
Abstract
Introduction:
Interfacility transport with helicopter from remote island clinics to urban hospitals account for a significant portion of the Hong Kong Government Flying Service missions. Currently, doctor and nurse escorts are deployed as volunteers only during the daytime from every Friday to Monday and on public holidays. While most transport runs smoothly, patient deterioration can occur during flight, warranting medical interventions on-board. Yet, little is known about the pattern and any clinical predictors of such interventions during helicopter interfacility transport missions.
Methods:
We collected Government Flying Service callout records from 1 January to 31 December 2016, and retrieved demographic, clinical and operational data. Interfacility transport mission was dispatched based on ‘Casualty Evacuation’ categories, which range from A+ (unstable), A (borderline) to B (stable). Univariate and multivariable logistic regression were used to identify independent predictors for in-flight medical interventions.
Results:
Of 1734 callout records, 386 interfacility transport missions escorted by volunteer doctors or nurses or both had complete flight medical records for analysis and 14.9% required in-flight medical interventions. Most interventions were related to oxygen therapy, intravenous fluid and administration of medications. Multivariable logistic regression showed that an age ⩾70 years, Casualty Evacuation A+ category, and any pre-flight emergency medical interventions were independent predictors for in-flight medical interventions.
Conclusion:
This study identified a few clinical predictors of in-flight medical interventions in an urban helicopter interfacility transport missions setting. Crewman training that focuses on the relevant procedural capabilities and clinical judgement is necessary to address the in-flight medical needs of interfacility transport missions.
Introduction
Interfacility transport (IFT) of patients from rural hospitals or clinics to tertiary hospitals accounts for a significant portion of flight missions of helicopter emergency medicine service (HEMS) in many countries.1–7 Despite pre-flight patient stabilization and preparation, patient deterioration can occur at any time during the flight, warranting in-flight medical interventions. In Switzerland, life-saving interventions are required in 4.1% of IFT missions. 7 The nature of such interventions dictates the level of crew medical competency and training. However, crew configuration varies considerably across HEMS for mission with similar profiles.8,9
Despite Hong Kong being one of the most densely populated metropolitans in the world, around 30,000 residents live on the outlying islands. 10 IFT to urban regional hospitals is often required for patients with major medical or surgical conditions not amenable to treatment provided by rural hospitals or clinics serving these regions. In Hong Kong, the Government Flying Service (GFS) is the sole provider of HEMS.11,12 Unlike the Franco-German physician-led model and Anglo-American paramedic-staffed model, 13 these helicopters are routinely staffed with air crewman officer (ACMO) trained in first-aid, basic life support and international trauma life support. The service is complemented by trained doctors and nurses who are deployed as volunteers only during the daytime every Friday to Monday and on public holidays. It is not clear whether such a crew configuration is optimal for patient safety during IFT.
Ideally, crew configuration should be determined by the anticipated needs and nature of in-flight medical interventions. Yet, studies of in-flight medical interventions for IFT are lacking, making pre-flight prediction impossible. To address these knowledge gaps, we conducted this study with an aim to characterize the pattern of medical interventions during IFT flight missions and identify predictors for such interventions.
Method
This was a retrospective observational study of consecutive GFS IFT flight missions from 1 January 2016 to 31 December 2016. De-identified data was obtained from the Controller of GFS (Reference number: L/M(5) to OPS/1/125). The study was approved by The University of Hong Kong/ Hospital Authority Hong Kong West Cluster Institutional Review Board (UW17-424). Written informed consent was not necessary because no patient data has been included in the manuscript.
Setting
GFS is a disciplined service of the Hong Kong Special Administrative Region (HKSAR) that provides round-the-clock flying services, including search and rescue, interfacility patient transport, internal security support and firefighting operations. 14 It covers the whole aerial space of Hong Kong and 276,000 km2 over the South China Sea. 15 Maritime Search-And-Rescue (SAR) operations can extend up to 1300 km south of Hong Kong. It serves the whole 7.5 million population in the city. The GFS base and helicopter hangers are located at the south-western corner of the Hong Kong International Airport on the North Lantau Island. At the time of the study, there were seven helicopters, including four Eurocopter EC155 B1 and three Eurocopter AS332L2. All helicopters can be mounted with a standardized panel of medical devices for in-flight patient treatment and monitoring (Figure 1).

Front view of the medical panel in EC 155 B1 cabin, with equipment labelling: (1) transport ventilator, (2) patient monitor, (3) defibrillator, (4) vacuum suction unit, (5) syringe pump, (6) oxygen cylinder, (7) blood pressure cuff and pulse oximeter and (8) stretcher.
IFT flight missions from outlying islands to urban hospitals are locally known as ‘Casualty Evacuation’ (CASEVAC). Figure 2 depicts the geographical locations of these rural and urban facilities. GFS Air Command and Control Centre (ACCC) receives callouts from rural hospitals or clinics and dispatches helicopters according to the urgency, availability of helicopters, time of the day and weather condition. The urgency of CASEVAC callouts are classified into three categories: 16 A+, A or B (Table 1). Clinicians in rural hospitals or clinics determine the CASEVAC urgency. When there is no on-site clinician in rural hospitals or clinics, the in-charge senior doctor in the Accident and Emergency department of Pamela Youde Nethersole Eastern Hospital (PYNEH) will determine the CASEVAC urgency. For CASEVAC A+ patients, they are usually airlifted directly from the requesting locations to the rooftop helipad of PYNEH located on the eastern part of Hong Kong Island.10,11 For more stable patients, they are usually transported to the heliport in Wan Chai and then sent to urban hospitals by ground ambulances.

Geographical locations of urban and rural hospitals and clinics covered by the Government Flying Service in Hong Kong.
Classification of urgency of casualty evacuation (CASEVAC).
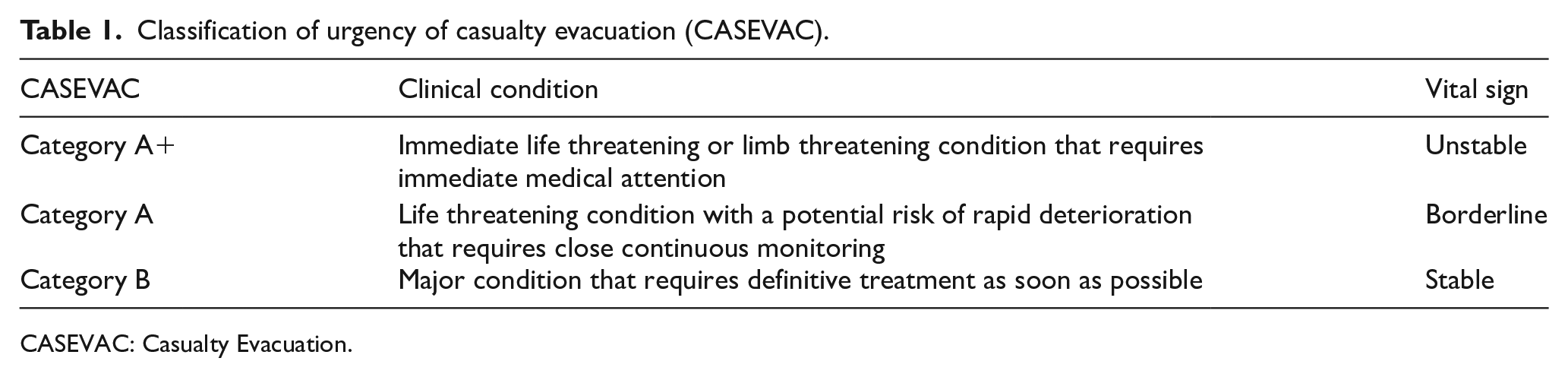
CASEVAC: Casualty Evacuation.
All ACMOs are required to complete a 90-h in-house medical training that covers basic flight physiology, basic life support, patient assessment and monitoring, management of trauma and medical emergencies. In addition, they need to undertake clinical attachments in local emergency departments and ambulances for 5 and 3 days respectively, followed by a 3-week emergency aeromedical technician course that focuses on outreach rescue medic skills. With the endorsement of the Paramedic Service Steering Committee of GFS, ACMOs are expected to provide immediate life support, basic airway intervention, oxygen therapy, defibrillation, external haemorrhage control, immobilization and heat illness management, independently. According to GFS protocols, ACMOs are allowed to administer glucose gel, salbutamol puff and methoxyflurane (Penthrox) on-board without a doctor’s prescription.
With regard to the level of expertise of volunteer medical staff, around 50% of doctors are experienced emergency physicians who have completed specialist training, while the rest are experienced anaesthetists, intensivists and surgeons. All the nurses have extensive experience from their local emergency departments. Before enlistment into the medical unit, all doctors and nurses are required to complete a 3-day training and assessment camp. Currently, volunteer doctors and nurses work from 09:30 to 18:30 from every Friday to Monday and on public holidays and they stand-by in the GFS base. When they are available, flight doctors or nurses take the lead in clinical management of patients during the flight. When they are not available during off hours and patients’ conditions are deemed unstable, nurses from remote clinics are requested to board the helicopter and assist the ACMO with essential treatment during flight.
Data
As a part of the aviation and callout records, patients’ demographic data, flight time and CASEVAC category are captured by the GFS ACCC computer system. During the study period, clinical diagnoses and type of medical interventions are charted in the Air Medical Service Clinical Record only when volunteer doctors or nurses are on-board. In this study, we retrieved and reviewed all consecutive IFT callout records and Air Medical Service Clinical Records within the study period. IFT callouts that were cancelled due to adverse weather conditions or other reasons were excluded. IFT missions with missing clinical records were not included in the analysis.
We collected the following data: patient’s demographic, callout time, request location and destination, CASEVAC category, clinical diagnosis, vital signs and medical interventions. We defined the time from callouts to take-off as the ‘activation time’, the time from take-off to scene arrival as the ‘response time’, the time from scene arrival to take-off to destination as the ‘scene time’ and the time from the requesting location to the destination as the ‘transport time’.
We defined in-flight medical interventions as any medical intervention performed within the ‘transport time’. Medical interventions are categorized as airway (insertion of supraglottic devices, endotracheal intubation, and surgical airway); breathing (provision or titration of supplemental oxygen therapy, bag-valve-mask ventilation, non-invasive ventilation, and mechanical ventilation); circulation (intravenous (IV) cannulation, intra-osseous access, administration of IV fluid, infusion of inotrope, blood transfusion, chest compression, and defibrillation/electrical therapy); and others (administration of medication, spinal immobilization, splintage and dressing). Both medical interventions performed prior to airlift in the requesting facility and during the flight were recorded. We defined any airway, breathing, circulatory intervention, administration of medication, spinal immobilization and splintage before the flight as ‘pre-flight emergency medical interventions because they reflect a higher acuity of the patient condition.
Statistical analysis
There was no imputation for missing values. Since there is a lack of similar studies before, we could not perform a prior sample size calculation. Continuous variables were reported as means ± standard deviation or median with interquartile range, as appropriate. Categorical variables were reported as proportions. Univariate analysis was performed to identify factors associated with in-flight medical interventions. Variables with a significant association with in-flight medical interventions were entered into a multivariable logistic regression model to identify independent predictors. All statistical analysis was performed using SPSS version 26.0. A two-tailed p value < 0.05 was considered statistically significant. The STROBE statement for cross sectional studies was used as reporting guideline during the study.
Results
During the study period, 1734 IFT callout records were identified and 165 flight missions were cancelled due to adverse weather conditions (n = 143), stand-down of callout requests from the requesting facilities (n = 15), competing missions (n = 5), patient refusal (n = 1) and unstable emotion of a patient with self-harm risk during the flight (n = 1). The demographic and operational characteristics of all the IFT missions, including missions escorted by volunteer doctors or nurses or both and those by ACMOs, are summarized in Table 2.
Demographic characteristics of the study population.
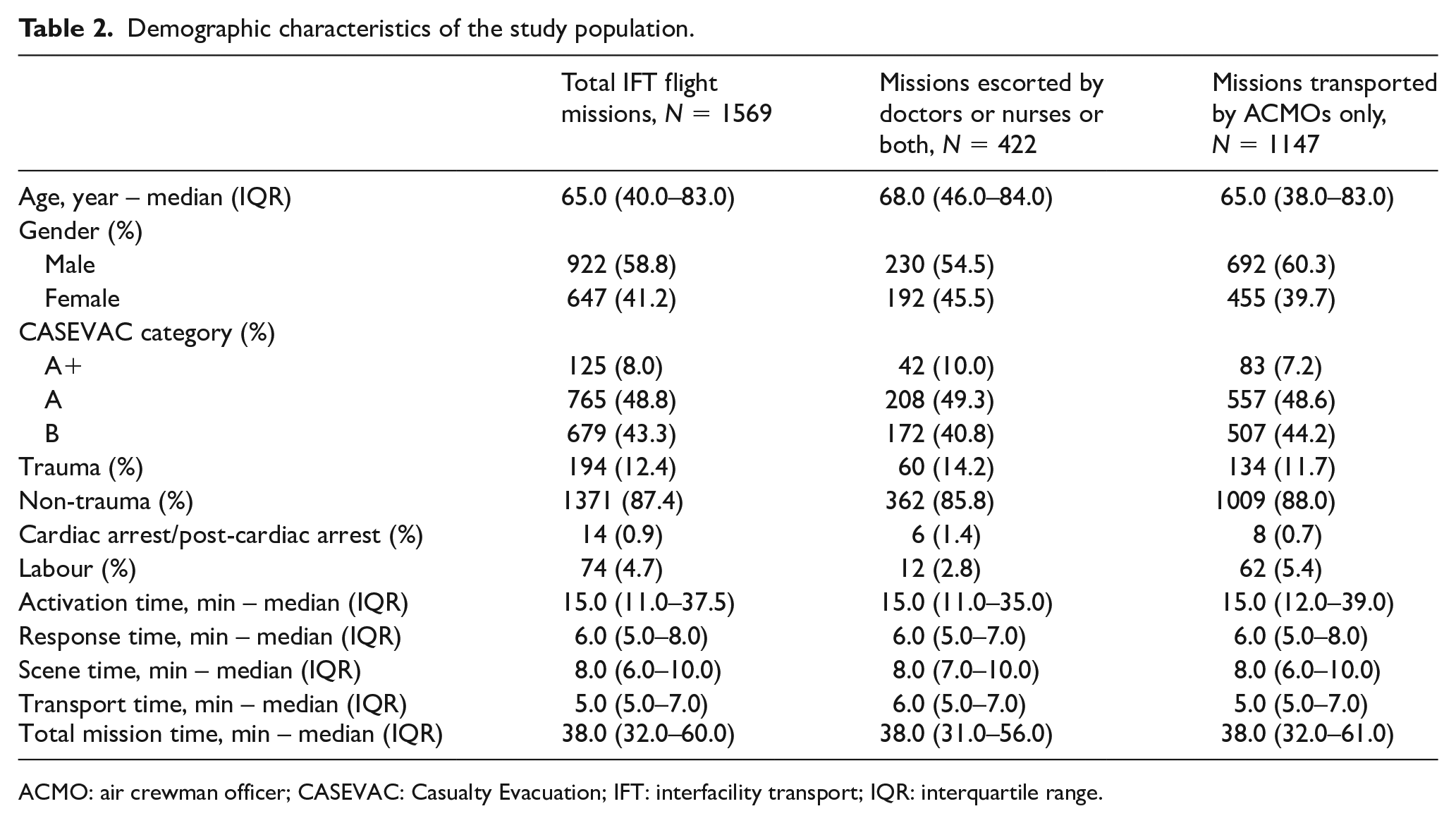
ACMO: air crewman officer; CASEVAC: Casualty Evacuation; IFT: interfacility transport; IQR: interquartile range.
Among 1569 IFT flight missions, 386 IFT patients with complete Air Medical Service Clinical Records for analysis, of whom (14.8%) required in-flight interventions. Table 3 shows the medical interventions performed before and during the flight missions. Despite the short median transport time of 5 min, 69 in-flight medical interventions were carried out. Among these interventions, provision or titration of supplemental oxygen therapy was the most common (n = 46), followed by administration of IV fluid (n = 8) and administration of medications (n = 4). The medications administered on-board included adrenaline in two cases, amiodarone in one case, midazolam and rocuronium in one case, and hydrocortisone in one case. Of note, two patients required chest compression and one required defibrillation during the flight. None required airway intervention.
Medical interventions provided before and during the flight.
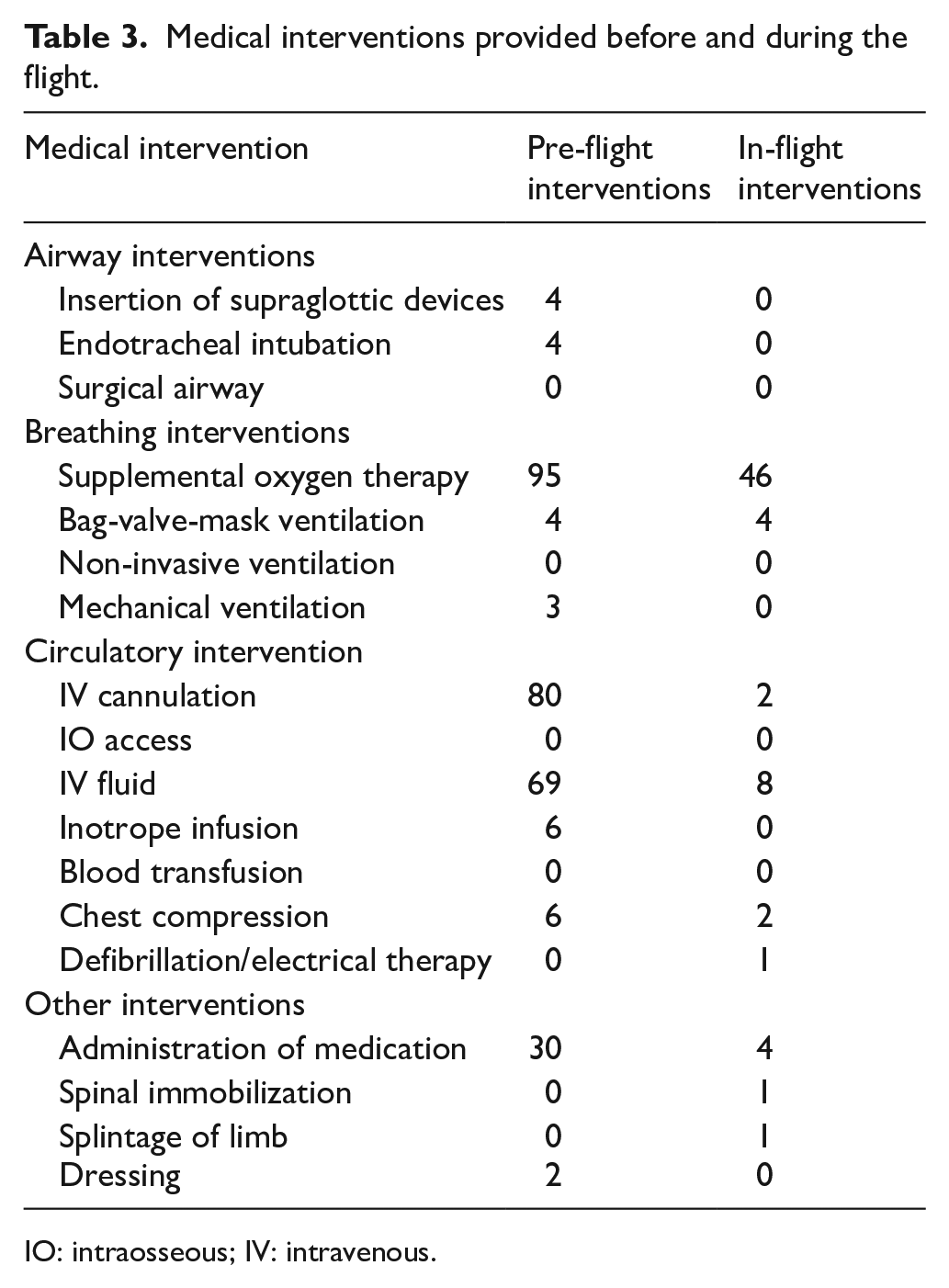
IO: intraosseous; IV: intravenous.
Univariate analysis comparing IFT patients who required in-flight medical interventions and those who did not, showed that patients in the intervention group were significantly older (median age 80.5 years vs 66.0 years, p < 0.001), with a higher CASEVAC category (p < 0.001) and a higher proportion of cardiac arrest/post-cardiac arrest (7.0% vs 0.6%, p = 0.005). Patients who required in-flight medical interventions were also more likely to have received airway (p = 0.002), breathing (p < 0.001), circulation (p < 0.001) and any emergency medical interventions (p < 0.001) before the flight. The presence of doctors as a crew member appeared to be associated with in-flight medical interventions (Table 4).
Comparison of characteristics of patients who required in-flight medical interventions and who did not.
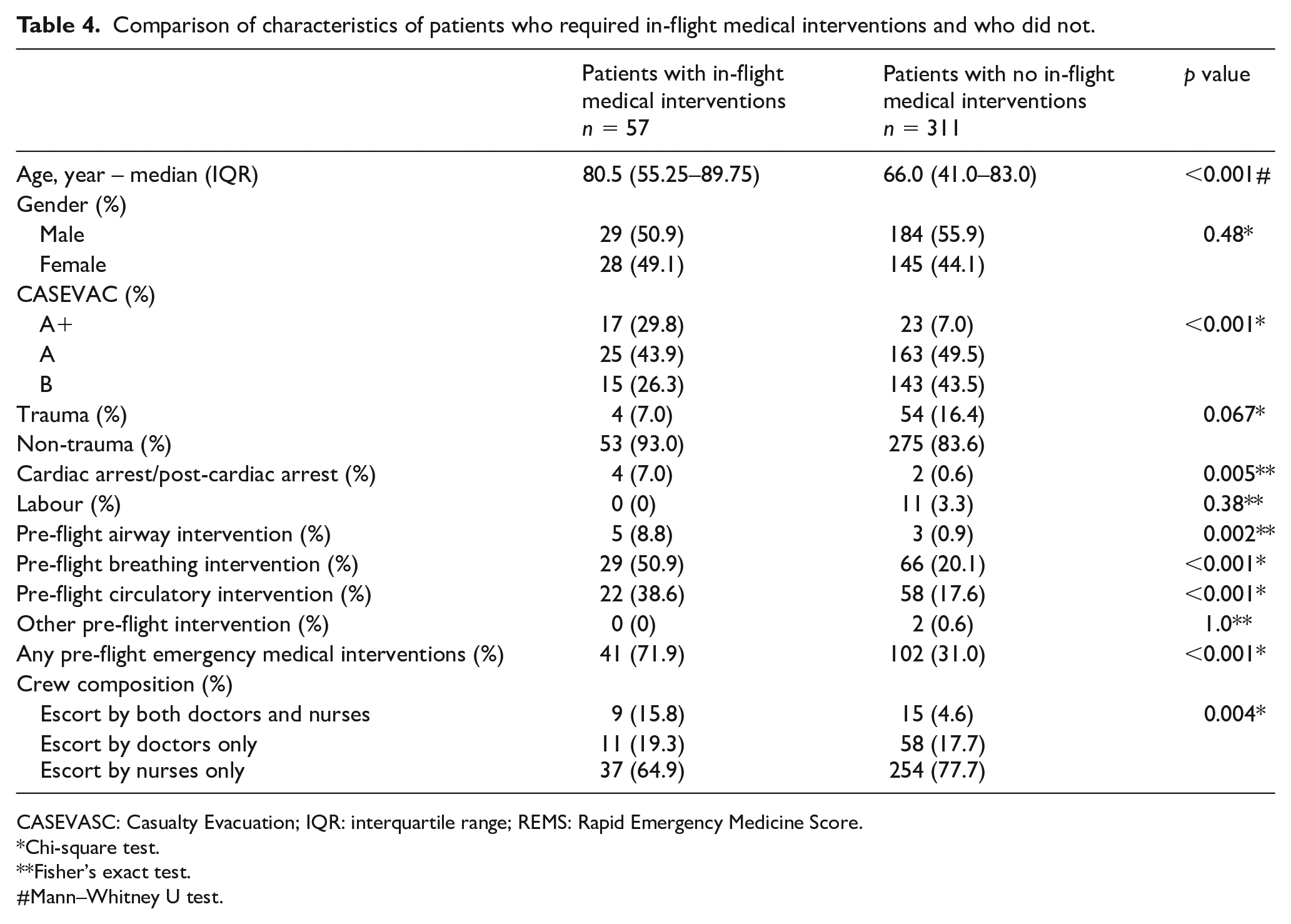
CASEVASC: Casualty Evacuation; IQR: interquartile range; REMS: Rapid Emergency Medicine Score.
Chi-square test.
Fisher’s exact test.
#Mann–Whitney U test.
The result of multivariable logistic regression is shown in Table 5. Since cardiac arrest/post-cardiac arrest cases are categorized as CASEVAC A+, we did not enter cardiac arrest/post-cardiac arrest into the regression model despite the significant association in univariate analysis. As for age, we used 70 years as the cut-off point to facilitate decision in daily operation. In multivariable logistic regression, only age ⩾ 70 years (OR 2.05, 95% CI = 1.06–3.96, p = 0.033), CASEVAC Category A+ (OR 4.54, 95% CI = 1.75–11.76, p = 0.002) and pre-flight emergency medical interventions (OR 3.74, 95% CI = 1.91–7.30, p < 0.001) remained independent predictors for in-flight medical interventions. The crew composition was not significantly associated with in-flight medical interventions after adjusting for the effect of other variables.
Independent predictors associated with in-flight medical interventions.
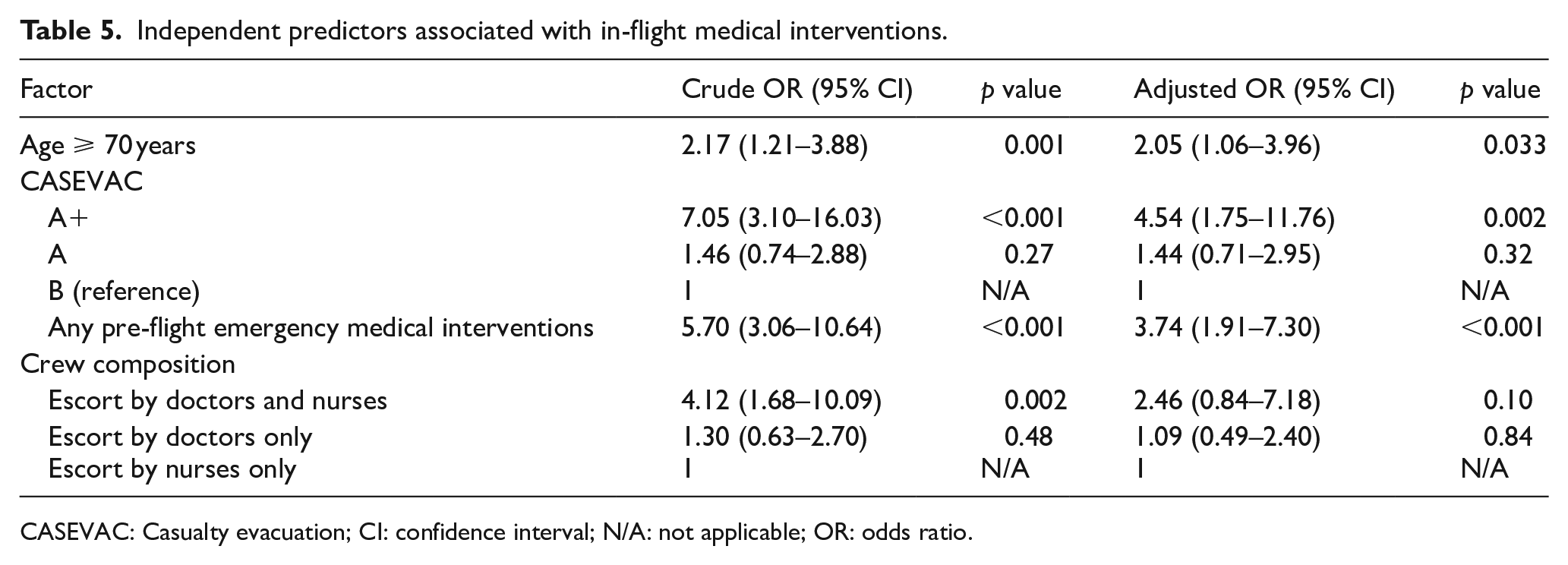
CASEVAC: Casualty evacuation; CI: confidence interval; N/A: not applicable; OR: odds ratio.
Discussion
Despite pre-flight patient stabilization and a short helicopter transport time of IFT flight missions in an urban setting with scattered outlying healthcare facilities, our study showed that 14.8% of the patients required in-flight medical interventions. We found that age ⩾ 70 years, CASEVAC Category A+ and any pre-flight emergency medical interventions were independent predictors for in-flight medical interventions.
Most in-flight medical interventions involved provision or titration of supplemental oxygen and administration of IV fluid. It is important to note that the medications given by volunteer flight doctors or nurses, including adrenaline, amiodarone, midazolam, rocuronium and hydrocortisone, are not currently allowed to be administered by ACMOs. Provision and titration of supplemental oxygen and IV fluid require not only competency in procedural skills, but also clinical judgement.
Ideally, trained doctors are deployed to IFT flight missions with a higher predicted risk for in-flight medical interventions. Our study showed that age ⩾ 70 years, CASEVAC Category A+ and any pre-flight emergency medical interventions are potentially useful criteria for risk stratification. Studies have demonstrated that even with similar procedural capabilities, physicians treat more aggressively than paramedics because of the freedom of exercising clinical judgement.17,18 However, the benefit of doctors in HEMS remains a subject of debate, 19 although the perceived patient and flight safety is higher when they are a part of the crew. 8 In primary trauma rescue missions, addition of trained physicians to the crew is associated with improved survival rates in some studies,17,20,21 but not in others. 22 For IFT, only limited literature exists. In ST-elevation myocardial infarction, Gunnarsson et al. 23 showed that patients transported by physician-staffed HEMS had a lower in-hospital adjusted adverse event risk compared with those transported by non-physician-staffed HEMS, although the in-hospital mortality did not differ between the groups. Burney et al. 24 found no difference in outcomes of patients transported by flight crew that included a doctor and a nurse compared with two nurses only. Our study found that the presence of doctors did not independently predict in-flight medical interventions. It is noteworthy that even deployment of doctors to high-risk IFT missions requires them to stand by at the base around the clock. Given the resource implications and limited availability of trained doctors suitable for the task, this strategy might not be practical.
The other strategy is to deploy a flight nurse or to mandate nurse escort from the requesting facilities in every high-risk IFT mission. In the literature, studies that compare nurse-escorted and paramedic-escorted IFT flight missions are lacking. While this approach might have less resource implications compared with deployment of flight doctors, experienced flight nurses are limited in number in our locality. Most rural hospitals and clinics have inadequate on-site nursing manpower to provide nurse escort routinely. Furthermore, nurses from rural hospitals or clinics might need to undertake training in flight medicine and transport medicine before they can fit into the role. Even with training, the types of life-saving medications that can be administered by nurses without a doctor prescription are still very limited.
Given the nature of in-flight medical interventions found in our study, it is feasible and more practical to train up ACMOs to reach the local paramedic skills level, which is sufficient for medical interventions such as oxygen therapy and IV cannulation. Such training should not only focus on procedural capabilities, but also on clinical judgement in the provision of such interventions in the flight environment. As such, there is a need to review the current training programme of ACMOs and they should be exposed to more ground inter-hospital transport activities to gain experience. While asking the ACMOs to reach the level of clinical judgement of a doctor or a registered nurse is not pragmatic, emphases should be placed on recognition of respiratory distress and haemodynamic instability that would warrant supplemental oxygen or IV fluid or both based on standardized protocols. Although the repertoire of medications is unlikely to be expanded vastly as limited by local legislations, advanced prescription before flight by the clinicians in the requesting facilities and standardizing drug administration/titration protocols may allow timely medication use during the flight. With the advent of telemedicine technology, real-time in-flight physician supervision of drug administration represents another avenue for future research.
Limitations
This study has several limitations. First, only IFT flight missions escorted by volunteer doctors or nurses or both had completed Air Medical Service Clinical Records for analysis. In-flight medical interventions in IFT missions transported by ACMOs, including those with escort nurses from rural hospitals or clinics, were not documented. We cannot extrapolate data from IFT flight missions escorted by volunteer doctors or nurses directly to missions transported by ACMOs. However, these missions, as shown in Table 2, had comparable characteristics, suggesting a similar need for in-flight medical interventions. Second, there might be information bias. Given the short transport time, the flight doctors or nurses might only have time to document major medical interventions, leaving the minor ones undocumented. Yet, we believe we have captured most major interventions carried out during the flight. Third, the Air Medical Service Clinical Records did not specify the exact provider of each in-flight medical intervention. In the presence of flight doctors and/or nurses, we believe most, if not all, interventions were provided by them. Fourth, we did not have data on the presence of the medic panel in the helicopter. The impact of mounting a medic panel on the readiness and provision of in-flight medical interventions is unclear. Fifth, the whole GFS helicopter fleet has been upgraded to Airbus H175 since the study. We believe the impact of such a change in helicopter model on in-flight medical intervention is minimal provided that the manpower provision and training has remained similar. Finally, the CASEVAC classification is developed and used solely in HKSAR. Our findings might not be generalizable to other HEMS with a different case-mix and risk stratification system. However, we believe the findings of age ⩾ 70 years and pre-flight emergency medical interventions as independent predictors might have some values in decision making across different services, which are worth confirmation with further studies. Future studies, best in the form of prospective observational study involving all IFT missions with a clear definition of scenarios, intervention and the role of each provider, are warranted to identify areas training effort should be focused.
Conclusion
Despite stabilization prior to flight and a short flight time in an urban HEMS, a sizable portion of IFT patients requires medical interventions on-board, with provision or titration of supplemental oxygen and IV fluid accounting for the majority. Age ⩾ 70 years, CASEVAC category A+ and any pre-flight emergency medical interventions independently predict the need for such interventions. Given the nature of in-flight medical interventions found in our study, training that focuses on the relevant procedural capabilities and clinical judgement of ACMOs represents the most practical way to address the in-flight medical needs of IFT missions.
Footnotes
Acknowledgements
The authors sincerely thank GFS Controller (Captain West Wu), ACMO (Mr Tony Cheung, Mr Jove Cheung) and Chief Air Medical Officers (Dr Willis Kwok and Dr Calvin Chau) for their unwavering support during the study. They also thank Ms Lujie Chen of the Emergency Medicine Unit for her contribution to this study.
Author contributions
A.C.K.C. and R.P.K.L. researched the literature and conceived the study. A.C.K.C. and E.P.H.N. acquired the data. R.P.K.L. and V.K.C. were involved in data analysis. A.C.K.C. and P.W.F.F. wrote the first draft of the manuscript. A.C.K.C., R. P.K.L. and T.H.R. were involved in the critical revision for important intellectual content. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Informed consent
Informed consent was not sought for the present study because the retrospective data retrieval would not affect patients’ clinical management.
Ethical approval
Ethical approval for this study was obtained from The University of Hong Kong/Hospital Authority Hong Kong West Cluster Institutional Review Board (UW17-424).
Human rights statement
This study was completed in accordance with the Helsinki Declaration.