
Abstract
Background:
The Korean Ministry of Health and Welfare decided to establish a trauma medical service system to reduce preventable deaths. OO hospital in Gangwon Province was selected as a regional trauma center and was inaugurated in 2015.
Objectives:
This study examines the impact of this center, comparing mortality and other variables before and after inaugurating the center.
Methods:
Severely injured patients (injury severity score > 15) presenting to OO hospital between January 2014 and December 2016 were enrolled and categorized into two groups: before trauma center (n = 365) and after trauma center (n = 904). Patient characteristics, variables, and patient outcomes (including mortality rate) before and after the establishment of trauma centers were compared accordingly for both groups. Risk factors for in-hospital mortality were also identified.
Results:
Probability of survival using trauma and injury severity score (%) method was significantly lower in the after trauma center group (81.3 ± 26.1) than in the before trauma center group (84.7 ± 21.0) (p = 0.014). In-hospital mortality rates were similar in both groups (before vs after trauma center group: 13.2% vs 14.2%; p = 0.638). The Z and W statistics revealed higher scores in the after trauma center group than in the before trauma center group (Z statistic, 4.69 vs 1.37; W statistic, 4.52 vs 2.10); 2.42 more patients (per 100 patients) survived after trauma center establishment.
Conclusion:
Although the mortality rates of trauma patients remained unchanged after the trauma center establishment, the Z and W statistics revealed improvements in the quality of care.
Introduction
The trauma-related preventable mortality rate in Korea gradually decreased from 50.4% in 1998 to 32.6% in 2007 with the development of an emergency medicine medical center system. 1 However, the latest reported preventable mortality rate in trauma patients (from 2012) was 35.2%, 2 which remained high, compared with other Organization for Economic Co-Operation and Development countries.
Studies regarding preventable mortality in Korea showed that most preventable deaths occurred during the hospital stage.1,2 They also suggested that specialized trauma centers and fast decision-making by dedicated trauma care teams are essential for reducing preventable deaths during the hospital stage.
In consideration of these issues, the Korean Ministry of Health and Welfare (KMHW) established a trauma medical service system. The main goal of the system is to reduce the preventable trauma mortality rate to less than 20% by 2020. KMHW planned to train and support trauma surgeons and to build 17 regional trauma centers by 2016. Therefore, KMHW invited medical institutions to apply to be regional trauma centers in 2012, and five hospitals, including OO Hospital, have been selected.
OO hospital started constructing a regional trauma center building from governmental funding in 2012, and opened its regional trauma center in 2015.
Gangwon province is characterized by transportation obstacles because of its primarily mountainous topography, and the injury severity of trauma patients in Gangwon province is relatively high compared with the severity in other provinces of the Korean peninsula. According to the 2011 annual report of the Korean Emergency Medical Service, the percentage of severely injured trauma patients (injury severity score (ISS) > 15) with an arrival time in the emergency department (ED) after injury of >1 h was 64.6% for all of Korea and 71.8% for Gangwon province. In addition, the mortality rate for severely injured trauma patients in Gangwon province was 5.2%, which was higher than in other provinces (Seoul, 1.2%; Gyeonggi, 2.1%; Gyeongbuk, 2.5%). 3
Based on the above statistics, regional trauma centers might be particularly important in Gangwon province, and indeed, there have been high expectations that they play a crucial role. However, it is unknown whether these expectations have been met. Therefore, the aim of the current study was to address this issue by comparing physiological characteristics, as well as variables and patient outcomes expected to improve with trauma center implementation (including mortality rates), of severely injured patients treated at a regional trauma center in Gangwon province before and after opening the center. Risk factors associated with in-hospital mortality were also identified.
Materials and methods
Patient selection
This study retrospectively analyzed data from trauma patients admitted via the ED at OO hospital during a 3-year period from January 1, 2014, through December 31, 2016. A total of 9103 trauma patients presenting to the ED were initially identified, with 2187 trauma patients excluded using the following criteria to compare severely injured trauma patients before and after the establishment of the trauma center: (1) dead on arrival, (2) discharged hopelessly, (3) discharged to home, (4) voluntarily discharged or transferred to another hospital from the ED, (5) iatrogenic injury, (6) self-inflicted hanging injury, and (7) under 18 years of age. Of the 6916 patients remaining after applying the exclusion criteria, 1269 with severe trauma (ISS > 15) were selected for inclusion in the study.
As this study focused on comparing data before and after 2015 (when the regional trauma center was established), the patients were divided into two groups: before trauma center and after trauma center. Each patient’s basic characteristics, ISS, revised trauma score (RTS), trauma and injury severity score (TRISS), injury mechanism, injury site (with an Abbreviated Injury Scale (AIS) severity score > 3), time from injury to ED arrival, and time to decision regarding admission were recorded. For all patients, we also recorded whether they were transferred from another hospital or triggered trauma team activation (TTA), as well as the results of decision making (e.g. admission to ward, admission to trauma intensive care unit (TICU), discharge). In-hospital mortality rates was recorded and analyzed as direct patient outcomes.
OO hospital regional trauma center
OO hospital is a tertiary general hospital with 1000 beds covering the western part of Gangwon province. Before the establishment of the trauma center, trauma and non-trauma patients shared the same rooms in the intensive care unit (ICU) and general wards. After the establishment of the trauma center, the trauma center had its own building, which could only be used by trauma patients. The OO regional trauma center building, as part of the Korean government project, consists of a trauma resuscitation room with two beds on the first floor; a general trauma ward with 40 beds on the second floor; a TICU with 20 beds and two operating rooms, including one hybrid operating room, on the third floor; and a helipad on the roof of the building. In 2015, a team dedicated to caring for trauma patients was created, which comprised seven general surgeons, two cardiothoracic surgeons, two neurosurgeons, two orthopedic surgeons, and three emergency medicine physicians. Trauma physicians dedicated to caring for trauma patients received their salaries from the government and were not allowed to provide any services to non-trauma patients under the KMHW regulations. Since its establishment, the KMHW conducts inspections of each regional center’s equipment, personnel, and operation once every 3–4 months. The role of the regional trauma center includes the following: carrying out trauma-related education, performing quality improvement activities, holding panel discussions for mortality case reviews, and holding regular regional trauma committee conferences. With the National Trauma Data Bank of the United States as a benchmark, the KMHW developed the Korean Trauma Data Bank (KTDB) with the intention that each regional trauma center collects the trauma-related variables determined by KMHW in their trauma registry system and sends them to KTDB. In order to perform these tasks, the regional trauma center’s registrar and coordinator workforce was funded by the KMHW.
Patient transportation
In cases of ground transportation, the trauma patient should be transported from the incident site to the nearest available primary care facility following the guideline of the 119 rescue team by the fire department themselves. Interhospital transportation was performed when further evaluation and treatment were required after primary care was completed in the hospital where the first transfer was made. In 2013, a hospital-based helicopter emergency medical service was introduced in our hospital, and it has been in continuous operation until now. The decision regarding helicopter transportation in case of major trauma patients was made through a hotline communication between the hospital and the fire department or between the hospital and the referring hospital. Since 2015, all severely injured patients transported to a regional trauma center were expected to have definitive care and not allowed transfer to other hospitals.
Treatment process for the trauma patients
Emergency medicine physicians started their initial management according to the advanced trauma life support guidelines when the severely injured trauma patients visited the ED. Simultaneously, it is the responsibility of the emergency medicine physicians on duty to decide whether to trigger TTA according to the TTA criteria (Appendix 1). When the trauma team was activated, a text message containing brief patient information (hospital number, name, age, sex, vital signs, vectors, and symptoms) was sent to all trauma team members. The trauma physicians on duty who received the text message must initiate the examination and treatment within 10 min of TTA, according to a rule established by the KMHW. Since the establishment of the trauma center, there has always been a trauma team, including at least a general surgeon, neurosurgeon, cardiothoracic surgeon, and orthopedic surgeon on duty daily. For trauma patients who meet the TTA criteria, extended focused assessment with sonography for trauma and trauma series (cervical spine, lateral view; chest, anteroposterior view; and pelvis, anteroposterior view) X-ray were performed immediately, and the decision to perform computed tomography was made by the trauma physicians on duty. For trauma patients requiring massive transfusion due to massive hemorrhage, it is the responsibility of the trauma physicians on duty to decide whether transfusion should be started according to a massive transfusion protocol. When the trauma physicians decided to perform massive transfusion, two no-matched packed red blood cells were transfused following a massive transfusion protocol within 30 min of the trauma patient’s visit. In addition, these trauma patients received a loading dose (1 g) of tranexamic acid, which is administered over 10 min, followed by an intravenous administration of 1 g with 100 mL bag of 0.9% normal saline over 8 h. 4 This decision was made by the trauma physicians on duty when the patient visited the ED within 3 h after the incident.
Statistical analysis
Data are shown as mean ± standard deviation, unless indicated otherwise. SPSS version 18.0 (SPSS Inc., Chicago, USA) was used for statistical analysis. The chi-square test and Fisher’s exact test were used to compare categorical variables, and Student’s t-test was used to compare continuous variables. Logistic multiple regression analysis was used to identify factors associated with in-hospital mortality. The significance level was set at a p-value < 0.05.
Z and W statistics were calculated to compare predicted and actual patient deaths between the before trauma center and after trauma center groups. The Z statistic was used to compare the mortality of the sample population with the Major Trauma Outcome Study (MTOS)-Predicted mortality, to determine whether the outcomes in the sample population were significantly better, unchanged, or worse than the predicted mortality. The W statistic measures the number of unexpected survivals or death per 100 patients. 5
Results
Patient characteristics
The before trauma center group contained 365 patients and the after trauma center group contained 904 patients. A total of 2108 patients meeting the inclusion criteria were admitted to the OO hospital regional trauma center in 2014; of these, 595 triggered TTA and 365 had an ISS > 15 (Figure 1). The total number of patients meeting the inclusion criteria in 2016 was 2438; of these, 1141 triggered TTA and 469 had an ISS > 15. The total number of patients and the number with an ISS > 15 gradually increased each year (Figure 1).
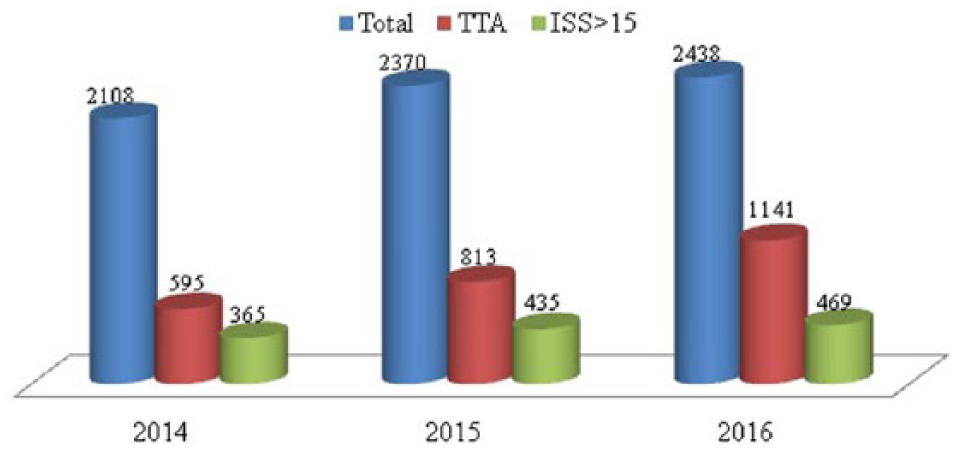
Total number of admissions, number of patients triggering TTA, and number of patients with an injury severity score > 15 in 2014–2016.
The general characteristics of both groups are summarized in Table 1. Probability of survival using TRISS (%) method was significantly lower in the after trauma center group (81.3 ± 26.1) than in the before trauma center group (84.7 ± 21.0) (p = 0.014).
General characteristics of both groups.
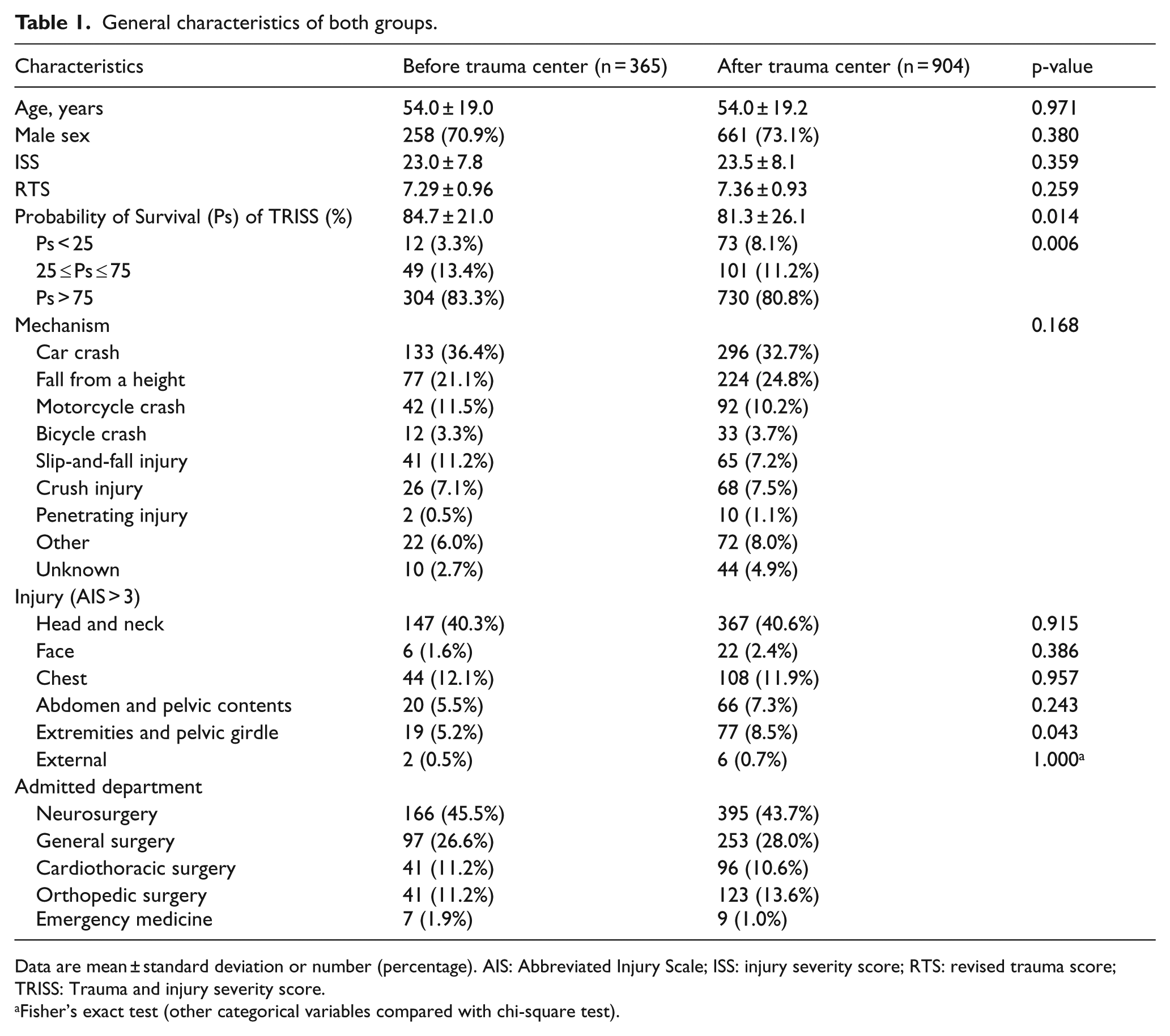
Data are mean ± standard deviation or number (percentage). AIS: Abbreviated Injury Scale; ISS: injury severity score; RTS: revised trauma score; TRISS: Trauma and injury severity score.
Fisher’s exact test (other categorical variables compared with chi-square test).
Variables and outcomes after the establishment of the trauma center
The frequency of TTA was higher in the after trauma center group (84.5% (764)) than in the before trauma center group (75.1% (274)) (p < 0.001). The percentage of TICU admission was similar in both groups (before vs after trauma center group: 74.0% (270) vs 76.8% (694); p = 0.291). The percentage of patients with time from injury to ED arrival <1 h was similar in both groups (before vs after trauma center: 32.3% (118) vs 28.2% (255); p = 0.145) (Table 2). The percentage with an ED arrival time from injury <3 h was also similar in both groups (before vs after trauma center: 64.1% (234) vs 61.0% (551); p = 0.294). The percentage of patients transferred from another hospital did not differ between groups (before vs after trauma center: 50.4% (184) vs 53.3% (481); p = 0.357). The percentage of patients with admission decisions in <1 h after ED arrival was significantly higher in the after trauma center group (before vs after trauma center: 24.4% (86) and 51.8% (455); p < 0.001). Likewise, the percentage of patients with admission decisions in <3 h after ED arrival was significantly higher in the after trauma center group (before vs after trauma center: 77.0% (274) and 88.5% (777); p < 0.001). The in-hospital mortality rates were similar in both groups (before vs after trauma center: 13.2% (48) vs 14.2% (128); p = 0.638). Significant differences between groups in deaths due to hemorrhage (before vs after trauma center group: 2.7% (10) vs 3.1% (28); p = 0.735), sepsis and multiple organ dysfunction syndrome (before vs after trauma center group: 3.0% (11) vs 3.4% (31); p = 0.708), and deaths due to severe brain injury (6.6% (24) vs 7.1% (64); p = 0.749) were not noted. The Z and W statistics revealed significantly higher scores in the after trauma center group than in the before trauma center group (Z statistic, 4.69 vs 1.37; W statistic, 4.52 vs 2.10); 2.42 more patients (per 100 patients) than before survived after the trauma center establishment (Table 2).
Process of care and outcomes after establishment of the trauma center.
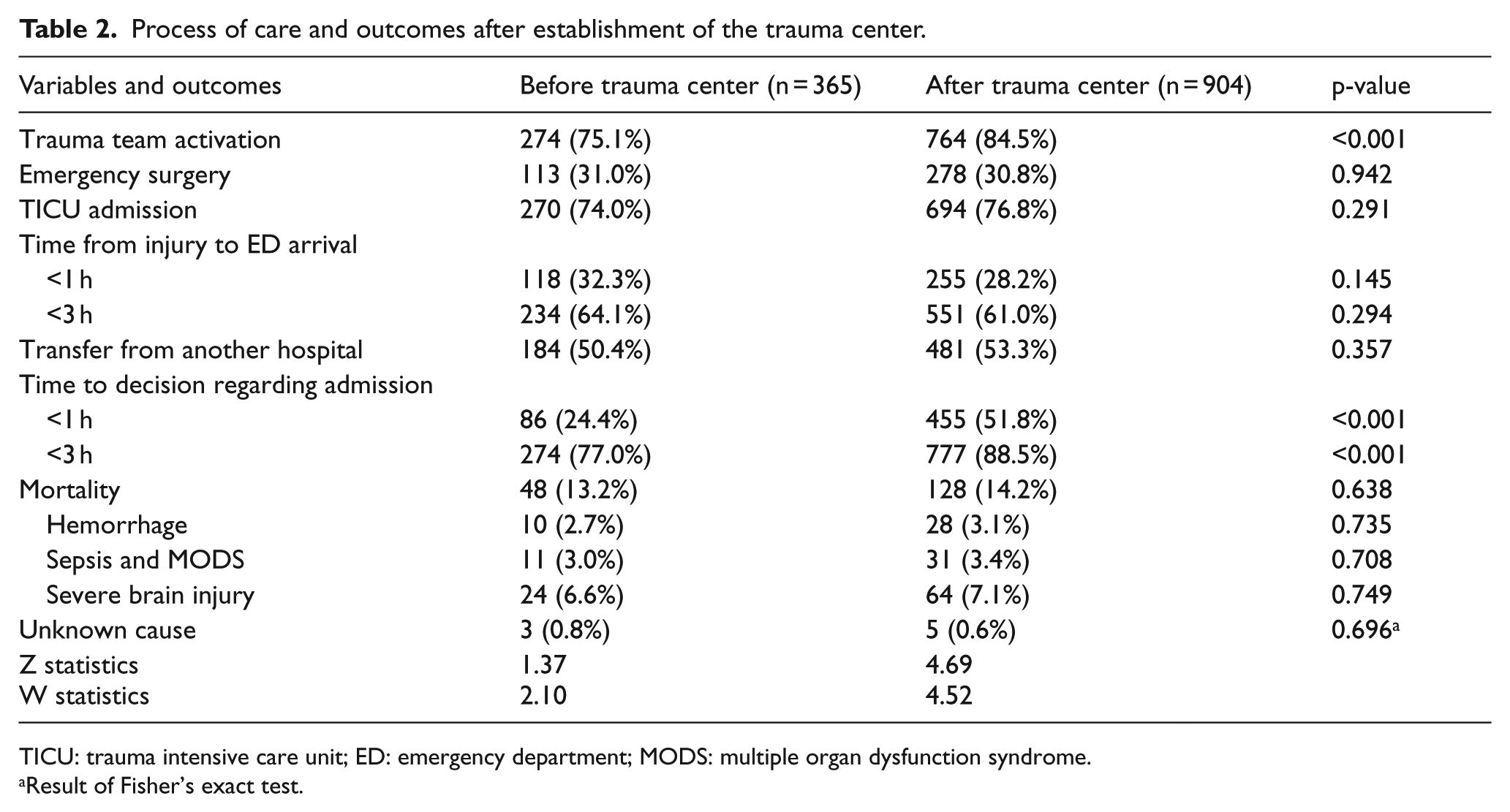
TICU: trauma intensive care unit; ED: emergency department; MODS: multiple organ dysfunction syndrome.
Result of Fisher’s exact test.
Factors associated with mortality
Univariate analysis revealed that these factors were associated with in-hospital mortality: older age; higher ISS; lower RTS; lower initial systolic blood pressure; higher initial pulse rate; cardiac arrest at arrival; transportation directly to the ED (vs transfer from another hospital); ED arrival time in the ED < 3 h after injury; decision-making time regarding admission < 3 h; emergency surgery; head and neck, chest, and extremities and pelvic girdle injuries (with an AIS severity score > 3); and admission to the TICU (Table 3). Multivariate analysis identified the following independent risk factors for in-hospital mortality: older age, higher ISS, lower initial systolic blood pressure, transportation directly to the ED, head and neck injury (with an AIS severity score > 3), and admission to the TICU (Table 4).
Characteristics of survivors and non-survivors.
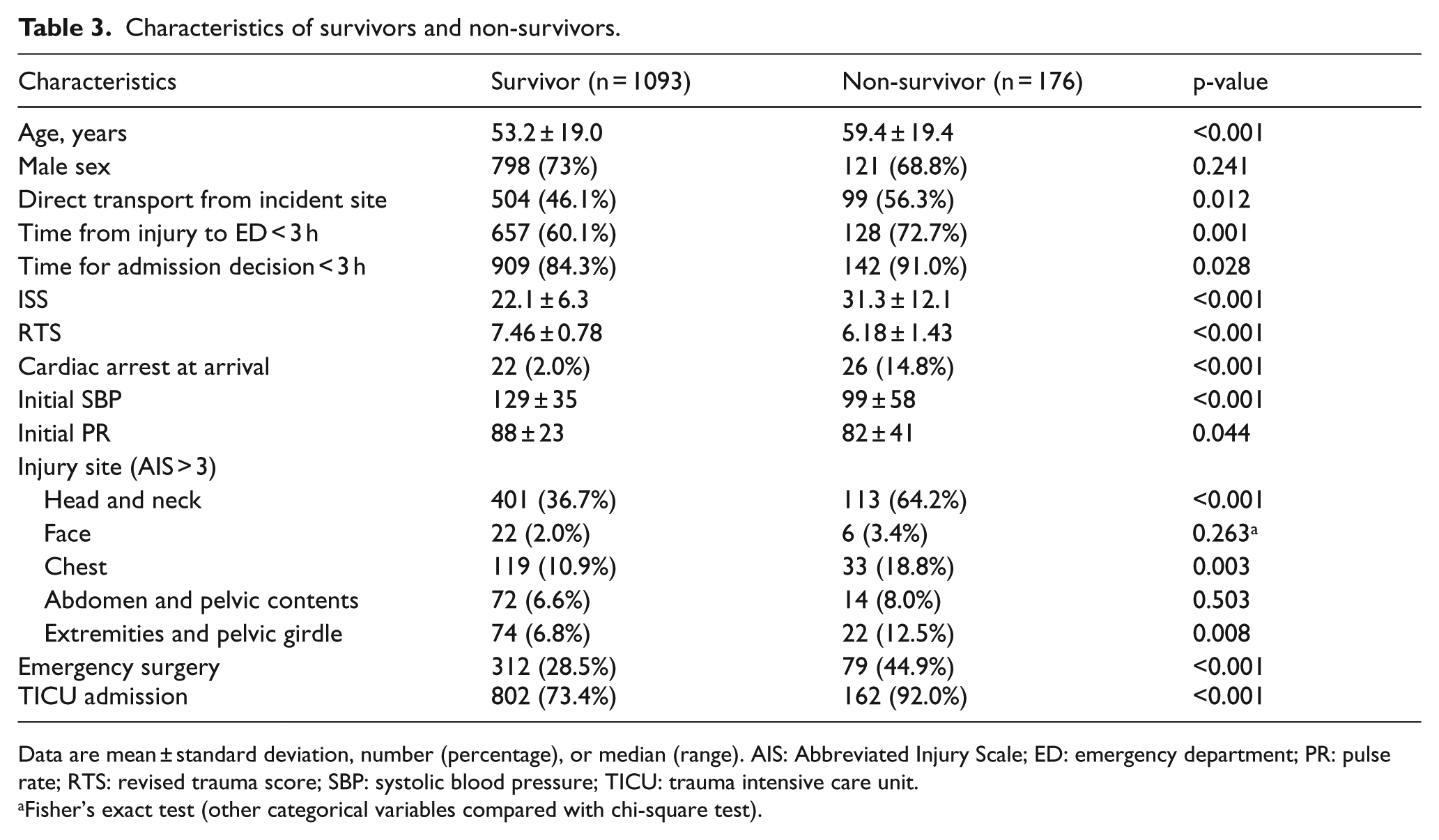
Data are mean ± standard deviation, number (percentage), or median (range). AIS: Abbreviated Injury Scale; ED: emergency department; PR: pulse rate; RTS: revised trauma score; SBP: systolic blood pressure; TICU: trauma intensive care unit.
Fisher’s exact test (other categorical variables compared with chi-square test).
Multivariate analysis of factors associated with mortality.
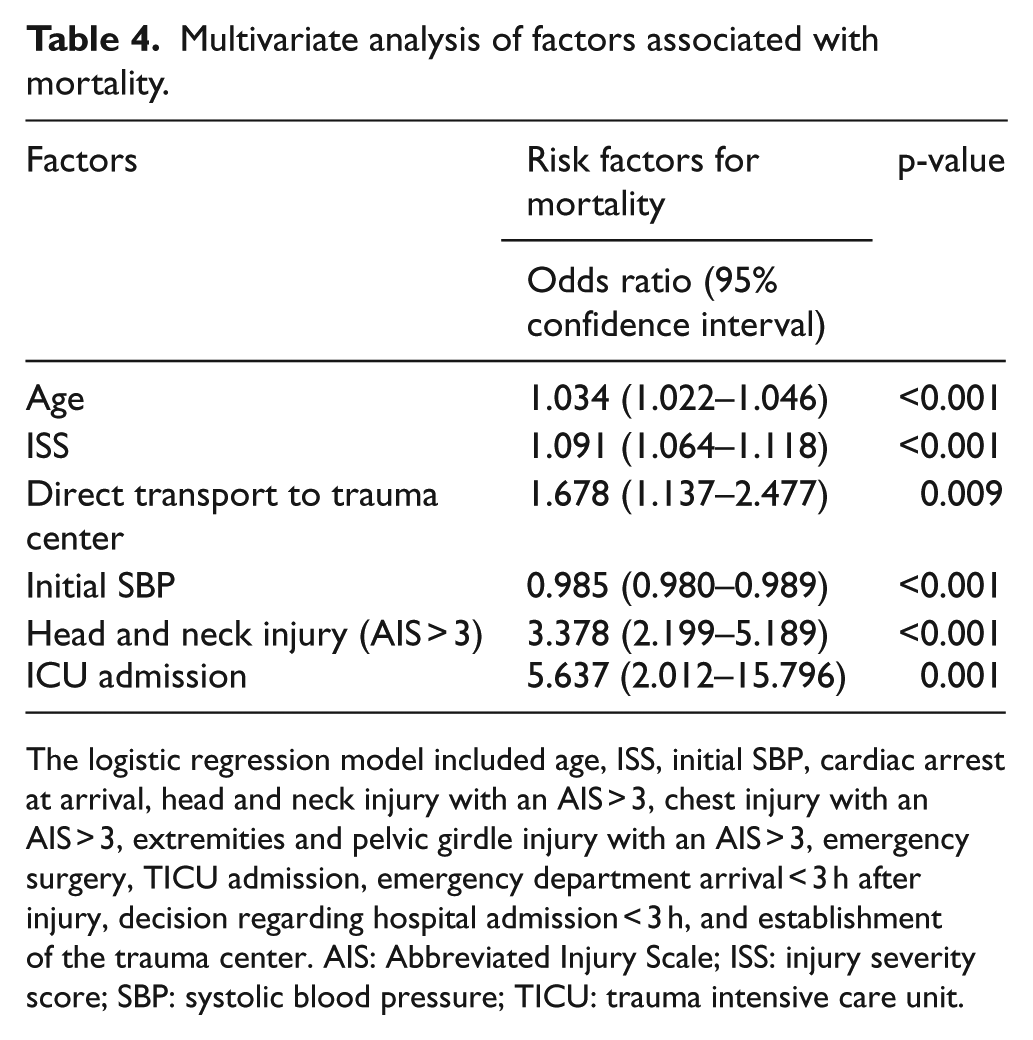
The logistic regression model included age, ISS, initial SBP, cardiac arrest at arrival, head and neck injury with an AIS > 3, chest injury with an AIS > 3, extremities and pelvic girdle injury with an AIS > 3, emergency surgery, TICU admission, emergency department arrival < 3 h after injury, decision regarding hospital admission < 3 h, and establishment of the trauma center. AIS: Abbreviated Injury Scale; ISS: injury severity score; SBP: systolic blood pressure; TICU: trauma intensive care unit.
Discussion
TTA
It is essential to use acceptable indications for TTA to avoid undertriage and overtriage. Undertriage may lead to delayed treatment and diagnosis, adverse patient outcomes, and increased preventable deaths. Conversely, overtriage results in overutilization of both financial and human resources. Since establishing a trauma team in 2011, OO hospital has used a modified field triage system (Appendix 1) that considers the patient’s condition on arrival in the ED. The Korean trauma project group, under the direction of KMHW, has managed and supervised the appropriateness of TTA since opening our regional trauma center. Our regional trauma center has used the same TTA criteria since it was opened; however, TTA has undeniably been performed more thoroughly under governmental supervision, especially in patients with less severe injuries, but who met the TTA criteria. The frequency of TTA at our center has thereby increased since 2015.
Shortened time to admission decision
The time to admission decision has been shortened since our regional trauma center was established. This can be explained by an increase in TTA and efforts of our dedicated trauma team to increase the speed of making decisions. Indeed, since the regional trauma center was established, the appropriateness of the admission and treatment for individual patients has been internally through daily monitoring of all admitted to our trauma center, review of patients who visited our ED the previous day, and other activities focusing on quality improvement, such as mortality conferences. These activities may have contributed to shortening the time to admission decision.
Based on our study design, we cannot determine whether shortening the decision-making time for admission was due to the presence of in-house attending trauma physicians. This is because our institution has had in-house attending trauma physician call coverage and mandatory presence for all patients triggering TTA since 2013, before opening the regional trauma center. A previous study reported that in-house trauma attending coverage was associated with shorter resuscitation times and reduced times to emergency operations. 6 In another study, in-house attending trauma physicians did not affect late (6-week) mortality. 7 Although the impact of in-house trauma attending cannot be conclusively determined by our study, the presence of an attending trauma physician in the hospital will continue because it may be life-saving in individual cases, and it is also important for teaching residents, medical students, and nurses.
Not changed in-hospital mortality rate
Previous reports indicated that the in-hospital mortality rate was approximately 10% (7.6%–10.9%) for patients with an ISS > 16 in level I trauma centers in the United States.8,9 Our mortality rate (14.2%) after the establishment of trauma center was still relatively high in comparison, despite the shorter time to admission decision-making. In addition, another study from Unites States reported that mortality rates for severely injured patients (ISS > 15) decreased from 14.11% to 8.99% after a level II trauma center was upgraded to a level I trauma center. 10 A similar study from Australia reported an 8% reduction in the mortality rate of trauma patients with an ISS > 15 after establishing a trauma center. 11
Although the quality of in-hospital management for traumatized patients obviously improved because of the presence of dedicated attending trauma physician and nursing staff, operating room availability, and daily monitoring for appropriateness of treatment, the mortality rate surprisingly did not decrease after establishing our regional trauma center; indeed, it increased slightly but not significantly. There are at least two possible reasons for this finding. One is that the number of severely injured patients (ISS > 15) visiting our trauma center increased. Furthermore, TRISS score of the after trauma center group was significantly lower than that of the before trauma center, confirming that severely injured patients with a high probability of mortality were more collected after the establishment of the trauma center. This was further confirmed by improved Z and W scores between the two periods. Another explanation may be the prolonged time from injury to arrival in our ED. The delayed arrival may be at least partly due to the mountainous terrain in our province, preventing fast transport from the incident site to the trauma center or between hospitals. A hospital-based helicopter emergency medical service can help in dealing with these geographical problems. Medical crew experts (emergency physicians) on board provide specialized primary emergency care within the helicopter; however, for the safety of the physicians, this service is possible during the daytime. In addition, this service is not restricted to trauma patients, as it is also used for critically ill medical patients. Therefore, it does not overcome all geographical limitations. Kim et al. 5 reported that 63 severely injured patients were transported by helicopter to our institution from October 2013 to June 2015. This modality may reduce arrival time from injury for individual patients; however, it might not be used in a sufficient number of cases to reduce the total transport time of trauma patients presenting to our ED. Another possible explanation for the long transport time is that our trauma center is still relatively new, and we have not yet systematized transfers and referrals of trauma patients. There is no control center to direct transfer and allocation of trauma patients between smaller hospitals in our province and trauma centers. In addition, the smaller hospitals do not yet have the facilities or personnel to care for trauma patients themselves or to efficiently and effectively prepare these patients for transfer. A third explanation for the delay between the time of incident and arrival at our ED is the increase in transfers from smaller hospitals to our trauma center after it was established (transferred patients: 50.4% in 2014, 51.4% in 2015, and 55.0% in 2016). The prognosis of patients transported directly from the incident site is better than the prognosis of patients transferred from another hospital. 12 Sampalis et al. 13 reported that the mortality rate for patients transported directly from the incident site was 4.8%, compared with 8.9% for patients transferred from another hospital. Length of ICU stay is also longer for patients transferred from another hospital, compared with patients transported directly from the incident (13.2 vs 16.0 days). 14 Poorer outcomes for the transferred from another hospital may not only reflect the time delay as patients stop over at a hospital where definite treatment is impossible, but it may also reflect poor communication between hospitals and the trauma center. Martin et al. 15 reported that the percentage of patients transferred from another hospital without prior notice was 22.0%. Soysal et al. 16 emphasized that proper communication between hospitals will contribute to successful transfer, and Ahn et al. 17 reported that communication between hospitals before patients are transferred facilitated faster treatment at the trauma center in terms of admission decisions. Therefore, it will be necessary to systematize the transfer of patients between surrounding hospitals and trauma centers once regional trauma centers are finalized, and increase efforts to support trauma education, facilities, and manpower at these hospitals to provide optimal treatment for severely injured patients.
Risk factors associated with mortality
In the current study, we found that mortality was associated with several widely accepted risk factors: older age, lower systolic blood pressure, higher ISS, combined head and neck injury, and admission to the TICU. Interestingly, transportation directly from the incident site without any stopover was associated with a higher mortality rate than patients transferred from another hospital. We performed subgroup analysis of patients who died to explore why mortality rates of directly transported patients were higher. ISS, RTS, and cardiac arrest at ED arrival were compared between directly transported patients and transferred patients. Directly transported patients had a significantly lower RTS and were more likely to arrive in cardiac arrest than patients transferred from another hospital (Table 5). Patients directly transported from the scene also had a higher ISS, although the difference did not reach statistical significance. These findings suggest that directly transported patients had a higher mortality because more severely injured patients, with less possibility of survival, tended to be transported directly to our regional trauma center.
Characteristics of non-survivors transported directly from the incident and non-survivors transferred from another hospital.
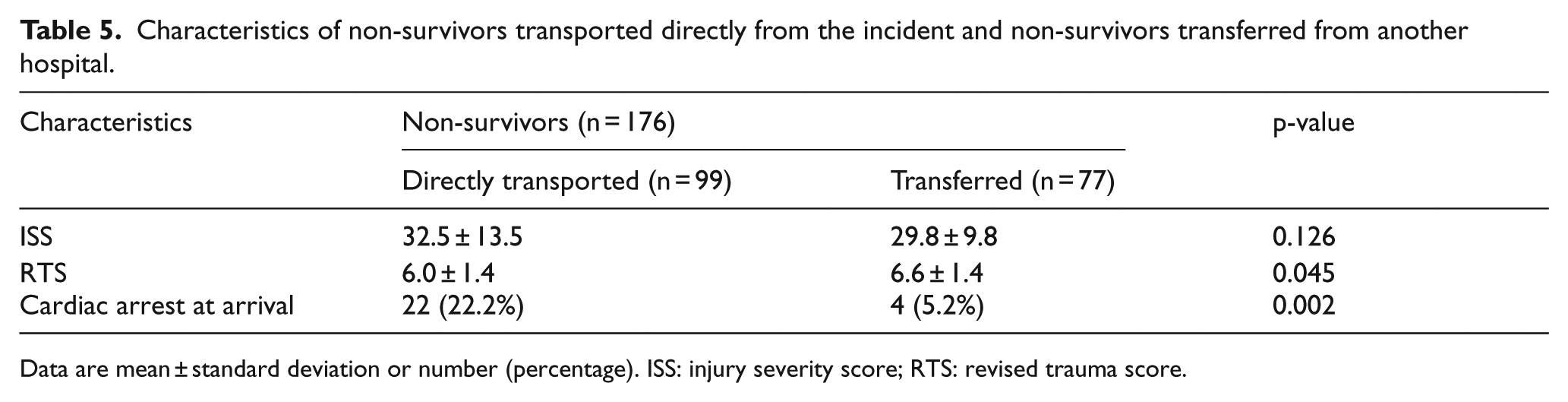
Data are mean ± standard deviation or number (percentage). ISS: injury severity score; RTS: revised trauma score.
Limitations and significance
This study has limitations. The main limitation is its retrospective design. In addition, this is a single-center study, which is also one of its limitations. Furthermore, only mortality rate was assessed as a direct patient outcome. Therefore, the study did not provide a full understanding of patient outcomes, including the quality of trauma center stay. Despite these limitations, this study is meaningful because it describes our experience of operating a regional trauma center that is part of the South Korean trauma system initiated a few years ago, and it provides information regarding whether establishing a regional trauma center actually improves outcomes for severely injured patients. In addition, the study provides important data regarding factors associated with trauma mortality in a specific region in Korea (Gangwon province), which may be useful for directing appropriate treatment and predicting outcomes.
Conclusion
In conclusion, in a regional trauma center in Gangwon province, increased triggering of TTA and implementation of several quality improvement activities conducted under active supervision of the government led to shortening of the time to decision-making regarding patient admission. Although length of hospital stay and mortality rate of trauma patients remained unchanged after the establishment of the regional trauma center, the Z and W statistics revealed improvements in the quality of care. The quality of managing individual injured patients after establishing the center increased because of the presence of in-house attending trauma physicians, trauma-dedicated nursing staff, and an active helicopter medical service. However, these benefits were counterbalanced by an increased number of severely injured patients presenting to our center and the relatively long time from the initial incident to arrival in our ED. Therefore, it is necessary to provide additional education and support to improve the treatment of trauma patients in surrounding hospitals and to establish a control center to coordinate the transfer of patients to our center. Factors associated with increased mortality rate in severely injured trauma patients were older age, higher ISS, direct transport from the incident scene, lower initial systolic blood pressure, head and neck injury (with an AIS > 3), and TICU admission. Close observation and aggressive interventions are recommended for patients with these risk factors to help reduce in-hospital mortality.
Footnotes
Appendix 1
Acknowledgements
We would like to thank all trauma surgeons and nurses for their dedication and commitment to the Korean trauma system. KK and JYJ conceived the study concept and participated in its design, data extraction, statistical analysis, and manuscript drafting and editing. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used during the current study are available from the corresponding author.
Ethical approval
This study was approved by the institutional review board of Wonju Severance Christian Hospital (IRB No: CR318014).
Human rights
As a retrospective study based on medical records, there is no conflict with the human rights of patients and consent is not required.
Informed consent
Informed consent was waived.