
Abstract
Introduction
Optimal dispatch of emergency medical services relies on accurate time estimates of the various prehospital stages. Hoist rescue work time intervals performed by the search and rescue (SAR) helicopter service in Norway have not been studied to date. We aimed to describe the epidemiologic, operational, and medical aspects of the SAR service in southeast Norway. To complement the prehospital timeline, we performed simulated hoist operations.
Methods
We reviewed time and patient descriptors and medical interventions in hoist operations performed at a SAR base over 5 y. In addition, a simulation study measuring hoist rescue time intervals was performed. Data are presented as mean ± SD, except National Advisory Committee for Aeronautics (NACA) scores, which are presented as modes.
Results
There were 148 hoist operations performed during the study period, involving 180 patients. Time to take-off was 13 ± 7 min. There were 88 patients (49%) who were injured; 53 (29%) had a medical condition, and 39 (22%) were evacuees. The mode of the NACA score was 3. Forty-five patients (25%) had an NACA score of 4 to 6. Medical interventions were performed on 77 patients (43%) in 73 operations (49%). Nine patients (5%) were endotracheally intubated, and 1 thoracostomy was performed. The simulated rescuer access time was 4 ± 2 min, the simulated anesthesiologist access time was 6 ± 2 min, and the simulated hoist extrication time was 13 ± 2 min.
Conclusions
Hoist rescue was performed in 10% (n=148) of the SAR operations. New information about hoist extrication time intervals can improve rescue helicopter dispatch accuracy.
Keywords
Introduction
The outcome of severely ill and injured patients depends on the time to critical care. Short response times for emergency medical services (EMS) remain pivotal. 1 –4 Helicopter rescue can be beneficial in offshore emergencies or when demanding topography makes it difficult or time consuming for ground EMS (GEMS) personnel to access the scene. 5 –14 In Norway, both helicopter EMS (HEMS) and the larger search and rescue (SAR) helicopters can be deployed to incidents. SAR helicopters have hoist capacity and perform patient extrication with a variety of slings and stretchers. SAR helicopters perform both offshore evacuations and rescue operations on land at all times and regardless of daylight. In contrast, HEMS helicopters can only perform daylight rescue operations with static rope. In both SAR and HEMS helicopters, a consultant anesthesiologist is the medically responsible crew member and performs advanced medical interventions when necessary. 15 –18
Both HEMS and SAR units are dispatched by local emergency medical communications centers (EMCC). SAR unit dispatch also requires approval by 1 of the 2 national joint rescue coordination centers. The EMCCs can ask the joint rescue coordination centers for SAR assistance when SAR is considered the most appropriate alternative. Reasons for requesting a SAR unit might include shorter distance to the scene, lack of daylight, offshore emergencies, demanding scene topography (vertical mountain cliffs or tall trees and deep gorges requiring longer hoist cables), or when it is desirable to ground both the rescuer and the anesthesiologist at the scene.
Norwegian EMCCs have indefinite guidelines for the dispatch of helicopter rescue in difficult terrain and choose between HEMS and SAR resources when both appear to be equivalent alternatives. The absence of dispatch support aids represents a shortcoming of the EMS system that can lead to delayed dispatch with adverse patient outcomes. Variations in dispatch practice have been described. 19 A reason for this shortcoming is a lack of information about prehospital time intervals related to the rescue work of SAR hoist rescue.
We aimed to describe the epidemiologic, operational, and medical aspects of SAR hoist rescue in the southeast region of Norway. Time expenditure of the various phases of SAR hoist rescue is, however, currently not recorded. To fill this gap in the prehospital timeline, we performed standardized simulated operations in which the duration of the various phases was measured.
OPERATIONAL SETTING
Southeast Norway has 1 SAR base, operated by the Royal Norwegian Air Force (under the auspices of the Ministry of Justice and Public Security), located at Rygge, 61 km southeast of the regional trauma center at Oslo University Hospital. The base uses a Westland Sea King Mk.43B helicopter and completes approximately 300 operations annually, of which one-third are SAR operations. The SAR crew consists of a pilot, copilot, flight engineer, system operator (navigator), rescuer, and anesthesiologist and is stationed in the hangar during weekdays from 0730 to 1530. Outside these hours, the crew members are quartered at the military camp area (2 km away). Four HEMS bases operate in the catchment area of the SAR base. The 5 bases cover a population of approximately 3 million people. The HEMS crews consist of a pilot, HEMS rescuer, and anesthesiologist, who are stationed on the base at all times. 20 The HEMS crews use a Eurocopter (EC) 135 P2 + or an EC 145 helicopter. All HEMS and SAR bases have at their disposal EMS vehicles, without patient transport capacity, used for nearby emergencies or when the weather prevents use of the helicopter. For patients whose condition requires transport (eg, to a hospital), an ordinary ground ambulance is necessary.
SAR HOIST OPERATIONS
The SAR helicopter is equipped with 2 variable-speed Breeze Eastern hydraulic hoist systems installed on the right side (pilot’s side) of the aircraft (Figure 1). The hoist cables are 77 m (245 ft) in length, and the hoists are capable of a maximum load of 272 kg (600 lb). To avoid delay, the SAR unit remains fully rigged for hoist rescue operations. Crew members, including the anesthesiologist, train regularly on numerous procedures of hoist rescue typical to their range of responsibilities. The rescuer is trained in advanced rescue procedures (eg, establishing a secure belay station in steep terrain). The personnel normally practice the procedures every 3 mo.

A search and rescue hoist rescue involving a Westland Sea King, with a rescuer on the ground with the patient. An anesthesiologist is in the hoist, which is operated by the flight engineer and system operator in the cargo door (photograph from training, courtesy of Norwegian Air Ambulance).
On a mission, the rescuer and the anesthesiologist decide the optimal method of extricating the patient. Shortly before the rescue operation starts, the 2 hoist operators (flight technician and system operator) take positions at the cargo door. In cooperation with the pilots and the rescuer, they perform reconnaissance of the terrain and potential obstacles. The operational risk management within the crew is ensured through continuous communication, both verbally by intercom and by hand signals. Choice of extrication method is flexible and depends on the circumstances. The rescuer and anesthesiologist can be hoisted individually or jointly, together with the appropriate extrication device, medications, and other necessary equipment. On-scene stabilization and packaging of the patient are performed by the rescuer and anesthesiologist jointly or individually prior to extrication. When required, additional equipment can be hoisted down from the helicopter. The rescuer or anesthesiologist can accompany the patient and when necessary perform patient treatment during hoisting (Figure 2).
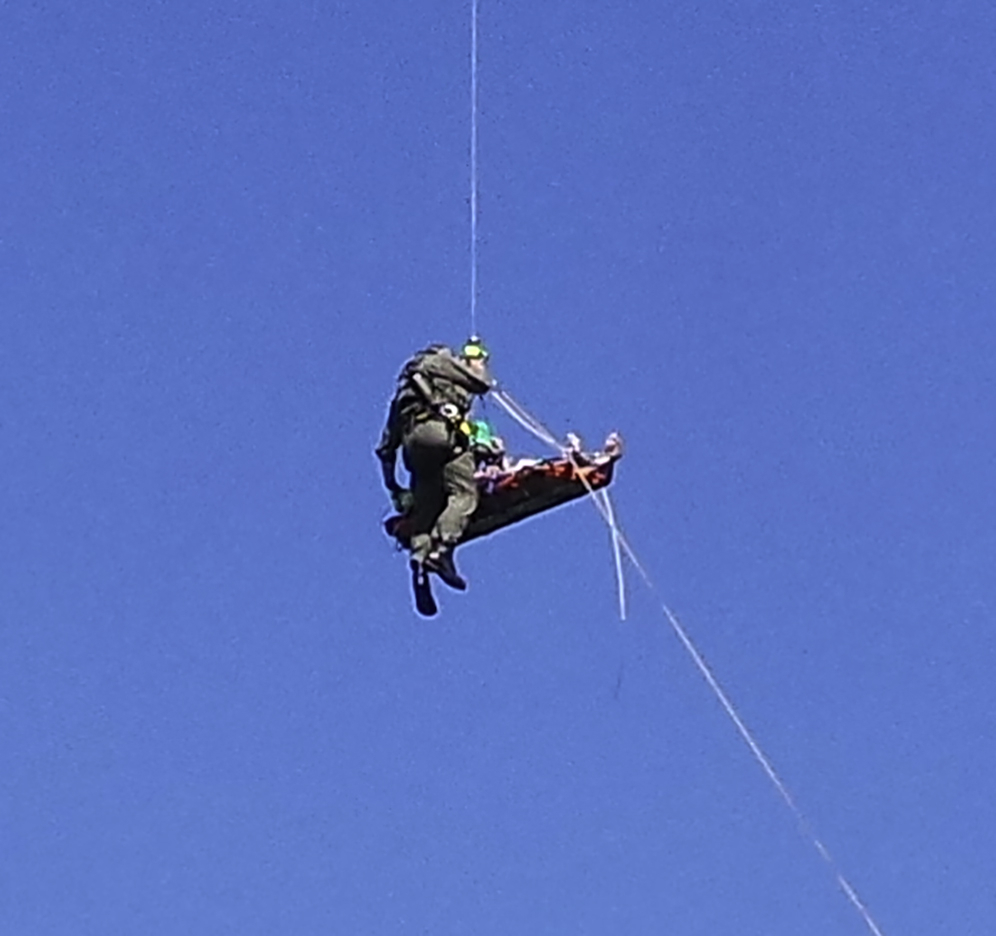
A search and rescue anesthesiologist performing mechanical chest compressions with a LUCAS device during hoisting (photo by Fabian Skalleberg Nilsen/NRK [Norwegian Broadcasting Corporation]).
After the patient enters the helicopter, further observation and treatment can be performed during the flight to the hospital. The HEMS helicopters operating in the same area do not have hoist capacity. The anesthesiologist functions as the navigator to direct the pilot when the HEMS rescuer is transported to the scene.
Methods
EPIDEMIOLOGY OF SAR
The medical database LabasNG (a proprietary database management system; NormannIT, Trondheim, Norway) was used to identify SAR hoist operations performed during the study period from January 1, 2013 to December 31, 2017. The following data were extracted from the database: operational descriptors (Figure 3, blue timeline intervals), patient descriptors (age, sex, diagnosis according to International Classification of Diseases, 10th Revision, severity of injury or illness, activity when injured or falling ill), and interventions provided. The anesthesiologist scores the severity of injury or illness according to the National Advisory Committee for Aeronautics (NACA) scoring system (Table 1) as part of mandatory reporting. No hospital medical records were accessed.
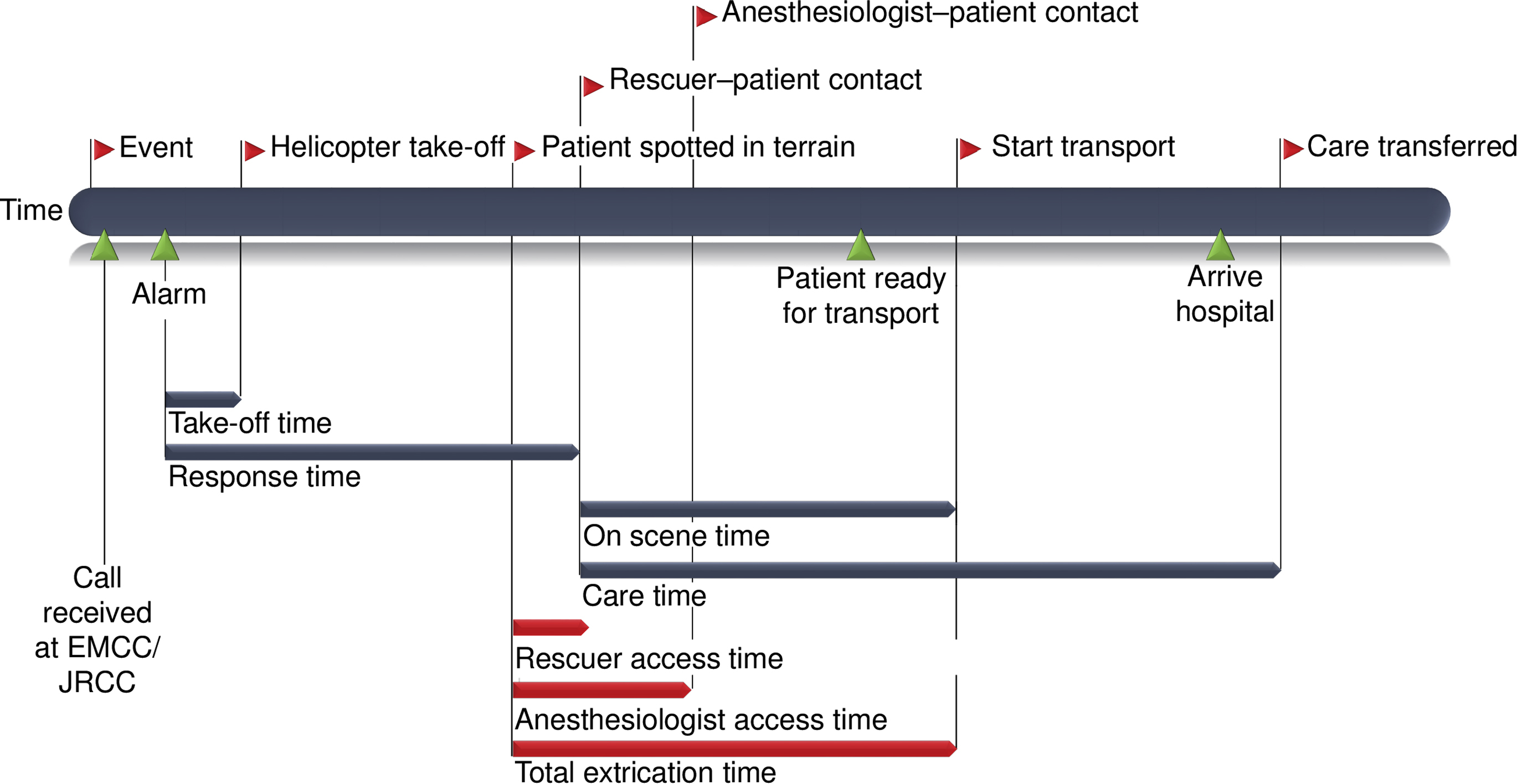
Search and rescue hoist rescue: time points and intervals.
Description of the NACA scoring system
NACA, National Advisory Committee for Aeronautics.
Daylight hours for Rygge SAR base were obtained by plotting alarm time and date in a sunset sunrise calculator application (
SIMULATION STUDY
Because rescue time intervals are not registered in the LabasNG system, simulated hoist operations were performed to complement the prehospital timeline. A full-size mannequin (Extri Kelly, 26 kg; Lærdal, Stavanger, Norway) was placed at 8 different locations in a lowland, hilly forest area. All scenes were unknown to the participating SAR crew members, and the simulation complied with the standard operating procedures (SOPs). The simulated operational setting was a time-critical situation at a scene that was inaccessible for GEMS and with no nearby landing site. Prior to all simulations, the crews were briefed before receiving the global positioning system coordinates of the scene. The hoist order to the scene in all simulations was as follows: first, the rescuer; second, the anesthesiologist; last, the rescue litter. This is the most common order during SAR missions, even though the rescuer and the anesthesiologist can be hoisted together or in the opposite order. The rescuer and anesthesiologist jointly packaged the mannequin and secured it in the litter. The anesthesiologist accompanied the mannequin on the rescue litter during hoisting from the scene. Finally, the rescuer was hoisted back to the cabin.
Time recording started when the airborne unit spotted the mannequin on the ground and recorded the following time points: when the rescuer reached the mannequin (rescuer–patient contact), when the anesthesiologist reached the mannequin (anesthesiologist–patient contact) and when the SAR unit was ready to start transport (start transport; Figure 3, red timeline intervals). No on-scene treatment or interventions other than extrication were simulated. Take-off times and flight times to the scene are already noted in the medical database and were thus not included in the simulation study. However, total hoist times were recorded to investigate the risk exposure of the patient and personnel. All times were recorded with a global positioning system clock device (Garmin Forerunner 620, Garmin, Schaffhausen, Switzerland) and exported to a Microsoft Excel (Microsoft Corporation, Redmond, WA) spreadsheet via Garmin software before being imported into IBM SPSS version 23 (IBM, Armonk, NY).
STATISTICS
Continuous data, including operational descriptors, patient characteristics, and times in the simulation study, are presented as mean ± SD. NACA scores are presented as modes. The χ2 test was used when assessing the difference in NACA scores between the medical and trauma groups. The t test was used when assessing the difference in take-off times when the crew was stationed in the hangar or was in quarters. All analyses were performed using IBM SPSS version 23.
ETHICS APPROVAL
The regional committees for medical and health research ethics/section southeast and the data protection officer at Oslo University Hospital classified this study as a quality assurance project not requiring approval. Dispensation from professional confidentiality requirements for other types of research was granted in accordance with research ethics/section southeast decision 2016/1072.
Results
EPIDEMIOLOGY OF SAR
A total of 1479 operations, 913 with the helicopter and 566 with the EMS vehicle, were completed during the study period. Five hundred (34%) of these were SAR helicopter operations. Of the SAR helicopter operations, 148 (30%) involved hoisting. Thirteen (9%) operations involved more than 1 person, and of the total 180 patients, 167 (93%) were extricated by hoist. The remaining 13 (7%) were extricated from the scene by collaborating HEMS with a static rope, referred to another EMS, or left at the scene after examination. Among the 148 hoist operations, 43 (29%) were performed outside of regular daylight hours. One adverse event was reported during the hoist operations, in which the helicopter downwash resulted in rockfall injuring 2 bystanders in a canyon. The 2 bystanders had minor injuries.
CHARACTERISTICS OF PATIENTS AND INCIDENTS
Of the 180 patients involved in the SAR operations, 88 (49%) were injured, and 53 (29%) had a medical condition (Table 2). The remaining 39 (22%) were uninjured but in need of evacuation because of potentially life-threatening situations (eg, members of a group with other casualties, people in drifting boats with engine trouble, or mountaineers who lost essential gear during climbing). Among the 180 patients involved in SAR operations, lower extremity injury was the most common traumatic injury (24% of the patients); the most common medical condition was neurologic disorders (8% of the patients). A total of 118 patients (66%) were men, 51 (28%) were women, and in 11 (6%) cases the sex was not reported (Table 3). In all the instances in which sex was not reported, the persons had no traumatic or medical condition. The age was 46 ± 19 y, with a range from 1 to 85 y. Nine patients were < 16 y old. The patients with a medical diagnosis had an age of 49 ± 19 y, as compared with the trauma patients with an age of 45 ± 18 y (P = 0.143). The age was unknown for 14 patients (8%) (1 with a medical condition and 13 evacuees). The patients were engaged in a variety of activities at the time of injury or illness (Table 4). A total of 128 (71%) were evacuated from land, and 38 (21%) were evacuated from a vessel, including 18 ferry passengers or employees on ships connecting Oslo with Denmark and Germany and 12 individuals (7%) evacuated from the water (Table 5). In 2 instances (1%), the scene characteristics were not reported.
Primary ICD-10 diagnosis of the patients, grouped
ICD-10, International Classification of Diseases, version 10.
Patient demographics
Activity of the patients at the time of the incident
Includes logging (3), suicide (2), and gardening.
Victims of flooding, uninjured.
Scenes of the incidents
The overall response time was 47 ± 28 min, including a total take-off time of 13 ± 7 min. The take-off time when the crew was quartered was 14 ± 7 min, as compared to a take-off time of 10 ± 4 min when the crew was stationed at the hangar (P = 0.012). The care time was 38 ± 23 min, including a scene time of 17 ± 13 min.
Hoist operations were performed more often during weekends (Saturday and Sunday; Figure 4) and more frequently in the period of May to July (Figure 5).
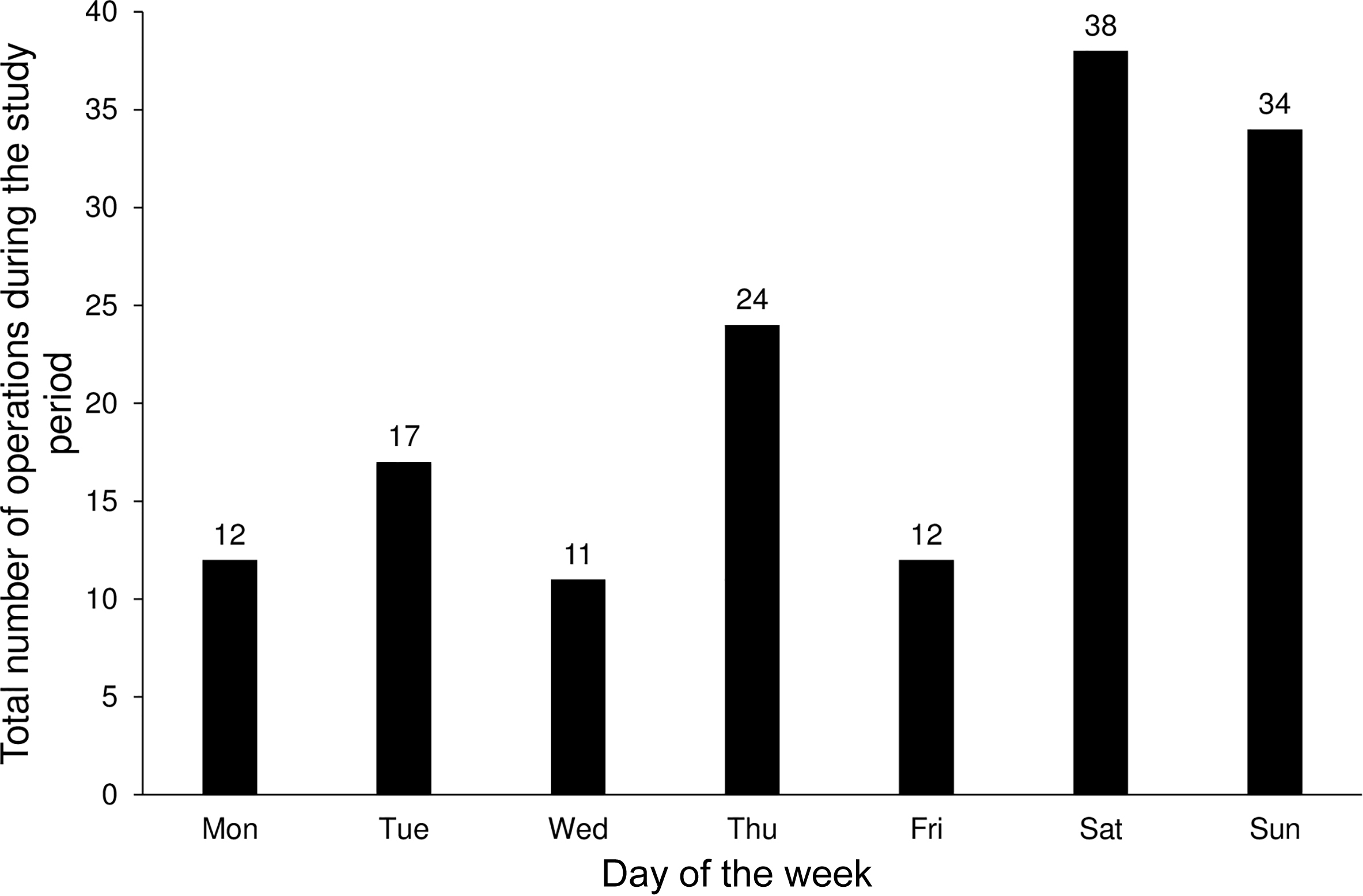
Total number of hoist operations by day of week during the 5-y period.
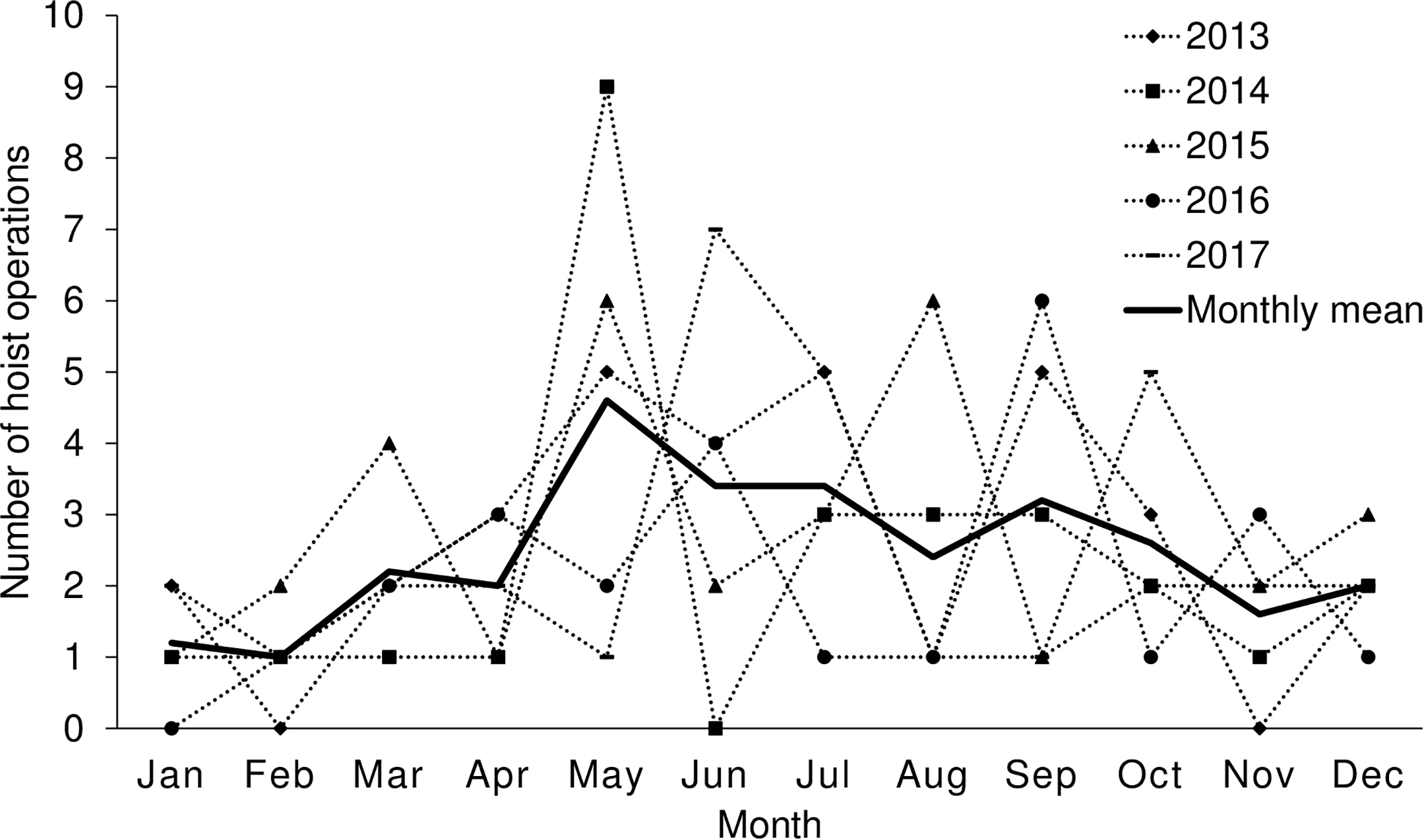
Number of hoist operations per month throughout the year for the 5-y period.
SEVERITY OF INJURIES AND ILLNESSES
The mode of the NACA score was 3 (Table 6). Forty-five patients (25%) had an injury or a medical condition, with a potential or actual life-threatening condition defined as an NACA score of 4, 5, or 6. Of the trauma patients, 21 (24%) had an NACA score of 4, 5, or 6. The corresponding number was 24 (45%) among patients with medical conditions (P = 0.026). Twelve patients (7%) had an NACA score of 7, of whom 7 (5 trauma patients and 2 with a medical condition) were pronounced dead at the scene.
Injuries and medical conditions by NACA score
NACA, National Advisory Committee for Aeronautics.
Of the 83 trauma patients who survived until reaching the hospital, 25 (30%) were admitted to the regional trauma hospital, 51 (61%) were admitted to local hospitals, 5 (6%) were referred to GEMS, and 1 (1%) was left at the scene after examination. In 1 (1%) instance, the destination was not reported.
Of the 51 medical patients who survived until reaching the hospital, 20 (39%) were admitted to university hospitals, 28 (55%) were admitted to local hospitals, and the remaining 3 (6%) were referred to GEMS.
MEDICAL INTERVENTIONS PERFORMED
Medical interventions were performed by the SAR unit on 77 patients (43%) in 73 operations (49%; Table 7). Oxygen treatment and analgesics were either initiated or continued in 42 (23%) and 35 (19%) patients, respectively. Nine patients (5%) were endotracheally intubated, of whom 8 patients were in cardiac arrest. An additional 2 patients (also experiencing cardiac arrest) were intubated by first-responding HEMS personnel prior to SAR arrival. Two of the endotracheally intubated patients were pronounced dead at the scene, and another 5 were pronounced dead in the emergency room at the hospital after continuous cardiopulmonary resuscitation during transport. Thoracostomy was performed on 1 trauma patient.
Interventions initiated or continued by the SAR crew
SAR, search and rescue.
SIMULATION STUDY
The rescuer access time was 4 ± 2 min, the anesthesiologist access time was 6 ± 2 min, and the total evacuation time for the 8 simulations was 13 ± 2 min.
The hoist time exposure for the rescuer was 1.6 ± 0.3 min, the anesthesiologist hoist time exposure was 1.7 ± 0.3 min, and the patient hoist time exposure was 0.8 ± 0.2 min.
Discussion
During the study period, hoist rescue was performed in 10% of all SAR operations. In a previous study, we showed that the corresponding proportion for HEMS static rope operations was 1%. 20 This shows that in this region of Norway, it is not often that patients need to be extricated by SAR or HEMS helicopter, but some of the extricated patients need immediate medical intervention. The high amount of hoist operations performed outside regular daylight hours, when HEMS static rope rescue is unavailable, highlights the importance of having a rescue service available at all times.
CHARACTERISTICS OF PATIENTS AND INCIDENTS
Patient age, sex, and condition resembled that reported in similar studies, both nationally and abroad. 14 ,20,21
The SAR take-off time when the crew was in quarters was 14 ± 7 min, and it was reduced to 10 ± 4 min when the crew was stationed in the hangar. This indicates that a way to avoid time delay is to station the crew in the hangar at all times and not only from 0730 to 1530. For severely ill or injured patients, reduced time in all phases of the mission is potentially beneficial. Persons in capsized boats and mountain climbers are examples of victims who can be in an exposed situation in which time to extrication is crucial even if they are not injured.
The median (quartiles) take-off time was 9 (5-13) min in HEMS static rope rescue operations. 20 In contrast to the SAR crew, the HEMS crew is stationed in the hangar at all times. The take-off times for the HEMS and SAR helicopters were almost identical during the part of the week that the SAR crew was stationed in the hangar. The SAR helicopter is bigger and has a larger crew; a longer take-off time was expected, so this finding was surprising. One explanation is that the SAR helicopter remains fully rigged for SAR hoist rescue operations, whereas the HEMS crew usually unloads unnecessary equipment to make room for static rope rescue equipment. Prevailing weight and space constraints prevent the HEMS helicopter from being equipped with a complete set of rescue equipment at all times. In situations when time is critical, optimal resource utilization can be crucial to the outcome. 22 The information that take-off times are comparable between SAR and HEMS helicopters can be useful when developing more precise dispatch criteria.
Almost half of the incidents occurred on Saturdays or Sundays. This is also the time when the most people are engaged in outdoor activities. The same temporal variation has been reported for HEMS static rope operations in the same region. 20 In addition, a seasonal variation was observed, with more incidents in the period May to July. This coincides with brighter days, the summer vacation, and the peak tourist season. Similar seasonal variations have also been found in other EMS systems. 4 ,23,24 One critical incident was reported among the 148 SAR operations. Among 59 HEMS operations in the same geographical region, no critical incident was reported. 20 However, the numbers are too small to evaluate whether one of the extrication methods is riskier than the other.
SEVERITY OF THE INJURIES OR ILLNESSES
Forty-five (25%) patients had an NACA score of 4 to 6, indicating a serious condition. Excluding uninjured evacuees, the proportion was 32%. In addition, 13 patients died (NACA score 7). This shows that even though the number of annual hoist operations was low, many patients were in need of rapid extrication to avoid potential deterioration. Patients with NACA scores < 4 may also profit from early medical assistance (eg, patients with painful extremity fractures in need of analgesics).
Patients with medical conditions had a significantly higher NACA score than trauma patients. This finding is consistent with results reported in other helicopter-based EMS studies in which patients with medical conditions had poorer outcomes and lower survival rates than those with traumatic injuries.14,25
MEDICAL INTERVENTIONS PERFORMED
Approximately half of the patients with trauma or a medical condition received medical treatment. The incidence of both endotracheal intubation and thoracostomy shows that advanced procedures were indicated in some cases. These findings are consistent with those of other studies. 14 ,20,21 According to the Norwegian SOPs, advanced prehospital life support procedures such as endotracheal intubation and chest tube drainage are normally performed by an anesthesiologist. The fact that the anesthesiologist has access to the patient at the scene, prior to extrication, is an argument for hoisting. According to the Norwegian Health Personnel Act, confirmation of death (NACA score 7) and the issuing of a death certificate can only be done by medical doctors. However, the requirements to professional conduct in emergency health care dictate the degree of autonomy health care providers have to initiate or to terminate advanced life support (ALS). This may represent another reason to bring the anesthesiologist to the patient before extrication. In certain situations, ALS can be stopped before performing a difficult hoist operation with ongoing cardiopulmonary resuscitation.
Several studies have indicated that prehospital treatment and helicopter transport improve patient outcomes. Trauma patients transported by helicopter were more likely to survive (odds ratio 1.22) and were more likely to be discharged home after treatment (odds ratio 1.05) when compared with those transported by ground ambulances, despite being more severely injured, having longer transport times, and requiring more hospital resources. 5 Patients with severe traumatic brain injury transported by HEMS had a lower rate of mortality (21%) compared with those transported by ground services (25%) and lower rate of severe neurological disabilities. 26 In a systematic review, some studies indicated a beneficial effect of ALS for patients with blunt head injuries or multiple injuries and suggested that ALS provided by paramedics and intubation without anesthesia could be harmful. 27 Another large multicenter cohort study found that prehospital management by emergency physicians in blunt trauma was associated with a significant reduction in 30-d mortality (odds ratio 0.55). 28
In Norway, the HEMS crew consists of 1 pilot, 1 rescuer, and 1 anesthesiologist. From the cockpit, the pilot cannot see the rescuer on the static rope or the patient on the ground. Therefore, the anesthesiologist operates as a navigator, guiding the pilot to the scene by radio communication, observations, and signals from the rescuer. One crew member in addition to the pilot must be on board the helicopter during static rope operations. According to the SOP this person is the anesthesiologist. In some countries, the rescuer can function as navigator while the physician is transported to the patient on a long line, but this is not the case in Norway. We believe that from a medical point of view, the anesthesiologist should get access to the patient as rapidly as possible. This implies that hoisting occasionally will be the preferred method within the restrictions of the existing Norwegian SOPs. An alternative would be to change the SOPs for HEMS static rope extrications, allowing the anesthesiologist to be on a long line in selected cases.
In Norway a specialty in emergency medicine was recently established. Such a specialist can be an acceptable alternative to an anesthesiologist when a patient is severely injured or ill and ALS skills are needed. However, the first Norwegian specialist in emergency medicine was authorized in July 2019 and it will probably take some years to see the full impact of this new specialty on the field of prehospital critical care.
SIMULATION STUDY
Hilly forest areas with no nearby landing site are highly representative of the geography in which land rescue typically takes place in this region of Norway. This kind of area was chosen for the simulation study.
An anesthesiologist access time of 6 ± 2 min suggests that hoisting enables early initiation of critical care procedures and administration of drugs that normally are provided exclusively by an anesthesiologist. It is reasonable to assume that hoist extrications are less time-consuming than static rope extrications because the HEMS helicopter must land and rig for static rope rescue before transporting the rescuer on a long line from the rig site to the scene. In a hoist operation, it is not necessary to land and rig. The hoisting can commence soon after the patient has been spotted. However, no studies reporting static rope rescue time expenditure have been published.
We have not included the entire response time in our study because the response time, among other factors, will be dependent on the location of the helicopter base relative to the scene of the accident, the speed of the helicopter, and the weather conditions.
Our results indicate that hoist extrication is rapid, but few studies have been published on this subject. 14 ,18,21 The rescue time intervals observed in this experimental study fill an information gap, providing points of reference for prehospital time intervals, allowing dispatchers and policymakers to compare different extrication methods of helicopter evacuation and improve operational planning.
LIMITATIONS
In-hospital data were inaccessible; therefore, it was not possible to determine morbidity and mortality or validate prehospital diagnoses. Nevertheless, other studies have found that NACA scores are significantly associated with clinical outcomes. 29 This study is retrospective, and the data variables are limited to existing registries. It is possible that time points and NACA scores were heterogeneously recorded by the different crews.
The external validity of the study is limited by the characteristics of the Norwegian SAR organization and similar EMS organizations abroad.
In Norway, the HEMS anesthesiologist cannot be transported on a long line to the patient. The evaluation of our findings may be different in HEMS systems where this is possible and allows the anesthesiologist to access the patient more quickly.
In time-critical situations it is beneficial to have the anesthesiologist on scene as rapidly as possible. Joint hoisting of both the rescuer and anesthesiologist is an advantage of SAR operations and was hence the intended hoist order in the simulation study. However, at the time of the study, there were restrictions on SAR hoist utilization due to ongoing troubleshooting that did not allow joint hoisting. Consequently, hoisting of the rescuer followed by the anesthesiologist and rescue litter was chosen because this was the most frequent hoisting order during SAR operations.
To compare the time course of the different extrication methods of hoist and static rope rescue, we had planned to simulate and time HEMS static rope extrication from the same locations. This was not possible because of safety concerns raised by the HEMS pilots, who declined to take part in such a study. The lack of static rope rescue simulation is a major limitation of the study.
Conclusions
Hoist rescue was performed in 10% (148) of the SAR operations. New information about hoist extrication time intervals can improve rescue helicopter dispatch accuracy.
Footnotes
Acknowledgments
We thank Hallstein Sørebø for data extraction from LabasNG, query building, and exporting of data.
Author Contributions
Study concept and design (MS, HE, JR, MS); acquisition of the data (MS); analysis of the data (MS, JR); drafting of the manuscript (MS, HE, LM, JR, MS); critical revision of the manuscript (MS, HE, LM, JR, MR, MS); approval of the final manuscript (MS, HE, LM, JR, MR, MS).
Financial/Material Support
The Norwegian Air Ambulance Foundation covered the salary for the corresponding author as a part-time research fellow. No other costs have accrued. No other sponsors or external sources of funding were involved in the study.
Disclosure
Martin Samdal and Helge Eiding are part-time research fellows at Norwegian Air Ambulance Foundation (NAAF). Lars Markengbakken is rescuer with a main responsibility of SAR hoist rescue. Jo Røislien is a professor of medical statistics at the University of Stavanger and a senior researcher at NAAF. Marius Rehn is a senior researcher at NAAF and a consultant anesthesiologist working at the Prehospital Division, Air Ambulance Department, Oslo University Hospital. Rehn is also an associate professor at the University of Stavanger. Mårten Sandberg works at the Prehospital Division, Air Ambulance Department, Oslo University Hospital and is a professor in prehospital emergency medicine at the University of Oslo, Norway. None of the authors have any other relationships, financial or personal, to disclose that could have inappropriately influenced this study.