
Abstract
Introduction:
Significant ventilator-associated pneumonia and mortality were found in COVID-19 patients who required mechanical ventilation which calls for non-invasive means in managing respiratory failure.
Methods:
We retrospectively reviewed patients admitted to the intensive care unit of Pamela Youde Nethersole Eastern Hospital in Hong Kong with severe acute respiratory syndrome coronavirus 2 infection from 28 November to 15 December 2020. Patients’ laboratory, respiratory parameters and outcome data were recorded and analysed.
Results:
Eleven received prone ventilation. The median age was 67 (inter-quartile range: 59–72) years, and median COVID-19 GRAM score was 151 (inter-quartile range: 133–181), representing a high-risk group. There were significant improvements 1 h after awake proning in SpO2 (95% vs 92%, p = 0.008), FiO2 (0.4 vs 0.5, p = 0.003), SpO2/FiO2 (240 vs 184, p = 0.005), respiratory rate (19 vs 26, p = 0.006) and respiratory rate – oxygenation index (13.22 vs 7.67, p = 0.003; Table 1). Although not reaching statistical significance, the median PaO2, PaCO2 and PaO2/FiO2 improved after proning. The overall intubation rate was 22% and intensive care unit mortality was 22%, which is in contrast to 65.5% and 27.6%, respectively, in the first three waves. Although did not reach statistical significance, those received prone ventilation tend to have a lower ICU mortality (9.1% vs 42.9%, p = 0.245) and hospital mortality (18.2% vs 42.9%, p = 0.326).
Conclusion:
Awake proning potentially minimizes complications from invasive ventilation and provides a low-cost low-risk treatment option in COVID-19 patients with respiratory failure. This is particularly important when healthcare resources are strained at times of a pandemic.
Keywords
Introduction
It has been 1 year since COVID-19 struck Hong Kong. To date, there have been more than 11,741 confirmed cases and 209 deaths, which has taken up 60% of intensive care unit (ICU) beds in Hong Kong. 1 Worldwide, it was estimated that around 5% of COVID-19 patients required intensive care, 2 and more than 50% mortality was observed in those requiring mechanical ventilation. This has called for non-invasive means in managing respiratory failure in COVID-19 patients.3–5
We share similar experience in Hong Kong. From February to August 2020 (the first three waves of COVID-19 outbreak), the intubation rate in our unit was 65.5%, compared to 61.3% among all COVID-19 patients admitted to other ICUs in Hong Kong. In our unit, Pamela Youde Nethersole Eastern Hospital (PYNEH), there were 32 critically ill COVID-19 patients admitted in the first three waves. There were 23 patients required invasive mechanical ventilation. We observed a higher incidence of ventilator-associated pneumonia (VAP; 23.8 vs 9.5 per 1000 ventilator days in non-COVID-19 patients; p = 0.16), difficult weaning and a high-mortality rate of 42.1% in mechanically ventilated COVID-19 patients. Since the start of the fourth wave in late November 2020, we sought to change the situation by adopting awake proning with high-flow nasal cannula (HFNC) or standard nasal oxygen therapy. Our primary outcome was intubation rate and secondary outcomes were respiratory physiological parameters, that is, SpO2, PaO2, FiO2, respiratory rate – oxygenation (ROX) index, ICU mortality and hospital mortality rate.
Methods
Study design and data collection
We retrospectively reviewed patients admitted to the ICU of PYNEH in Hong Kong with positive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in respiratory sample from 28 November 2020 to 15 December 2020. One patient electively intubated for procedure was excluded. PYNEH is a 1700-bed regional hospital that provide extensive services except cardiothoracic and burns. Our ICU is a mixed surgical and medical unit with 24 beds.
Non-intubated patients were encouraged to maintain a prone position (awake proning) and only returned to supine position for nursing care and interventional procedures. They were able to mobilize while in the prone position.
Patients’ medical records, data in clinical management systems and clinical information systems (IntelliVue Clinical Information Portfolio, Philips Medical, Amsterdam, Netherlands) were reviewed. Baseline demographics, laboratory, respiratory parameters and outcome data were recorded and analysed. Patients received dexamethasone, anti-virals or immunomodulatory agents after multidisciplinary discussion with in-house infectious disease specialists. Severity of illness was quantified by Sequential Organ Failure Assessment (SOFA) score 6 and COVID-19 GRAM score. 7
Statistical analysis
Continuous variables were compared between two time-points and three time-points using Wilcoxon signed rank test and Friedman test, respectively. Chi-square or Fisher’s exact tests were used to compare categorical variables. Statistical Package for Social Sciences for Mac, version 24.0 (SPSS, Chicago, United States) was used to perform analyses.
Ethics
This study was approved by the Hong Kong Eastern Cluster Ethics Committee of the Hospital Authority, and written informed consent was waived (HKECREC-2020-135).
Results
Eighteen patients were included, of whom 11 were men. Eleven of them received awake proning and seven did not. Patients who did not receive awake proning either could not cooperate or were already intubated prior to PYNEH ICU admission. Supplementary Table 1 showed the baseline demographics, laboratory parameters and outcome of the 18 patients. The median age was 67 (inter-quartile range (IQR) 59-72), median SOFA score was 6, and median COVID-19 GRAM score was 151 (IQR: 133–181), representing a high-risk group. 7 One patient received extra-corporeal membrane oxygenation (ECMO).
The median days from symptoms onset to ICU admission was 7.5 days (IQR: 5–10.5 days) and median fraction of inspired oxygen (FiO2) requirement was 0.5. Inflammatory markers were elevated with median C-reactive protein of 46 mg/L, lactate dehydrogenase of 377 IU/L and ferritin of 2164 pmol/L. One patient required continuous veno-venous haemofiltration and four patients received vasopressors.
The median prone duration was 18 h. There were significant improvements 1 h after awake proning in SpO2 (95% vs 92%, p = 0.008), FiO2 (0.4 vs 0.5, p = 0.003), SpO2/FiO2 (240 vs 184, p = 0.005), respiratory rate (19 vs 26, p = 0.006) and ROX index 8 (13.22 vs 7.67, p = 0.003; Table 1, Figures 1 and 2). Although not reaching statistical significance, the median PaO2, PaCO2 and PaO2/FiO2 showed improvement after proning. The overall intubation rate was 22% and ICU mortality was 22%, which is in contrast to 65.5% and 27.6%, respectively, in the first three waves. Although not statistically significant, those received prone ventilation had a lower ICU mortality (9.1% vs 42.9%, p = 0.245) and hospital mortality (18.2% vs 42.9%, p = 0.326). Two patients (2/11) failed prone ventilation and required intubation subsequently and one of the two patients died during ICU stay.
Parameter changes among patients received prone positioning (n = 11).
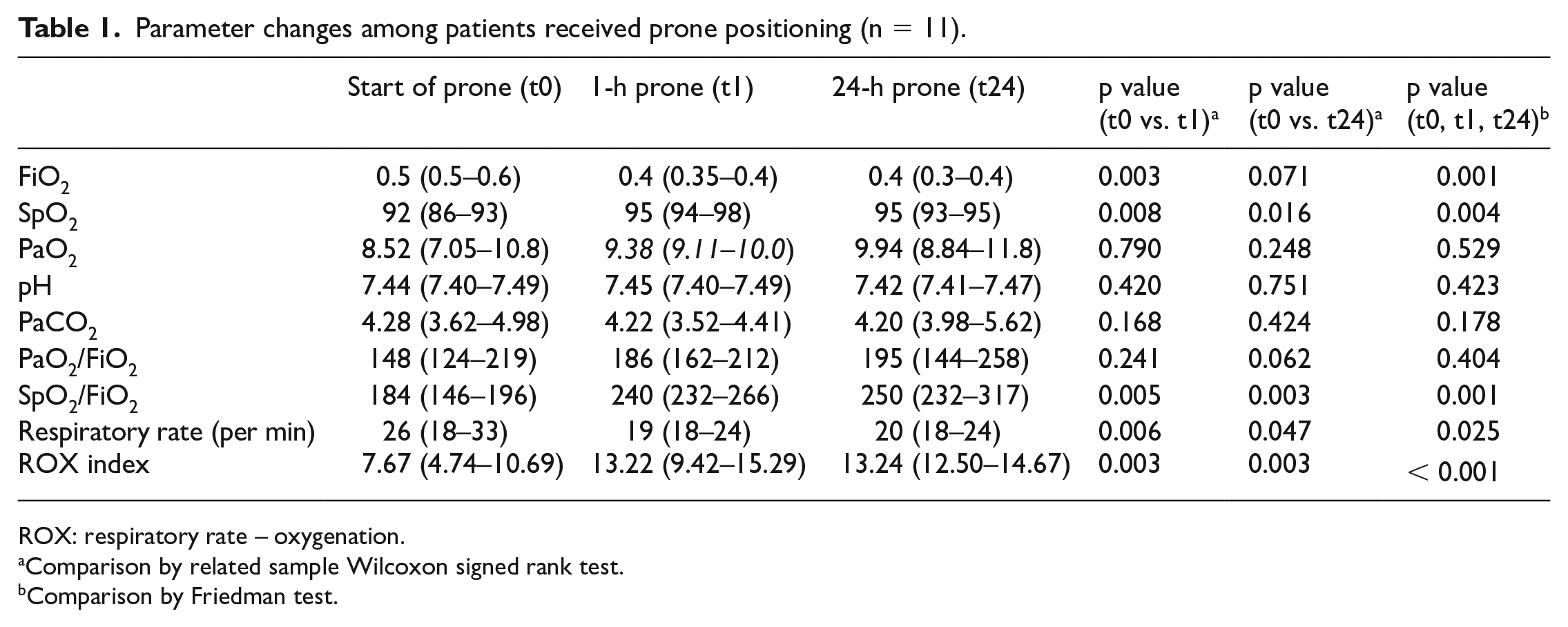
ROX: respiratory rate – oxygenation.
Comparison by related sample Wilcoxon signed rank test.
Comparison by Friedman test.
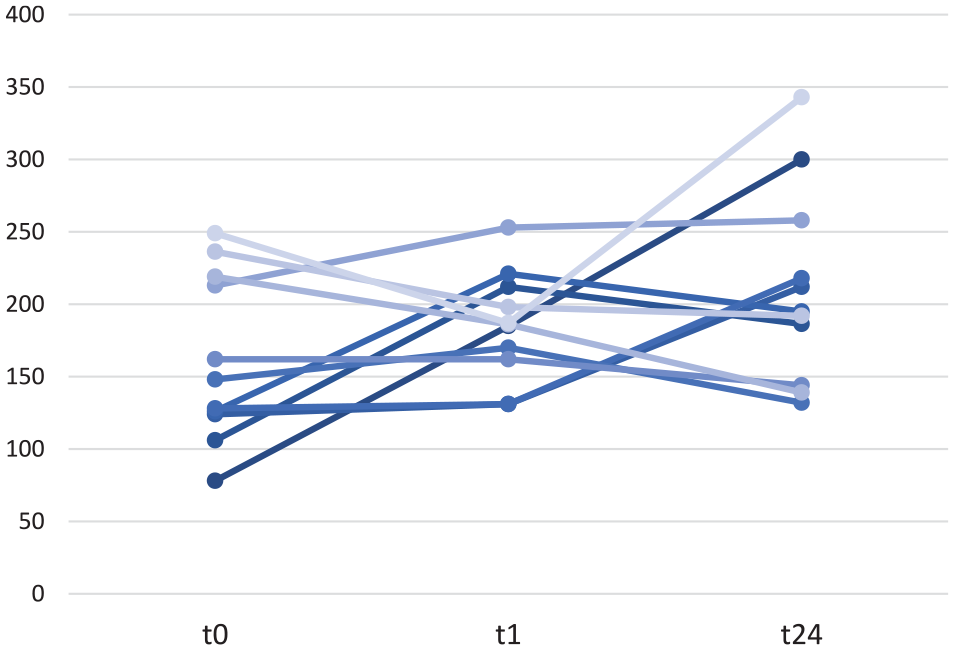
Change of PaO2/FiO2 ratio over time.
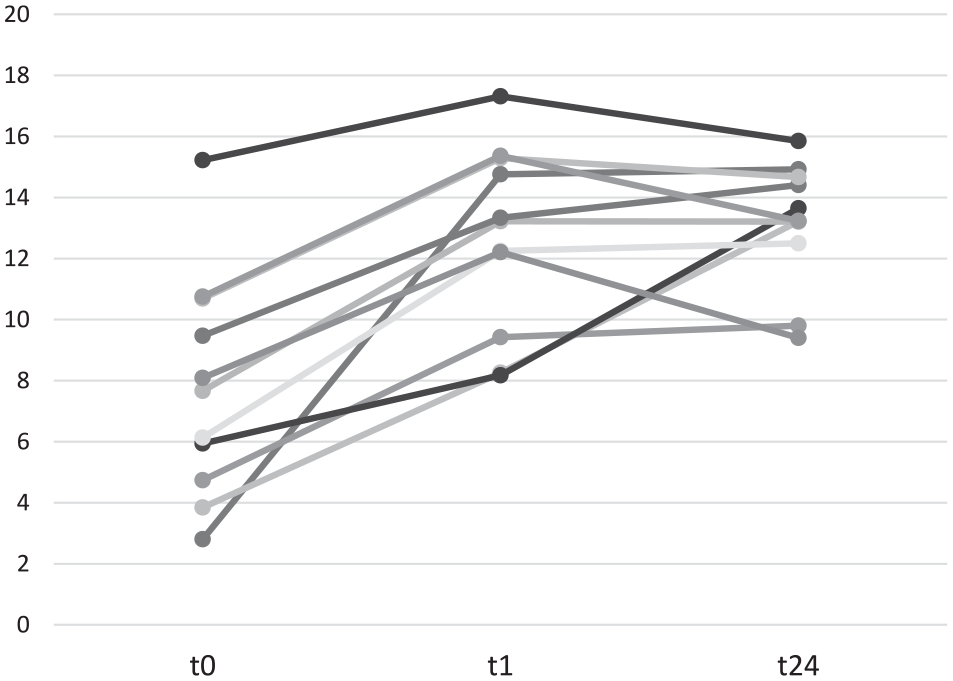
Change of ROX index over time.
As for adverse events on awake proning, two patients developed grade 1 pressure sore over the chin and face. There were no major haemodynamic compromise or dislodgements of important lines and tubings. There were six patients required sedative agents to facilitate prolonged proning and improve patients’ comforts.
Discussion
This is by far the first awake prone positioning study in non-intubated COVID-19 patients with respiratory failure in Hong Kong. Albeit a limited case series of 18, significant improvement in respiratory parameters and trend towards fewer intubation and ICU mortality were observed, highlighting the feasibility of awake proning and its potential benefits in patients with moderate to severe respiratory failure.
Recent studies reported short proning durations of 1–3 h per session. 9 As early prolonged proning (>16 h per day) has beneficial physiological effects in improving ventilation–perfusion matching, and homogenizing ventilation in mechanically ventilated patients, 10 our patients were encouraged to remain in the prone position as tolerated and repeated proning was recommended. The median prone duration was 18 h per day (IQR: 16–23 h), at times facilitated with the use of anxiolytics and analgesics.
In our cohort, a reduction in respiratory rate and PaCO2 were shown. HFNC provides better heated humidification and dead space flushing. A combination of HFNC and prone positioning may have additive effect in improving dyspnoea and reducing the work of breathing. 11 Coppo et al. 9 found a tendency towards reduced dyspnoea in patients who received prone positioning, and postulated that prone positioning may reduce self-induced lung injury. Patient’s subjective comfort and objective measurements of work of breathing maybe worth noting in future studies.
In Europe, a high VAP rate of 58% in ventilated COVID-19 patients was similarly observed. 12 The reasons for such a high VAP rate is likely multi-factorial. Vasculopathy, thrombosis and dysregulated inflammation commonly found in COVID-19 patients may predispose them to secondary bacterial infection. 13 On the contrary, prolonged mechanical ventilation together with immunosuppressants used as part of the treatment cocktails may further increase the risks of VAP.
While concerns may be raised in delaying intubation in patients receiving awake proning, 14 we believe close monitoring of patient’s clinical response and respiratory parameters in the ICU or high dependence units may identify early non-responders. Recently, the Intensive Care Society in the United Kingdom published a guideline on prone positioning in non-intubated patients with COVID-19, providing a pragmatic algorithm in the non-invasive management of COVID-19 with moderate-to-severe respiratory failure, and highlighted the importance of early trial with cautious reassessments. 15
There are several limitations to the current series. First, intubation criteria was not standardized but was based on intensivists’ clinical judgement. Second, compliance and patients’ comfort assessments by validated methods were not available in this cohort. However, analgesics and sedatives were liberally used to minimize discomfort and to facilitate proning. Due to small sample size, statistically significant comparisons between groups were suboptimal, future randomized controlled studies on awake proning will be needed to address the uncertainties, that is, optimal duration, timing of initiation, treatment endpoints, patient selection and predictors of prone-responders.
Conclusion
Awake proning is feasible and potentially minimizes complications from invasive ventilation and provides a low-cost low-risk treatment option in COVID-19 patients with respiratory failure. This is particularly important when healthcare resources are strained at times of a pandemic. We believe upcoming randomized controlled trials in awake proning are necessary to shed light on areas of uncertainties.
Supplemental Material
sj-pdf-1-hkj-10.1177_10249079211022914 – Supplemental material for Prone positioning in non-intubated patients with coronavirus – A single-centre experience in Hong Kong
Supplemental material, sj-pdf-1-hkj-10.1177_10249079211022914 for Prone positioning in non-intubated patients with coronavirus – A single-centre experience in Hong Kong by Man-Yee Man, Sin-Man Lam, Hoi-Ping Shum, Kin-Chio Li, Swan Lau, Vincent Hing-Lung Ip and Wing-Wa Yan in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
M.Y.M. carried out primary study search, data collection and drafted the manuscript. H.P.S. carried out primary study search, study design and statistical analysis. K.C.L., S.L. and H.L.I. carried out primary study search, data collection and drafted the manuscript. S.M.L. and W.W.Y. critically revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical and consent
This study was a retrospective study which did not involve alteration to clinical treatment. It was approved by the Hong Kong Eastern Cluster Ethics Committee of the Hospital Authority, and written informed consent was waived (HKECREC-2020-135).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.