
Abstract
Introduction:
Emergency department management of transient ischaemic attack varies from admission for all to outpatient referral. We studied the short-term outcomes of transient ischaemic attack managed with an agreed protocol. Predictors of stroke can be different for Asians and non-Asians. ABCD2 as initial triage of transient ischaemic attack is debatable. The predictive ability of ABCD2 score was studied as well.
Methods:
This was a prospective observational study with consecutive subject recruitment in Emergency department. All transient ischaemic attacks were admitted, hard and e-records of Emergency department, transient ischaemic attack clinic, Medical and Neurosurgical department and general follow-ups in Hospital Authority hospitals were studied up to 1 year. Stroke-day was measured from symptom-onset to time-of-stroke.
Results:
In 18-month period, 124 patients were recruited. The median onset-to-door time was 3.5 h. All computed tomography brain positive findings, except one subdural haematoma, were ischaemic in origin. Six strokes, all disabling, recurred within 90 days, three on day 1–3, two died in 6 months. The stroke risks at 2, 7, 90 days and 1 year were 1.61%, 3.23%, 4.84% and 4.84%, respectively. No significant trend was observed in stroke risk across ABCD2 scores (p = 0.783) with area under the curve of 0.537 (95% confidence interval = 0.380–0.694; p = 0.762). The short-term stroke risk was associated with atrial fibrillation (p = 0.002). The median Emergency Medicine ward length of stay was 1.33 days.
Conclusion:
In our Emergency department–based management, the short-term stroke risk of transient ischaemic attack is low, and the predictivity of ABCD2 score in risk stratification cannot be validated. Stroke recurrences were associated with atrial fibrillation. A low ABCD2 could be falsely reassuring. As half of the strokes recurred very early, we recommend admission in the hyperacute phase.
Introduction
Published findings on early strokes risks after transient ischaemic attack (TIA) were highly heterogeneous. 1 This can be accounted for by different study methods or clinical settings. There are findings of low stroke risk with patients managed in Emergency department (ED) by Emergency physicians and in a population base study with or without neurologist ascertainment.2,3
ABCD/ABCD2 scores in stroke risk predictive ability after TIA are conflicting, ranging from limited predictive ability to good external validity has been reported by studies other than the original derivation or validation studies.2–6 There are debates as to whether ABCD2 score is useful as a triage for urgent management, as stroke recurrences could occur in patients with low scores.7,8 Perry et al. 2 found ABCD2 inaccurate in imminent stroke prediction at any cut-point. Fothergill et al. 4 found 25% of low ABCD2 score patients with 7-day stroke.
Controversies do exist whether hospitalization is warranted for most of the TIA patients;7,8 decision in the acute management in ED varies from all admission to outpatient referral.1,5,9 Hoshino et al. 10 found that Asians had different predictors of stroke and lower recurrent stroke risk than non-Asians, ABCD2 being an independent predictor in non-Asians, but not in Asian, Asians have a lower rate of TIA, more small vessel disease, and a higher prevalence of intracranial stenosis.10–12
In Hong Kong, specialist Emergency Medicine (EM) physicians manage acute patients expected for a short stay in Emergency Medicine ward (EMW), with access to various modalities of investigations, inter-specialty consultation and are providing 24-h thrombolytic with neurologist cover. In collaboration with the neurologists, EM physicians have a role to play to minimize stroke risks in patients with TIA, by close neurological observation, investigations and early secondary prevention in EMW, instead of admitting all to medical ward where bed occupancy is always high. In this study, we aimed to investigate the short-term stroke risk and outcomes of Chinese patients presented as TIA in ED managed with an agreed protocol with neurologists (Appendix 1), and to evaluate the predictive ability of ABCD2 score in stroke risk.
Methods
This was a prospective observational study conducted in a major Hospital Authority (HA) public hospital with an annual ED attendance of 150,000 in Hong Kong. The HA is a statutory organization financed by the government to manage all public hospitals and provides universal access to primary, secondary and tertiary health care for the 7.5 million population. 13 All ED-diagnosed Chinese TIAs confirmed by EM physicians from 1 October 2011 to 31 March 2013 were consecutively recruited. TIA is defined as rapidly developed clinical signs of focal or global disturbance of cerebral function, lasting less than 24 h, with no apparent non-vascular cause. The primary outcome was stroke, using the WHO definition. 14 All patients for whom there was sufficient clinical suspicion with focal or global disturbance of cerebral function to justify diagnostic testing for a neurovascular cause were eligible for inclusion in this study. 5 The symptom-onset time and onset-to-door time (ODT) were precisely captured. All subjects were being followed up for 1 year from the index TIA through case notes and HA electronic Patient Record (ePR) that cover all ED attendances, hospital admissions, TIA clinic, all subsequent Specialist clinic and Family Medicine follow-up visits. The rate of stroke with 95% confidence interval (CI) was calculated at 2, 7, 90 days and 1 year from symptom-onset. The predictive capability of ABCD2 score in stroke risk stratification in TIA patients was assessed using the Mantel–Haenszel test for trend and receiver operating characteristic (ROC) curve. The association between history of atrial fibrillation (AF)/paroxysmal atrial fibrillation (pAF) and stroke was assessed by Fisher’s exact test. Statistical analyses were performed with SPSS (Windows version 23.0; IBM Corp, Armonk, NY, USA). Ethical approval for this study was obtained and the requirement for patient informed consent was waived, as patients were receiving the care usually provided.
Results
A total of 124 Chinese TIA patients (mean age = 65.3 ± 13.7 years; 55.6% male) were recruited and followed up for a year (Figure 1). Table 1 shows the demographic and clinical characteristics. The median ODT was 3.5 h ranging from 0.2 to 159.7 h. There were 47.6% (59/124) and 88.7% (110/124) patients with ODT <3 and <24 h, respectively. All patients underwent computed tomography (CT) brain scan, of whom 60.4% (75/124) and 88.7% (110/124) done within 6 and 12 h from ED registration, respectively. Fifty-nine patients (47.6%) had normal findings. All positive findings were ischaemic in origin, except one with subdural haematoma. Aspirin was started once CT brain confirmed no haemorrhage. Eighty of the 95 (84.2%) patients who were not already on antiplatelets or anticoagulants were prescribed aspirin, of whom 67.1% and 96.1% were started within 24 and 48 h after ED registration, respectively (Table 1).
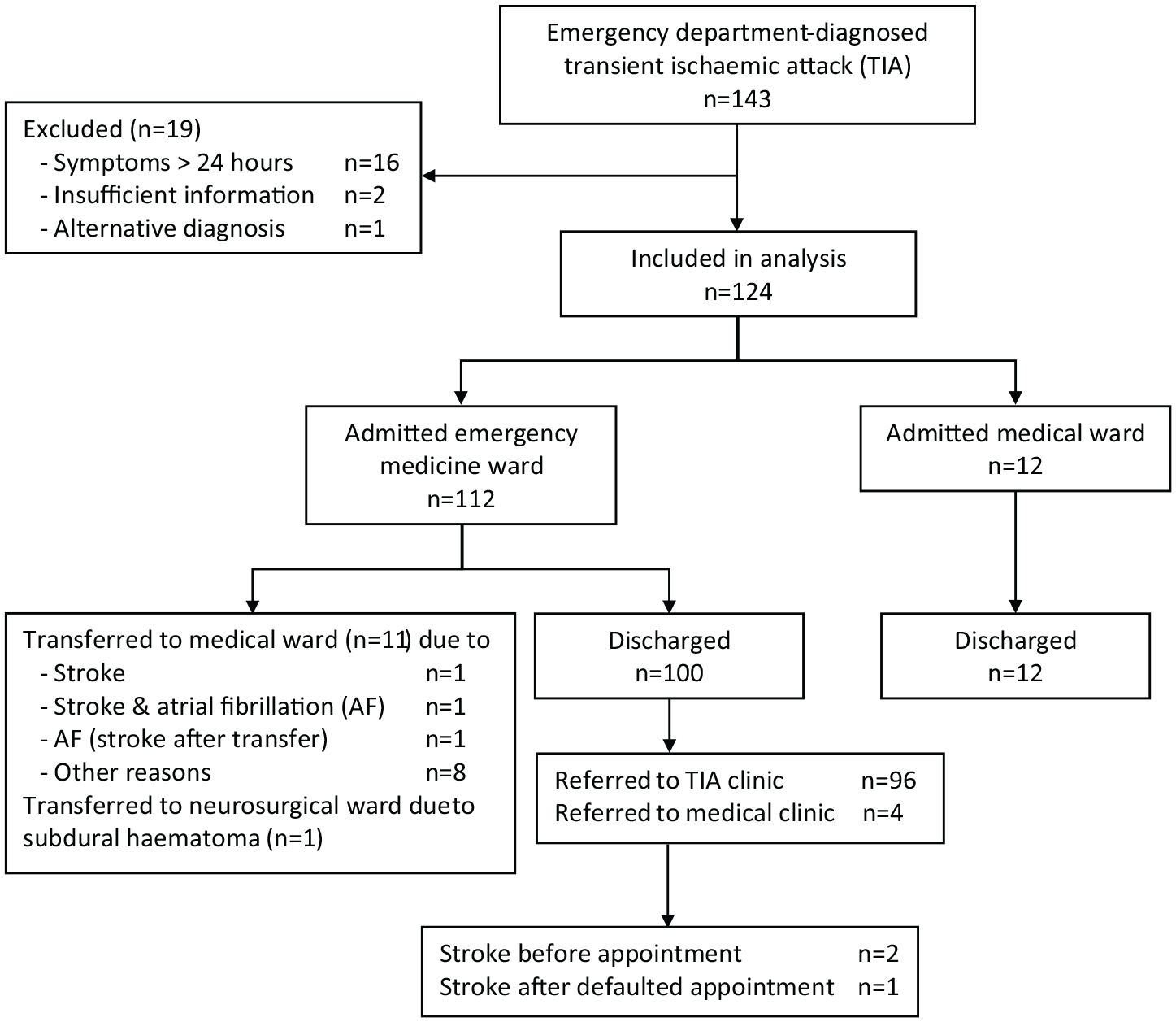
Recruitment flow chart of patients with transient ischaemic attack (TIA).
Baseline characteristics, investigations and disposition of transient ischaemic attack patients (n = 124).
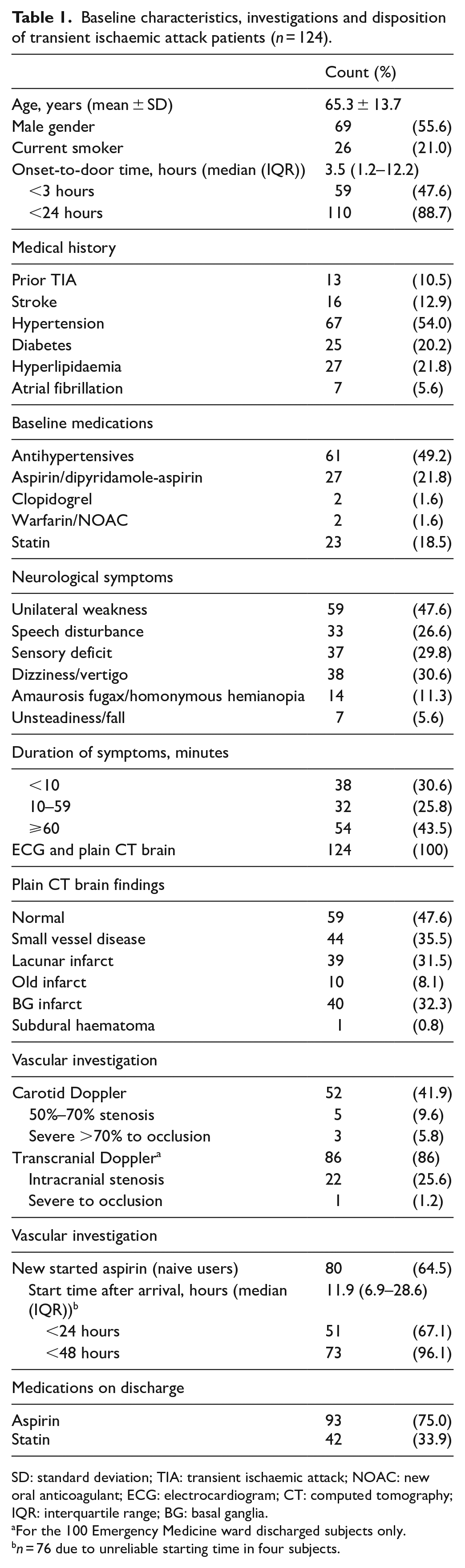
SD: standard deviation; TIA: transient ischaemic attack; NOAC: new oral anticoagulant; ECG: electrocardiogram; CT: computed tomography; IQR: interquartile range; BG: basal ganglia.
For the 100 Emergency Medicine ward discharged subjects only.
n = 76 due to unreliable starting time in four subjects.
Stroke risk/recurrent TIA
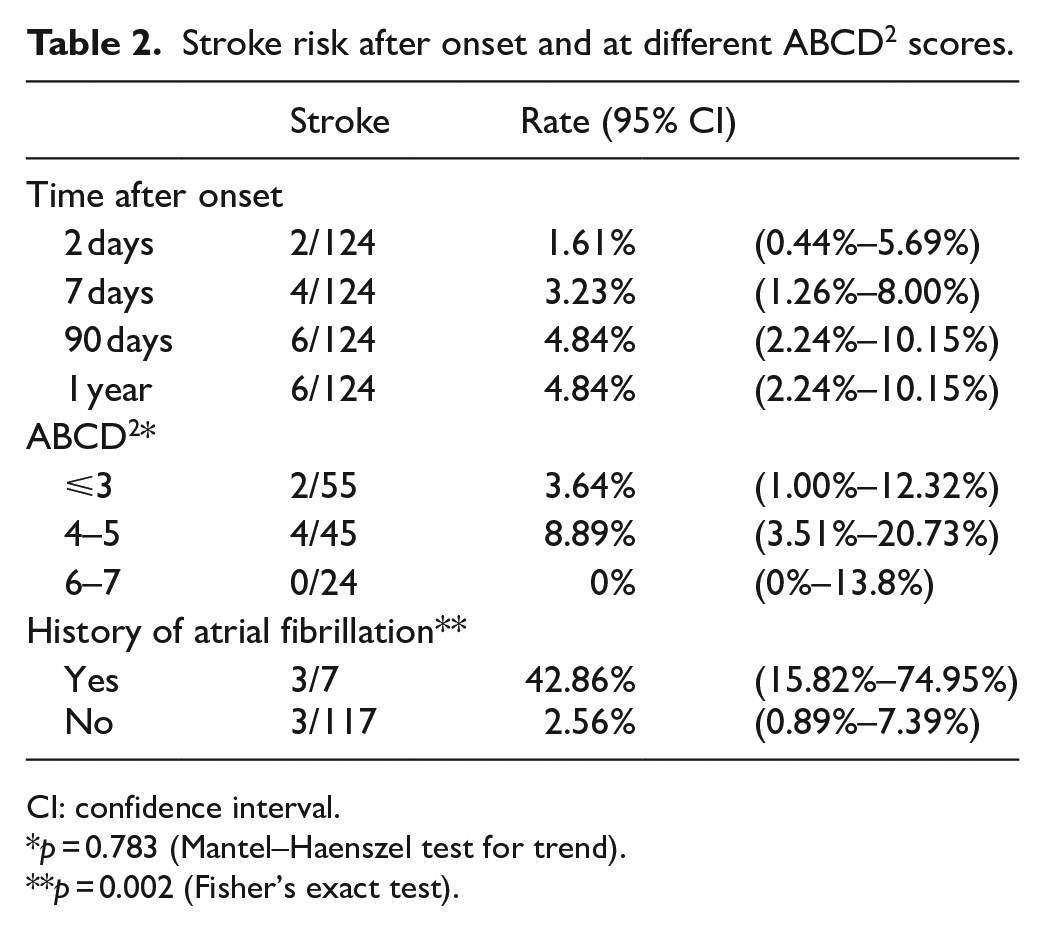
Six patients in total developed stroke on day 1, 2, 3, 4, 13 and 30, respectively, two in EMW and one in acute stroke unit (ASU) (Figure 1). One of them had a second stroke at 4 months. The cumulative stroke risks at 2, 7, 90 days and 1 year were 1.61%, 3.23%, 4.84% and 4.84%, respectively (Table 2). The rate of stroke for ABCD2 score ⩽3, 4–5 and 6–7 was 3.64% (2/55), 8.89% (4/45) and 0% (0/24), respectively. No significant trend was observed in stroke risk across ABCD2 scores (p = 0.783). The area under the ROC curve (AUC) of 0.537 (95% CI = 0.380–0.694; p = 0.762) indicated a low predictive ability of ABCD2 score on stroke risk (Figure 2). Three of the seven patients with AF/pAF, all not anticoagulated, had stroke recurred on day 2, 3 and 13, and died 14 months, 6 months and 87 days, respectively. Two of the four early strokes that recurred within 7 days were in AF; these two AF patients had stroke recurred at 24 and 50 h after admission. All four were major strokes, their ABCD2 score being 4, 3, 5 and 2, respectively (Table 3). The short-term stroke risk after a TIA was associated with a history of AF (p = 0.002; Table 2). The patient who developed stroke on day 4 had severe intracranial stenosis in the left anterior cerebral artery and right posterior cerebral artery detected in transcranial Doppler (TCD), with no extracranial stenosis. No severe intra or extracranial stenosis was detected in the other five stroke cases. Seven patients had recurrent TIA in 1 year, five being ascertained TIA in Medical ward (n = 4) or TIA clinic (n = 1), one labelled ‘not TIA’ in TIA clinic had recurrent TIA and one defaulted the appointment. None of them developed stroke in 1 year.
Stroke risk after onset and at different ABCD2 scores.
CI: confidence interval.
p = 0.783 (Mantel–Haenszel test for trend).
p = 0.002 (Fisher’s exact test).
Description of the six stroke cases.
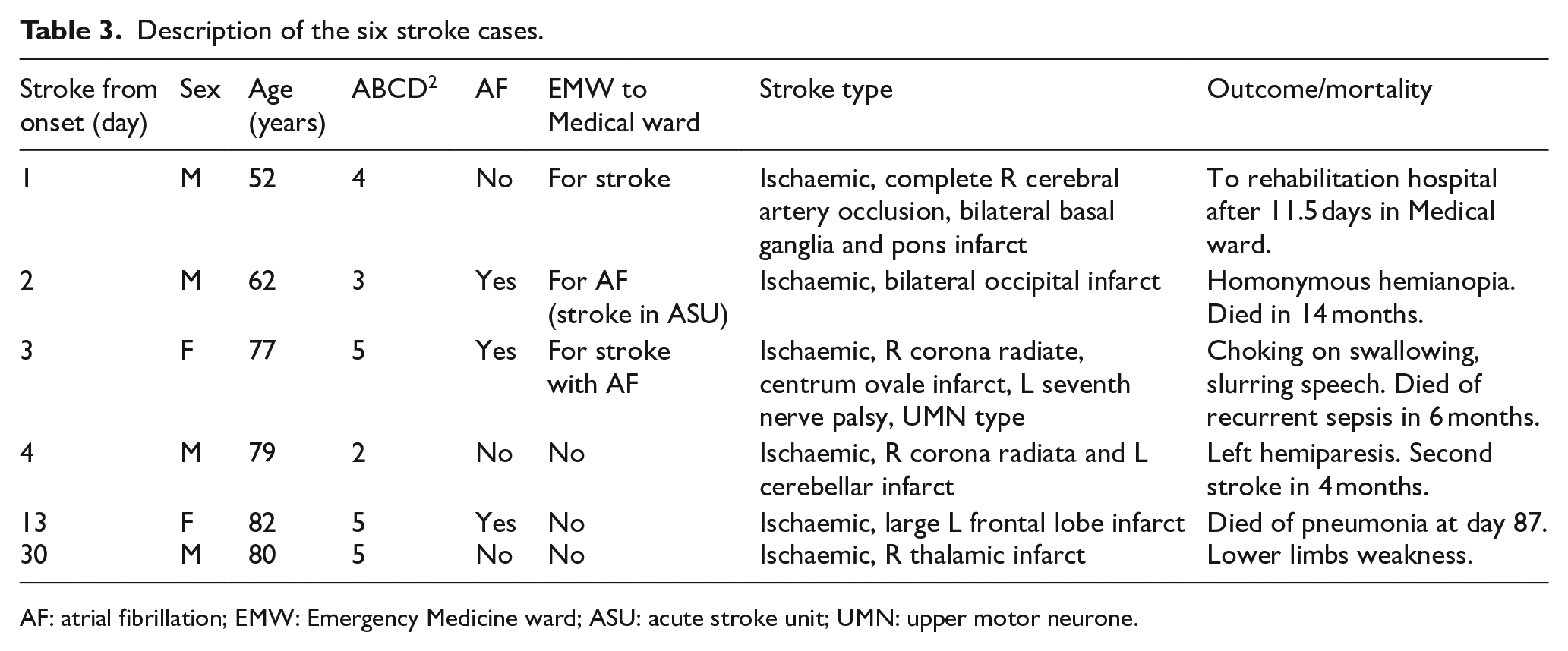
AF: atrial fibrillation; EMW: Emergency Medicine ward; ASU: acute stroke unit; UMN: upper motor neurone.
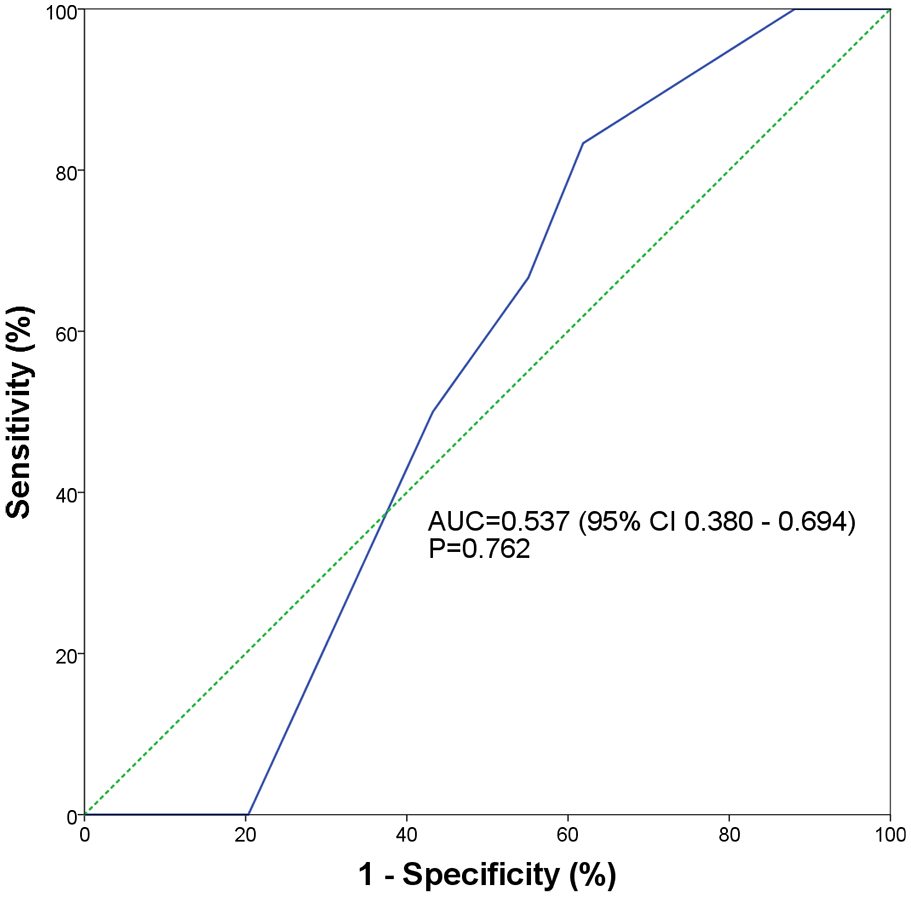
Receiver operating characteristics curves (ROCs) of ABCD2 score for predicting 90-day stroke recurrence.
Length of stay
Of the 112 EMW admissions (Figure 1), 100 (89.3%) patients were discharged from EMW with a median length of stay (LOS) of 1.33 days (interquartile range (IQR) = 0.93–1.93 days; 93.7% stayed <3 days). Eleven EMW patients were transferred to Medical ward for stroke recurrence, AF, fall assessment and prevention, other comorbidities or social reasons, and one patient with subdural haemorrhage with left chronic subdural haematoma was transferred to Neurosurgical ward. The median LOS of the 12 patients directly admitted to Medical ward was 0.95 day (IQR = 0.77–2 days).
TIA clinic within 2 weeks
There were 96 patients discharged from EMW being referred to TIA clinic (Table 4). Three could not be assessed in the TIA clinic, as two strokes recurred before the appointment and one stroke recurred after defaulted the appointment. All these three stroke patients were hospitalized with significant morbidity (Table 3). Among the 91 patients who attended the TIA clinic, 32 (25.8% of the cohort) were TIA mimic or ‘not TIA’. The TIA mimics were migraine, hypoglycemia, cervical spondylosis, subclavian steal, drug induced dystonia and anxiety. The ‘not TIA’ were migraine, transient diplopia, blurring of vision, vertigo, depression, hand clumsiness, numbness, anxiety, transient global amnesia and five inconclusive diagnoses. One ‘not TIA’ had a recurrent TIA after 5 months had L middle cerebral artery stenosis. If ‘TIA mimic’ and ‘not TIA’ (n = 32) were excluded, the stroke risk at both 90 days and 1 year would be 6.52% (6/(124-32)) and that for EMW discharged patients only would be 4.69% (3/(96-32)). No neurologist-ascertained TIA/minor stroke or probable TIA developed stroke in 1 year.
Outcome/diagnosis of Emergency Medicine ward discharge cases referred to TIA clinic (n = 96).
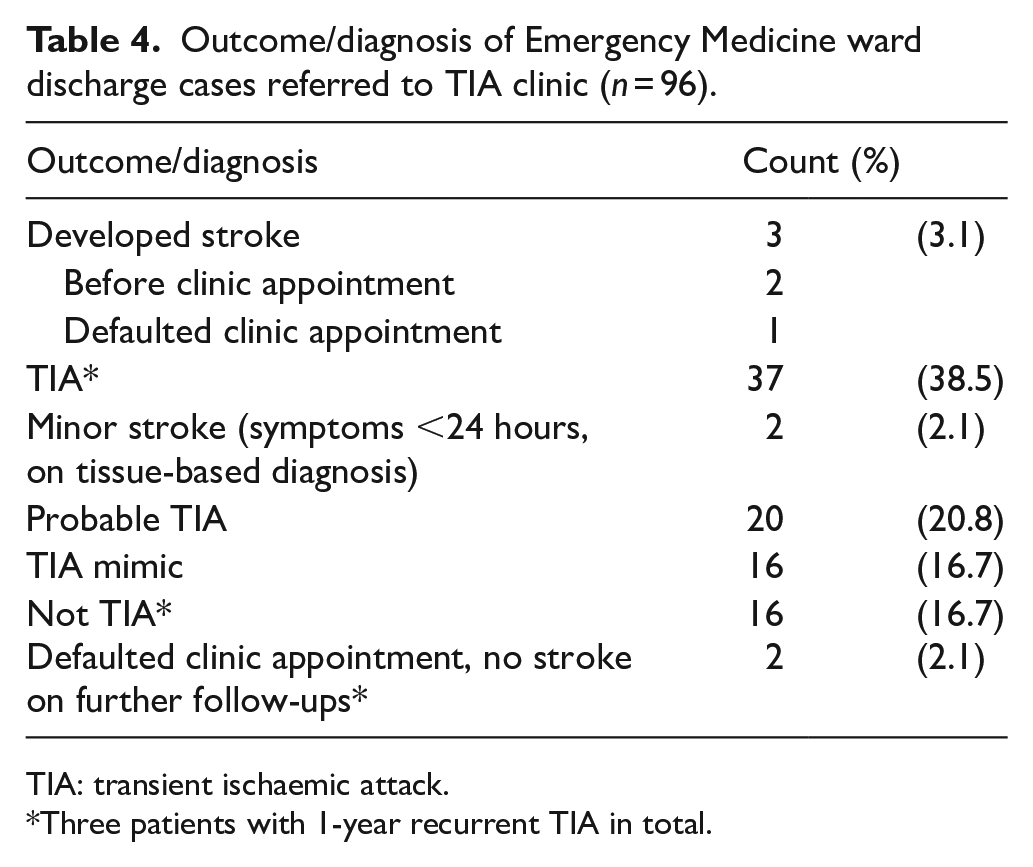
TIA: transient ischaemic attack.
Three patients with 1-year recurrent TIA in total.
Discussion
Stroke risk after TIA
The short-term stroke risk in this cohort is low with 1-year stroke risk as 4.84% (95% CI = 2.24%–10.15%), which is consistent with findings of a retrospective study in Hong Kong Chinese, an international study using TIAregistry.org and a Western multicentre study.2,10,15 The highly heterogeneous findings of early strokes risks after TIA can be explained by various methodology, clinical settings and ethnicity factor.1,10–12,15 One may attribute the low risk to possible overdiagnosis or to the early aspirin.16–18 But the benefit of aspirin per se in preventing short-term stroke cannot be overestimated.17–19 A combined analysis of 40,000 patients from the Chinese Acute Stroke Trial and the International Stroke Trial shows an absolute risk reduction of only 0.7% in stroke recurrence for the group given aspirin in the first 48 h. 19 Dual antiplatelet therapy (DAPT) with clopidogrel and aspirin given within 24 h further reduces the stroke risk by 2%–3.5%. Since it is not ethical to withhold aspirin in this study protocol, we started monotherapy with aspirin early, 67.1% <24 h after ED registration, to our patients who never had aspirin before. This is comparable to Johnston’s pioneer article, where patients in the derivation and validation groups of the ABCD2 score to predict very early stroke risk after TIA were also treated groups, given aspirin (47%–89%), ticlopidine/clopidogrel (0%–16%) and anticoagulation (4%–14%). 20 Many studies include TIA and minor stroke in stroke risk calculation,10,17,18 because the distinction between TIA and minor stroke is imprecise and remains controversial, as the definition of using cut-off time of symptoms resolved within 24 h is purely arbitrary before the era of imaging. 21 If minor strokes with symptoms >24 h but with complete recovery were included in this study, the stroke risk would be even lower.
ABCD2 score in risk stratification
There is no significant trend observed in stroke risk across ABCD2 scores in our cohort. The low AUC of 0.537 (95% CI = 0.380–0.694) shows that ABCD2 score has limited predictive value in risk stratification. Similar result was demonstrated in a multicentre prospective study in EDs with an AUC of 0.56 (95% CI = 0.47–0.65). 2 Hoshino et al. 10 found the ABCD2 score predictive ability was similar between Asians (C statistic = 0.595) and non-Asians (C statistic = 0.596). A low ABCD2 score could be falsely reassuring as patients with low score could still develop stroke within 2–7 days.2–4,7,8,22 All our six stroke cases had ABCD2 score ⩽5 (presumed not high risk), of whom two early stroke recurrence had score 2 and 3, while a TIA mimic with subdural haematoma scored 2. The National Institute for Health and Care Excellence UK (NICE) 2019 Stroke and TIA guideline recommends that ‘do not use scoring systems, such as ABCD2, to assess risk of subsequent stroke’ in the initial management of suspected or confirmed TIA in the 48 h after symptoms onset. In this study, if ABCD2 scores were used as the only triage reference, some very early stroke recurrences and non-benign TIA mimics would have been missed. Admission of TIA patients for acute observation with ready access to thrombolysis irrespective of ABCD2 scores is therefore recommended.
AF and stroke risk
The association of non-anticoagulated AF with stroke after a TIA in our cohort was significant. Three of the seven AF patients developed major strokes on day 2, 3 and 13, with a high mortality (two died within 1 year and one in 14 months). Early anticoagulation should be considered for TIA patients with new or known AF after admission. 22
Short ODT
In early 2000s, stroke patients were still presenting late, 44.4% ⩾1 day.23,24 As public awareness is increasing in ‘Golden hours in stroke’ through social media, patients were presenting much earlier over the past two decades in Hong Kong.24,25 A long, or imprecise ODT, and day-of-stroke measured from the time-of-presentation would result in unreliable 2-and 7-day stroke risk, as most strokes recur very early, patients who arrive 3 days after TIA are past the period of highest risk.2,6 When TIA patients with very early stroke recurrence were presenting late, they would present with stroke rather than TIA and could not be captured and included in very early stroke risk calculation. Patients who delay to present might present as stroke recurrence after TIA, and so could not be captured as TIA. The ODT in our cohort is short and precisely captured, with a median of 3.5 h (IQR = 1.2–12.2; 47.6% <3 h), and we measured day-of-stroke from symptom-onset instead of from ‘time-of-presentation to stroke recurrence’, both enable a more reliable stroke risk calculated.3,20
The admit-or-discharge controversy
Three major strokes recurred after admission from day 1 to day 3, which is comparable to the finding half of all recurrent strokes during the 7 days after a TIA occurred in the first 24 h.2,6 Two more discharged patients had stroke recurred before the TIA clinic appointment. The safer way is to admit all TIA patients to stay for 2 days in the acute phase for early secondary prevention and neurological observation to avoid missing the ‘Golden hours in stroke’.
There are concerns of over-admission, as 32/124 of our cohort were TIA mimic and non-TIA. In a survey of stroke prevention clinics in the United Kingdom, the proportion of patients with a final diagnosis of TIA/minor stroke was between 11% and 60%, 26 and a significant number of patients referred as TIA had a final diagnosis of a non-cerebrovascular event or TIA mimic after expert assessment.16,22,27
However, observer agreement for the diagnosis of TIA among physicians is poor. 16 The discrepancies in diagnosis among stroke-trained neurologists regardless of the statistical test used further complicate the position of mimics and ‘probable TIA’. 28 Even some ED-diagnosed TIA finally diagnosed as mimics, they are not all benign, some do involve serious conditions that warrant urgent treatment. 27 One of our TIA mimics found to have subdural haematoma, score 2, had an uneventful recovery after burr hole drainage.
Brain imaging cannot be the solution of discrepancies in TIA diagnosis either, as a normal CT or magnetic resonance imaging (MRI) is still compatible with a definite TIA diagnosis. A meta-analysis with 9078 definite TIA patients from 47 studies revealed that on average 65.7% patients with definite TIA had a negative MRI diffusion-weighted imaging (DWI) finding, which could not be explained by available data. 29 There are still limitations in timely brain imaging availability, and in the timing of image being positive, with the DWI-positive rate varied with time between TIA and scanning, ‘DWI lesions may disappear very rapidly, being present at 4 hours after symptom onset but resolving completely from DWI and other MR sequences by 24 hours’. 29 Diagnosis of TIA still rests on clinical diagnosis rather than tissue-based. 30
To admit or to discharge becomes a consideration in resource availability, hospital LOS and immediate availability of tissue plasminogen activator (tPA). SOS-TIA can afford ‘one-stop’ hospital clinic service with 24-h access to neurologist assessment, neural, arterial and cardiac imaging within 4 h, 22 or EXPRESS service with neurologist assessment within 3 days; 17 while some provide non-emergency outpatient assessment that patients could have no evaluations within 1 month. 9 Either round-the-clock SOS-TIA, 22 EXPRESS service, 17 or immediate discharge with non-emergency outpatient assessment are on the extremes of the spectrum in management. 9 Given the high very early stroke risk after TIA, discrepancies in TIA diagnosis among neurologists even with brain imaging, limited predictivity of ABCD2 score, possible non-benign mimics and a short LOS (mean 1.33 days) in our cohort, we recommend TIA patients with high likelihood of impending stroke, especially those with a thromboembolic source, for example, AF, or severe intra/extracranial stenosis, be admitted for early secondary preventions, and to avoid missing the ‘Golden hours’, when specialist Emergency physicians are providing thrombolytic with neurologist cover.
Fast-track TIA clinic
In this study, patients discharged from EMW were referred to TIA clinic within 2 weeks. As most (5/6) of our strokes occurred prior to the clinic appointment, the agreed waiting time of ⩽14 days is suboptimal. A fast-track TIA clinic within days might further minimize stroke risk, where neurologists can further investigate as in this cohort, for example, MRI/magnetic resonance angiography (MRA), CT angiogram, 24 h Holter to detect pAF to start anticoagulation; referral to cardiologists for echocardiogram, to identify cardioembolic sources in patients with low ejection fraction or with patent foramen ovale; to neurosurgeon for carotid endarterectomy/stenting for patients with severe carotid stenosis.
Strengths and limitations
This study used a prospective observational design with consecutive subject recruitment. The short ODT in our patients (median = 3.5 h, IQR = 1.2–12.2; 47.6% <3 h) enables reliable stroke risk calculation, as patients who arrive 3 days after symptom-onset are past the period of highest risk, 6 and day-of-stroke measured from symptom-onset enables a reliable stroke risk calculation. Our ODT were precise because the presentation time to ED was electronically captured, symptoms recall bias by patients and the patients’ relatives who witnessed the event would be low because our patients presented early, as accurate diagnosis relies heavily on the patient’s account of their history. Nowadays, patients attend and arrive early at ED as the first medical contact after TIA. The ED-diagnosis approach reflects patient care in ‘real-life’ setting as in Rothwell’s and Johnston’s pioneer articles and Sheehan’s article, where probable and suspected TIAs are included.3,20 Our practice of ED-led instead of awaiting neurologist assessment on decision on early treatment and investigations is more relevant to our everyday patient care. The limitation in this study is that this is a single-centre study with a relatively small sample size. The number of carotid Doppler and transcranial Doppler done in the cohort was inadequate and the timing of investigation was suboptimal. Further multicentre studies with radiologist collaboration in Hong Kong are recommended.
Conclusion
In our ED-based management, the short-term stroke risk of TIA patients was low. Our prospective cohort cannot validate a high predictive value of ABCD2 score in risk stratification. A low ABCD2 could be falsely reassuring. Early stroke recurrence was associated with AF. As half of the strokes recurred very early, we recommend admission in the hyperacute phase.
Supplemental Material
sj-pdf-1-hkj-10.1177_10249079211004319 – Supplemental material for Short-term outcomes of Chinese transient ischaemic attack patients in an Emergency department in Hong Kong: Result of management with an agreed protocol with neurologists
Supplemental material, sj-pdf-1-hkj-10.1177_10249079211004319 for Short-term outcomes of Chinese transient ischaemic attack patients in an Emergency department in Hong Kong: Result of management with an agreed protocol with neurologists by Simon Lai Hong Chiu, William Cheung Lun Wong and Ellen Lok Man Yu in Hong Kong Journal of Emergency Medicine
Footnotes
Appendix
Acknowledgements
The authors thank all the medical and nursing staff in Accident & Emergency Department, Princess Margaret Hospital for subject identification, Ms May Ng who helped keep good case records and cases tracing in Emergency Medicine ward. The authors also thank Ms Amelia Wong (RN) on retrieving all hard and e-records with all the help of medical record office and IT department, Princess Margaret Hospital. The authors also thank Neurology team, Princess Margaret Hospital, especially Dr B Sheng and Dr KK Lau, for writing the protocol for TIA management.
Author contributions
S.L.H.C. and W.C.L.W. researched the literature, conceived the study and were involved in protocol development, gaining ethical approval, patient recruitment and data acquisition. All authors were involved in data analysis and interpretation. S.L.H.C. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
The requirement for patient informed consent was waived, as patients were receiving the care usually provided.
Ethical approval
Ethical approval for this study was obtained from the Kowloon West Cluster Research Ethics Committee, Hospital Authority (reference no. KW/EX-13-027(60-11)).
Human rights statement
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.