dose, route, time, place and reason of exposure), clinical data (clinical features and investigation results), management data (use of decontamination, antidotes and other specific treatment) and outcome data (disposal for AED patients, final outcome and its relationship with the poison exposure). For reporting cases, only patient demographic data, poison data and outcome data are inputted.
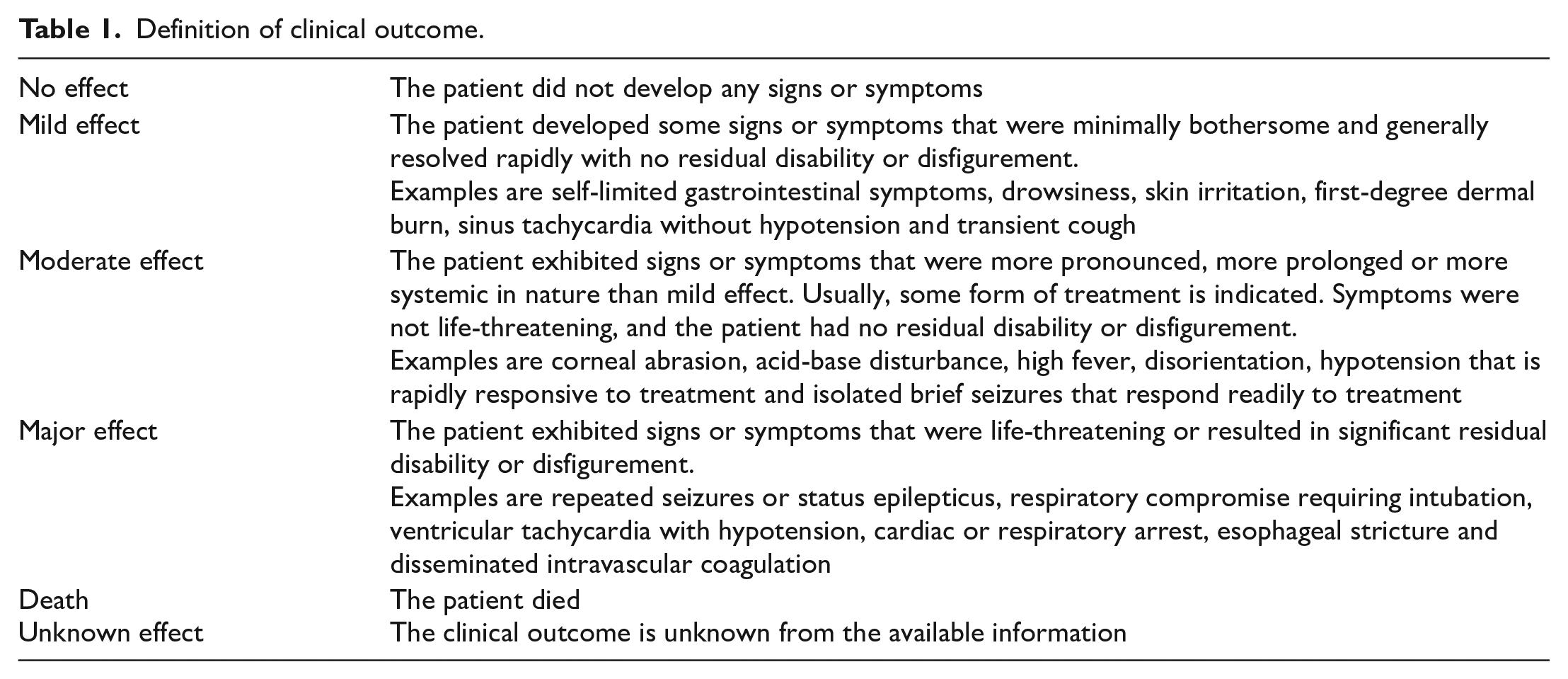
Senior doctors in HKPIC classify the outcome of the cases into five categories: no effect, mild effect, moderate effect, major effect or death with reference to the American Association of Poison Control Centers’ National Poison Data System (Table 1). 1 The relationship between poison exposure and clinical outcome is graded as definite, probable, possible, not related or undetermined/not applicable according to available information. All death or major effect cases are further reviewed by a second senior doctor to ensure appropriate grading.
Definition of clinical outcome.
The information used in this annual report was considered as a part of the usual clinical data routinely collected by HKPIC and was handed to the researchers anonymously. Only aggregate data were reported. As such, research ethics approval and informed consent were not required according to the prevailing policy of the Research Ethics Committee of Kowloon Central/East Cluster (REC(KC/KE)) of HA where HKPIC is located. Research ethical approval was previously applied for HKPIC annual report and judged to be not required by the REC(KC/KE).
Results
After exclusion of duplicate and invalid cases, our search in PICMS identified 4016 valid cases in 2019, including 2100 (52.3%) consultation cases and 1916 (47.7%) reporting cases for analysis.
The age and gender distribution of the cases are shown in Figure 1. There were 1698 male patients (42.3%), 2312 female patients (57.6%) and 6 sex-unspecified patients (0.1%). A female predominance was noted in majority of the age groups except for children aged 0–5 and elderly patients aged 60–69 years. Regarding the age distribution, there were around 14% of the total population in each of the age groups 20–29, 30–39, 40–49 and 50–59 years, which together accounted for 56.8% of all cases. Around one-tenth of the cases (10.5%) were teenagers 13–19 years of age this year, and 5.9% were elderly aged 80 years or above.
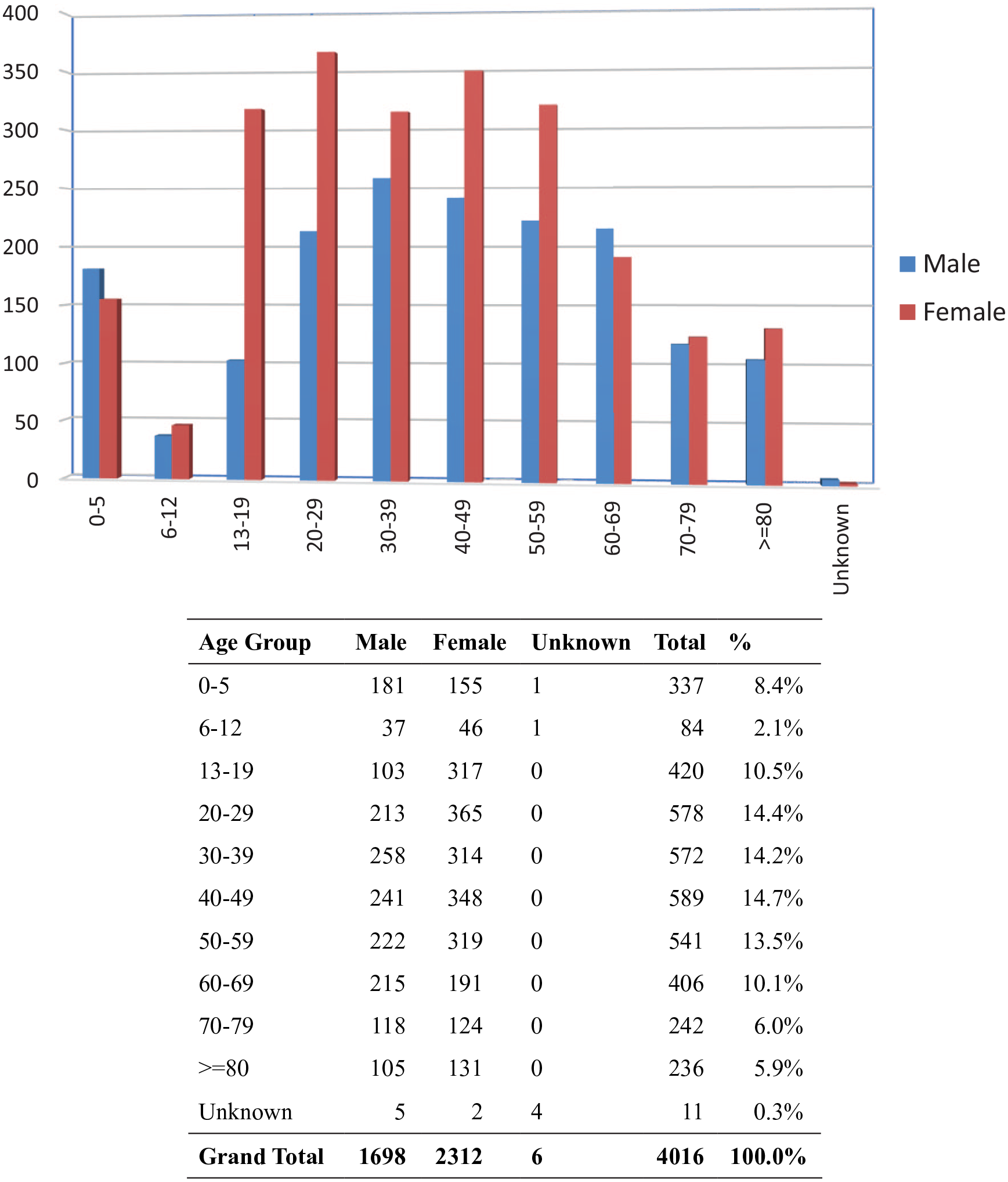
Age and gender distribution.
The reasons for poisoning are listed in Figure 2. Suspected self-harm/suicidal attempt was the most frequent reason, which accounted for 42.1% of the cases. Poisoning due to unintentional exposure (18.1%) and abuse (11.1%) ranked the second- and third-most common cause, respectively. Together with venomous bites and stings (6.9%) and adverse reactions to herbal or proprietary Chinese medicine (7.0%), these five most common reasons for poisoning contributed to the vast majority (85.2%) of the cases. As shown in Figures 3 and 4, the most common place of exposure was patient’s residential place (64.5%). The most common route of poisoning was ingestion (82.0%), followed by inhalation (7.6%) and dermal exposure (5.4%).
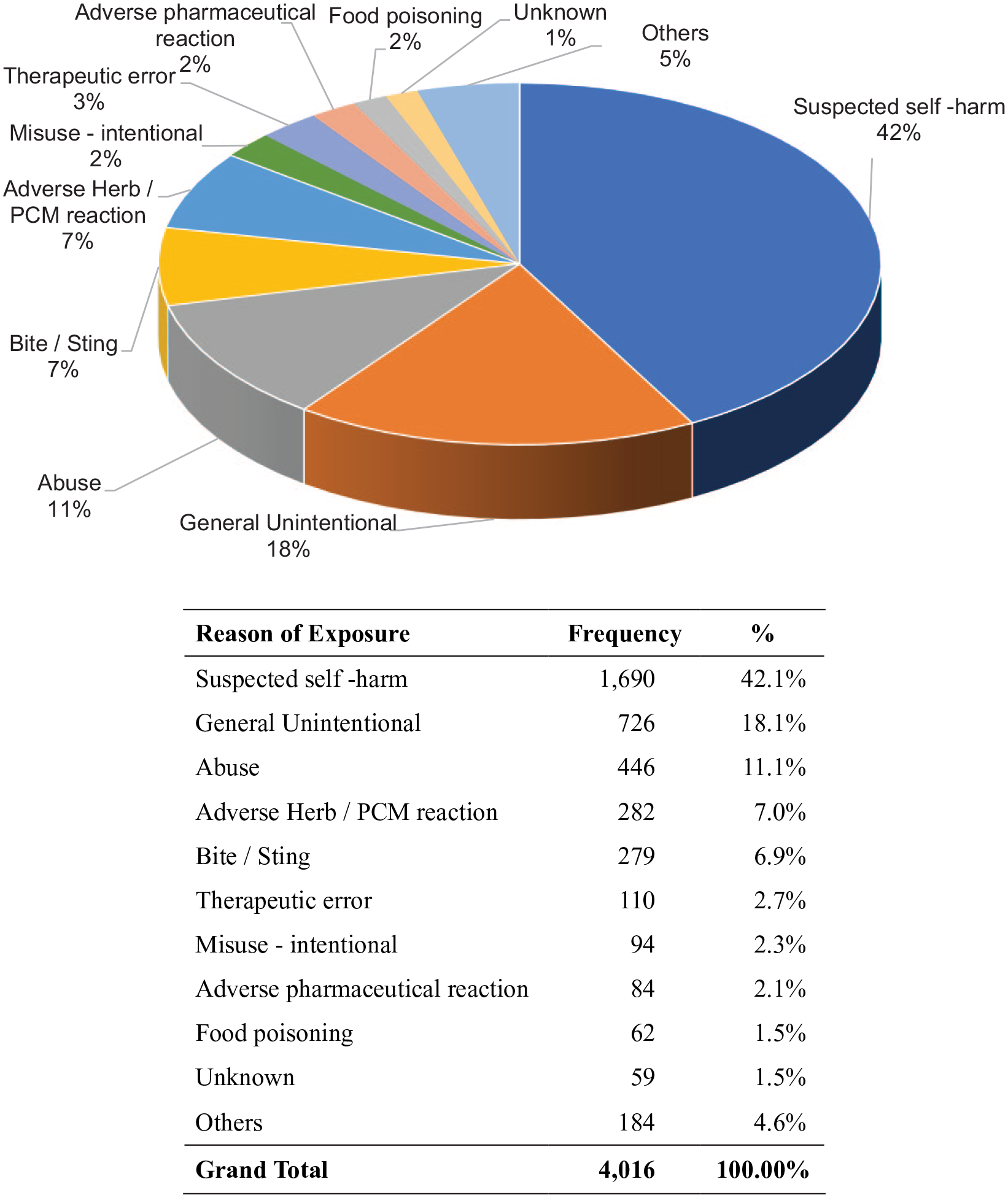
Reason of exposure.
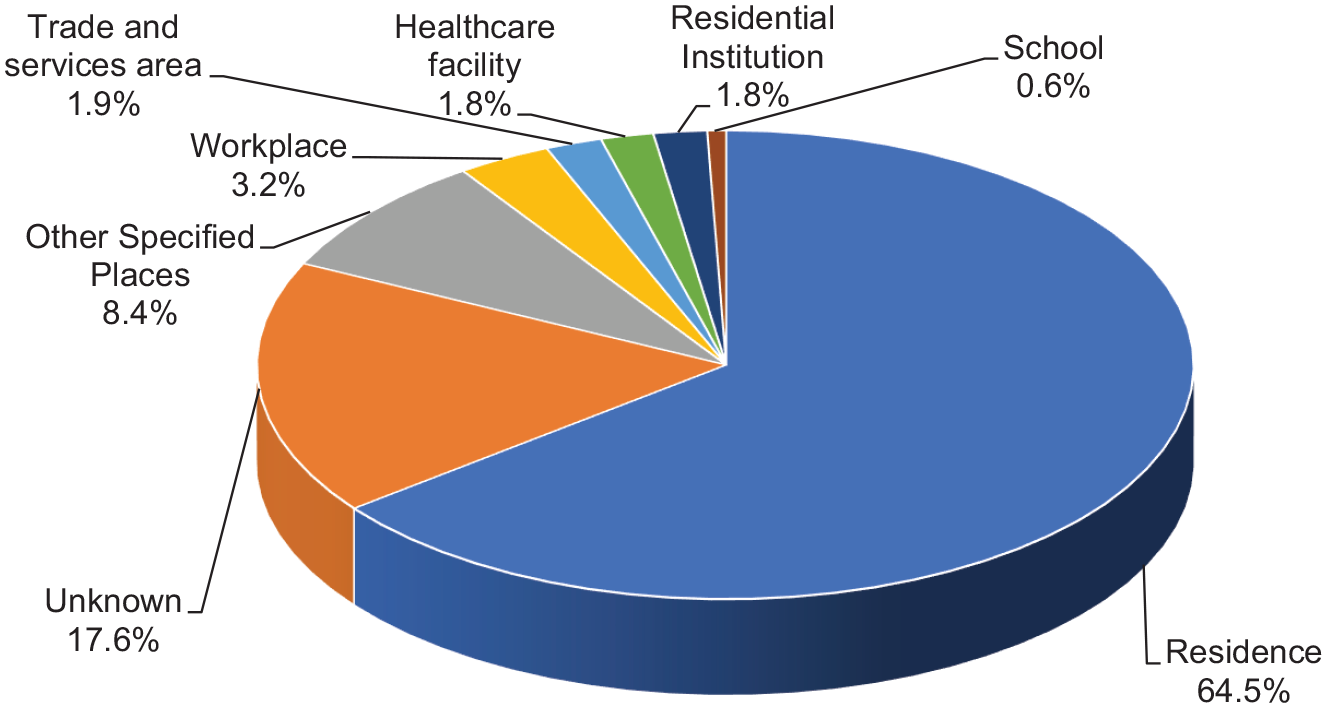
Place of exposure.
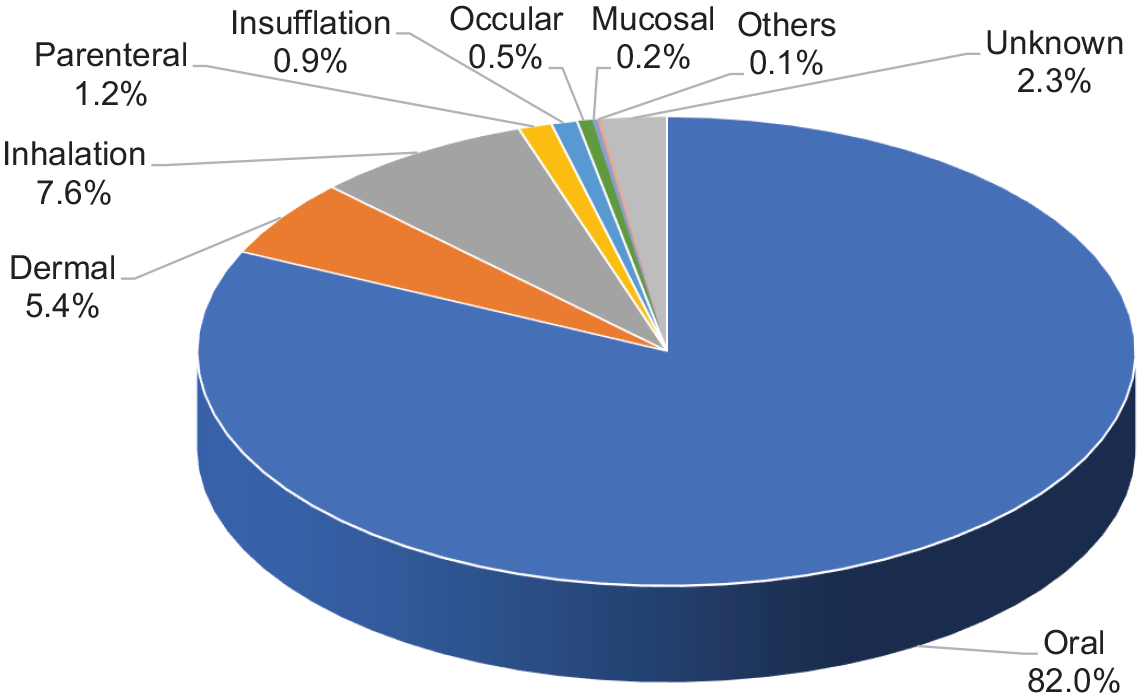
Route of exposure.
A total of 6152 poisons were involved in the 4016 cases, of which 70.9% had exposure to a single poison and 29.1% had exposure to multiple poisons. The types of poison exposure are shown in Figure 5. Apart from ethanol, which was commonly involved as a co-ingestant, the five most common types of poison were benzodiazepines (417 cases), paracetamol (364 cases), household products (292 cases), zopiclone (289 cases) and Chinese herbal medicine (CHM; 251 cases).
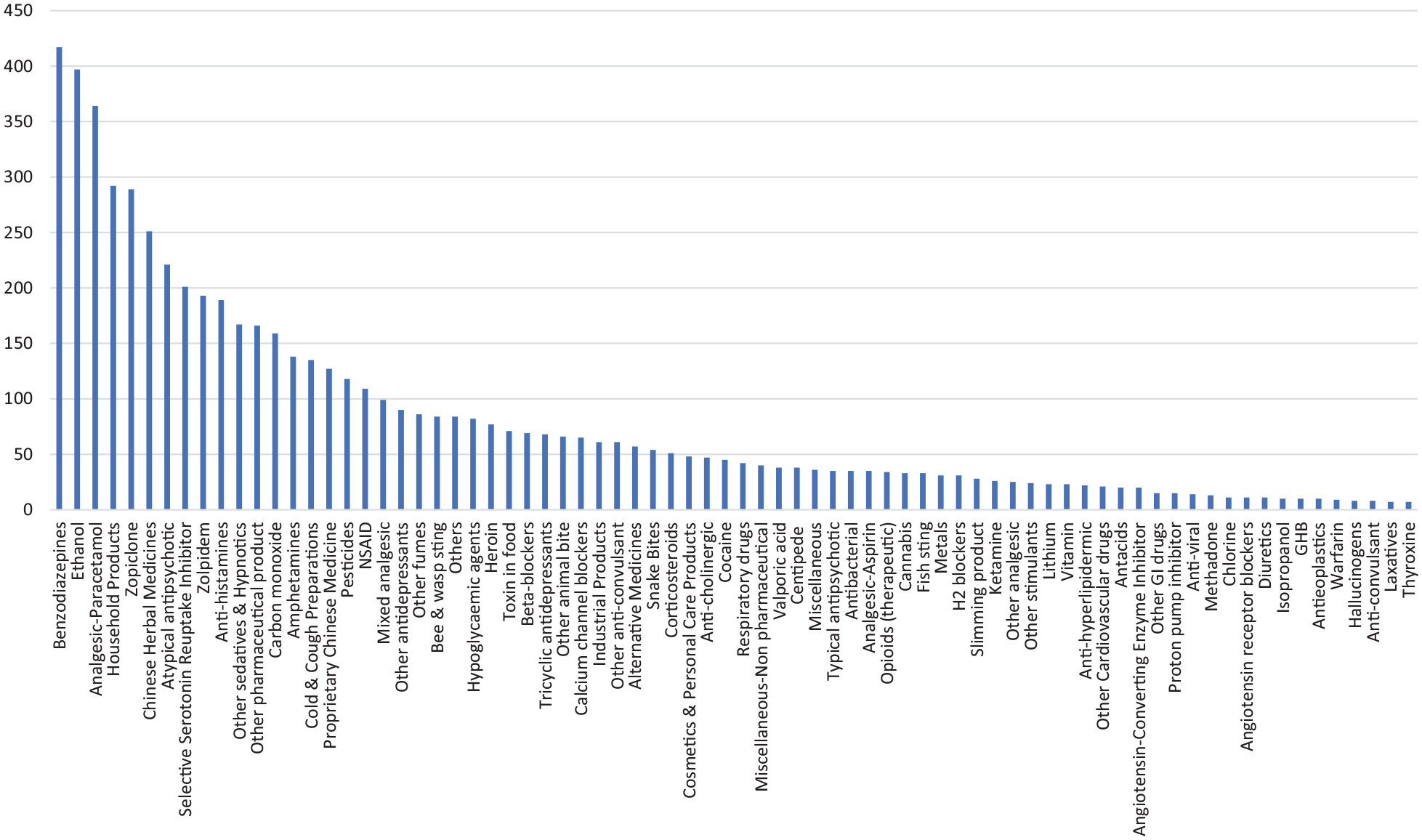
Type of poison exposed.
As for the analysis on the use of decontamination and antidote, only consultation cases were included. Among the 2100 consultation cases, 346 (16.5%) patients underwent decontamination, including 14 cases who received multiple decontamination methods. The most common decontamination method was single-dose activated charcoal (AC; 91.0%), followed by multiple-dose AC (MDAC; 5.2%) and gastric lavage (2.9%), as shown in Table 2. Regarding the antidote use, 353 (16.8 %) patients were treated with antidotes and 46 of them were given more than one antidote. The five most common antidotes used were N-acetylcysteine (NAC), benzodiazepines, hyperbaric oxygen, sodium bicarbonate and snake antivenin/calcium (Table 3).
Decontamination.
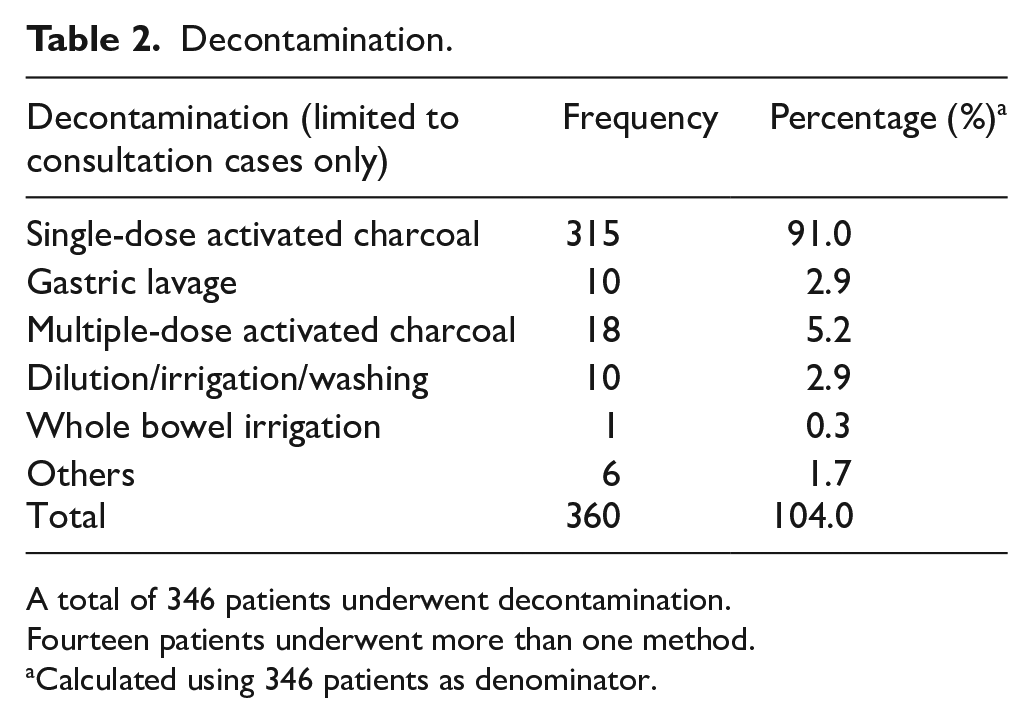
A total of 346 patients underwent decontamination.
Fourteen patients underwent more than one method.
Calculated using 346 patients as denominator.
Antidote.
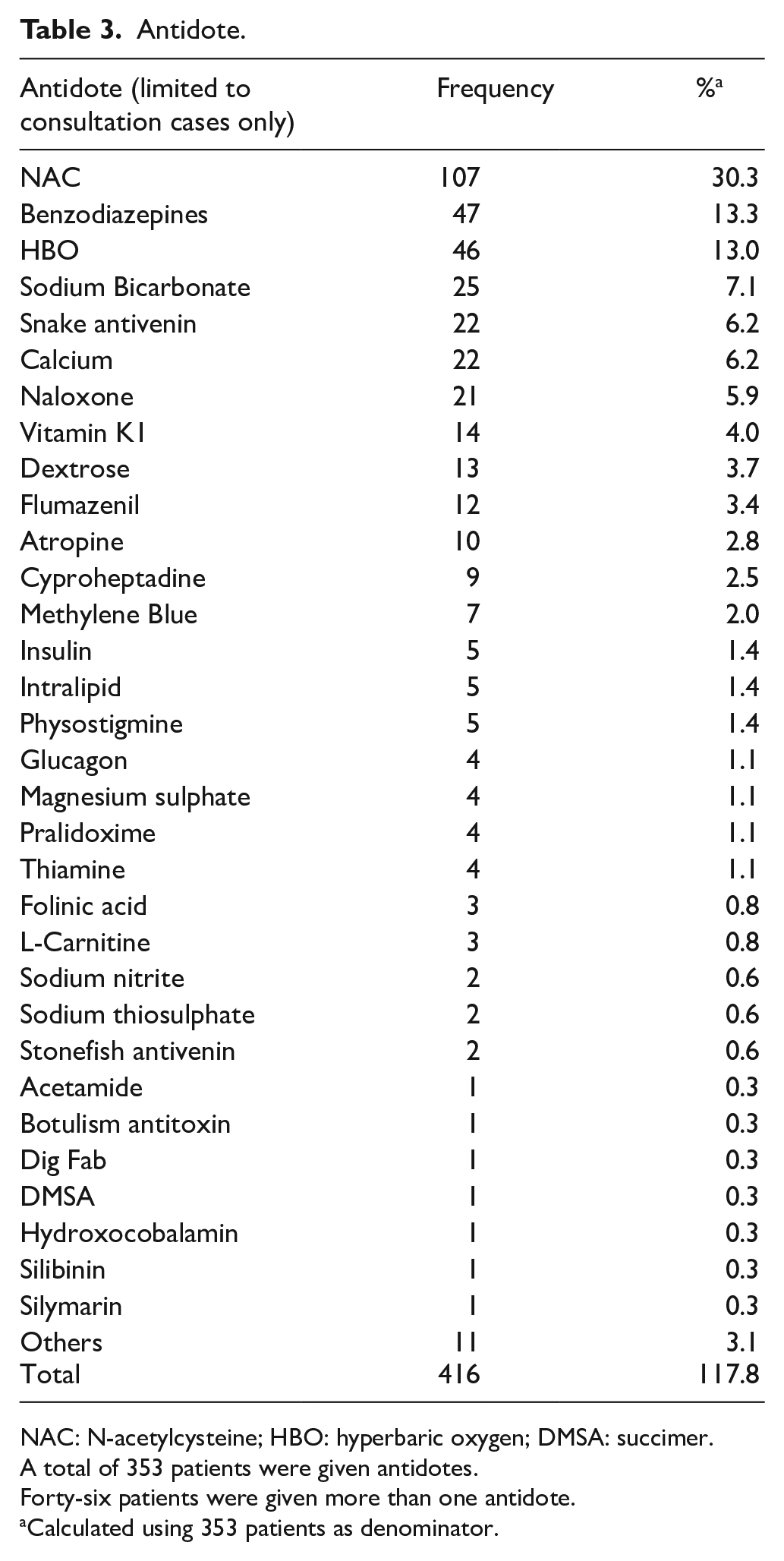
NAC: N-acetylcysteine; HBO: hyperbaric oxygen; DMSA: succimer.
A total of 353 patients were given antidotes.
Forty-six patients were given more than one antidote.
Calculated using 353 patients as denominator.
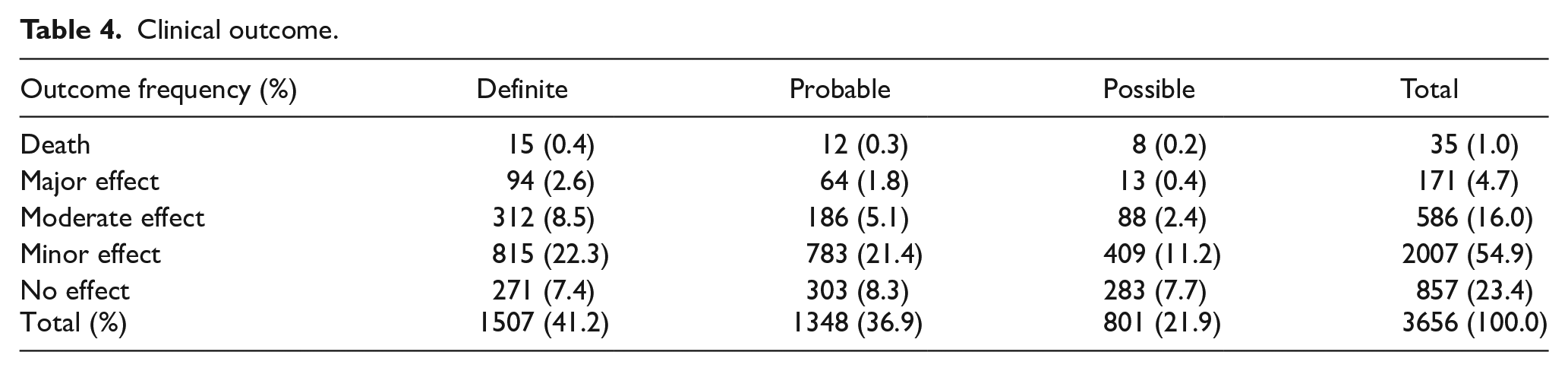
After excluding 360 cases in which the clinical outcomes were graded as not related to the poison exposure, or clinical outcome could not be assessed from the available information, the remaining 3656 cases (100%) were analysed for the outcome. There were 35 deaths (1.0%), 171 cases of major effects (4.7%), 586 cases of moderate effects (16.0%), 2007 cases of mild effects (54.9%) and 857 cases of no effect (23.4%), as shown in Table 4. As for the relationship between poison exposure and the outcome, 41.2%, 36.9% and 21.9% of the outcomes were graded as definitely, probably and possibly related to the poison exposure, respectively.
Clinical outcome.
In 2019, we received 317 consultations on pre-hospital AC administration. Among these 317 patients, 191 (60.3%) patients were given AC by ambulance paramedics. The remaining 126 (39.7%) patients were either not indicated for AC administration or judged to be not suitable for AC administration during the ambulance transfer.
Discussion
This 14th annual report of HKPIC analysed the data of 4160 poisoned cases in 2019, which represented the most updated pattern of poisoning in Hong Kong.
Reporting of poisoning to HKPIC is not compulsory in Hong Kong and it remains one of the intrinsic limitations of our data, which is common in other poison databases in developed countries. However, HKPIC records around 4000 cases yearly with comparable figures of death and major outcomes over the past few years. We believe that we have captured majority of poisoning cases in our locality and the data are representative.
The age and gender distribution, and routes of exposure were grossly similar when compared with our previous reports and overseas data.1,2 This year, the previously observed rising trend of poisoning in the teenage group (13–19 years) continued, with the proportion increasing from 6.3% in 2016, 7.6% in 2017, 8.9% in 2018 to 10.5% this year. A rising trend is also observed in the elderly group (> 80 years), from 3.9% in 2016, 4.7% in both 2017 and 2018 to 5.9% this year. Increasing teenager poisoning is a potential public concern. Continued monitoring of the trend and further analysis of the data are suggested to look into these two problems in details.
The three most common reasons of exposure, namely suspected self-harm, unintentional exposure and substance abuse, remained the same as in previous years.
The five most common types of poison exposure were benzodiazepines, paracetamol, household products, zopiclone and CHM. According to our previous data, they had remained the five most common poisons exposed since 2011, with benzodiazepines and paracetamol ranking either the first- or second-most common since 2010, each being involved in 8%–10% of all poisoning cases every year. Benzodiazepines had outnumbered paracetamol and remained the most common type of poison involved in all poisoning cases for 4 years since 2016. Paracetamol, being the most common single agent, followed by zopiclone, can be explained by their availability in both over-the-counter and prescription medication. Paracetamol, benzodiazepines and zopiclone were commonly involved in intentional self-harm as a sole poison or co-ingestants. For CHM poisoning, whose rank dropped from the third in 2018 to the fifth in 2019, herb-induced liver injury accounted for around one-third of cases, followed by herb-related renal injury and matrine poisoning. We observed a significant drop in the case number of aconite poisoning from 16 cases in 2018 to only two cases in 2019. Household products were commonly encountered in intentional poisoning in adults as well as accidental exposure in children. Cleansing agents, antiseptics, bleaches and desiccants/oxygen absorbent were the most common poisons involved in household product poisonings.
In this year, the proportion of consultation cases treated with decontamination (16.5%) and antidotes (16.4%) were both higher than that in last year (13.5% and 13.7%, respectively), and also the respective 5-year average figures. Their utilization rates have fluctuated in recent years (Table 5). Concerning the method of decontamination, single-dose AC remained the most common, which is consistent with our local experience and overseas poison centre data.1,2
The HKPIC annual reports important figures in the latest 5 years.
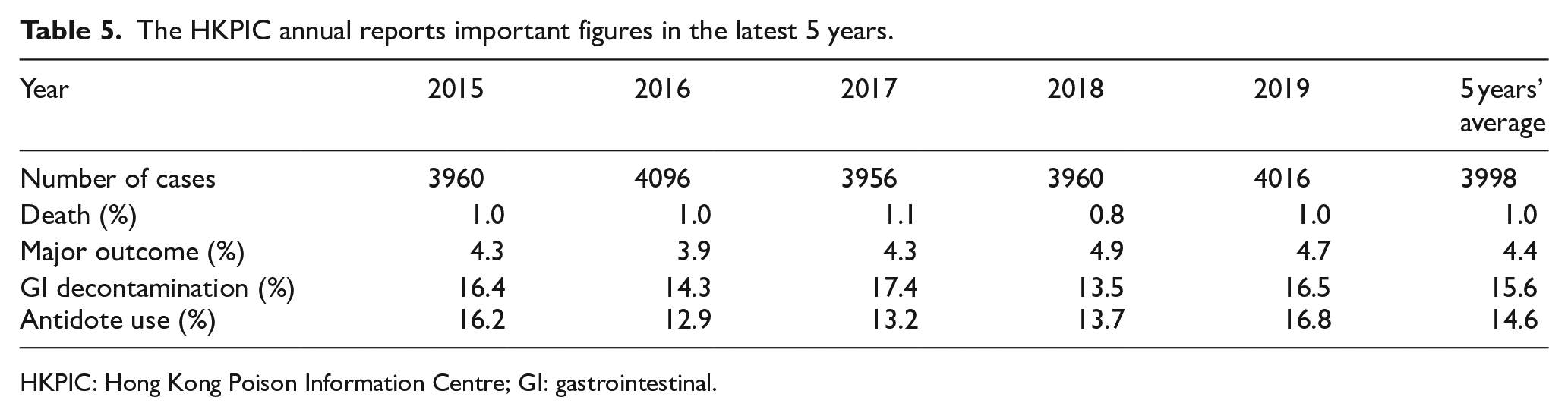
HKPIC: Hong Kong Poison Information Centre; GI: gastrointestinal.
Among all types of antidotes, NAC, benzodiazepines and hyperbaric oxygen (HBO) were the three most frequently used. NAC has been the most common antidote in all of our previous annual reports except in 2008. NAC was administered in around one-fourth of paracetamol poisoning cases. It was also used to treat other poisonings such as amatoxin and paraquat poisoning, although the evidence remains limited. The proportion of benzodiazepine uses (13.3%) was about the same as in previous years except in 2017, when an exceptionally high utilization (22.1%) was recorded and we believe it was an outlying observation. There was a sharp rise in the use of HBO, mainly for patients with carbon monoxide (CO) poisoning, from three cases in 2018 to 46 cases in 2019, making it the third-most common antidote used this year. The reason of such a rise is likely due to the opening of the first public hospital-based hyperbaric oxygen therapy (HBOT) centre, which has started to provide 24/7 services to CO poisoning or other emergency cases since November 2018. Sodium bicarbonate and snake antivenins ranked fourth and fifth most commonly used antidotes. Together with calcium, the pattern of their use was similar compared with that recorded in previous years.
Concerning the clinical outcome, the overall poisoning death rate in 2019 was 1.0%, which was similar to the average rate of 1.0% over the past 5 years (Table 5). The proportion of cases with a major effect was 4.7%, which is comparable with the average rate of 4.4% recorded in recent years. Majority of cases (78.3%) were classified as no effect or mild effect, which again was similar to our previous data.
There are several limitations of this report as in our previous annual reports. First, reporting of poisoning cases in Hong Kong is voluntary. Second, data obtained from the consulting healthcare professionals may not be complete. However, since most poisoning cases are managed in HA hospitals with clinical records accessible in the centralized data repository ePR, the accuracy and amount of information are expected to be much better than data obtained in other poison centres, which may not have direct access to patient records in their managing hospitals. Third, in some of the cases with limited clinical information, it is difficult to establish the causal relationship between poison exposure and the outcome.
Conclusion
This 14th annual report provides the most updated epidemiological information on poisoning in Hong Kong in 2019. It highlights several changes in poisoning demography, decontamination and antidote use as compared with our previous reports. Concerning the outcome, 1.0% and 4.7% of the cases resulted in death and a major outcome, respectively. HKPIC will continue to monitor the poisoning pattern in Hong Kong to facilitate formulation of strategies in local poison control and prevention.
Interesting cases
Case 1 – high-dose intravenous vitamin C
A woman in her 70s with an unknown glucose-6-phosphate dehydrogenase (G6PD) status presented with jaundice, tea-coloured urine and dyspnoea on exertion after receiving intravenous (IV) infusion of vitamin C in a private doctor’s clinic 2 days before admission. Blood tests revealed anaemia with haemogoblin of 7 g/dL, unconjugated hyperbilirubinaemia, low haptoglobin concentration and mild methaemoglobinaemia (8.3% methaemoglobin; normal < 1.5%). According to the patient, she was given IV infusion of 30 g of vitamin C over 2 h as a treatment of left hemifacial spasm. The patient has no known drug allergy and it was the first time she received IV vitamin C. The patient was diagnosed to have haemolytic anaemia and methaemoglobinaemia induced by high-dose vitamin C administration. Her symptoms resolved shortly after blood transfusion. G6PD deficiency was confirmed 5 months later in subsequent blood test.
Vitamin C, also known as ascorbic acid, is an essential nutrient and antioxidant. Despite its widespread use as health supplement by the general population, there are only a few established therapeutic indications. For instance, IV vitamin C 200 mg daily for 7 days is recommended to treat vitamin C deficiency (scurvy). 3 IV vitamin C is also an essential component of the hydrocortisone, ascorbic acid and thiamine (HAT) therapy, an investigational adjunctive therapy for severe sepsis. IV vitamin C 1500 mg given every 6 h, together with hydrocortisone and thiamine, has been reported to be effective in reducing the duration of septic shock. 4 Owing to its antioxidant effect, IV vitamin C has been reported as an alternative treatment of methaemoglobinaemia when standard treatment with IV methylene blue is not available or contraindicated. Up to 10 g every 6 h was given intravenously in a case report with no significant adverse effect. 5 Nevertheless, the use of IV vitamin C for hemifacial spasm is non-conventional and has not been reported in the literature.
The use of vitamin C by non-mainstream physicians was reported to be common. Though controversial, both IV and oral vitamin C are used by complementary and alternative medicine (CAM) practitioners to treat infections, autoimmune diseases, cancers and illnesses of uncertain origin. The reported median dose of IV vitamin C used was 50 g per treatment in a CAM practitioner survey in the United States in 2008. 6 The safety profile of high-dose IV vitamin C has not been established. Although vitamin C is considered to be non-toxic in most oral and IV single acute overdose, 7 there are less than 10 case reports of haemolysis related to high-dose IV vitamin C in the literature related to underlying G6PD deficiency.8–10 The pathological mechanism is not well-established, but it is believed to be related to the oxidant stress generated by high-dose IV vitamin C use in susceptible individuals, for example, patients with G6PD deficiency. This condition has never been reported in oral vitamin C use. Another more commonly reported complication of prolonged high-dose vitamin C use is oxalate crystalluria and the resultant renal impairment. Clinicians should be aware of these complications when vitamin C is used in susceptible individuals.
Case 2 – IV paracetamol
A woman in her 50s, with stage IIIC ovarian cancer, cachexia and a bodyweight of 42 kg, was admitted for intestinal obstruction. Exploration laparotomy was performed, and she was prescribed IV paracetamol 1 g every 6 h and morphine for pain control post-operatively. A total of seven doses of IV paracetamol were given in 2 days. Derangement of her liver function started on day two of IV paracetamol treatment, with alkaline aminotransferase (ALT) 1538 IU/L, aspartate aminotransferase (AST) > 3000 IU/L, bilirubin 42 μmol/L and INR 5.6. Her baseline liver function and clotting profile were normal. Paracetamol level at 28 h after the last IV paracetamol dose was 423 μmol/L. Paracetamol-induced hepatotoxicity was suspected and NAC was started. Viral hepatitis markers were all negative. Ultrasonography of the abdomen revealed suboptimal images, but it showed liver parenchymal change, a right hepatic cyst and gall bladder sludge. Her subsequent liver function improved after NAC treatment. However, the clinical course was complicated with Bacillus bacteraemia despite antibiotic treatment, leading to a progressive downhill course. The patient finally succumbed on post-operation day 25 despite the improvement of ALT to 46 IU/L.
The use of IV paracetamol is gaining popularity locally in recent years, especially for patients who cannot tolerate oral intake or for whom oral intake is not allowed (e.g. peri-operative patients). Paracetamol is generally regarded as safe within the normal therapeutic dose range. When overdosed, it can lead to hepatotoxicity, which can be life-threatening. A peri-operative patient has additional risk factors for developing paracetamol-induced liver toxicity as they are often fasted for a period of time to prepare for surgery or malnourished due to underlying diseases, depleting their body store of glutathione. Overdose of IV paracetamol is commonly reported in the literature as accidental infusion of a 10-fold dose of Perfalgan® (IV preparation that contains 10 mg of paracetamol per mL of solution for infusion) due to dose miscalculation. 11 Repeated supra-therapeutic overdose, on the contrary, is seldom reported.
We hereby report a case of repeated supra-therapeutic overdose of IV paracetamol leading to hepatotoxicity. In addition to fasting, our patient was cachexic and underweight. She was also suffering from long-standing intestinal obstruction leading to malnourishment, which posed an additional risk to paracetamol hepatoxicity. Although she was prescribed with a daily dose of 4 g (1 g every 6 h) IV paracetamol, which is considered a common adult therapeutic dose of oral paracetamol, given the low body weight of 42 kg, it is already higher than the recommended daily maximum dose. It is important to highlight the difference in dose recommendation between IV and oral paracetamol for this specific group of low-body-weight adults (> 33 kg but < 50 kg) to avoid paracetamol toxicity. The recommended maximum daily dose of paracetamol infusion is only 60 mg/kg, without exceeding 3 g, for adults heavier than 33 kg but lighter than 50 kg. 12 This is different from oral paracetamol, for which a maximum daily dose of 4 g is recommended for all adults without specifying the body weight. 13 Therefore, the practice of administering IV paracetamol 1 g every 6 h should be avoided in adults weighing less than 50 kg. This is, in fact, also true for oral paracetamol in adults with a body weight < 50 kg, for whom a lower dose of paracetamol is recommended. Due to the difference in pharmacokinetics, the Rumack–Matthew nomogram is not applicable to IV paracetamol overdose.
Case 3 – nephrotoxic mushroom
A woman in her 50s developed delayed gastrointestinal symptoms 13 h after ingestion of wild mushroom foraged near a hiking path in the East Kowloon region. She presented after having repeated vomiting and diarrhoea for 2 days. On admission, she was found to have liver and renal impairment with serum ALT level at 488 IU/L and creatinine concentration at 300 μmol/L. She was treated in the intensive care unit for suspected Amanita poisoning but her liver function soon improved after admission. However, she developed renal failure and auria, requiring renal replacement therapy over the next 10 days. Nephrotoxic mushroom poisoning became the likely diagnosis, for which there is no known specific antidote. She described the mushrooms as small white mushrooms with a cap, which was collected a little bit further into the trackside she walked. She consumed all the collected mushrooms so that species identification by mycologist could not be performed. Fortunately, her urine output returned after 10 days of admission with rapid improvement of renal function over the week that followed. She was discharged 3 weeks after admission with a creatinine concentration of 156 μmol/L. Her serum creatinine level subsequently returned to normal 6 weeks after mushroom consumption. It was the first case of nephrotoxic mushroom poisoning recorded by HKPIC and probably in Hong Kong.
Two types of nephrotoxic mushroom poisoning have been reported in the literature: the long known one caused by Cortinarius spp. 14 and the other by Amanita spp. 15 Although the existence of the former has been documented in Hong Kong, 16 the clinical presentation of our patient, characterized by initial moderate liver enzyme elevation and rapid-onset but reversible anuric renal failure, was more compatible with nephrotoxic Amanita mushroom poisoning. Nephrotoxic Amanita poisoning had been reported in other parts of the world as well as in South China where at least six Amanita species have been identified as the culprit. The toxic mechanism has not been well studied. Toxic amino acids capable of inducing renal epithelial cell necrosis have been proposed as the cause. Currently, no confirmatory laboratory tests and no specific treatment are available for the condition. The local existence of another organ-toxic mushroom in addition to the hepatotoxic Amanita spp. speaks strongly against consumption of wild mushrooms. The public should be warned that in addition to liver failure, renal failure is another risk associated with eating locally gathered wild mushrooms.
Case 4 – button battery
A 3-year-old boy was brought to a hospital for epigastric pain after swallowing several button batteries at home. Abdominal radiography confirmed the presence of three roundish metallic foreign bodies of around 9 mm in diameter in the epigastrium compatible with button batteries. There were no signs of bowel perforation or obstruction. Emergency oesophago-gastro-duodenoscopy (OGD) performed showed no foreign bodies or mucosal abnormalities down to duodenum. Mini-laparotomy and small bowel enterotomy were performed with successful removal of three intact button batteries from the small bowel.
Button batteries ingestion is a potentially fatal surgical emergency, which can lead to gut wall necrosis, perforation and fistula with adjacent organ structure. In vitro studies have demonstrated the electric current from the swallowed batteries can result in the formation of hydroxide radicals from water, which can then lead to alkaline burn. Necrosis within the esophageal lamina propria can occur as soon as 15 min after ingestion with extension to the outer muscular layer within 30 min. A large review on 8600 human cases of button batteries ingestion reported 13 deaths and a major complication rate of 0.8%. 17 Reported complications included tracheoesophageal fistula, oesophageal perforation, recurrent laryngeal nerve injury, severe gastric erosion and aortoenteric fistula. Emergency removal of button battery in the oesophagus and stomach is recommended and it should also be considered for all symptomatic patients regardless of the site of location in the bowel. In vitro studies have demonstrated the protective effect of honey and sucralfate suspension for button battery–induced oesophageal injury. 18 HKPIC now recommends repeated oral sucralfate suspension within 12 h of ingestion prior to removal of button battery lodged in the oesophagus.
Case 5 – yew (紅豆杉)
A man in his 50s attended the emergency department for back and lower limbs pain after taking a wine claimed to be prepared from yew tree (紅豆杉). The wine was prepared by his friend in mainland China and he took around 20 mL of the wine around 30 min before symptom onset. He appeared dehydrated, with a blood pressure 97/72 mmHg, pulse rate 98/min, SpO2 97% on room air and temperature of 38.8 °C. Blood tests revealed leukocytosis with a white cell count of 25.8 × 109/L and an absolute neutrophil count of 22.7 × 109/L. Serum creatinine was 139 μmol/L, urea 8.8 mmol/L, creatine kinase 1609 U/L, high-sensitivity troponin I 1609 ng/L (reference ⩽ 34.2 ng/L). He later developed respiratory distress, and a chest X-ray showed progressive pneumonitis around 30 h after wine consumption. His renal function deteriorated and creatinine level peaked at 614 μmol/L. His condition gradually improved with sustained low-efficiency diafiltration (SLEDf) and corticosteroids. Toxicology analysis of the wine showed the presence of paclitaxel and baccatin III (a marker for a yew tree), and baccatin III was found in the patient’s urine.
Consumption of yew products has been deliberately but falsely promoted for cancer prevention. 19 All parts of a yew tree (Taxus spp.) are potentially toxic (except the fleshy red part of the aril) and contain taxine alkaloids as the main toxic ingredients. Most patients had no symptoms or mild poisoning with nausea and vomiting after accidental exposure to Taxus species. 20 Significant poisoning may result in cardiotoxicity with bradycardia, hypotension, ventricular tachycardia and ventricular fibrillation. Taxine B is believed to have the greatest cardiac toxicity, which involves the elevation of cytoplasmic calcium in cardiac myocytes with sodium and calcium antagonism, increasing atrioventricular (AV) conduction time and QRS duration. 21 In addition, taxine B causes a marked reduction in the maximum depolarization rate of action potential in isolated papillary muscle and, thus, resembles the action of class I antiarrhythmic drugs. 22 Progressive neurological symptoms, often leading to coma, may also occur. 22 Yew trees, especially the Pacific yew (Taxus brevifolia), also contain paclitaxel. Paclitaxel is a chemotherapeutic agent that inhibits microtubule disaggregation, thereby blocking mitosis. Some of the adverse effects of paclitaxel include hypersensitivity reactions, neutropenia and pulmonary toxicity with interstitial pneumonitis. 23 Interstitial pneumonitis can develop within days to weeks of receiving paclitaxel, or it may arise later in the course of therapy. Both direct paclitaxel toxicity and an immune mechanism have been proposed in the development of paclitaxel-associated interstitial pneumonitis. 24
Natural products are often perceived as safe by the public without recognizing the potential toxicity. Since most chemotherapeutic agents have a narrow therapeutic index, using a chemotherapeutic agent intended for cancer treatment as an agent for cancer prevention is a dangerous practice and may cause significant poisoning.
Case 6 – ‘needleless wrinkle reduction’ (霧化除皺)
A woman in her 50s presented with facial asymmetry, neck muscle weakness and difficulty in breathing for 1 week. She had a cosmetic procedure, claimed to be ‘needleless wrinkle reduction’ (霧化除皺), in a beauty centre in Hong Kong 9 days before. It was said to be a needleless administration of collagen, hyaluronic acid, active peptides and telomerase, to her face and both sides of the neck. She noticed difficulty in swallowing, neck muscle weakness and facial asymmetry 3 days after the procedure. Her symptoms had remained static over the week. On physical examination, her vital signs were stable with no respiratory insufficiency. There was muscle weakness on the right side of the face and neck flexors. Adverse drug reaction from botulinum toxin was diagnosed clinically and the incidence was notified to the Department of Health for further investigation. She was treated conservatively with observation as the patient’s condition had been static for 1 week already with no respiratory muscle weakness. The muscle power gradually improved and was near normal 20 weeks after the initial attendance. Toxicology analysis showed the presence of botulinum neurotoxin A in a bottle of powder and lidocaine in one of the bottles of liquid used in the cosmetic procedure.
Botulinum toxin A has been used off-label for cosmetic purposes to reduce wrinkles on the face and neck. 25 It has to be administered by a registered medical practitioner in Hong Kong. Adverse drug reaction to botulinum injection usually begins within 2–3 days of injection and is localized at the site of injection with adjacent muscle weakness. 26 The use of unlicensed botulinum toxin products in beauty centres has been associated with significant adverse reactions, including dysphagia and respiratory muscle weakness, necessitating the use of botulinum antitoxin in both mainland China and Hong Kong.27,28 Needleless or needle-free injection of drugs, for example, botulinum toxin for the treatment of hyperhidrosis 29 and insulin for diabetes mellitus, 30 have become more popular. It was based on the principle of pressure jets that push the liquid from the micropores and penetrate through the skin to the subcutaneous tissue with a spray-like diffusion. 29 To our knowledge, this is the first reported case of botulinum toxin poisoning from the needleless route of administration.
CO poisoning outbreak
In March 2019, there was an outbreak of CO poisoning in a private dance party involving more than 100 people inside a ballroom of 1200 square metres due to malfunctioning of the exhaust system in the kitchen. There were 32 patients in total, including waiters and chefs, and 14 cases were reported to our Centre by four hospitals. Their age ranged from the 30s to 70s with a male to female ratio of 1 to 2.5. Most of them presented to AED shortly afterward, with two presenting late by more than a day after the incident. All of them complained of dizziness at the scene. Other reported symptoms included breathing difficulty, headache, chest discomfort, palpitation, nausea and vomiting. Four of them had transient loss of consciousness, among whom two were the chefs who collapsed in the kitchen. All patients were fully conscious upon arrival to AED with normal vital signs and oxygen saturation. Initial carboxyhaemoglobin (COHb) level within 6 h of the incident ranged from 5.2% to 34%. Two of them received HBOT, while the others were given normobaric oxygen therapy. All patients were discharged subsequently but two reported memory impairment with features of anxiety or depression in subsequent follow-up.
The outbreak of accidental CO poisoning is a recurring problem in Hong Kong. Indoor areas using fuel-burning appliances (e.g. food premises) with poor ventilation are at risk. Early symptoms of CO poisoning are often non-specific, including dizziness, nausea, headache and tiredness. CO is colourless and odourless, and it is often unnoticed until patients start to develop more severe symptoms such as loss of consciousness. A high index of suspicions is necessary, especially in scenarios involving an indoor combustion source, and early measurement of the COHb level helps confirm the diagnosis. Besides public health education and control measures, the installation of CO detectors in high-risk places may improve early detection of this ‘silent killer’ and prevent accidental CO poisoning. 31
Tear gas
From June to December 2019, HKPIC recorded 55 cases related to tear gas exposure, including 37 reporting cases from local AEDs and 18 consultation cases. The median age of the exposed patients was 27 years and the male to female ratio was 1:1.1. For the 37 reporting cases from local AEDs, the clinical presentation was related to the acute effects of tear gas exposure. The most common presenting symptoms included respiratory tract irritation with cough and dyspnoea (73%), skin and eyes irritation (30%) and associated injuries (16%). Thirty-five out of 37 cases were directly discharged from AEDs after treatment. Two cases required short duration of in-patient observation. The clinical outcome of all patients ranged from mild to moderate severity.
Among 18 consultation cases, 13 patients were journalists referred to HKPIC out-patient toxicology clinic for assessment of persistent symptoms after tear gas exposure. All these cases had repeated tear gas exposure because of their occupation. Persistent cough was the chief complaint in 54% of cases. The clinical presentation was compatible with bronchial hyper-responsiveness and all cases improved after termination of exposure and symptomatic treatment. Increased bowel movement with loose stool and diarrhoea was also a common chief complaint, which was present in 54% of cases. The gastrointestinal symptoms were self-limiting, which typically lasted for several days after each exposure. All cases improved after termination of exposure and medical treatment was not required. Other reported symptoms included urticaria, headache, decrease menstrual flow, flare-up of allergic rhinitis, eyes tearing, throat discomfort, insomnia and decreased appetite. No long-term complication was observed at the time of writing and all cases were discharged from out-patient clinical follow-up.
Tear gas is a riot control agent typically containing o-chlorobenzalmalononitrile, code named CS. After dermal or inhalational exposure, it causes intense local irritation and temporarily disables the exposed individual. Mucosal and skin irritation cause pain over the eyes, nose, mouth, throat, airway and exposed skin area. It causes excessive tearing, difficulty in eye opening, coughing and sensation of breathing difficulty. These symptoms generally diminish within 30 min after exposure. Vomiting, abdominal pain and diarrhoea may also result from swallowing tear gas particles in respiratory secretions. Some patients develop persistent symptoms that may last for several weeks due to sensitization of the airway. Infants or patients with underlying respiratory disease, for example, asthma, may develop life-threatening exacerbation after exposure.
The mainstay of management after tear gas exposure includes termination of exposure and surface decontamination with copious amount of water (with soap, if available). As the symptoms are usually self-limiting, most patients do not require medical treatment after tear gas exposure.
Footnotes
Authorship
We certify that we have each made a substantial contribution so as to qualify for authorship and that we have approved the contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was previously applied for our annual report and judged to be not required by the Research Ethics Committee (Kowloon Central/Kowloon East).
Informed consent
Since this is an annual report with no patient contact and intervention involved, written informed consent was considered not necessary by our institution and no patient identifiable data have been included in the manuscript. Our previous annual reports were also published in this journal without informed consent.