
Abstract
Introduction:
Ultrasound guidance is commonly used during central venous cannulation. Subclavian vein is a commonly chosen site, but previous studies found varying results in the ideal positioning of the shoulder for subclavian vein cannulation. The objective of this study is to determine which shoulder position results in the greatest cross-sectional area of the right subclavian vein for cannulation.
Methods:
In this prospective observational study, ultrasound was performed on healthy adult volunteers to visualise the right subclavian vein in three different shoulder positions: neutral, abduction and retraction. A blinded independent investigator measured the cross-sectional areas by computer software using planimetry method. Statistical analysis was performed by one-way repeated measures analysis of variance.
Results:
Forty-four adults participated in the study. The mean cross-sectional area of the right subclavian vein in shoulder neutral, abduction and retraction positions were 1.05 ± 0.33 cm2, 1.01 ± 0.31 cm2 and 0.82 ± 0.28 cm2, respectively. When compared to shoulder retraction, the cross-sectional areas were significantly increased in shoulder neutral (P < 0.01) and abduction (P < 0.01) positions. There was no significant difference between shoulder neutral and abduction position (P = 0.71).
Conclusion:
Positioning the shoulder in neutral or abduction results in the greatest cross-sectional area of the right subclavian vein and may be more ideal for ultrasound guided cannulation.
Introduction
Background and rationale
Central venous catheter (CVC) insertion is an essential skill for managing critically ill, sepsis and trauma patients commonly encountered in the emergency department.1–6 The internal jugular, femoral and subclavian/axillary vein (SV) are often used for cannulation. Centers for Disease Control and Prevention (CDC) guidelines recommended placing subclavian lines in adult patients as it is associated with fewer catheter-related infections. 7 It is also associated with a lower risk of catheter-associated deep vein thrombosis. 8 Under certain clinical situations, it may be most appropriate site, such as in polytrauma with cervical spine injury. However, SV cannulation is associated with potential serious complications, such as pneumothorax, haemothorax and arterial puncture.8,9 Existing evidence suggests that ultrasound-guided SV cannulation increase the success rate and reduce complication rate when compared to landmark-guided technique.10–12
Due to SV’s anatomical site and its surrounding fascial attachments, different shoulder positions may alter its local anatomical relations and the cross-sectional area (CSA), thus affecting the cannulation. However, previous studies found varying results in the ideal positioning of the shoulder for SV cannulation.
The ‘classical’ position for SV cannulation is the retracted shoulder position, achieved by placing a shoulder roll at the upper back between the scapula.13–15 This allows the shoulder to fall backwards with gravity, moving the humeral head and deltoid prominence away from the path of needle insertion. However, there is a lack of evidence to support this shoulder position. Two small studies showed that shoulder retraction reduced SV’s CSA when compared to neutral position.16,17 Another study did not find any significant difference in CSA between shoulder retraction and neutral position. 18
Other authors have proposed shoulder abduction since the visualisation of the SV may be enhanced by displacing the clavicle cranially. 19 A small study showed that shoulder abduction reduced the skin-to-vein distance when compared to shoulder adduction, but it did not alter the diameter of SV. 20 Another small study by Sadek et al. 21 showed that shoulder abduction increased the CSA of SV, when compared to neutral position.
Objectives
The objective of this study is to determine which shoulder position results in the largest CSA for right subclavian line insertion. We hypothesised that the CSA will be largest in shoulder abduction since the compressive effect by the clavicle on SV will be the least.
Methods
Study design and setting
This is a prospective observational study conducted in Queen Elizabeth Hospital in Hong Kong. Recruitment and data collection were conducted between April 2019 to June 2019. This study was reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 22
Participants
Healthy volunteers aged 18 years or above working at Department of Accident and Emergency in Queen Elizabeth Hospital were recruited by convenience sampling. Written informed consent was obtained for all subjects. Volunteers were excluded if they have a history of trauma or surgery to the shoulder, clavicle or spine. Volunteers with history of deep arm vein thrombosis were also excluded. Demographic data including age, gender, height, weight and body mass index (BMI) were collected.
Variables and measurement
Ultrasound was performed on subjects in supine position using the L10-5v linear probe (frequency: 5–12 MHz) of the Siemens ACUSON P500 machine. The same setting was used as default for all scans. The ultrasound transducer is placed inferior and perpendicular to the right clavicle, at the junction between medial and middle one-third of the clavicle. The location and patency of SV was confirmed by assessing its compressibility, lack of pulsation and colour flow Doppler. A single investigator obtained all images in order to achieve consistency. The investigator is a higher trainee and member of Hong Kong College of Emergency Medicine (HKCEM) with certificate in Ultrasound Induction Course by HKCEM.
Images of the right SV were recorded at 3 different positions (Figure 1):
Shoulder Neutral: supine with both arms straight in natural position, adjacent to the trunk.
Shoulder Abduction: supine with right shoulder externally rotated, arm abducted to 90°, and elbow flexed to 90°.
Shoulder Retraction: supine with a 1 L saline bag longitudinally placed at the back between the scapulae and a 5-cm head rest behind the occiput, with both arms straight in natural position, adjacent to the trunk.
Images were captured at end-expiration for consistency. Minimal pressure is applied to the probe to reduce compression. At each position, the short-axis image showing the largest SV diameter will be recorded and stored anonymously.
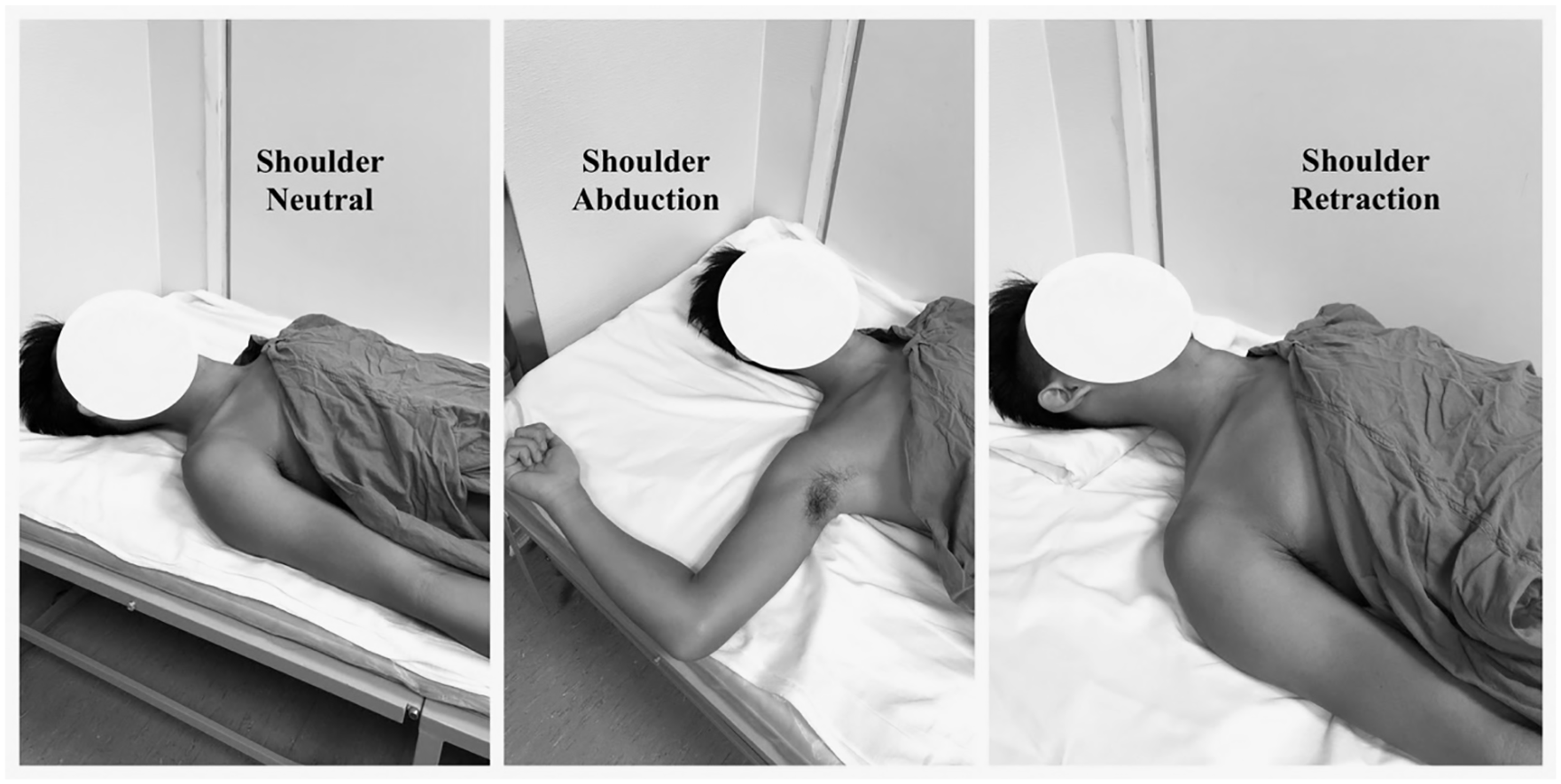
Demonstration of 3 different shoulder positions
A second independent investigator blinded from the shoulder positions analysed all the images and performed measurements using OsiriX MD version v.7.0.3 (Pixmeo, Geneva) on computer. The blinded investigator is a specialist in Emergency Medicine with Certificate in Clinician Performed Ultrasound (CCPU) by Australasian Society for Ultrasound in Medicine. CSAs (primary outcome) were measured by planimetry method (Figure 2). Skin-to-vein distance were also measured at each position.
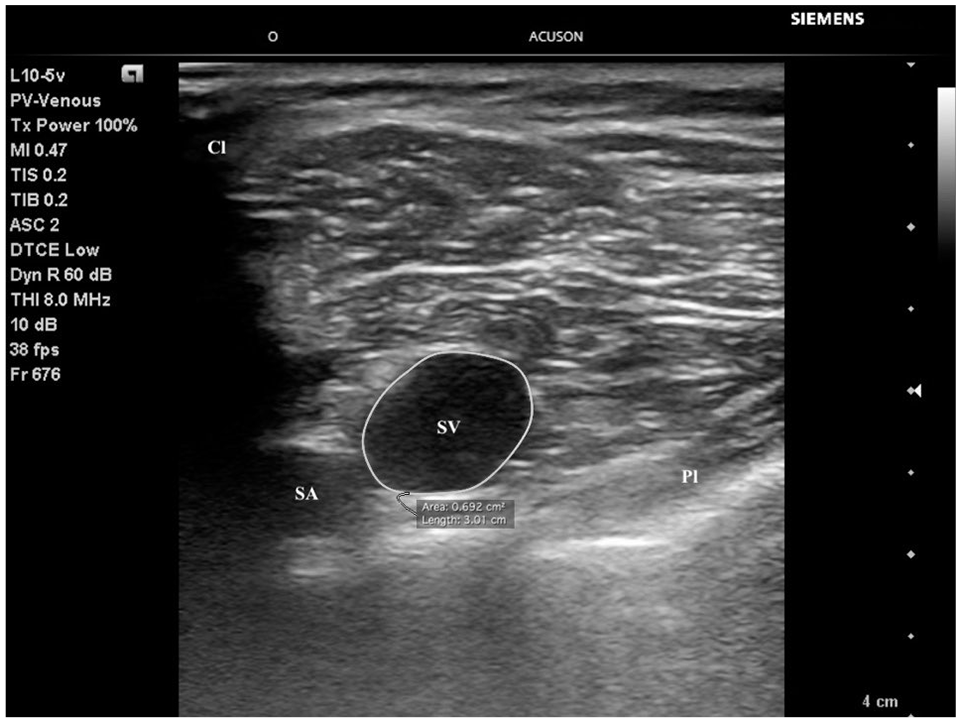
Measurement of subclavian vein’s cross-sectional area by planimetry method.
Study size and statistical methods
From literature review, the right SV CSA was 124 ± 46 mm2 in supine position. 21 To identify a 25% difference in CSA with 80% power and type 1 error <0.05, a sample size of 28 is needed.
Quantitative data are presented as means with standard deviation. One-way repeated measures analysis of variance (ANOVA) with Bonferroni post hoc analysis was performed to compare the means of three shoulder positions. A P value < 0.05 defined statistical significance. To determine if the data met the normality and sphericity assumptions for repeated measures ANOVA, the Shapiro–Wilk’s test and Mauchly’s test of sphericity were used. Student’s T-test and Pearson’s correlation coefficient were used to determine the association between gender and body habitus with CSA measurements. Data were analysed using SPSS version 23 (IBM Corp, Armonk, NY).
Results
Participants and descriptive data
Forty-four volunteers were recruited in this study. Ultrasound images and measurements and were available for all 44 participants, resulting in 132 images for analysis. The demographics of the subjects were as follow: age = 36 ± 10 years, height = 169 ± 9 cm, weight = 65 kg ± 14 kg, body mass index 22.8 ± 3.6 kg m−2, 33 male. The data in all three positions met the assumptions of normality and sphericity.
Main results
The main results are shown in Table 1. The mean CSA of the right SV in shoulder neutral, abduction and retraction were 1.05 ± 0.33 cm2, 1.01 ± 0.31 cm2 and 0.82 ± 0.28 cm2, respectively. When compared to shoulder retraction, the CSAs were significantly increased in shoulder neutral (P < 0.01) and abduction (P < 0.01) positions, with a mean increase of 0.23 ± 0.30 cm2 and 0.19 ± 0.29 cm2, respectively. There was no significant difference between shoulder neutral and abduction positions (P = 0.71).
Right subclavian vein CSA and skin-to-vein distance in different positions.
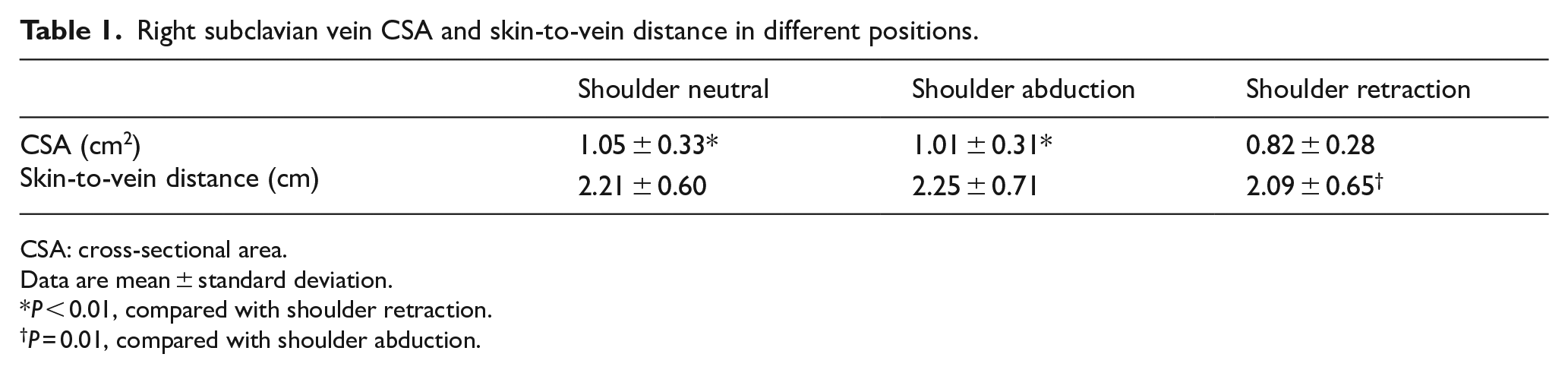
CSA: cross-sectional area.
Data are mean ± standard deviation.
P < 0.01, compared with shoulder retraction.
P = 0.01, compared with shoulder abduction.
Male had significantly larger right subclavian CSA when compared to female (Table 2) in shoulder neutral and shoulder abduction positions (P < 0.05). There was no significant difference in shoulder retraction position (P = 0.50).
Right subclavian vein CSA (cm2) compared between genders.

Using measurements in shoulder neutral position, height and right subclavian CSA were found to be moderately positively correlated, r(42) = 0.382, P = 0.01. There was no significant correlation between CSA and weight (P = 0.08) or BMI (P = 0.42).
The mean skin-to-vein distance of the right SV in shoulder neutral, abduction and retraction were 2.21 ± 0.60 cm, 2.25 ± 0.71 cm and 2.09 ± 0.65 cm, respectively. The skin-to-vein distance was significantly reduced in shoulder retraction when compared to shoulder abduction (P = 0.01). There was no significant difference when comparing shoulder neutral to shoulder abduction (P > 0.99) and shoulder retraction (P = 0.08).
Discussion
Key results and interpretation
Placing the right shoulder in neutral or abduction similarly increased the CSA when compared to shoulder retraction, with a mean increase of 0.23 ± 0.30 cm2 and 0.19 ± 0.29 cm2, respectively. The CSA was increased by 28% in shoulder neutral position when compared to shoulder retraction. The findings confirms a previous smaller study with 18 subjects 16 which found shoulder retraction reduces the CSA of SV, likely due to the anterior–posterior compression between the clavicle and the rib. However, in contrast to Sadek et al.’s 21 study, shoulder abduction did not increase the CSA when compared to shoulder neutral, possibly due to the different demographics between the participant groups.
The results showed that male gender and height correlated with a greater CSA. An ultrasound study by Lavallée et al. 23 also showed that male have a larger subclavian/axillary vein area. Interestingly, in shoulder retraction position, the difference in CSA between male and female is diminished (Table 2). A possible explanation is due to the larger pectoralis muscle bulk causing a greater compressive effect in shoulder retraction position. Body weight and BMI did not correlate with CSA.
The skin-to-vein distance was significantly decreased in shoulder retraction when compared to shoulder abduction (P = 0.01) but not shoulder neutral. Although a shorter skin-to-vein distance is more ideal, a difference of 0.16 cm (i.e. 1.6 mm) during ultrasound-guided cannulation would have little clinical significance. In practice, the advancement of needle tip would be under direct ultrasonic visualisation while gentle aspiration is performed to confirm venous puncture. A larger CSA in shoulder neutral or abduction position would have a greater clinical significance on the cannulation attempt.
Based on these findings, shoulder neutral position may be more ideal for SV cannulation. Shoulder neutral position is also practical in clinical setting as it minimises patient movements, such as turning to place a shoulder roll or manipulation of the upper limb and neck. In shoulder abduction, the right arm may also hinder the procedural field.
Limitations and generalisability
There are few limitations of this study. First, the subjects recruited were healthy young volunteers. In clinical situations where central venous catheterisation is indicated, the findings may be affected by hypovolemic state, old age or positive pressure ventilation. Second, a larger CSA visualised on ultrasound may not directly infer a higher success rate or lower complication rate. Other factors including changes in local anatomical relationships, visualisation of other important structures (e.g. pleura, artery), and ease of performing procedure in each position would also influence the success or complication rates. The probe will also be covered with sterile plastic sheath during real situation. Third, ultrasonic visualisation of SV is more difficult compared to internal jugular vein and femoral vein, especially in subjects with higher body mass index. The clavicle may partially obscure the view of the vein. Also, slight rotation, fanning or pressure to the probe can affect the short-axis view of SV resulting in an elliptical shape. These may lead to inaccurate measurements and a potential source of error.
Conclusion
Positioning the shoulder in neutral or abduction results in the greatest CSA of the right SV and may be more ideal for ultrasound-guided cannulation. Further studies are required to assess the safety and success rates in the clinical application of subclavian line insertion.
Footnotes
Acknowledgements
The authors thank Dr Rex Lam Pui Kin for providing advice on study design and statistical analysis.
Author contributions
Conceptualisation of the study was by L.H.J. and Y.L.C.M. Data curation was performed by W.L.Y. and L.H.J. Investigation (performing the scans), project administration and writing – original draft was by L.H.J. Formal analysis was performed by Y.L.C.M., L.H.J. and P.C.S. Study resources were given by L.H.J. and Y.L.C.M. Study supervision was performed by Y.L.C.M. and P.C.S. Visualisation of the study was by L.H.J., W.L.Y. and Y.L.C.M. Methodology and writing – review and editing was by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The data set for this study is available from the corresponding author.
Ethical approval
Ethical approval was granted by Kowloon East and Central Cluster Research Ethics Committee of the Hospital Authority in Hong Kong (KC/KE-19-0060/ER-4). A chaperone of the same gender as the volunteer was present during the data collection. Data storage and encryption followed the Committee’s recommendations.
Informed consent
Written informed consent was obtained by all volunteers participating in the study.
Human rights
There is no human rights issue in this study.