
Abstract
A 50-year-old man with history of type II diabetic mellitus attended the emergency department with persistent foreign body sensation after swallowing a drug pill. He also had mild odynophagia. Tracing his history, it was found that he had progressive dysphagia in previous 2 months. There was no coughing or choking immediately after swallowing the pill and speech quality was normal. He denied weight loss in last 6 months. On physical examination, no palpable mass or thyroid goiter was noted. Laboratory data were in acceptable range. A point-of-care ultrasound with a linear probe over the patient’s neck was done. Later, computed tomography was done for confirming the diagnosis.
Case report
A 50-year-old man with history of type II diabetic mellitus attended the emergency department with persistent foreign body sensation after swallowed drug pill. He also had mild odynophagia. Tracing his history, it was found that he had progressive dysphagia in previous 2 months. There was no coughing or choking immediately after swallowing the pill and speech quality was normal. He denied body weight loss in last 6 months. On physical examination, no palpable mass or thyroid goiter were noted. Laboratory data were in acceptable range. On physical examination, no palpable mass or thyroid goiter was noted. Laboratory data were in acceptable range. A point-of-care ultrasound (POCUS) with a linear probe over the patient’s neck was done (Figure 1, and Video 1). Later, computed tomography (CT) was done for confirming the diagnosis (Figure 2).
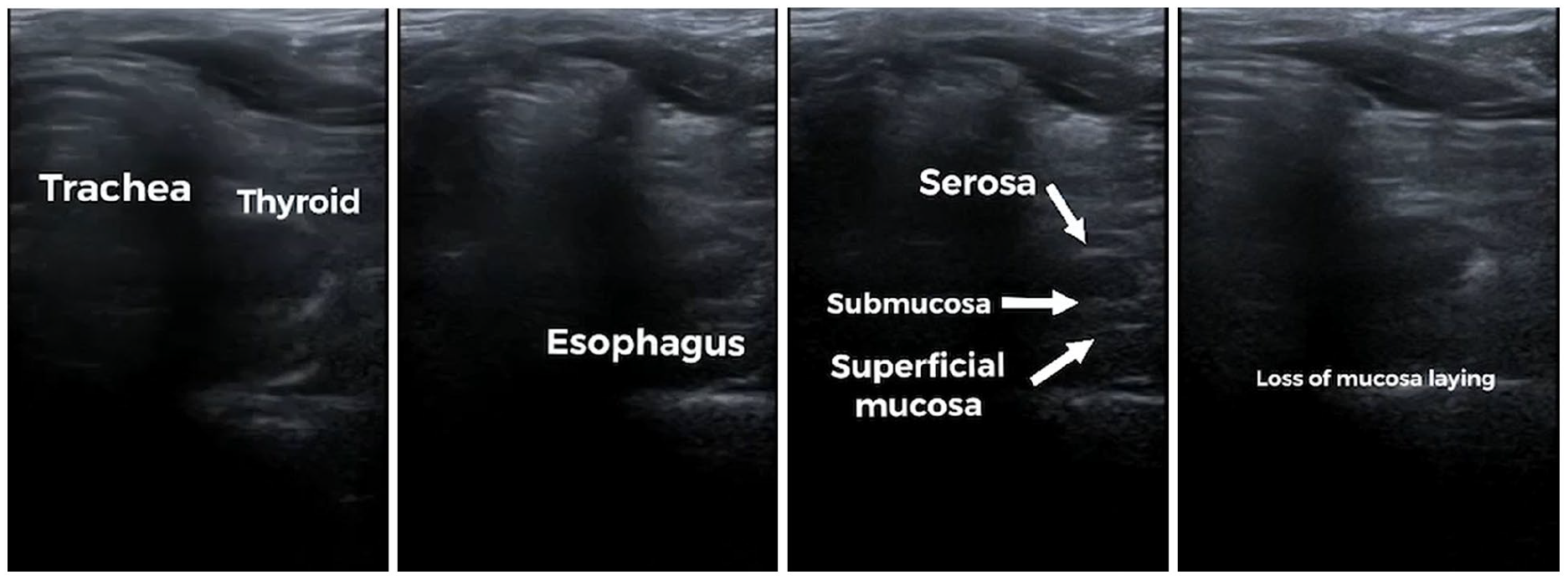
Bedside point-of-care ultrasonography demonstrates the layout of the cervical esophagus between the trachea and vertebrae. A hypoechoic lesion with loss of normal gut signature over the cervical esophagus is seen.
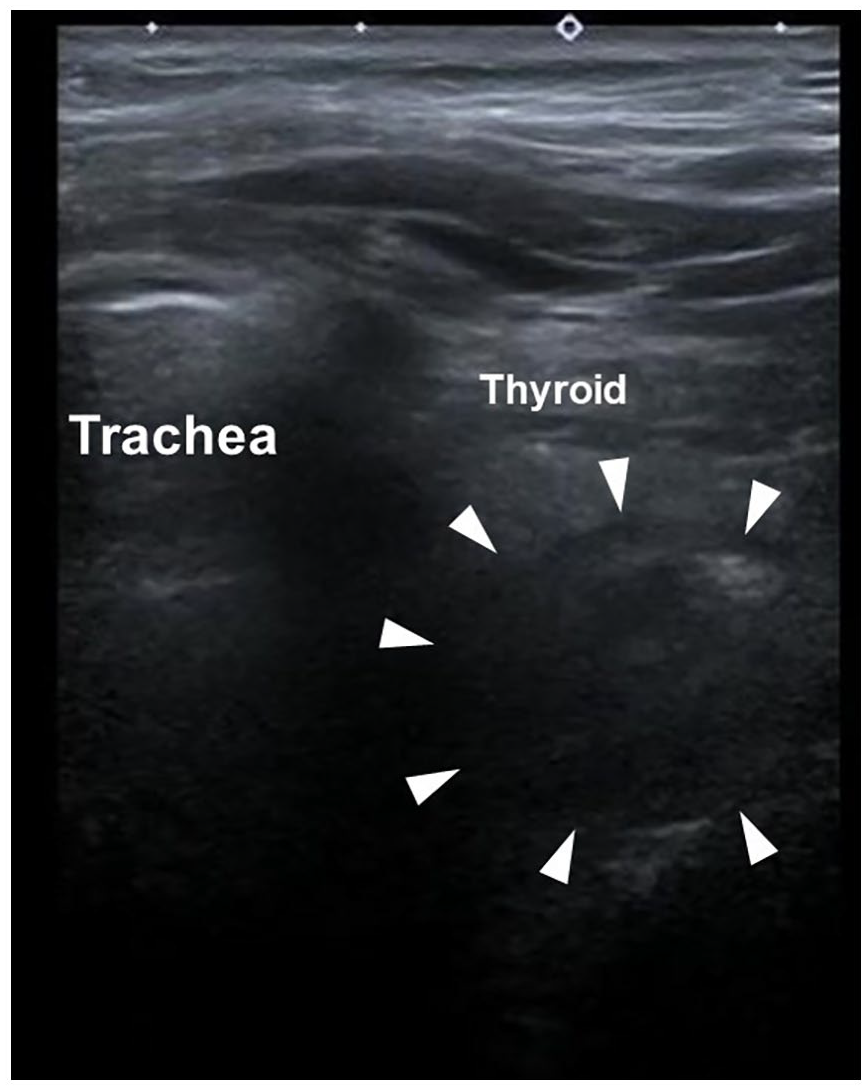
Point-care-of-ultrasound with linear probe: transverse view of the left neck at the level of the thyroid showing a hypoechoic lesion (arrowhead) with loss of normal gut signature over the cervical esophagus.
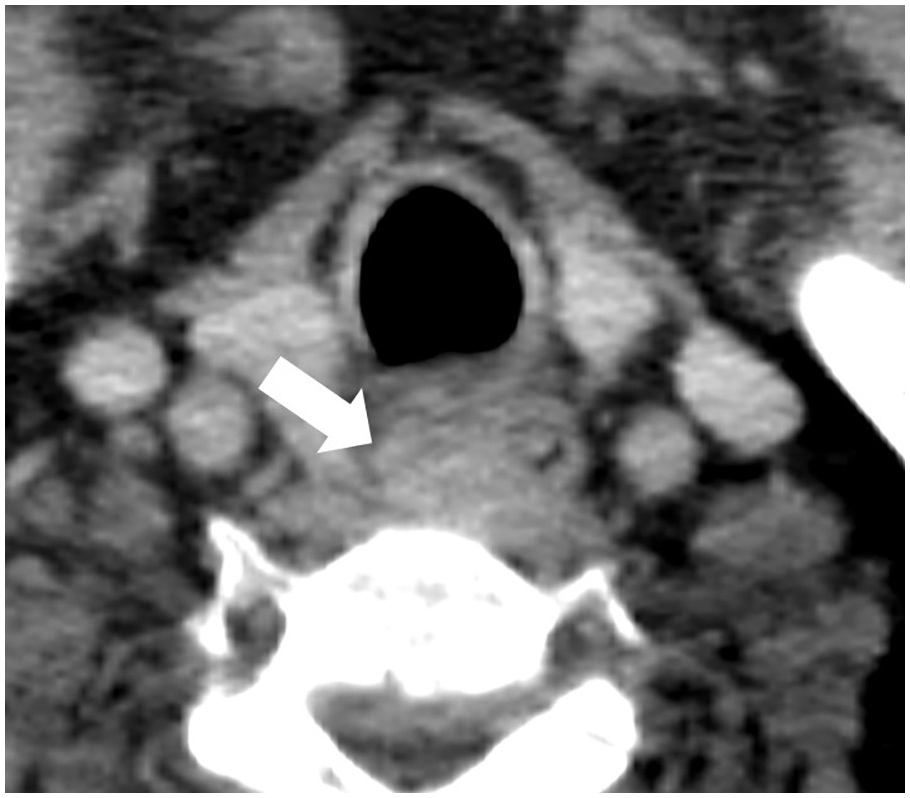
A 2.5 cm × 1.7 cm soft-tissue lesion (arrow) is observed at the most proximal part of the cervical esophagus.
Question
Please describe the POCUS finding.
What are the differential diagnoses of acute dysphagia and which of them is the most concerning in this case?
Answer
The cervical esophagus located left of the trachea, starting from the left lower lobe of the thyroid. It is a tubular structure with wall thickening < 3 mm and the typical layer structure (Figure 3). A hypoechoic lesion with loss of normal gut signature over the cervical esophagus.
Food impaction is the most common cause for acute onset of dysphagia in adults. In this case, foreign body sensation developed suddenly after swallowing a drug pill. In the setting of dysphagia for 2 months and relatively small size of pills, underlying structural anomaly should be considered and POCUS can aid evaluation of underlying pathology of cervical esophagus. The disruption of the layers is the most common presentation of a malignancy.
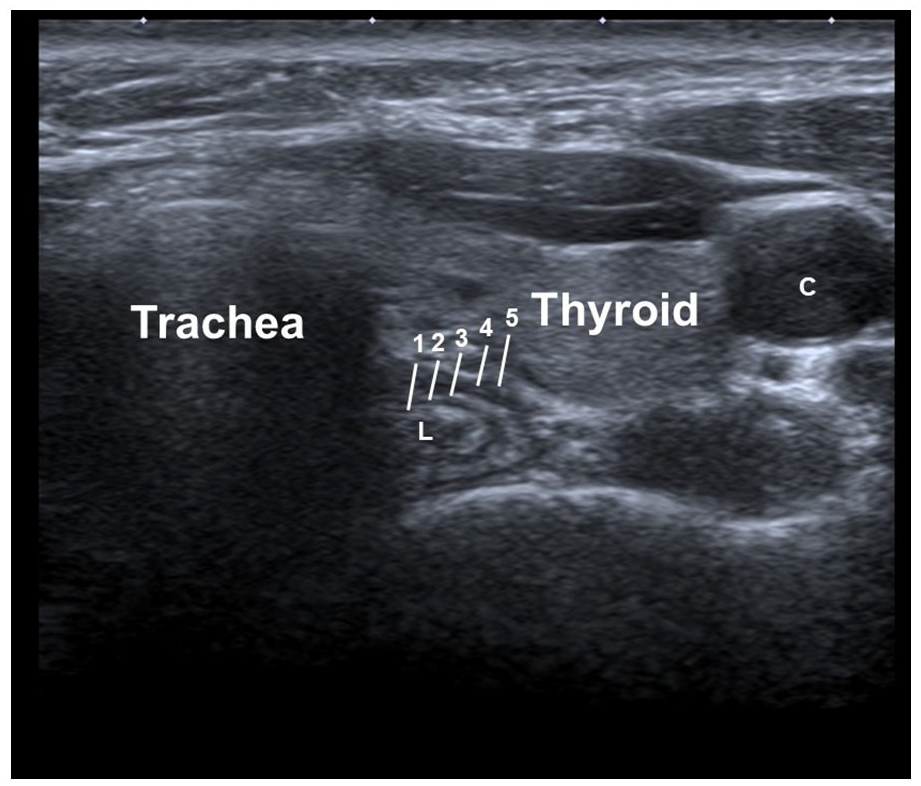
Normal cervical esophagus of transverse cut. C, left common carotid artery; 1, submucosa; 2, inner circular layer of muscle; 3, connective tissue between the circular and longitudinal muscle layers of the muscularis propria; 4, outer longitudinal layer of muscle; and 5, adventitia.
CT (Figure 2) revealed a 2.5 cm × 1.7 cm soft-tissue lesion in the most proximal part of the cervical esophagus, corresponded with POCUS image. The patient was diagnosed with esophageal cancer after endoscopic biopsy and received the neoadjuvant concurrent chemoradiotherapy followed by surgery.
Discussion
Foreign body (FB) sensation is a common complaint in emergency department. Most common from food origin, especially fish or fragmented bone. Food impaction is the most common cause for acute onset of dysphagia in adults, may present with foreign body sensation. FB obstruction and food bolus impaction most often occur at sites of narrowing or angulation, due to natural anatomy or underlying esophageal pathology that disrupts normal passage. Etiologies associated with esophageal impaction including benign etiology, esophageal malignancy, extrinsic compression, and esophageal motility disorder. 1 Most ingested foreign bodies pass through the esophagus and gastrointestinal system without harm, although 10%–20% will require intervention.
Due to the relative superficial location of the cervical esophagus, POCUS is a useful, quick, safe and simple tool for evaluating patients with dysphagia and foreign-body sensation. The cervical esophagus is detectable to the left of the trachea, starting from the left lower lobe of the thyroid. It is a tubular structure with wall thickening < 3 mm and the typical layer structure. 2 The esophageal foreign body can be detected by POCUS with little added risk or cost. Direct visualized esophageal foreign body is possible and indirect sign of esophageal foreign body including esophageal dilatation, hyperechoic or hypoechoic lesion with mixed echogenic contents in food or secretion, and no change with swallowing efforts. 3
The cervical esophagus wall usually appears to be composed of 5 layers, although 7 layers can also be seen in some cases in cadaveric study, especially as the transducer frequency is increased. 4 The innermost layer is hyperechoic and corresponds to the superficial mucosa. The next layer is hypoechoic and corresponds to the deep mucosa and muscularis mucosae. The third layer is again hyperechoic and corresponds to the submucosa and its interphase with the muscularis propria. The next layer is hypoechoic and corresponds to the muscularis propria and the final fifth layer is hyperechoic and corresponds to the adventitia. The disruption of the layers is the most common presentation of a malignancy. 5 Differential diagnosis may include severe corrosive injury or severe inflammatory bowel disease, rarely.
In this case, foreign body sensation developed suddenly after swallowing a drug pill. In the setting of dysphagia for 2 months and relatively small size of pills, underlying structural anomaly should be considered and POCUS can aid evaluation of underlying pathology of cervical esophagus.
Footnotes
Acknowledgements
To ensure the language is clear and free of errors, English editing was performed by Editage, a division of Cactus Communication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the patient included in the study. There’s no patient identifiable information in the study.